Research | Open Access | Volume 9 (2): Article 67 | Published: 24 Apr 2026

Views: 2,087
Menu, Tables and Figures
| Year | Institutional live births | Institutional neonatal deaths | Neonatal mortality rate (per 1,000) [95% CI] | ||
|---|---|---|---|---|---|
| Year | Institutional live births | Early (%) | Late (%) | Total | Neonatal mortality rate (per 1,000) [95% CI] |
| 2018 | 12,478 | 15 (71.4) | 6 (28.6) | 21 | 1.7 [1.0 – 2.6] |
| 2019 | 13,895 | 29 (90.6) | 3 (9.4) | 32 | 2.3 [1.6 – 3.2] |
| 2020 | 14,536 | 38 (95.0) | 2 (5.0) | 40 | 2.8 [2.0 – 3.7] |
| 2021 | 16,020 | 57 (91.9) | 5 (8.1) | 62 | 3.9 [3.0 – 5.0] |
| 2022 | 16,652 | 39 (100.0) | 0 (0.0) | 39 | 2.3 [1.7 – 3.2] |
| Total | 73,581 | 178 (91.8) | 16 (8.2) | 194 | 2.6 [2.3 – 3.0] |
Table 1: Characteristics of neonatal deaths, Savannah Region, 2018-2022
Chrysantus Kubio1, Williams Azumah Abanga2,&, Cynthia Kubio3, Abubakr Ahmed Farhan1, Jonas Abodoo1, Kwabena Adjei Sarfo1, Wadeyir Jonathan Abesig4, Christopher Sunkwa Tamal5, Michael Rockson Adjei5
1Savannah Regional Health Directorate, Ghana Health Service, Savannah Region, Damongo, Ghana, 2Saboba District Health Directorate, Ghana Health Service, Northern Region, Saboba, Ghana, 3Tamale Metropolitan Health Directorate, Ghana Health Service, Northern Region, Tamale, Ghana, 4Bole District Hospital, Ghana Health Service, Savannah Region, Bole, Ghana, 5WHO Country Office, Accra, Ghana
&Corresponding author: Williams Azumah Abanga, Saboba District Health Directorate, Ghana Health Service, Northern Region, Saboba, Ghana, Email: willabanga@gmail.com ORCID: https://orcid.org/0009-0003-6523-3171
Received: 30 Mar 2025, Accepted: 21 Apr 2026, Published: 24 Apr 2026
Domain: Maternal and Child Health
Keywords: Neonatal mortality rate, live births, DHIMS-2, Savannah Region, Ghana
©Chrysantus Kubio et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Chrysantus Kubio et al. Trends and distribution of neonatal mortality rate in the Savannah Region, Ghana, 2018-2022. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):67. https://doi.org/10.37432/jieph-d-25-00083
Introduction: Globally, there has been slow progress in the reduction of neonatal mortality. Sub-Saharan Africa accounts for 43% of the global neonatal mortality burden. Given the variation in neonatal mortality in Northern Ghana, coupled with the paucity of baseline information in the Savannah Region, this study is envisaged to inform preventive measures to improve newborn health outcomes. We determined the rate, trend and distribution of neonatal mortality in the Savannah Region of Ghana.
Methods: We conducted a descriptive secondary data analysis of District Health Information Management System 2 (DHIMS2) neonatal mortality data in the Savannah Region from January 2018 to December 2022. Aggregated data on births, category of neonatal death, district and year mortality occurred were extracted and analysed using Microsoft Excel 2016 and Quantum Geographic Information System Software version 3.3. Descriptive statistics were performed using proportions and rates, with the findings presented in tables, graphs and maps.
