Research | Open Access | Volume 9 (1): Article 24 | Published: 04 Feb 2026
Views: 1,038
Menu, Tables and Figures
| Demographic variable | Frequency N=90,381 | Percentage [95% CI] |
|---|---|---|
| Age Group | ||
| <1 month | 1,397 | 1.5 [1.5 – 1.6] |
| 1–11 months | 27,239 | 30.1 [29.8 – 30.4] |
| 12–59 months | 61,745 | 68.3 [68.0 – 68.6] |
| Sex | ||
| Male | 47,160 | 52.2 [51.9 – 52.5] |
| Female | 43,221 | 47.8 [47.4 – 48.1] |
| District | ||
| Bole | 33,362 | 36.9 [36.6 – 97.2] |
| Central | 18,538 | 20.5 [20.2 – 20.8] |
| East Gonja | 6,654 | 7.4 [7.2 – 7.5] |
| North Gonja | 6,696 | 7.4 [7.2 – 7.6] |
| North-East Gonja | 2,113 | 2.3 [22.4 – 24.4] |
| Sawla-Tuna-Kalba | 13,122 | 14.5 [14.3 – 14.7] |
| West Gonja | 9,896 | 10.9 [10.7 – 11.2] |
| Year | ||
| 2017 | 22,683 | 25.1 [24.8 – 25.4] |
| 2018 | 18,416 | 20.4 [20.1 – 20.6] |
| 2019 | 18,720 | 20.7 [20.4 – 21.0] |
| 2020 | 14,540 | 16.1 [15.8 – 16.3] |
| 2021 | 16,022 | 17.7 [17.5 – 18.0] |
| Years | Cases | Population at risk | Incidence rate per 1,000 [95% CI] |
|---|---|---|---|
| 2017 | 22,683 | 92,886 | 244 [241 – 247] |
| 2018 | 18,416 | 97,377 | 189 [187 – 192] |
| 2019 | 18,720 | 97,274 | 192 [190 – 195] |
| 2020 | 14,540 | 115,680 | 126 [124 – 128] |
| 2021 | 16,022 | 120,854 | 133 [131 – 134] |
| Total | 90,381 |
Farouk Umar Saeed1, Abdul Rahman Mohammed1, Joseph Alphonsus Chantiwuni Nindow2, Gyesi Razak Issahaku3, Delia Akosua Bandoh3, George Akowuah3, Magdalene Odikro3, Ernest Kenu3, Chrysantus Kubio1
1Savannah Regional Health Directorate, Ghana Health Service, Damongo, Ghana, 2Ghana Health Service, Bole District Hospital, Bole, Savannah Region, Ghana, 3Ghana Field Epidemiology and Laboratory Training Program, School of Public Health, University of Ghana
&Corresponding author: Farouk Umar Saeed, Savannah Regional Health Directorate, Ghana Health Service, Damongo, Ghana. Email: fkumar470@gmail.com
Received: 19 Dec 2024, Accepted: 30 Jan 2026, Published: 04 Feb 2026
Domain: Infectious Disease Epidemiology
Keywords: Surveillance data, diarrhoea diseases, children under-five, Savannah Region, Ghana
©Farouk Umar Saeed et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Farouk Umar Saeed et al., Surveillance data analysis of diarrhoea diseases in children under five years, Savannah Region, Ghana, 2017 – 2021. Journal of Interventional Epidemiology and Public Health. 2026; 9(1):24. https://doi.org/10.37432/jieph-d-24-02058
Introduction: Diarrhoea constitutes a significant cause of morbidity and mortality among children under five, globally. The disease situation among children under five in the Savannah Region has not been studied. This study described diarrhoea morbidity data to determine the distribution of cases among children under five years in the Savannah Region of Ghana.
Method: We conducted a descriptive cross-sectional study using diarrhoea data of children under five extracted from the health system database from 2017 to 2021. The data was exported to Microsoft Excel 2019 and STATA 15.1 for analysis. Descriptive statistics were used to express the results as frequencies, percentages, and rates. We plotted the cases month-by-month for each year to determine seasonality.
