Research | Open Access | Volume 9 (1): Article 32 | Published: 20 Feb 2026
Views: 2,720
Menu, Tables and Figures
| Characteristics | Frequency | Proportion (%) |
|---|---|---|
| Age Group | ||
| 0-<2 | 78 | 2.7 |
| 2-<5 | 118 | 4.0 |
| 5-<19 | 463 | 15.7 |
| 19-<45 | 1681 | 57.0 |
| ≥45 | 608 | 20.6 |
| No age specified | 44 | 1.5 |
| Gender | ||
| Male | 1884 | 63.0 |
| Female | 1108 | 37.0 |
| District | ||
| Ilala | 1578 | 52.7 |
| Kinondoni | 912 | 30.5 |
| Kigamboni | 284 | 9.5 |
| Temeke | 218 | 7.3 |
| Months 2023 | ||
| January | 401 | 13.4 |
| February | 344 | 11.5 |
| March | 332 | 11.1 |
| April | 400 | 13.4 |
| May | 871 | 29.1 |
| June | 644 | 21.5 |
| t-Test: Paired Two Sample for Means | Year 2021 | Year 2022 | Year 2022 | Year 2023 | Year 2021 | Year 2023 |
|---|---|---|---|---|---|---|
| Mean | 1165 | 861 | 861 | 1285.5 | 1165 | 1285.5 |
| Variance | 17296 | 13980.8 | 13980.8 | 826063.1 | 17296 | 826063.1 |
| 95% CI for the mean | (1161.92, 1168.08) | (857.78, 864.22) | (857.78, 864.22) | (1265.21, 1305.79) | (1161.92, 1168.08) | (1265.21, 1305.79) |
| Observations | 6 | 6 | 6 | 6 | 6 | 6 |
| P(T≤t) two-tail | 0.005 | 0.265 | 0.751 | |||
Table 2: Student t-test comparison of malaria cases in 2021 to 2023
Peter Richard Torokaa1,2,&, Jasper Kimambo1,2, Mariam Mbwana1,2, Mariam Monah1,2, Sephord Ntibabara1,2, Nemes Josephat1,2, Khalifa Munisi3, Sijenunu Aaron3, Ford Chisongela4, Ally Adinani Omary5, Ally Hussein2
&Corresponding author: Peter Richard Torokaa, Muhimbili University of Health and Allied Sciences, School of Public Health and Social Sciences (MUHAS, SPHSS), Dar es Salaam, Tanzania, Email: petertorokaa@gmail.com ORCID: https://orcid.org/0009-0003-3843-3434
Received: 01 May 2025, Accepted: 19 Feb 2026, Published: 20 Feb 2026
Domain: Field Epidemiology, Outbreak Investigation
Keywords: Malaria, outbreak investigation, Dar es Salaam, Tanzania
©Peter Richard Torokaa et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Peter Richard Torokaa et al. Seasonal patterns in malaria cases: An outbreak investigation in Dar es Salaam, Tanzania, 2023. Journal of Interventional Epidemiology and Public Health. 2026; 9(1):32. https://doi.org/10.37432/jieph-d-25-00109
Introduction: Malaria is endemic and causes considerable morbidity and mortality in Mainland Tanzania. Circulating rumours on social media about an unusual rise in malaria cases in the Dar es Salaam region from April to June 2023 activated this investigation. The aim of this investigation was to ascertain whether the reported increase in malaria cases was an outbreak.
Methods: The retrospective cross-sectional study was conducted in all five Councils of the Dar es Salaam region. We reviewed outpatient department (OPD) and malaria testing results using data from the District Health Information System (DHIS2) from January to June 2021 to 2023 to identify patterns and trends. Furthermore, laboratory-confirmed malaria cases from the registers for the months of January to June 2023 were line-listed and analysed. The malaria positivity rates were calculated by dividing the number of positive mRDT tests by the total number of tests conducted. The cumulative sum (CUSUM) method and paired t-test were used to establish an outbreak.
