Research | Open Access | Volume 9 (2): Article 76 | Published: 12 May 2026

Views: 666
Menu, Tables and Figures
| Table I: Measles vaccination coverage by region, Mali, 2019-2023 | |||
|---|---|---|---|
| Characteristic | Frequency (n=5,218,714) | Estimation of annual targets (n=4,505,901) | Percentage (%) |
| Regions | |||
| Bamako | 840226 | 690355 | 121.7 |
| Gao | 176017 | 161034 | 109.3 |
| Kayes | 702115 | 601570 | 116.7 |
| Kidal | 19058 | 19158 | 99.5 |
| Koulikoro | 908120 | 755790 | 120.2 |
| Menaka | 25343 | 25600 | 99.0 |
| Mopti | 550487 | 446789 | 123.2 |
| Ségou | 810518 | 791023 | 102.5 |
| Sikasso | 981998 | 845000 | 116.2 |
| Taoudéni | 37484 | 35675 | 105.1 |
| Tombouctou | 167348 | 133907 | 125.0 |
Table I: Measles vaccination coverage by region, Mali, 2019-2023
| Table 2: Measles coverage by year and sex in Mali, 2019-2023 | ||
|---|---|---|
| Characteristic | Frequency (n=5,218,714) | Percentage (%) |
| Years | ||
| 2019 | 768378 | 14.7 |
| 2020 | 906762 | 17.3 |
| 2021 | 1035236 | 19.8 |
| 2022 | 1212279 | 23.22 |
| 2023 | 1296059 | 24.8 |
| Sex | ||
| Male | 2624940 | 50.29 |
| Female | 2581787 | 49.47 |
Table 2: Measles coverage by year and sex in Mali, 2019-2023
| Table 3: Impact of the pandemic on vaccination programs from 2019 to 2023 | ||||
|---|---|---|---|---|
| Periods | Percentage points by year | Coefficient for the variable | IC 95% | p-value |
| Pre-pandemic | 2.76 | β1 = -0.0276 | -0.0322 ; -0.0231 | 0.0014 |
| During pandemic | 6.59 | β2 = -0.0659 | -0.0819 ; -0.0499 | 0.0031 |
| Post-pandemic | NA | NA | NA | |
| NA: Not Available | ||||
Table 3: Impact of the pandemic on vaccination programs from 2019 to 2023
Souleymane Togola1,2,&, Souleymane Sékou Diarra2,4, Yaya dit Sadio Sarro1,3, Bassirou Diarra1,3, Cheick Abou Coulibaly1, Salia Keita1, Ibrahim Bah1,4, Seydou Doumbia1,3
1Public Health Teaching and Research Department, Bamako, Mali, 2National Public Health Institute, Bamako, Mali, 3University Clinical Research Centre, Bamako, Mali, 4Mali Hospital, Bamako, Mali
&Corresponding author: Souleymane Togola, Public Health Teaching and Research Department, Bamako, Mali, Email: souleymanetogola2020@gmail.com ORCID: https://orcid.org/0009-0008-3948-8230
Received: 23 Apr 2025, Accepted: 06 May 2026, Published: 12 May 2026
Domain: Infectious Disaese Epidemiology
Keywords: Impact of COVID-19, measles immunization activities, Mali
©Souleymane Togola et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Souleymane Togola et al., Impact of COVID-19 pandemic on measles immunisation activities in Mali: A five-year descriptive analysis of vaccination uptake and missed opportunities. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):76. https://doi.org/10.37432/jieph-d-25-00100
Introduction: Measles is a highly contagious disease. The study demonstrated the impact of the COVID-19 pandemic on measles vaccination coverage in Mali.
Methods: This was a cross-sectional study based on a secondary analysis of the measles vaccination (EPI) database in Mali from 2019 to 2023. Sociodemographic characteristics were analysed. Frequency, mean, and logistic regression were used to analyse the results using SPSS version 25. The significance level was set at p<0.05.
Results: The vaccination coverage rate for the mobile strategy decreased more sharply from 2020 to 2021 than for the fixed and advanced strategies. The total number of vaccinated children declined between 2020 and 2021 compared to 2019. Between 2020 and 2021, during the COVID-19 pandemic, a marked increase in the number of children who missed vaccination was observed. The pandemic acted as an immediate and statistically significant exogenous shock to the vaccination system. The coefficient for the intervention variable (β2=−0.0659, p=0.0031) indicates that there was an immediate drop of 6.59 percentage points in the vaccination rate in 2020 (95% CI: −0.0819; −0.0499, p<0.05), exceeding the declining trend already observed
Conclusion: The analysis shows a drop in measles vaccination coverage at the national level between 2020 and 2021.
Measles is a viral disease caused by the measles virus [1]. It is a highly contagious, airborne disease that can lead to serious complications and even death. According to the World Health Organization (WHO), measles vaccination prevented an estimated 60 million deaths between 2000 and 2023. Nevertheless, approximately 128,000 measles-related deaths occurred worldwide, predominantly among unvaccinated or under-vaccinated children under five years of age, despite the availability of a safe and cost-effective vaccine. By 2022, around 83% of the world’s children had received a dose of measles vaccine before their first birthday through routine health services, the lowest coverage rate since 2008.