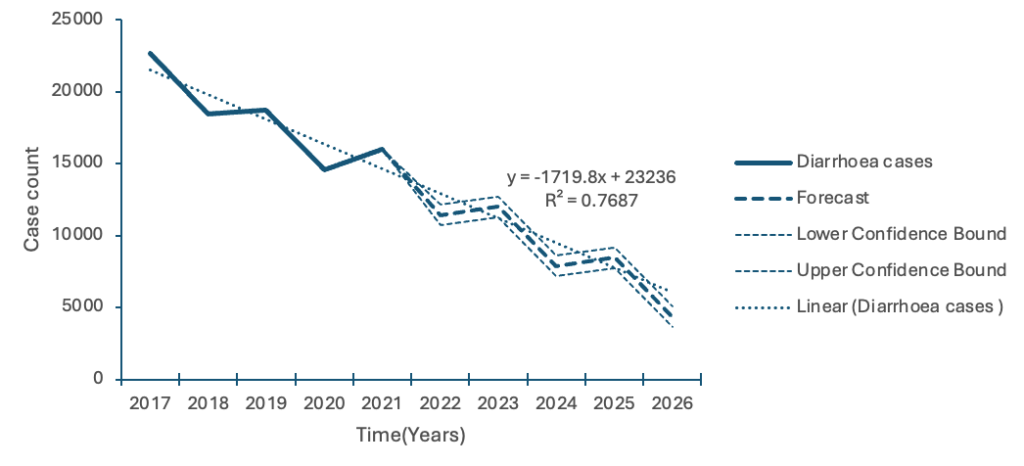
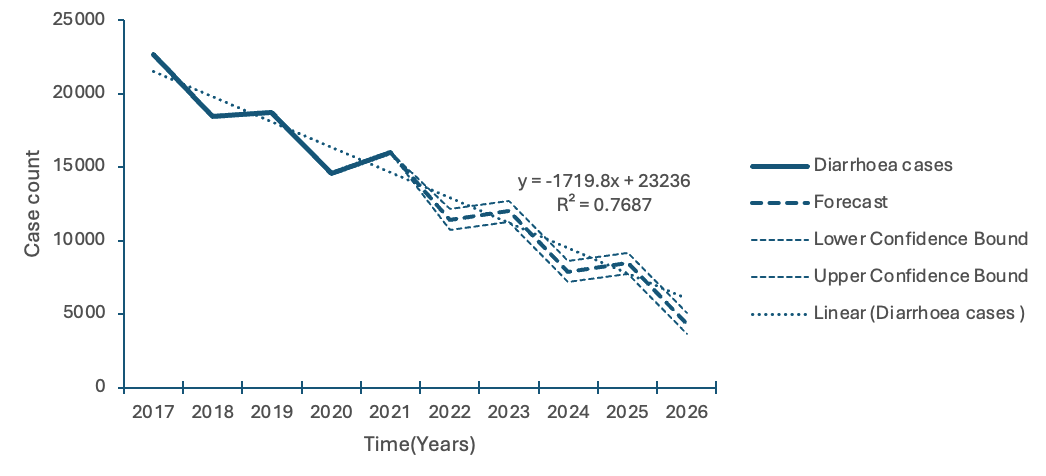
Results: A total of 90,381 cases of diarrhoea were reported, with the highest cases among children aged 12-59 months, 61,745 (68.3%). Most cases were among males, 47,160 (52.2%). Cases declined with the highest incidence in 2017 and lowest in 2020, 244 and 126 per 1000 persons, respectively. Bole district recorded the highest incidence (618 per 1000 persons in 2017). Two major peaks were recorded in January and June, with minor peaks in March and August. Rainfall did not significantly influence diarrhoea pattern (p>0.05). A five-year forecast projected a decrease in cases from approximately 11400 in 2022 to about 4300 cases by 2026.
Conclusion: Children within the age category 12-59 months and males accounted for most cases. The study illustrated seasonal variations in diarrhoea diseases, with cases in both the wet and dry seasons. All districts were affected, with the Bole having the highest burden. Cases are projected to decrease over the next five years. Health officials should strengthen surveillance and sustain interventions to reduce the incidence of diarrhoea in the region.
Globally, diarrhoea is a major public health concern with close to 1.7 billion cases reported annually among children [1]. It is the eighth leading cause of death among all age groups and the fifth leading cause of death in children younger than five years old globally [2]. It is estimated that nearly 525,000 children under five years die every year; that is almost 1,500 deaths each day from diarrhoeal diseases across the world [1]. South-East Asia and Sub-Saharan Africa contribute the highest burden of the overall global incidence of severe diarrhoeal disease [3]. These disease incidences pose a considerable threat to the attainment of Sustainable Development Goal 3 (SDG3) which aims at reducing under-five mortality to as low as 25 per 1000 live births by 2030 [4].