Results: A total of 2992 confirmed malaria cases from January to June 2023 were investigated. Majority 1884 (63%) were male, from the Dar es Salaam City Council, formerly named Ilala, 1441 (48%), aged 19-45 years, 1681 (57%). Data from DHIS2 revealed an increase of outpatients’ department (OPD) and inpatient department (IPD) confirmed malaria cases in May and June 2023. We found that there was a significant decrease in the mean of malaria cases by year 2021(1165, 95%CI:1161.92 – 1168.08) as compared to year 2022 (861,95%CI: 857.78, 864.22, p<0.05). The threshold was calculated by using the CUSUM method, which shows that from 1st January to 23rd June 2023, there were increase in malaria confirmed cases. A high peak was noted at month of May 2023, week 17.
Conclusion: Findings suggest a seasonal increase of malaria cases in May-June 2023 rather than a true outbreak. Strengthened surveillance and continuous monitoring are recommended to ensure early detection and effective response to potential future outbreaks.
Malaria remains one of the most significant global public health challenges, affecting low and middle-income countries, particularly in sub-Saharan Africa [1]. According to the World Health Organization (WHO), there were an estimated 249 million malaria cases reported globally in 2022 across 85 malaria-endemic countries. The incidence rate was calculated at 58 cases per 1,000 people at risk, leading to approximately 608,000 deaths [2]. The geographical distribution of malaria burden is heavily skewed with approximately 70% of global malaria cases occurring in eleven countries: Nigeria (27%), the Democratic Republic of the Congo (12%), Uganda (5%), Burkina Faso (4%), Mozambique (4%), Cameroon (3%), Ghana (3%), Mali (3%), Niger (3%), Tanzania (3%) and India (1.5%) [2]. This highlights the critical need for localised strategies to combat the disease while addressing systemic gaps in prevention and treatment efforts [1].
Among the affected populations, the mortality rate reached 14.3 deaths per 100,000 people at risk, with four countries accounting for over half of all malaria-related deaths in 2022. Nigeria had the largest mortality rate (31%), followed by the Democratic Republic of the Congo (12%), Niger (6%) and Tanzania (4%) [2]. This impact underscores the devastating impact of the disease on vulnerable communities in poor countries [1], calling for increasing investments and targeted interventions in these high-burden areas to reduce suffering and mortality rates [1,3].
There are an estimated 7.7 million confirmed and clinical cases of malaria each year in Mainland Tanzania, where malaria accounts for more than 26% of all outpatient visits signifying its vast influence on healthcare utilization [4]. Despite concerted efforts to reduce malaria incidence and mortality, factors such as climate variability, socio-economic disparities and inadequate access to healthcare contribute to persistent challenges [5].
Recently, Dar es Salaam region has seen fluctuations in malaria transmission due to diverse environmental factors and rapid urbanization. In early June 2023, social media platforms were flooded with rumours regarding a spike in malaria cases and severe manifestations of the disease in Dar es Salaam. These reports created widespread concern among residents and healthcare providers alike, prompting the National Malaria Control Program (NMCP) to deploy six Tanzania Field Epidemiology and Laboratory Training Program (TFELTP) residents to conduct a comprehensive investigation into rumours. The TFELTP is a vital tool for enhancing global health security and enhancing outbreak response capabilities in Tanzania. The primary objective of this investigation was to verify the validity of these claims and assess the presence of a malaria outbreak in Dar es Salaam. This investigation serves as an essential tool for guiding public health decision-making and implementing evidence-based strategies for malaria control and prevention.
Study design and setting
This investigation employed a retrospective cross-sectional study design for the period of January to June each year from 2021 to 2023 at Dar es Salaam region. The investigation was conducted across five councils in Dar es Salaam Ubungo Municipal Council (MC), Temeke MC, Kinondoni MC, Kigamboni Municipal Council and Dar es Salaam City Council, where an increase in malaria cases had been claimed. Although initially planned for all five councils, data collection at the facility level for Ubungo Municipal Council could not be carried out due to limited time constraints. A total of 13 high-volume public and private health facilities within the remaining councils were purposefully selected for the investigation. These facilities are: Mwananyamala Regional Referral Hospital (RRH), Amana RRH, Temeke RRH, Sinza Palestina Hospital, Lugalo Zonal Referral Hospital, Rabininsia Hospital, Agha Khan Hospital, Shree Hindu Mandal Hospital, Regency Medical Center, Hubert Kairuki Memorial Hospital, Saifee Hospital, IST Clinic, and Vijibweni Hospital.
Study participants and sample size
The study was conducted among all adults and children with malaria symptoms residing in Dar es Salaam. Sample size included all malaria cases collected from selected health facilities. A total of 2,992 confirmed malaria cases were line listed from January-June, 2023 were investigated.