Results: The Savannah Region recorded 73,581 institutional live births between 2018 and 2022, with 0.26% (194/73,581) neonatal mortalities. The majority, 91.8% (178/194), of neonatal deaths occurred in the early neonatal period. The regional neonatal mortality rate over the study period was 2.6 [95% CI: 2.3 – 3.0] per 1,000 live births. Neonatal mortality increased from 1.7 [95% CI: 1.0 – 2.6] per 1,000 in 2018 to a peak of 3.9 [95% CI: 3.0 – 5.0] per 1,000 in 2021 and declined to 2.3 per 1,000 in 2022. The district neonatal mortality rate varied between 0.6 and 6.9 deaths per 1,000 live births in North-East Gonja and West Gonja Districts, respectively.
Conclusion: Despite the general increasing trend of neonatal mortality over the period, the overall rate was low compared to the national rate. All districts in the Savannah Region recorded neonatal mortalities, with the West Gonja Municipality reporting the highest rate. Local health authorities need to design strategies to promote healthy care practices in the early neonatal period to sustain the low neonatal mortalities.
Globally, there has been slow progress in the reduction of neonatal mortalities, with an estimated 2.4 million newborn deaths recorded in 2020, accounting for 47% of children under-five mortalities [1]. Sub-Saharan Africa recorded the highest estimated neonatal mortality rate (NMR) of 27 deaths per 1,000 live births and accounts for 43% of the global burden of neonatal deaths [1]. Neonatal deaths occur mostly among rural residents and are suggested to be correlated with maternal socioeconomic status and healthcare delivery factors such as level of education, income level, skilled delivery, distance and travel time to health facilities [2–4]. The implementation and scale-up of interventions such as facility-based delivery, quality post-natal care and effective treatment of sick newborns have helped to reduce NMR, aiming towards the global target of less than 12 deaths per 1,000 live births by 2030 [5]. The prevention of neonatal mortalities hinges on access to cost-effective interventions during pregnancy, childbirth and the postnatal period through quality antenatal care, safe and clean delivery and comprehensive care for sick newborns, low birth weight and preterm babies at health facilities [5, 6].
Early neonatal mortalities generally account for the majority of newborn deaths [7–9]. There has been a declining trend of NMR globally, including Ghana [3, 10, 11]. Findings have shown geographical variations of neonatal mortalities, with clustering of high rates at localities in Tanzania [12], Ethiopia [13], Ghana [14, 15], and across districts in East and West Africa [16].
The Savannah Region is one of the newly created regions in Ghana with limited resources to meet the health needs of the population, such as access to antenatal care (ANC), skilled deliveries, immunisations, postnatal care (PNC) and intensive care units for sick newborns [17]. The region has a low (30.1%) proportion of pregnant women receiving two or more doses of tetanus toxoid vaccination [18], a risk factor for neonatal tetanus, which accounts for substantial newborn deaths [19]. Given the variation in neonatal mortalities in Northern Ghana, coupled with the paucity of baseline information in the Savannah Region, findings on neonatal mortality rates, trends and distributions in the region may help inform preventive measures to improve newborn health outcomes. Child health program managers may also use the study findings to evaluate the effectiveness of newborn survival interventions implemented over the past decade. This study, therefore, determined the rate, trend and distribution of neonatal mortality in the Savannah Region of Ghana for 2018 to 2022.
Study design and settings
Secondary data analysis was conducted using neonatal mortality data from the District Health Information Management System 2 (DHIMS2) of the Savannah Region from 2018 to 2022. This study was conducted in the newly created Savannah Region of Ghana. There are seven districts in the region with a projected population of 653,266, with 26,131 expected pregnancies in 2022 [20]. The region is predominantly rural, with the majority of inhabitants being farmers. There are 148 Community-based Health Planning and Services (CHPS) compounds, 23 health centres, and five primary hospitals. CHPS is an initiative aimed at improving access to primary health care, including postnatal and newborn care in rural communities across Ghana. The region has five neonatal intensive care units (NICU) located in the Bole, Sawla-Tuna-Kalba, Central Gonja, East Gonja and West Gonja District Hospitals, which provide inpatient care to seriously ill neonates [17]. Nonetheless, the CHPS compounds and health centres have the capacity to provide care to sick neonates and appropriately refer to higher-level health facilities.