In Ghana, diarrhoea cases in children under five years remain high, with an estimated prevalence of 17 per cent [5]. Diarrhoeal diseases kill about 5.6 per cent of the children population each year in Ghana [6]. Ghana has been cited as one of the countries in Africa with little progress towards the reduction of under-five mortalities [7]. As part of measures to address the high under-five morbidities and mortalities, the Ghana Health Service (GHS) continues to implement several interventions and policies, such as the free Maternal and Child Health Policy and the Community-based Health Planning and Services (CHPS) Policy. Despite these interventions, diarrhoea incidence in children remains a challenge in Ghana [8].
The incidence of childhood diarrhoea varies with the season and a child’s age [9]. Children younger than five years old are the most at risk of developing severe diarrhoea and dehydration, mainly due to poor nutrition [10]. In low-income countries, children under five years of age experience, on average, about three episodes of diarrhoea every year. Each episode of diarrhoea deprives the child of the necessary nutrition for growth and development. Multiple episodes of diarrhoea can have a negative impact on a child’s growth and cognitive development [11]. In the Savannah Region of Ghana, there are two weather patterns: a wet season and a dry season. The wet season, which occurs between May and September in the northern part of the country, is short and is characterised by heavy rain [12]. The Region is grappling with inadequate water supply, sanitation and hygiene facilities. Several communities in the region practice open defecation, posing serious health challenges for the people [13].
Several studies have explored diarrhoea in children under five in relation to risk factors, prevalence, patterns and seasonality in some regions and districts in Ghana [5, 9, 14]. A study by Apanga et al. on risk factors for diarrhoea in children under five years old found the lack of formal education for mothers to be associated with a higher prevalence of diarrhoea [5]. In the Jasikan District of Ghana, a study by Tetteh J et al. on diarrhoea trends found a higher incidence among children under five years and a decreasing trend between 2012 and 2016 [14]. Anyorikeya et al. identified seasonal variations in diarrhoea cases among children under five years [9]. There is a surveillance system for diarrhoeal diseases in children under five in Ghana. Data from this system has not been analysed to describe the pattern of diarrhoea cases in children under five years in the Savannah Region. It is therefore important to provide evidence that will support the implementation of policies towards the realisation of SDG3. We described the distribution and determined the age-specific and seasonal patterns of diarrhoeal cases among children under five years in the Savannah Region using data from 2017 to 2021 and forecast the trend in the next five years. The evidence from this study will guide policy and direct public health interventions to where they are most likely to cause change.
Study design
We conducted a descriptive cross-sectional study using secondary data of diarrheal diseases in children under five years. Data was extracted from the District Health Information Management Systems version 2 (DHIMS-2) software.
Study setting
The study was conducted in the Savannah Region which occupies about 15% of the total land mass of Ghana. The Region is divided into seven administrative districts of which two are municipalities. The districts are namely; Bole, Central Gonja, East Gonja, North Gonja, North-East Gonja, Sawla-Tuna-Kalba and West Gonja. Health service in the Region is provided by a network of sub-district health facilities comprising five district hospitals, two private hospitals, three polyclinics, fourteen health centres and one hundred and forty-eight CHPS Compounds. These facilities provide diarrheal preventive and treatment services for all children under five. The Region has a population of 653, 266 with an annual growth rate of 2.1% and a population density of 18.8 persons per km2. The population is characteristically distributed in small settlements with populations of 200 – 500 people. There are over 1,250 settlements in the Region, out of which about 17% have a population less than 200 people. [15]. The distances between settlements are far apart. This peculiar pattern of distribution of population in the region has adverse implications for service delivery, as sub-district health teams (SDHTs) going on out-reach services travel long distances only to reach a small proportion of their target population.
Description of the surveillance system for diarrhea diseases in children under five in the Savannah Region
The surveillance system for diarrhea diseases in children under five in the Savannah Region operates a passive system. Health facilities report cases of diarrhea to health authorities using a standard case definition. The cases are reported as part of the outpatient morbidity report, which captures inpatient cases as well. The system also reports cases of acute watery diarrhea into the weekly and monthly integrated disease surveillance and response system (IDSR). These cases are aggregated and captured electronically into the DHIMS software. The cases are verified and validated each month by the health facility and district management teams for accuracy and timeliness. These data are available to the national and sub-national levels of the health system for decision-making.
Data collection
Data was extracted from the DHIMS software. Variables extracted included age, sex, districts, diarrhea cases and the study period. Data on children aged below five years from the DHIMS platform had been pre-categorised as <1 month, 1-11 months and 12-59 months. We obtained data on the district geo-coordinates and the arch file of the map from the surveillance unit of the Savannah Regional Health Directorate. Monthly rainfall data in the region were obtained from the office of the Ghana Meteorology Agency in the Savannah Region.