Inclusion and exclusion criteria
We included all confirmed malaria cases recorded between January and June for the year 2023, DHIS2 monthly summary records from all Dar es Salaam councils for the years 2021 to 2023, for comparison between years. We excluded suspected malaria cases without laboratory confirmation and duplicate entries or incomplete records lacking key variables (e.g., date of onset, test result, residence).
Variables
Variables included in this investigation were date of onset, date seen at the facility, age, sex, residence, malaria test results, health facility name and council names.
Data collection
Data were collected from health facility information systems from January to May 2023 and the District Health Information System 2 (DHIS2) from January to June for the years 2021 to 2023. This included data related to malaria testing, outpatient and inpatient department records and laboratory results records. These data sources were systematically reviewed to ensure comprehensive representation of the malaria cases.
The study involved a thorough review of malaria-related data recorded at health facilities, including outpatient department (OPD) malaria registers, laboratory testing registers and monthly summary forms. Data were extracted from the DHIS2 and facility-level records to analyse seasonality patterns, trends and case counts during the period from January to June for the years 2021 to 2023.
Data analysis
The collected data were analysed using Epi Info 7.2.5.0 version. Descriptive statistics, such as frequencies, proportions and measures of central tendency, were calculated to summarise the data. Temporal trends in malaria cases and positivity rates were assessed. The confirmed cases threshold was calculated from the line list from January to