Data collection
Institutional births and neonatal mortalities of the Savannah Region for the period of 2018 to 2022 were extracted from the DHIMS2 database. The DHIMS2 is an electronic platform used to maintain and update data on diseases and health events by the Ghana Health Service (GHS). All health facilities record data on births in the delivery registers and collate it using the monthly midwife form and reported into the DHIMS2 database. Neonatal deaths are also collected using the monthly midwife form and reported into DHIMS. We extracted aggregated data on live births, category of neonatal deaths, district and year of mortality occurrence.
Definition of terms
Early neonatal death: Death among live births between zero and seven days after birth.
Late neonatal death: Newborn death occurring after seven days to 28 days following birth.
Data quality and validity
The extracted data from DHIMS2 was verified with monthly midwife reports generated at health facilities and reported into the database. This process helped to ensure that quality data was used for the analysis. Also, it has been shown that there is over 90% maternal health data accuracy and completeness in Ghana, suggesting a high level of data quality [21, 22].
Data analysis
Descriptive statistics were performed based on person, place and time using Microsoft Excel version 2016 and Quantum Geographic Information System (QGIS) version 3.3. A choropleth map was created and used to display the disparities of neonatal mortalities with a colour gradient using the join and symbology tools of QGIS. The NMR was calculated by dividing the total neonatal deaths by total live births per 1,000 for each district and year. The five-year overall NMR was also calculated by dividing the overall five-year reported neonatal deaths by the five-year live births per 1,000. The results were presented as proportions and rates in tables, graphs and maps.
Ethical consideration
Neonatal deaths are routinely reported as part of the Integrated Disease Surveillance and Response framework as anonymised data into the DHIMS2 database. This study used aggregated secondary data for the analysis. Thus, no formal ethical approval and/or informed consent were required. This is in line with Act 851, 2012, Ghana’s Public Health Act, which requires surveillance data on public health events and diseases to be maintained and updated by the Ghana Health Service. Nonetheless, the Savannah Regional Health Directorate granted administrative authorization to access the DHIMS2 database and extract the dataset for the study.
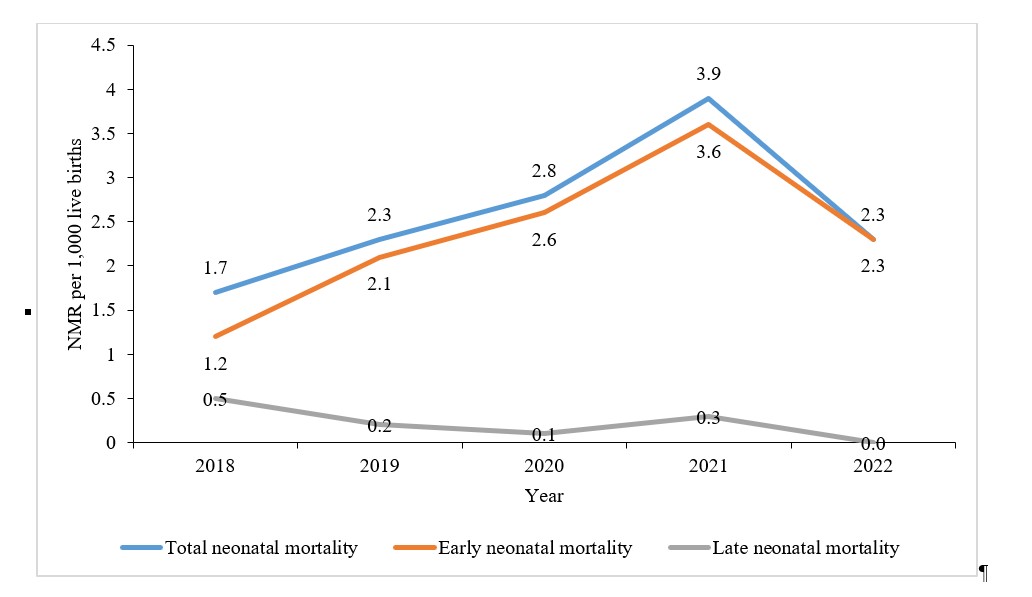
Over the five-year study period, a total of 194 neonatal deaths were recorded in the Savannah Region. The majority of neonatal deaths occurred in the early neonatal period (Table 1). The overall NMR over the five years was 2.6 [2.3 – 3.0] per 1,000 live births. There was an increasing trend of NMR, which peaked in 2021 with a rate of 3.9 [95% CI: 3.0 – 5.0] deaths per 1,000 live births and declined to 2.3 [95% CI: 1.7 – 3.2] per 1,000 live births in 2022. Early neonatal mortalities substantially increased from 1.7 to 2.3 per 1,000 live births between 2018 and 2022. However, there was a decline in late NMR from 0.5 to 0.0 per 1,000 live births over the five years (Figure 1).