Between 2022 and 2023, a total of 144,767,764 children were vaccinated against measles in the WHO African Region across 24 countries through 32 mass vaccination campaigns [2]. In 2023, 125,957 suspected measles cases were reported through the case-based surveillance system, of which 73,625 (58%) were confirmed either by laboratory testing, epidemiological linkage, or clinical compatibility [2]. During the COVID-19 pandemic in 2020 and 2021, many countries in the African Region and globally experienced significant declines in vaccination coverage and surveillance performance.
Mali experienced its second major measles epidemic in 2001, with 4,464 reported cases, largely due to a substantial number of unvaccinated individuals vulnerable to infection. The outbreak reported at the end of 2008 persisted in areas with incomplete vaccination coverage. Between 2020 and 2021, Mali documented 3,648 suspected measles cases, with 618 confirmed [3]. Even before the COVID-19 pandemic, Mali faced a recurrent measles burden despite having a well-established Expanded Program on Immunisation (EPI) since the 1980s [4]. The disease manifested through sporadic outbreaks, notably in 2001 and 2008, underscoring the vulnerability of unvaccinated populations.
Vaccination efforts in Mali have historically relied on two main strategies: Routine vaccination (fixed and advanced). Routine immunisation is provided at Community Health Centres (CSCom) and Referral Health Centres (CSRef). Mass vaccination campaigns (mobile): Catch-up campaigns are periodically organised to reach children who have missed routine vaccinations, particularly in remote, nomadic, or hard-to-reach areas [4].
The COVID-19 pandemic represented the largest public health crisis in modern history [5]. On January 30, 2020, WHO declared COVID-19 a Public Health Emergency of International Concern [6], and on March 11, 2020, the organisation characterized the outbreak as a pandemic [2]. Unlike some countries that implemented strict nationwide lockdowns, Mali did not impose total lockdown. However, several restrictive measures were introduced from March 2020, including the suspension of gatherings of more than 50 people, a nighttime curfew (9:00 p.m. – 5:00 a.m.), and the suspension of international flights except for humanitarian operations [7].
The COVID-19 pandemic acted as an external shock that directly disrupted immunisation strategies, leading to a decline in vaccination coverage between 2020 and 2021 [8]. The implementation of restrictive health measures, the diversion of human and financial resources toward the pandemic response (including testing, public awareness of preventive measures, and COVID-19 case management), as well as fears of infection in health facilities, led many parents to avoid seeking health services. These disruptions created a large pool of unvaccinated children, thereby increasing the population’s vulnerability to measles resurgence [8].
Despite extensive epidemiological surveillance, reinforcement of the Expanded Program on Immunization (EPI), and considerable resources deployed through mass immunization campaigns led by the Ministry of Health and Social Development in collaboration with WHO, UNICEF, GAVI, and the Bill & Melinda Gates Foundation, measles transmission persists in Mali. In the context of the COVID-19 pandemic, which significantly disrupted health services, it was therefore necessary to assess its impact on measles vaccination coverage between 2019 and 2023, with the aim of informing interventions to accelerate measles elimination.
Study area
Mali is a vast country with an area of 124,123,8 km2, located in the heart of West Africa. According to the latest General Population and Housing Census of Mali (RGPH-5) in 2022, its population was estimated at 2,239,548 inhabitants. In March 2023, the Malian authorities adopted a bill on administrative divisions, leading to a territorial reorganisation. Mali now has 19 administrative regions and the district of Bamako, 156 circles, 466 districts, 819 communes, and 12,712 villages. In terms of health, the country is subdivided into 11 health regions (Kayes, Koulikoro, Sikasso, Ségou, Mopti, Gao, Timbuktu, Kidal, Menaka, Taoudeni, and Bamako) and 75 health districts.
Mali’s Expanded Program on Immunization (EPI), implemented since the 1980s, has evolved considerably in terms of the number of diseases covered, strategies, and vaccination coverage, particularly for the measles-containing vaccine (MCV), combining fixed, advanced, and mobile strategies across the country. The measles vaccine has been administered as a single dose to 9-month-old children since its introduction. A second dose (MCV2) was successfully introduced into the routine immunization schedule in October 2019, in line with WHO recommendations to enhance herd immunity. In 2024, Mali replaced the single-dose measles vaccine with the combined measles-rubella (MR) vaccine, administered in two doses to children aged 9–11 months and 15–23 months.
Mali’s health policy is based on a pyramidal structure. The first level is that of the Community Health Centers (CSCom), with decentralised governance; the second is that of the Reference Health Centers (CSRef); and the third and fourth levels are occupied by regional and national hospitals, respectively. According to the Severe Malaria Observatory, the public health sector includes: The first level was the Community Health Center (CSCom). It offers the Minimum Package of Activities (MPA), including curative, preventive, and promotional care. 1404 community health centres at the operational level. Added to this are the 1679 for-profit private health establishments. Surveillance data from CSCOM, CSREF, and private sources are directly collected by the General Directorate of Health and Public Hygiene (DGSHP), and those from hospitals are collected at the ministry’s office. The second echelon, or first reference, assumes responsibility for the reference coming from the first echelon; 65 functional reference health centres. The third level consists of Public Hospital Establishments or University Hospital Centre EPH/CHU; it has seven hospitals
Study design and study period
We conducted a cross-sectional study based on secondary analysis of the Mali Program on Immunization (EPI) against measles (VAR) database from 2019 to 2023. The study ran from 13 June 2024 to 09 October 2024.