June 2023 on a daily basis to investigate the possibility of an outbreak. We used the CUSUM method to establish the malaria threshold based on all the data points per month per district, and the 3rd quantile was used as the limit of malaria outbreak measure. Additionally, a paired t-test was conducted to compare monthly malaria case counts across matched time periods (January–June) between consecutive years 2021 to 2023 to establish the malaria outbreak. The corresponding 95% confidence interval for the mean was reported for the year compared from 2021 to 2023. Seasonality analysis was conducted by comparing malaria data from January to June between the previous year historical data and the current year (2023), using monthly case counts from DHIS2 for each council in the Dar es Salaam region.
Ethical considerations
The outbreak investigation was conducted as part of an outbreak response, which is one of the mandates of the Ministry of Health and did not require a formal review by Ethical Review Committees. Confidentiality of all the malaria cases was assured and maintained during and after the study. We anonymised the data before it was analysed to ensure patient confidentiality.
Demographic characteristics of study participants
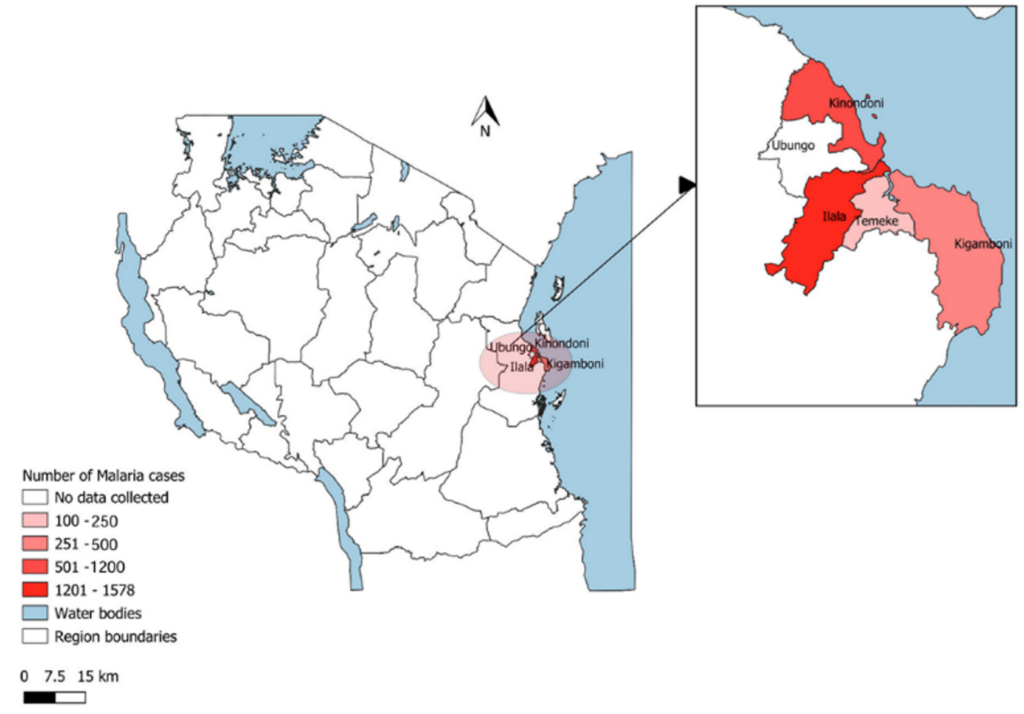
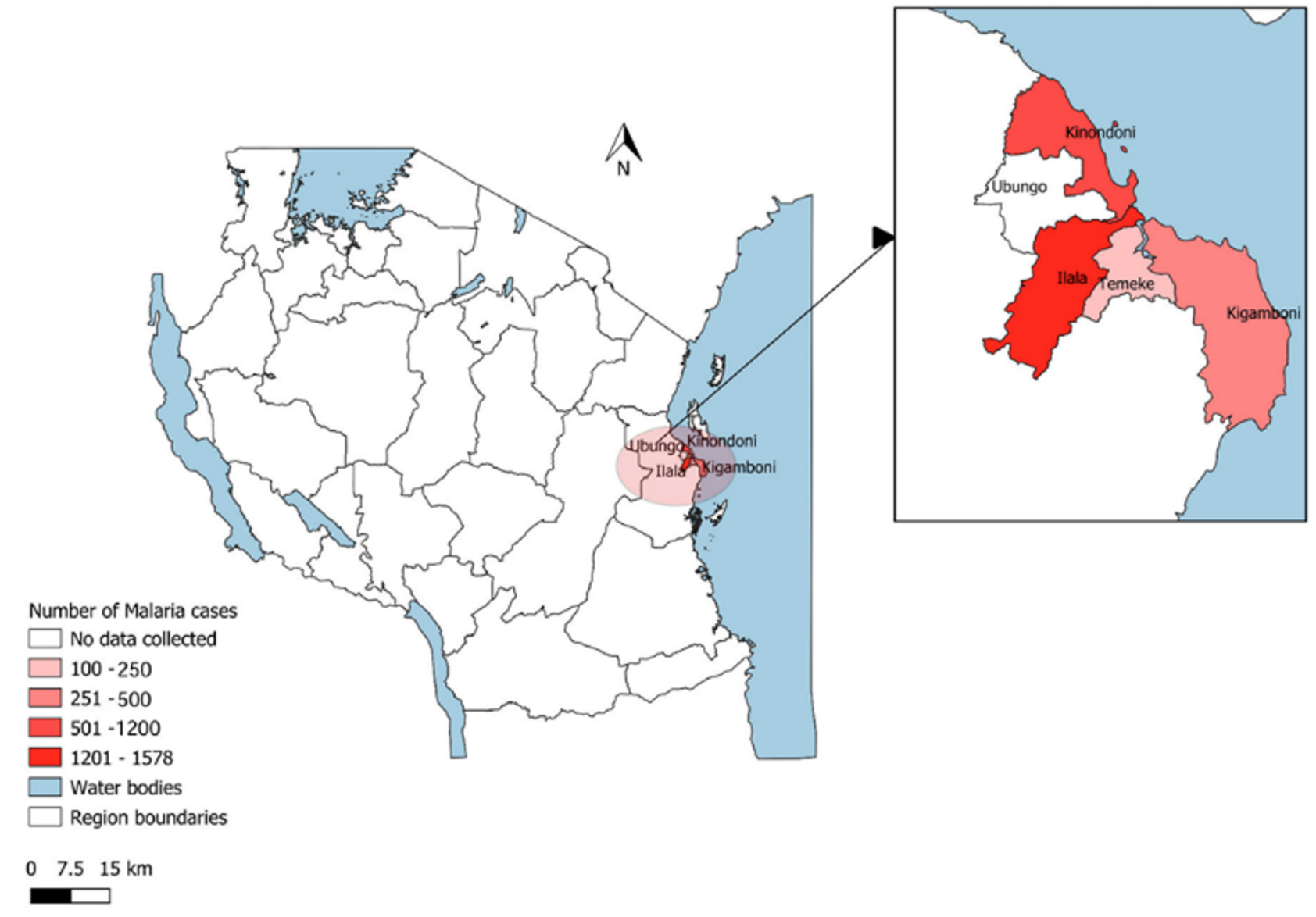
A total of 2992 cases were reported from the laboratory registers for malaria-confirmed cases from the visited facilities. The largest number of cases were from the age group of 19-<45 years, 1681 (57.02%). The Month of May had the highest number of Malaria confirmed cases of 871 (29.11%) (Table 1). Majority of cases were males, 1884 (63.0%), from Dar es Salaam City Council, 1578 (52.7%) and Kinondoni Municipal Council, 912 (30.5%) (Figure 1 and Table 1).