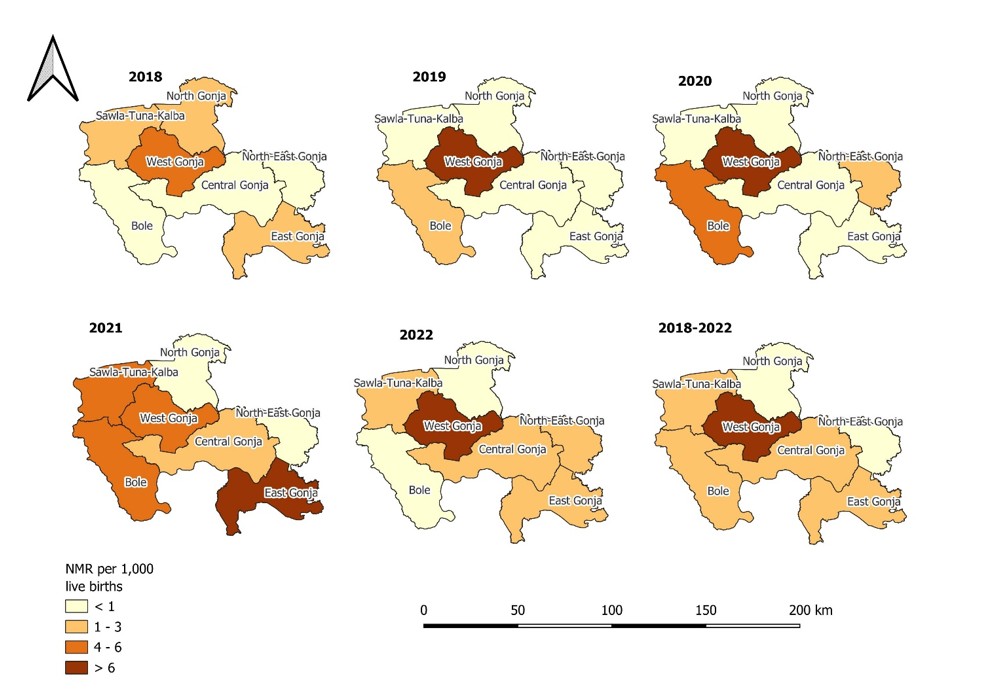
Neonatal deaths were recorded across all the districts in the Savannah Region, with district overall rates varying from 0.6 to 6.9 per 1,000 live births. The highest rate of 6.9 per 1,000 was reported in West Gonja District, with the lowest rate of 0.6 per 1,000 observed in North-East Gonja (Figure 2).