Study population and sampling
All data from the Expanded Program on Immunization (EPI) against measles (VAR) from 2019 to 2023 obtained from the District Health Information Software 2 (DHIS2) were taken into account. All measles vaccination data (VAR) were fully recorded in DHIS2 from 2019 to 2023. Rows containing missing or atypical data for the variables of interest were excluded from the analysis. VAR cases recorded in the databases outside the study period were excluded. We used an exhaustive sampling of all VAR cases from the DHIS2 surveillance system database.
Data source and variable of interest
DHIS2 is used as the source for collecting our information. From this source, the data were extracted and saved on a USB key. The data from DHIS2 were aggregated. Dependent variable was the total vaccinated while the independent variables included gender, a dichotomous qualitative variable (male and female), vaccination status, a qualitative dichotomous variable (vaccinated, unvaccinated), residence, a multi-modal qualitative variable (Kayes, Koulikoro, Sikasso, Ségou, Mopti, Gao, Timbuktu, Kidal, Menaka, Taoudeni regions), rate of vaccination completion in fixed, advanced and mobile strategies, total vaccinated males and females, number of children who missed vaccination and impact of the pandemic.
Definitions of concepts
Suspected case: A suspected case is a person who presents clinical signs and symptoms suggestive of an illness, according to a standardized definition, but without biological confirmation yet.
Confirmed case: A confirmed case is a case whose diagnosis has been verified and validated by a laboratory examination or by epidemiological links (a case linked to a confirmed case) or by strict clinical confirmation.
The fixed vaccination strategy refers to the approach where vaccination sessions take place in a fixed health centre, on regular dates, and the beneficiaries (parents with children) travel to come and be vaccinated.
The mobile vaccination strategy is an approach where the vaccinating team travels with all the necessary equipment to remote or difficult-to-access areas, generally lacking permanent health structures.
The advanced vaccination strategy is an intermediate approach between the fixed strategy and the mobile strategy. It consists of sending a vaccination team from a health facility to a location located at a moderate distance, but accessible within one day, to bring the service closer to the population.
We considered 2019 as the pre–COVID-19 period, 2020 and 2021 as the COVID-19 pandemic period, and 2022 and 2023 as the post–COVID-19 period.
Data analysis plan
The qualitative variables were expressed in proportion with their confidence intervals, as for the quantitative ones, we calculated the means with their standard deviations. Regarding the distribution over time, we made a trend curve over the years. We did a simple logistic regression model to identify the possible explanatory variables to integrate into the multiple logistic regression model. Parameters were calculated at 95% confidence intervals. Variables with a p-value < 0.2 were considered candidates for inclusion in the multivariable models. A p-value of less than 5% (p<0.05) suggested enough evidence to conclude that a link existed. The data was processed on SPSS version 25. We used the Interrupted Time Series (ITS) analysis method to evaluate the direct impact of the pandemic on measles vaccination coverage over time using RStudio software.
To achieve this, we created three key variables: Time (to model the pre-pandemic trend), Intervention (to mark the start and duration of the pandemic), and Post-Intervention Trend (to capture the long-term change in slope following the pandemic). We then defined the Interruption variable to determine the starting year of the pandemic.
Regression analysis was employed for the core modeling, where the vaccination rate is the dependent variable, and the independent variables include time (to model the baseline trend) and indicator variables for the interruption, following the segmented regression formula:
Yt=β0+β1(Time)+β2(Intervention)+β3(Post-Intervention Trend)+εt
Ethical consideration
Permission to use the national epidemiological surveillance database of the Director General of Health and Public Hygiene (DGSHP) was requested by the Department of Public Health Studies and Research of the Faculty of Medicine of Mali as part of our master’s thesis in public health. Patient’s personal information was anonymised during data extraction and analysis to ensure confidentiality.
Analysis of the vaccination coverage database obtained from DHIS2 showed that several regions reported coverage rates exceeding 100%, notably Tombouctou (125.0%), Mopti (123.2%), Bamako (121.7%), and Koulikoro (120.2%) (Table I). Males accounted for the majority of the vaccinated population, representing 50.3%. The years 2022 and 2023 recorded the highest proportions of vaccinations, contributing 23.2% and 24.8% of all vaccinations, respectively (Table 2).