Data analysis
We exported the data to Microsoft Excel 2019 for cleaning by removing data with missing and duplicate information. Descriptive statistics like frequencies and percentages was used to present demographic information. The population of children under-five for the period under study was used to calculate the incidence rate for each year. Given the use of aggregate surveillance data, diarrheal incidence was estimated using an episode-based approach. The total number of reported diarrheal episodes among children under five during the surveillance period was divided by the estimated mid-year under-five population and expressed as episodes per child per year. The calculated incidence in the Excel was converted to a Geographical Information System (GIS) compatible format (CSV). The data was exported to a GIS software (version 3.3.4) and assigned a georeference. The choropleth map function in the GIS was then used to produce a colour gradient to represent incidence rates. The maps layout was done by adding layers, labels, and legends. The essential elements like title, scale bar, and the north arrow were added to the map and exported as a JPEG file (2017.jpeg). Using annual cases data and exponential smoothing (ETS) in Excel, diarrhea cases were forecasted for the next five years. The “Forecast.ETS” function in Excel was used to generate the forecast data with historical annual cases (2017-2021) as the input series. The five-year forecast (2022-2026) and 95% confidence interval were specified using the function “FORECAST.ETS.CONFINT”. Forecasted values were summarized and visualized using a line graph. To compare the relationship between diarrhea cases and rainfall, a time series analysis was done using an autoregressive integrated moving average (ARIMA) with the “ARMAX” syntax in the STATA software (version 15.1, Stata Corp, USA) to determine the level of significance. A p value less than 0.05 was considered statistically significant. Results were presented using tables and charts.
Ethical consideration
The study did not collect samples from humans or animals but used deidentified secondary data routinely reported into DHIMS. Permission to use the DHIMS data was obtained from the Savannah Regional Health Directorate through the Regional Director of Health Services. Ethical clearance was not sought because the data were generated and used for routine service provision. All data were secured on a computer with a password and were only accessible to the authors.
From 2017 to 2021, a total of 90,381 diarrhoeal cases among children under five years were reported. The age group with the highest number of cases was 12-59 months, 61,745 (68.3%), with the least among the age group under 1 month, 1,397 (1.5%). More than half of the cases were males, 47,160 (52.2%). The Bole District recorded the highest proportion of the cases, 33,362 (36.9%), while the least was recorded in the North-East Gonja District, 2,113 (2.3%). The highest proportion of cases was recorded in the year 2017, 22,683 (25.1%) while the least was recorded in the year 2020, 14,540 (16.1%) (Table 1).