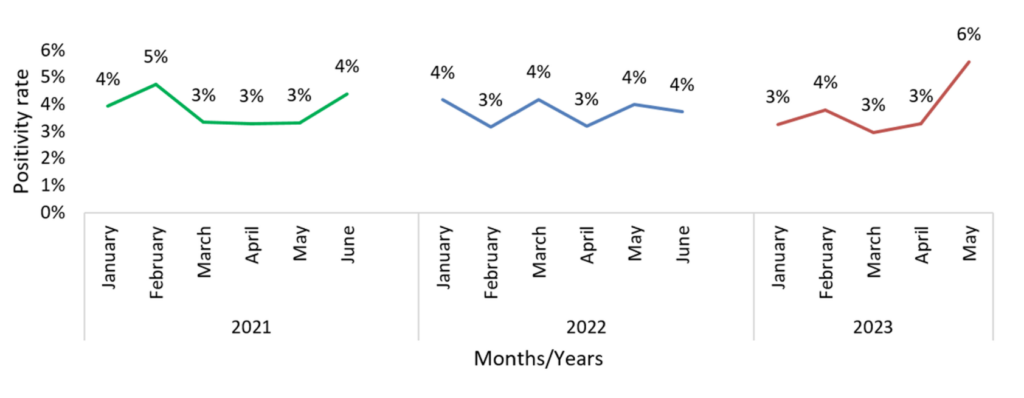
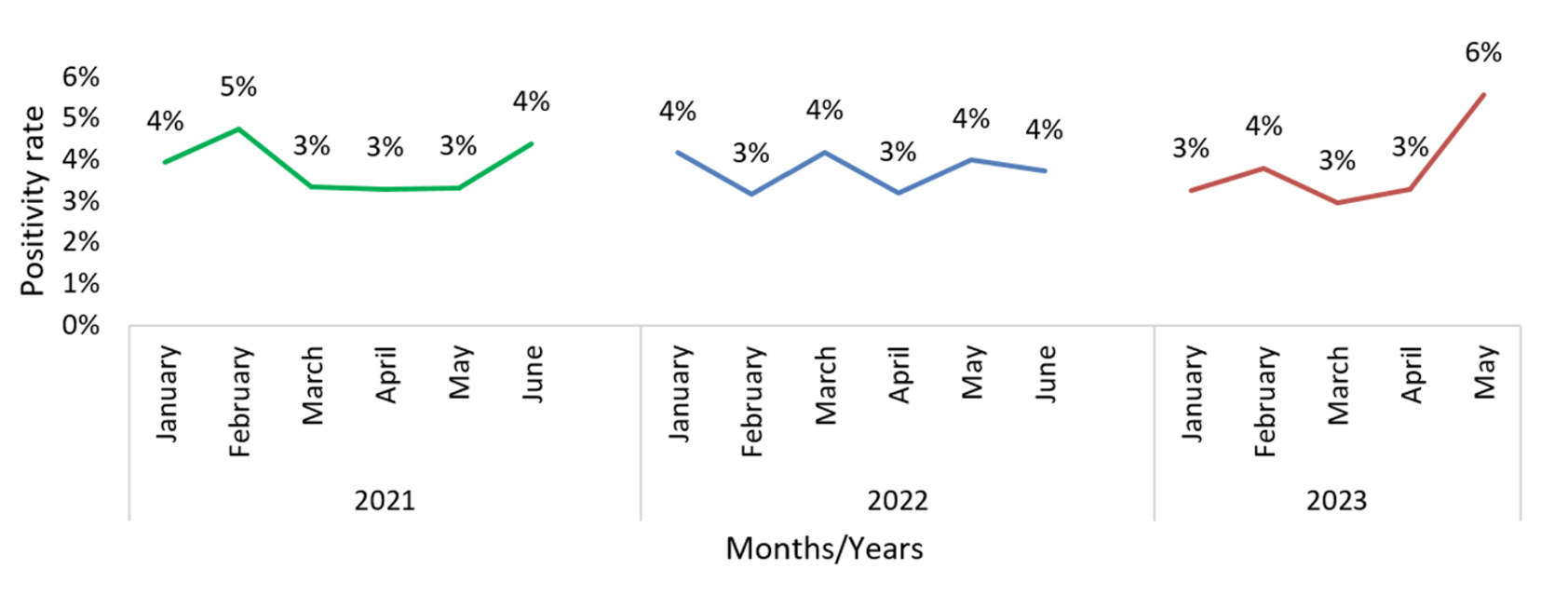
Laboratory positivity rate
The malaria positivity rate revealed a trend of increasing of malaria positive samples at the laboratory from January to June 2021 to 2023. The rise in laboratory positivity rates was similar to the increase in OPD-confirmed cases observed from January to June 2023 compared to the same period in previous years. In May 2023, the positivity rate reached almost 6% of all the cases investigated in that month (Figure 2).