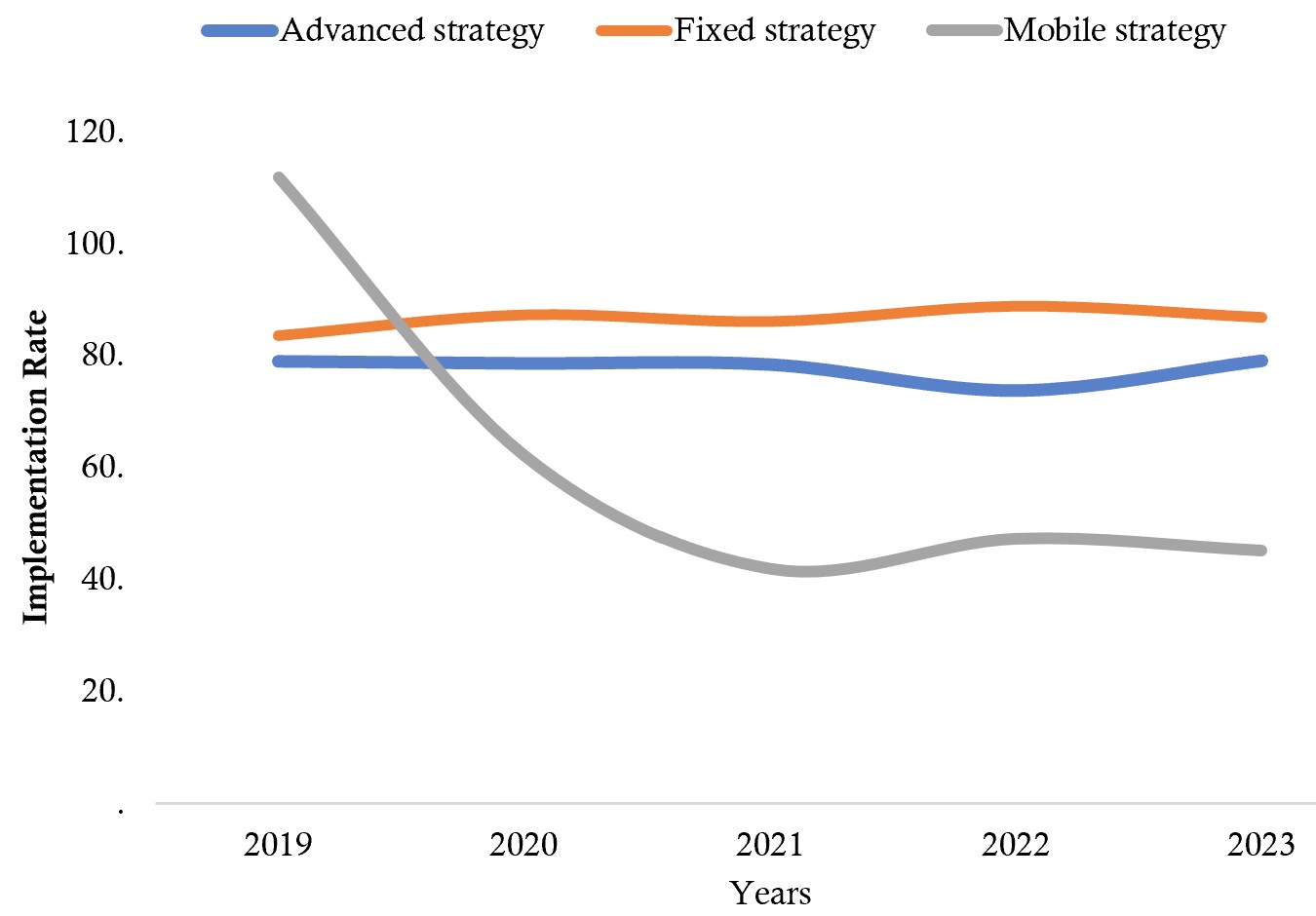
Analysis of the vaccination coverage database obtained from DHIS2 showed that all vaccination strategies experienced a decline in implementation rates between 2020 and 2021. The vaccination coverage rate for the mobile strategy showed a more pronounced decrease from 2020 to 2021 compared to the fixed and advanced strategies (Figure 1).