The highest incidence rate of diarrhoea was recorded in the year 2017, with 244 per 1000 children under-five whilst the lowest incidence was recorded in 2020, 126 per 1,000 children under-five. Between 2018 and 2019, the incidence rate increased from 189 per 1,000 persons to 192 per 1,000 persons (Table 2).
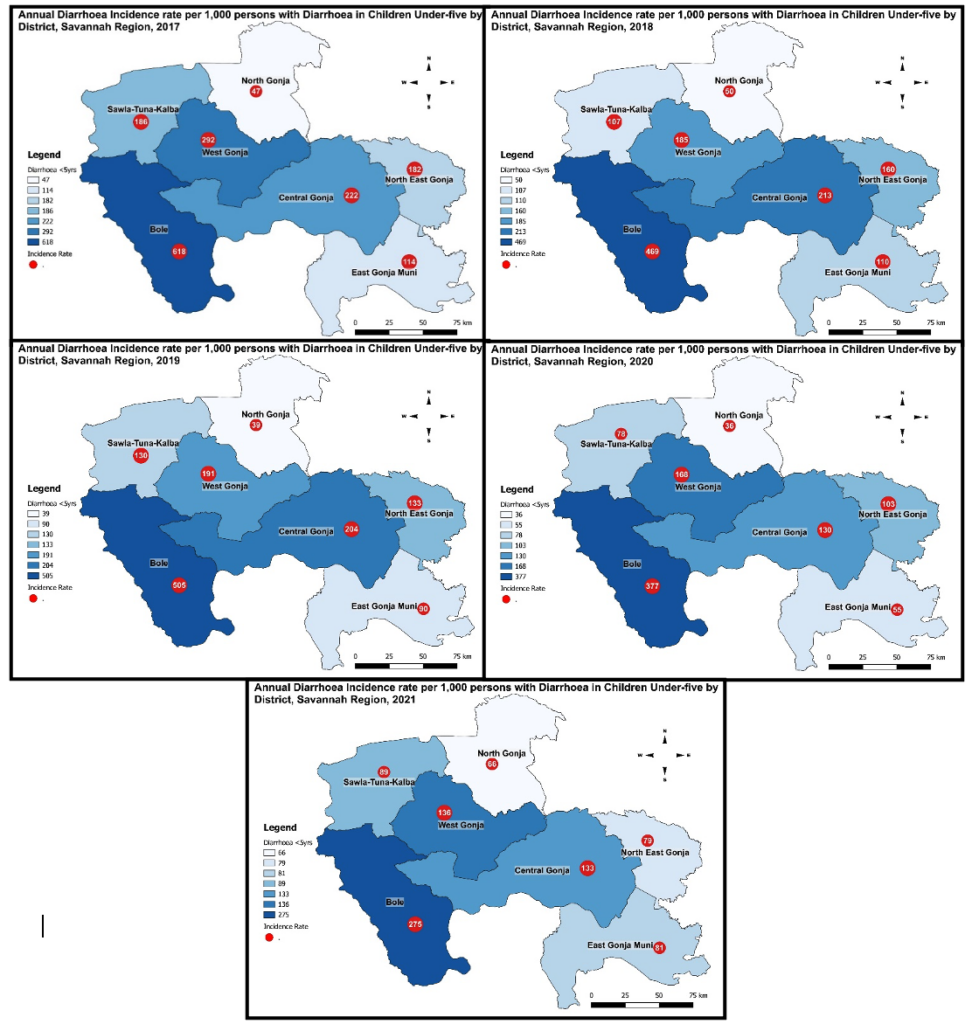
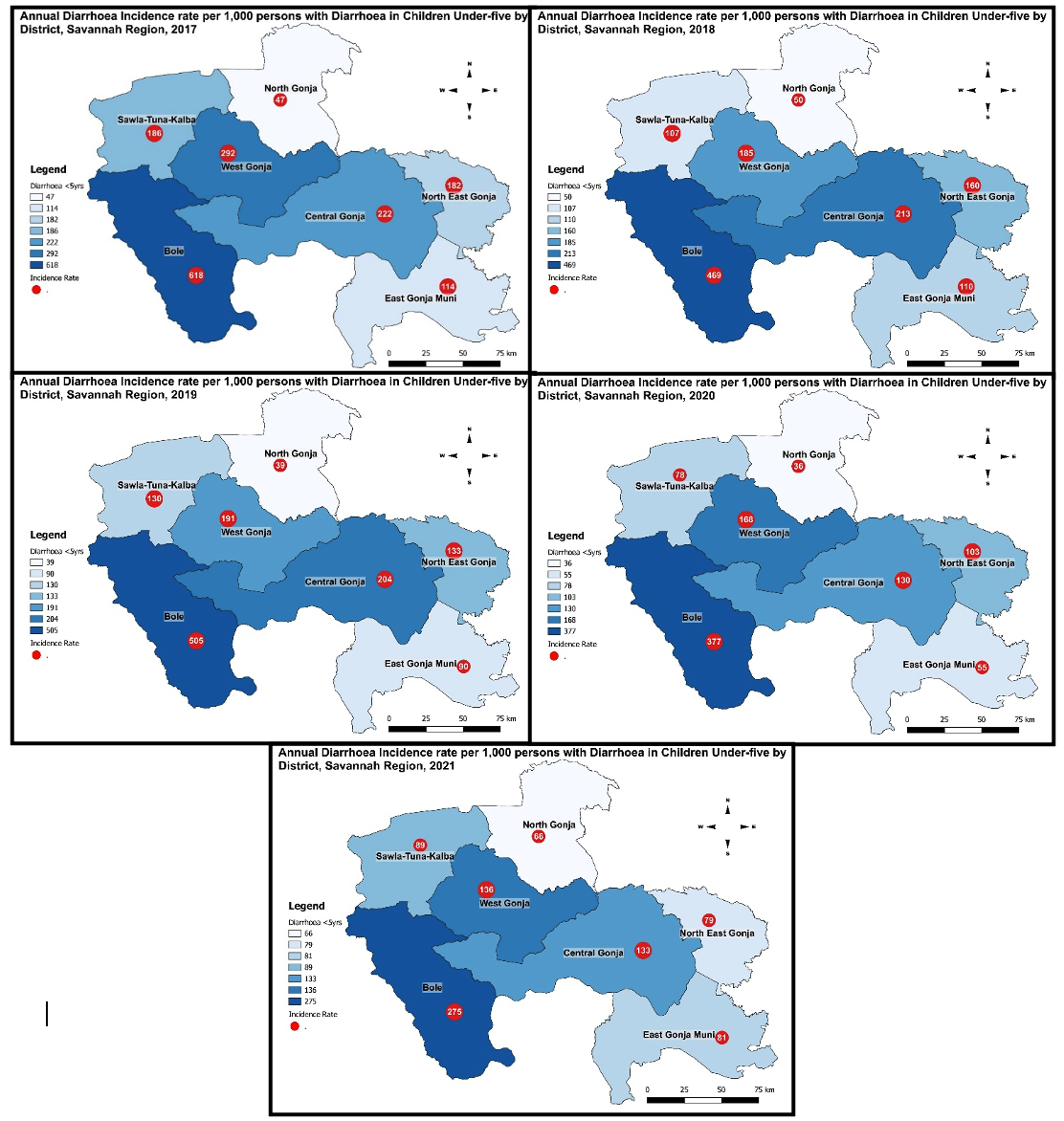
There was a general decline in diarrhoea incidence across all districts in the region between 2017 and 2021. Bole District accounted for the highest burden with incidences ranging from 618 per 1,000 persons in 2017 to 275 per 1,000 children under-five in 2021. The North-East District recorded the least incidences which increased from 47 to 66 per 1,000 children under-five within the same period (Figure 1).
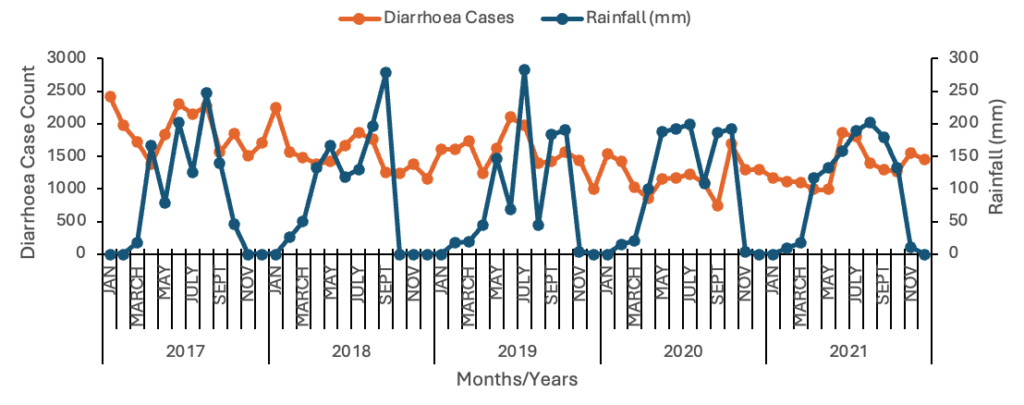
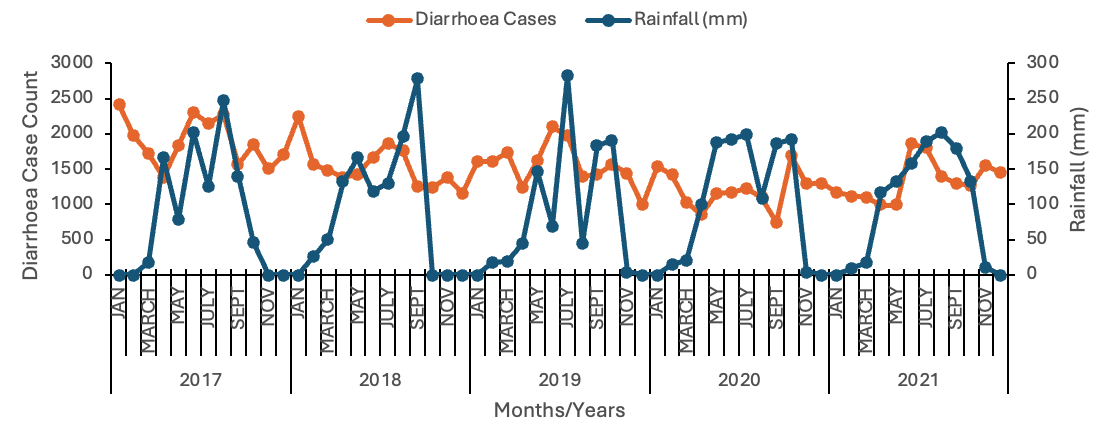
Figure 2 shows the seasonal pattern of rainfall and diarrhoea cases in children under-five from 2017 to 2021. Over the period, the pattern of diarrhoea cases can be described as fluctuating with peaks in both periods of high and low rainfall. The highest peak was recorded in the month of January, 2017 in which there was no rainfall. Three major peaks were recorded in the months of January 2017, January 2018, June 2019, October 2020 and June 2021. There were minor peaks in August 2017 and March 2019. There was a general increase in rainfall from March with a decline from September to December of each year (Figure 2).