We analyzed neonatal mortality secondary data of the Savannah Region from 2018 to 2022, which showed a low NMR with an increasing trend over the period. The review showed that NMR was low over the five-year period, which suggests that the Savannah Region is on track to achieve the neonatal mortality target (12 per 1,000 live births) of the Sustainable Development Goals. The improvement of health infrastructure, such as the establishment of two primary hospitals between 2021 and 2022, may have influenced the low NMR [17]. The reported high coverage of essential maternal health services, such as four or more ANC visits (79.5%), institutional deliveries (70.6%) and PNC within two days following birth (81.5%) [18] may be potential factors for the low incidence observed in this study. Comparatively, secondary data analysis of NICUs data in Ghana from the Tamale Teaching Hospital [23], Korle-Bu Teaching Hospital [24], Komfo Anokye Teaching Hospital [25], Regional and District Hospitals in the Upper West Region [26] and facility-based studies in Ethiopia [9, 27] found higher newborn mortality rates. These studies were based on sick newborns at various inpatient health facilities, mostly referred from lower health facilities, which may account for the high mortality rates. Additionally, community-based studies in Ethiopia [28] and Uganda [29] reported high neonatal mortality rates of 22.2 and 34 per 1,000 live births, respectively. Furthermore, the national NMR of 17 per 1,000 live births and 32 per 1,000 live births for the Savannah Region, as documented in the Ghana Demographic and Health Survey, were high compared to the findings of this study [18]. Limited access to inpatient neonatal care facilities and low coverage of essential postnatal care services may have influenced the high mortality rates observed in these community-level studies.
We found that over 90% of neonatal mortalities occurred within the first seven days following birth. The inadequate postnatal care for a substantial number of newborns and persistent home deliveries (29.4%) in the Savannah Region [18] may be contributing to the inability to timeously identify sick neonates and provide effective treatment, thus resulting in these preventable deaths. Similarly, facility-based studies in Ghana [23] and Ethiopia [9] revealed that the majority of newborn deaths occur within the early neonatal period. These studies suggested that sub-optimal care provided to critically ill newborns and low coverage of essential neonatal health services may have contributed to the high deaths recorded in the early neonatal period. Therefore, it is crucial to improve the quality of postnatal care in the region to help identify danger signs in newborns and provide essential care to mitigate neonatal deaths within the first seven days following delivery.
The trend of neonatal mortality increased over the study period, especially between 2020 and 2021. This period coincided with the COVID-19 pandemic. Research in Ghana showed that COVID-19 was linked to about 25% to 65% decline in the coverage of maternal health services such as ANC visits, skilled delivery and family planning services [30]. This disruption of health delivery and reduced utilisation of essential health services due to the COVID-19 pandemic could have potentially influenced the substantial increase in newborn mortalities between 2020 and 2021. However, there was a reduction in neonatal mortalities in 2022. In that same year, two primary hospitals, equipped with NICUs and trained health professionals, were operationalised in the Central Gonja and Sawla-Tuna-Kalba Districts. The functionality of these facilities may have endeared community members in the two districts to seek treatment for sick newborns. This may have contributed to improved access to essential life-saving care for newborns. Thus, the neonatal mortalities may have declined in 2022 alongside the NICU expansions. Contrarily, previous findings in Ghana using the Ghana Demographic and Health Survey data from 1998 to 2017 and facility data from 2013 to 2017 showed a declining trend of neonatal deaths [11, 23]. Other studies also found a decreasing trend of neonatal mortality rates in Brazil [3] and multiple countries globally [10], which were attributed to the training of personnel on neonatal resuscitation, essential newborn care and increasing access to inpatient infrastructure for neonates.
Newborn deaths were recorded across the seven districts of the Savannah Region, with geographical variations and the highest rate observed in West Gonja Municipal. Until recently, the Sawla-Tuna-Kalba and Central Gonja Districts lacked primary hospitals. Therefore, critically sick newborns in these districts were almost always referred to West Gonja Municipal Hospital for inpatient neonatal care, which may have contributed to the high incidence of neonatal mortality. Also, delayed referral, sub-optimal pre-referral treatment practices and poor care along the referral continuum could have influenced the deaths of newborns upon arrival at the NICU in the West Gonja Municipal Hospital. The lack of equipment, essential medicines, competent and skilled staff at the referral unit to resuscitate sick neonates may be potential factors for high mortalities. Consistent with this finding, studies in Ghana [14, 15], Burundi [31], Tanzania [12] and Ethiopia [13] indicated geographical variations of neonatal mortalities with clusters of high incidence.