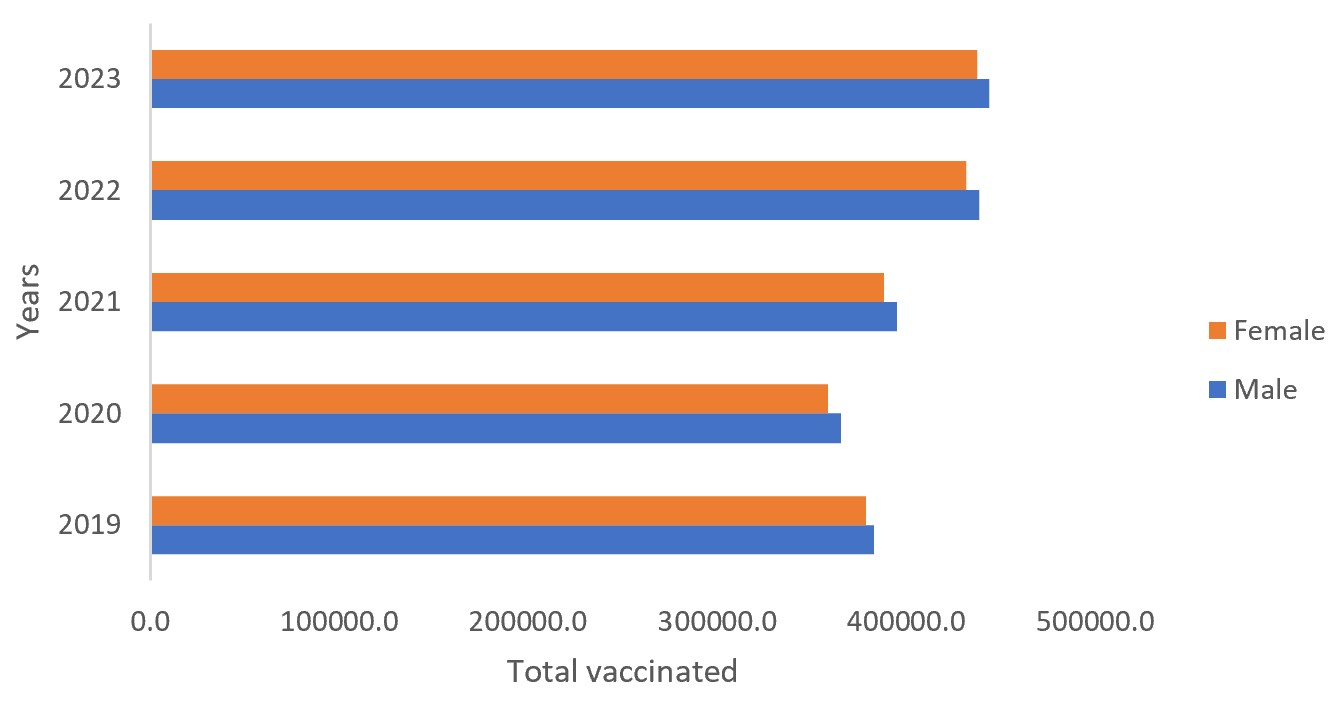
The males represented the majority of vaccinated children. The total number of vaccinated children (male and female) declined between 2020 and 2021 compared to 2019. However, an increase exceeding 2019 levels was observed in 2022 and 2023 (Figure 2).
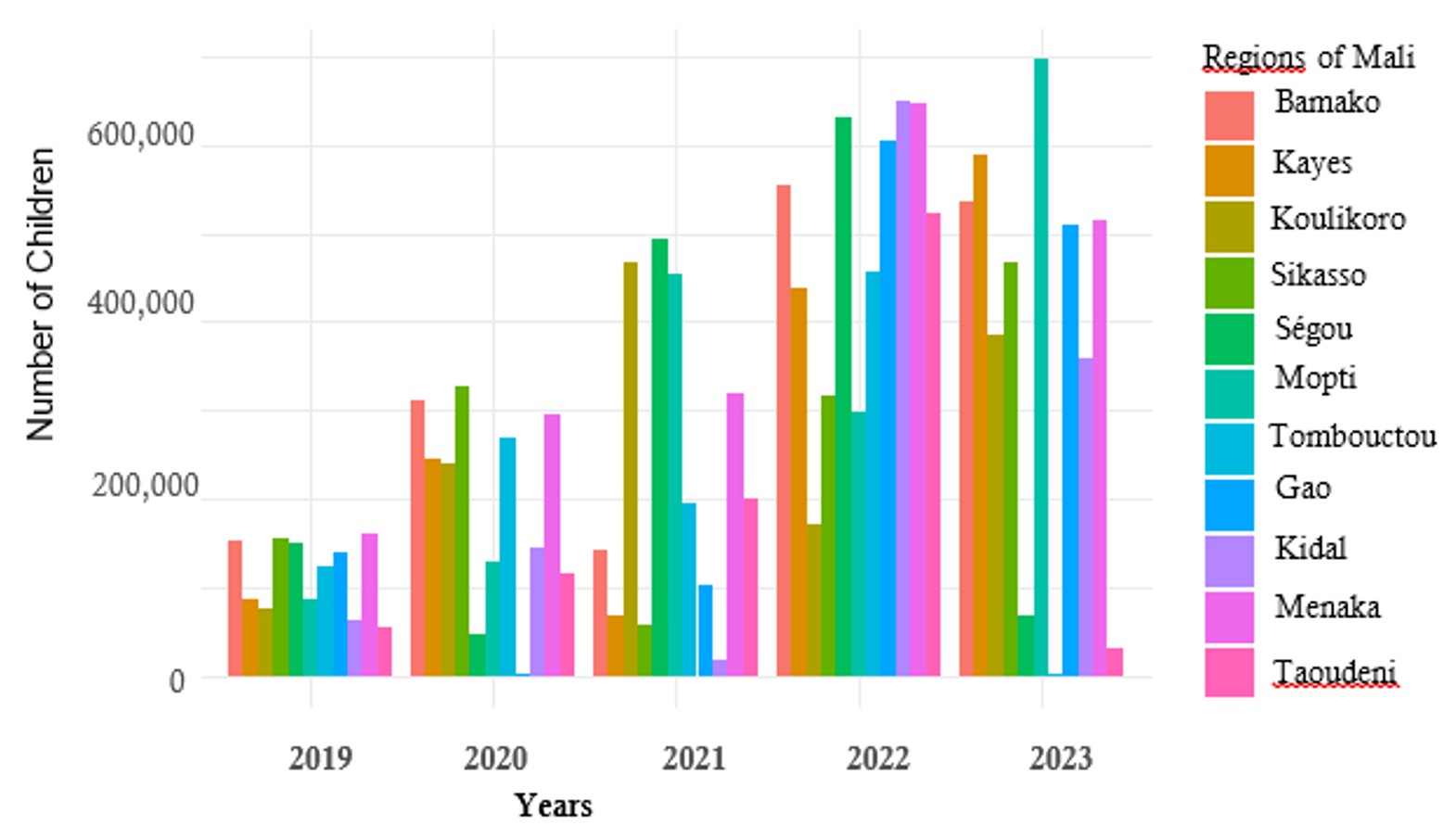
In 2019 (pre-pandemic), no region exceeded 200,000 children who missed vaccination. The Ménaka region recorded the highest number of unvaccinated children, followed by the Ségou and Koulikoro regions, and the district of Bamako.