Figure 3 illustrates the five-year forecast of annual diarrhoea cases in children under-five from 2022 to 2026. The central dashed line indicates the forecasted cases with the lower and upper 95% confidence bounds. The cases are projected to decrease steadily over the period from approximately 11,440 cases in 2022 to about 4300 cases by 2026. The upper confidence limit suggests that annual cases could reach up to 5075 by 2026, whereas the lower limits point to a potential drop to a minimum of 3620 (Figure 3).
Time series analysis
The ARIMA analysis showed a weak positive relationship between diarrhoea cases and rainfall over the period. The relationship was not statistically significant, p<0.05. The relationship within each year was also not statistically significant, as observed in the following coefficients and p-values: 2017, 0.034 p>0.05; 2018, -0.056 p>0.05; 2019, 0.137 p>0.05; 2020, -0.016 p>0.05; 2021, -0.019 p>0.05.
This study examined the distribution of diarrhoea diseases in children under five years old in the Savannah Region from 2017 to 2021. The study found that the most affected age group was children aged 12-59 months. This finding contrasts an earlier study by Anyorikeya et al. which found that children within the age category 0-11 months were the most affected [9] but consistent with a study in Nigeria that found children 12-59 months to be the most affected [16]. The older age group being impacted more might be because they are active and play with little attention from their mothers compared with the younger age group. In Ghana, children 0-5 months old are exclusively breastfed followed by complementary feeds [17]. Although the study did not assess this practice, we could associate the lower cases among the younger age groups with these events if the mothers practice exclusive breastfeeding. Breastfeeding provides innate immunity and reduces the risk of diarrhoea [18]. Moreover, there could be possible contamination of complementary feeds being introduced to the older age groups by their mothers.
The annual incidence of diarrhoea diseases over the five-year period showed a declining trend with the highest incidence in 2017 and the least in 2020. There was a slight increase in the incidence rate from 2020 to 2021. The reduction in diarrhoea incidence in 2020 could be because of the promotion of hand washing and IPC interventions as part of the public health response to the outbreak of COVID-19. Several other interventions are being championed to improve water, sanitation and hygiene promotion across all regions in Ghana. Key among these interventions are the World Vision Ghana and UNICEF Ghana WASH programs in communities and households aimed at reducing communicable diseases including diarrhoea morbidities in children under five[13]. The decline in diarrhoea incidence over the years could be attributed to the impact these interventions have made over the years. A study by Appiah-Effah et al. in Northern Ghana revealed the impact WASH interventions had on the reduction of diarrhoea diseases [19]. We can also attribute this observation to improved data validation and auditing at the various tiers of reporting. The increase in the incidence from 2020 to 2021 could be due to the reluctance of WASH interventions after the COVID-19 pandemic was controlled [20].
An analysis of the case incidence by geographical area showed Bole District experienced the highest burden of diarrhoeal disease in children under -five. The district with the least burden of diarrhoeal disease in under-five children was North-East Gonja. One plausible reason could be the number of health facilities dotted in and around communities. Bole District for instance has one of the biggest hospitals, functional CHPS and health centers in the region with a high OPD attendance. There is therefore improved access to health and surveillance for diarrhoea in the district. In contrast, the North-East Gonja District has fewer health facilities and no major hospital. Moreover, the Bole District is particularly affected by the activities of illegal miners such as diverting water bodies and use of chemicals to extract gold that could potentially lead to the contamination of sources of drinking water via heavy metal poisoning for people in the affected communities.
The study illustrated seasonal variations of diarrhoea among children under-five with cases reported in both the dry and wet seasons. The months with the highest cases of diarrhoea coincided with the short rainy season of the year in the region, having peaked in June 2019 and 2021, and October 2020. Other peaks were recorded in the dry season with the highest peak in January, 2017 and a minor peak just before the rainy season in March, 2019. In a similar study by Anyorikeya et al., diarrhoea cases among children under-five showed a bimodal seasonality with the highest peaks in the rainny season except in January and minor peaks in the dry season [9]. The rainy season in the Savannah Region of Ghana is characterised by heavy rainfall with pockets of floods. These floods exacerbate conditions by carrying human fecal matter through open sewage into homes and drinking water sources. . On the other hand, the dry season limit access to clean and safe drinking water with some people resorting to stagnant water for drinking. These events could be indirectly impacted by the global climate change. In a study in the Nepal on the effects of climate change on diarrhoea among children under-five, increase in rainfall and temperature was associated with a rise in diarrhoea cases among chilidren under five years [21].