Strengths and limitations
The findings from this study offer baseline information about the incidence of neonatal mortalities in the newly created Savannah Region of Ghana. This study also paves the way for local health authorities to design strategies to improve neonatal survival. Nonetheless, the aggregated data from DHIMS2 limited the data analysis. The data used for the analysis did not capture information on neonates admitted for treatment and the causes of neonatal mortalities. This affected the detailed analysis. Also, about 30% of deliveries in the region occurred outside health facilities [18]. Neonatal deaths could have been recorded among these deliveries that were not reported in the facilities. This could have led to an underestimation of the NMR. Despite the stated drawbacks, this research is the first to document the incidence, trend and geographical variation of neonatal mortalities in the Savannah Region, paving the way for further investigations into potential barriers to neonatal survival in the region. However, we recommend a policy review to make provision for the variability of neonatal mortality data captured in the DHIMS-2 to enable greater analytical depth.
The regional neonatal mortality rate was low over the five-years, with an increasing trend which peaked in 2021. The majority of neonatal deaths occurred within the early neonatal period. There was observed geographical variation of newborn deaths in the Savannah Region. The West Gonja Municipality recorded the highest neonatal mortalities. Local health authorities need to design strategies to promote healthy neonatal care practices in the early neonatal period to sustain the low neonatal mortalities. Also, there is the need for regular upgrading and retooling of NICU equipment, advanced neonatal care training for staff attending to sick newborns in the West Gonja Municipality to help mitigate the district’s high NMR. Furthermore, neonatal referral systems and neonatal death audits should be instituted to help identify gaps in the neonatal healthcare continuum for targeted interventions. The regional health authorities should organise community durbars on newborn health care and healthy practices. The Regional Research Unit should conduct further studies to ascertain the potential factors contributing to the high newborn mortalities in West Gonja Municipality and also determine the true burden of neonatal mortalities at the community level. It is imperative to provide the requisite equipment and health personnel to the NICU of West Gonja Municipal Hospital to facilitate quality care rendered to sick neonates. There is a need to improve the referral system in the region to ensure sick neonates in districts without primary hospitals are promptly transferred to facilities with NICUs for treatment.
What is already known about the topic
What this study adds
CK and WAA: conceptualized the study. CK, WAA, JA, CK and KAS: extracted, analyzed and interpreted the data. CK, WAA and AAF: drafted the manuscript. WJA, CK, CST and MRA: reviewed the manuscript. All authors read and approved the final version of the manuscript for submission.
| Year | Institutional live births | Institutional neonatal deaths | Neonatal mortality rate (per 1,000) [95% CI] | ||
|---|---|---|---|---|---|
| Year | Institutional live births | Early (%) | Late (%) | Total | Neonatal mortality rate (per 1,000) [95% CI] |
| 2018 | 12,478 | 15 (71.4) | 6 (28.6) | 21 | 1.7 [1.0 – 2.6] |
| 2019 | 13,895 | 29 (90.6) | 3 (9.4) | 32 | 2.3 [1.6 – 3.2] |
| 2020 | 14,536 | 38 (95.0) | 2 (5.0) | 40 | 2.8 [2.0 – 3.7] |
| 2021 | 16,020 | 57 (91.9) | 5 (8.1) | 62 | 3.9 [3.0 – 5.0] |
| 2022 | 16,652 | 39 (100.0) | 0 (0.0) | 39 | 2.3 [1.7 – 3.2] |
| Total | 73,581 | 178 (91.8) | 16 (8.2) | 194 | 2.6 [2.3 – 3.0] |