Between 2020 and 2021, during the COVID-19 pandemic, a marked increase in the number of children who missed vaccination was observed. In 2020, the Sikasso region, the district of Bamako, and the Taoudeni region recorded the highest numbers, each reaching approximately 300,000 unvaccinated children. In 2021, the Koulikoro, Ségou, and Mopti regions reported the largest numbers, each exceeding 500,000 unvaccinated children per year.
Between 2022 and 2023 (post-pandemic), all regions experienced a substantial increase in the number of children who missed vaccination compared to the pre-pandemic and pandemic periods. In some regions, the increase exceeded 600,000 unvaccinated children (Figure 3).
Impact of the COVID-19 pandemic on vaccination programs from 2019 to 2023
Before the COVID-19 pandemic, the analysis revealed that the measles vaccination rate was already on a significant decline trajectory. The coefficient for the Time variable (β1=−0.0276, p=0.0014) indicates that the vaccination rate was decreasing by an average of 2.76 percentage points per year (95%CI: −0.0322 ;−0.0231, p<0.05) during the pre-intervention period (Table 3).
The pandemic acted as an immediate and statistically significant exogenous shock to the vaccination system. The coefficient for the Intervention variable (β2=−0.0659, p=0.0031) indicates that there was an immediate drop of 6.59 percentage points in the vaccination rate in 2020 (95%CI: −0.0819; −0.0499, p<0.05), exceeding the declining trend already observed. This result highlights an acute disruption of routine services starting in the first year of the pandemic (Table 3).
This study provides an overview of vaccination coverage across regions, highlighting substantial geographic disparities in performance relative to annual targets. Overall, the total number of vaccinated children (n = 5,218,714) exceeded the estimated annual targets (n = 4,505,901). Several regions reported coverage rates exceeding 100%, notably Tombouctou (125.0%), Mopti (123.2%), Bamako (121.7%), and Koulikoro (120.2%). Such overperformance may reflect strong immunization activities, including intensified campaigns and effective community mobilization. It may also be explained by population movements, underestimation of target populations, or inclusion of children from neighbouring areas, which are common challenges in administrative coverage estimates in low-resource settings. Conversely, regions such as Ménaka (99.0%) and Kidal (99.5%) did not reach their targets. Intermediate performance was observed in regions like Ségou (102.5%) and Taoudéni (105.1%), where coverage slightly exceeded targets. The observed heterogeneity underscores the importance of interpreting administrative coverage data with caution. Coverage above 100% does not necessarily indicate optimal performance but may instead reflect inaccuracies in denominator estimates or cross-border utilization of services. Therefore, complementing administrative data with survey-based estimates (e.g., cluster surveys) is essential for a more accurate assessment of vaccination coverage.
Regarding the temporal distribution, the years 2022 and 2023 recorded the highest proportions of vaccination, with 23.2% and 24.8%, respectively. This increase may be associated with an intensification of vaccination activities following the disruptions observed during the COVID-19 pandemic period, or with a progressive improvement in the electronic immunization management system. In our study, analysis of the vaccination coverage database obtained from DHIS2 showed all vaccination strategies suffered a drop in the completion rate from 2020 to 2021. The vaccination rate in the mobile strategy suffered a clear drop from 2020 to 2021 compared to the fixed and advanced strategy. Our result was similar to that of Amy Winter et al [9] in Zambia, who found a drop in the vaccination rate compared to before the 2020 pandemic period. In their systematic review, Alice Packham et al [10] found a disruption of vaccination programs during the COVID-19 period in low- and middle-income countries. H Attoh Touré et al [11] in their study carried out in a reference vaccination centre in Treichville in the Ivory Coast found a drop in the completion of measles vaccination by 20% compared to 2019. In contrast to our result, Kelvin Mwangilwa et al [12] found an increase in measles vaccination trends at dose 2 of approximately 0.3% during the COVID-19 pandemic due to additional vaccination activity.