The annual cases forecast showed a projected decrease between 2022 and 2026. The projected downward trend suggests that the burden of diarrhoea disease is likely to decrease, should conditions remain the same. This may be associated with factors such as improvement in surveillance and reporting of cases, broad sector collaborations, health education and improved water and sanitation conditions. Policy makers should therefore be guided by this projection to put in an adequate preparedness plan and sustain the current interventions to reduce the diarrhoea disease burden over the forecasted period.
Limitations
This research is not without limitations. First, our study utilised diarrhoea data extracted from DHIMS II database that was collected by health facilities based on a clinicians’ understanding and application of case definition for diagnosis of diarrhoea. As a result, there is the potential for misclassification of diarrhoea diseases since laboratory confirmation is not routinely recommended for surveillance purposes. This therefore presents the opportunity for inaccuracies in reporting of cases. Secondly, there could be underreporting of cases due to limited access to healthcare in some districts. Again, the lack of laboratory confirmation limits the identification of different causative agents of diarrhoea. Lastly, the data extracted from DHIMS have been precoded into specific age categories as <1 month, 1-11 months and 12-59 months. This made it impossible to estimate the burden of diarrhoea among children aged 12-23 months.
Children within the age category 12-59 months and males were the most affected. The study showed seasonal variations in diarrhoea diseases with cases occuring in both the wet and dry seasons. Diarrhoea incidence declined over the period with the Bole District disproportionately affected. Cases are projected to decline steadlily over the next five years. The regional health directorate should collaborate with the local government to implement programs aimed at strengthening water, sanitation and hygiene practices and distribute water purifier tablets to house holds especially during the rainny season. The Ghana Water Company should improve the supply of portable water to the communities to reduce the incidence of dirrhoea diseases in the region.
What is already known about the topic
What this study adds
FUS, CK, JACN, were responsible for conceptualization of the study. FUS was responsible for data collection and analysis. FUS, CK and JACN drafted the manuscript. GRI, DAB, GA, EK critically reviewed and equally contributed to the content of the manuscript. All authors read and approved of the final manuscript.
| Demographic variable | Frequency N=90,381 | Percentage [95% CI] |
|---|---|---|
| Age (months) | ||
| <1 | 1,397 | 1.5 [1.5 – 1.6] |
| 1–11 | 27,239 | 30.1 [29.8 – 30.4] |
| 12–59 | 61,745 | 68.3 [68.0 – 68.6] |
| Sex | ||
| Male | 47,160 | 52.2 [51.9 – 52.5] |
| Female | 43,221 | 47.8 [47.4 – 48.1] |
| District | ||
| Bole | 33,362 | 36.9 [36.6 – 97.2] |
| Central | 18,538 | 20.5 [20.2 – 20.8] |
| East Gonja | 6,654 | 7.4 [7.2 – 7.5] |
| North Gonja | 6,696 | 7.4 [7.2 – 7.6] |
| North-East Gonja | 2,113 | 2.3 [22.4 – 24.4] |
| Sawla-Tuna-Kalba | 13,122 | 14.5 [14.3 – 14.7] |
| West Gonja | 9,896 | 10.9 [10.7 – 11.2] |
| Year | ||
| 2017 | 22,683 | 25.1 [24.8 – 25.4] |
| 2018 | 18,416 | 20.4 [20.1 – 20.6] |
| 2019 | 18,720 | 20.7 [20.4 – 21.0] |
| 2020 | 14,540 | 16.1 [15.8 – 16.3] |
| 2021 | 16,022 | 17.7 [17.5 – 18.0] |
| Years | Cases | Population at risk | Incidence rate per 1,000 [95% CI] |
|---|---|---|---|
| 2017 | 22,683 | 92,886 | 244 [241 – 247] |
| 2018 | 18,416 | 97,377 | 189 [187 – 192] |
| 2019 | 18,720 | 97,274 | 192 [190 – 195] |
| 2020 | 14,540 | 115,680 | 126 [124 – 128] |
| 2021 | 16,022 | 120,854 | 133 [131 – 134] |
| Total | 90,381 |