In March 2020, the authorities instituted a nationwide curfew from 9:00 p.m. to 5:00 a.m., thereby restricting nighttime mobility except for essential services (medical personnel, security forces, and the transportation of goods). This measure helped reduce attendance at public places but also disrupted certain health services. In addition, some health workers and logistical resources were redirected toward the COVID-19 response, including community awareness, testing, and the implementation of preventive measures. Furthermore, fear of infection led to decreased attendance at vaccination sites in some areas. The Ministry of Health and Social Development should explicitly reposition mobile vaccination as a core pillar of immunisation delivery, rather than a complementary activity. Dedicated budget lines for mobile teams, fuel, maintenance of vehicles, and per diem support should be secured within annual EPI plans, with particular emphasis on Tombouctou, Ménaka, Taoudeni, and other high-risk regions. DHIS2 data should be systematically used to identify communes, health areas, and population groups with the highest numbers of zero-dose and under-immunised children. Mobile vaccination routes and schedules should be redesigned using these data to ensure targeted, frequent, and predictable outreach to underserved communities, rather than sporadic campaigns.
The sex ratio was 1:1, confirming parity between males and females, although the percentage shows a slight, non-significant predominance of males. This difference is explained by sociocultural and behavioural factors that influence access to vaccination, as some communities place a greater priority on male access to preventive health services. Similar studies conducted in African settings have also reported a male predominance among vaccinated children, suggesting potential gender-related disparities in the utilization of health services. This has been documented in studies by Favin et al. [13], Wiysonge et al [14], Canavan et al. [15], Antai et al. [16], and Odusanya et al. [17] conducted in Nigeria and other African contexts.
The decline in the total number of vaccinated children observed between 2020 and 2021 coincides with the COVID-19 pandemic period. This period was characterized by major disruptions to the health system, including the reallocation of human and logistical resources to the pandemic response, movement restrictions, curfews, and fear of infection within health facilities. These factors contributed to a reduction in attendance at routine immunization services as well as advanced and mobile outreach activities.
The increase observed in 2022 and 2023, exceeding 2019 levels, is consistent with the findings of Danovaro-Holliday MC et al [18], WHO reported a decline in vaccination coverage during the COVID-19 pandemic followed by catch-up efforts implemented in several countries, including those in Africa. Our results may be attributed to the catch-up interventions implemented after the progressive lifting of COVID-19–related restrictions by health authorities, as documented by the Ministry of Health and Social Development of Mali in the 2022–2023 Annual Report of the Expanded Program on Immunization (EPI). These interventions included mass vaccination campaigns and the resumption of routine immunization activities, in line with WHO’s guidance document “Maintaining essential immunization services during the COVID-19 pandemic: guidelines for the African Region” (WHO AFRO, 2021). This trend reflects the resilience of Mali’s EPI and the effectiveness of corrective strategies implemented to address immunization gaps accumulated during the pandemic.
Our analysis showed that In 2019 (pre-pandemic), none of the regions reached the threshold of 200,000 children who missed vaccination. The Ménaka region accounted for the largest number of unvaccinated children, followed by the Ségou and Koulikoro regions, and the district of Bamako. This distribution likely reflects both geographic and systemic disparities in immunization service delivery, including challenges in reaching remote or insecure areas such as Ménaka, as well as variations in population density and health service access between regions. Recruiting and training vaccinators from within local communities can improve acceptance, reduce security risks, and ensure continuity of services when external teams cannot travel. Mobile vaccination sessions should be integrated with other essential services such as nutrition screening, vitamin A supplementation, deworming, antenatal care, and health education. This integrated approach increases efficiency, community demand, and caregiver participation, while reducing missed opportunities for vaccination. In regions like Tombouctou and Ménaka, vaccination strategies must be aligned with population mobility patterns. This includes mapping transhumance routes, seasonal movements, markets, and gathering points, and scheduling mobile sessions accordingly. Cross-border coordination with neighboring countries should also be strengthened to vaccinate children moving across borders.
Between 2020 and 2021, during the COVID-19 pandemic, significant increases in the number of children who missed vaccination were observed across several regions. In 2020, the Sikasso region, the district of Bamako, and the Taoudeni region recorded the highest numbers, each reaching approximately 300,000 unvaccinated children. In 2021, the Koulikoro, Ségou, and Mopti regions reported the largest numbers, each exceeding 500,000 unvaccinated children annually. These findings reflect the substantial disruptions to routine immunization services during the pandemic period, including reduced access to health facilities, resource reallocation toward COVID-19 response, and population movement, which collectively contributed to a widening immunity gap in these regions. Our findings are consistent with those of Causey K et al [19], whose modeling analysis estimated disruptions to vaccination services worldwide, including in Africa, published in The Lancet in 2021, as well as with the work of Roberton et al [20], which demonstrated how reduced access to maternal and child health services, including vaccination, during the COVID-19 pandemic could lead to an increase in preventable mortality. It is necessary to ensure the continuity of immunization activities even during emergencies through emergency preparedness planning and decentralized service delivery, while strengthening health system readiness by maintaining essential health services during crises through adequate resource allocation, workforce protection, and flexible service delivery strategies (e.g., mobile and outreach teams). Enhancing community engagement and communication is also crucial to address fears and misinformation and to encourage caregivers to continue accessing vaccination services during emergencies. In addition, strengthening surveillance and data systems is essential to rapidly identify and respond to immunity gaps, thereby enabling timely corrective measures.
Between 2022 and 2023 (post-pandemic), all regions experienced a considerable increase in the number of children who missed vaccination compared to both the pre-pandemic and pandemic periods. In some regions, this increase exceeded 600,000 unvaccinated children. This trend may reflect the cumulative effects of service disruptions during the pandemic, which created a large cohort of susceptible children, combined with delays in implementing effective catch-up strategies. Additionally, logistical challenges, population movements, and health system recovery constraints may have further contributed to the widening immunity gap observed during this period. These findings highlight the critical need for robust post-pandemic recovery plans, including intensified catch-up campaigns, strengthened routine immunization, and targeted interventions in regions with the highest immunity gaps. The authority can revitalize mobile strategies must go hand in hand with intensified social mobilization. Community and religious leaders, women’s groups, and local radios should be actively involved to raise awareness about the importance of vaccination, counter misinformation, and encourage caregivers to bring children to mobile sessions. Mobile vaccination activities should be closely supervised, with real-time reporting through DHIS2 or simplified digital tools. Regular feedback at district and regional levels will help identify implementation gaps, ensure data quality, and rapidly adjust strategies to reduce the number of missed children
The results of the ITS model are concerning. They confirm not only a pre-existing vulnerability of the EPI (Expanded Program on Immunization), illustrated by a baseline decline of 2.76 percentage points per year, but also the sheer scale of the pandemic’s acute impact. The immediate drop of 6.59 percentage points in 2020, attributable to the shock of health measures and resource reallocation, has accelerated the accumulation of the pool of unvaccinated children, signalling an increased risk of a post-pandemic measles epidemic. Although the long-term effect (change in trend) could not be estimated by this annual model, the level change effect strongly suggests that massive catch-up efforts are immediately required to compensate for this deficit
Limitation
Our study had some limitations, such as the lack of data from certain patients, which, when they do exist, are sometimes incomplete. The underestimation of annual targets hinders the effective interpretation of some of our results. During the ITS analysis, the coefficient for Post-Intervention Trend (TendancePost) was not defined (NA) due to singularities. This indicated a problem with the model or data structure, most likely related to the small number of data points (only 5 years) and the fact that our segmented regression model was perfectly fitted to the remaining degrees of freedom. While the findings are relevant, there remains a significant disconnect between the study’s stated objectives and the results provided. Furthermore, the lack of denominator-based data limits the depth of the analysis.
The analysis reveals a decline in measles vaccination coverage at the national level between 2020 and 2021. Although the number of children vaccinated after the pandemic appears to be higher than pre-pandemic levels, there has been a simultaneous and significant increase in the number of unvaccinated children. This paradox of persistent non-vaccination despite progress is often due to a combination of factors, including supply disruptions, conflict, and instability, which must be considered in achieving measles elimination goals in Mali. while overall vaccination performance appears encouraging, significant regional disparities persist. Addressing these gaps will be critical to ensuring equitable access to immunization services and achieving national and global vaccination goals.
What is already known about the topic
What this study adds
Souleymane Togola was responsible for data collection, analysis and interpretation. Souleymane Diarra, Keita, Yaya Sarro supervised the development of the study protocol, data collection, analysis, and final report. Yaya Sarro was responsible for revising the manuscript and approving the final version for submission. The authors would like to thank all DGSHP staff and INSP serology staff for their support.
| Table I: Measles vaccination coverage by region, Mali, 2019-2023 | |||
|---|---|---|---|
| Characteristic | Frequency (n=5,218,714) | Estimation of annual targets (n=4,505,901) | Percentage (%) |
| Regions | |||
| Bamako | 840226 | 690355 | 121.7 |
| Gao | 176017 | 161034 | 109.3 |
| Kayes | 702115 | 601570 | 116.7 |
| Kidal | 19058 | 19158 | 99.5 |
| Koulikoro | 908120 | 755790 | 120.2 |
| Menaka | 25343 | 25600 | 99.0 |
| Mopti | 550487 | 446789 | 123.2 |
| Ségou | 810518 | 791023 | 102.5 |
| Sikasso | 981998 | 845000 | 116.2 |
| Taoudéni | 37484 | 35675 | 105.1 |
| Tombouctou | 167348 | 133907 | 125.0 |
| Table 2: Measles coverage by year and sex in Mali, 2019-2023 | ||
|---|---|---|
| Characteristic | Frequency (n=5,218,714) | Percentage (%) |
| Years | ||
| 2019 | 768378 | 14.7 |
| 2020 | 906762 | 17.3 |
| 2021 | 1035236 | 19.8 |
| 2022 | 1212279 | 23.22 |
| 2023 | 1296059 | 24.8 |
| Sex | ||
| Male | 2624940 | 50.29 |
| Female | 2581787 | 49.47 |
| Table 3: Impact of the pandemic on vaccination programs from 2019 to 2023 | ||||
|---|---|---|---|---|
| Periods | Percentage points by year | Coefficient for the variable | IC 95% | p-value |
| Pre-pandemic | 2.76 | β1 = -0.0276 | -0.0322 ; -0.0231 | 0.0014 |
| During pandemic | 6.59 | β2 = -0.0659 | -0.0819 ; -0.0499 | 0.0031 |
| Post-pandemic | NA | NA | NA | |
| NA: Not Available | ||||