Trend of malaria cases from January to June 2023 in Dar es Salaam
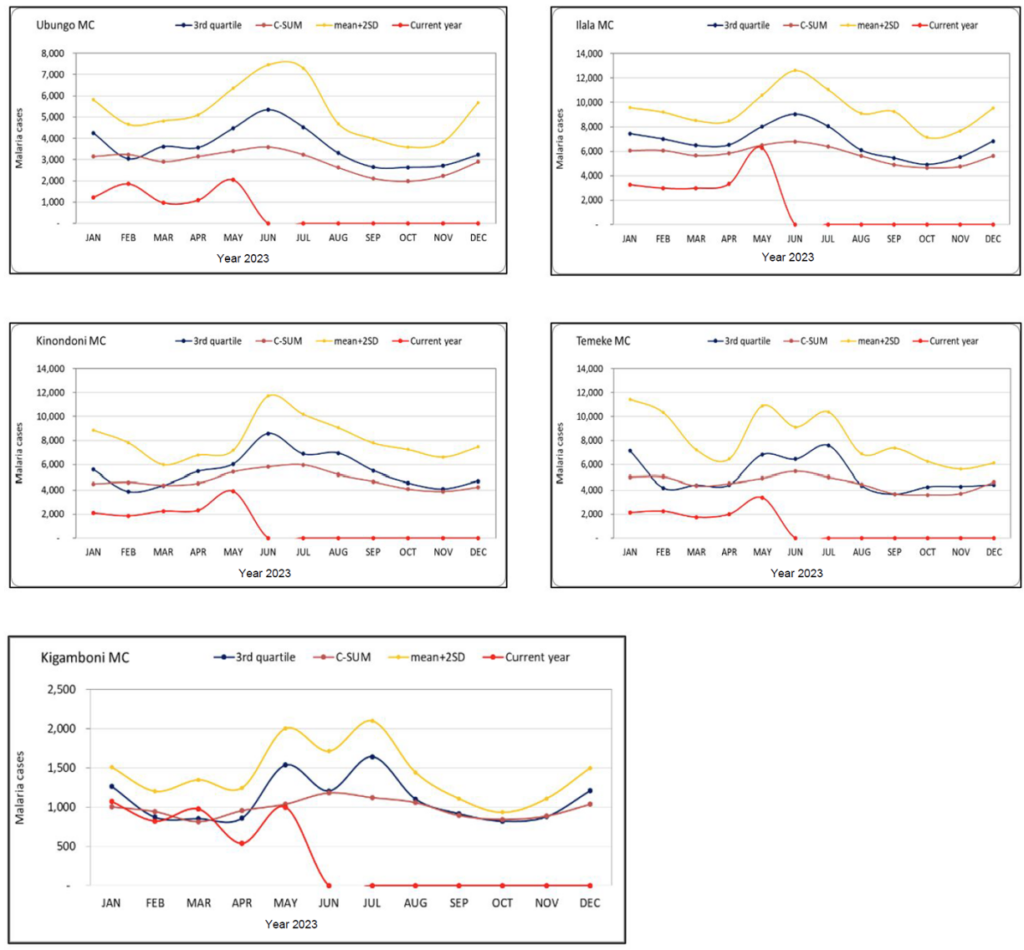
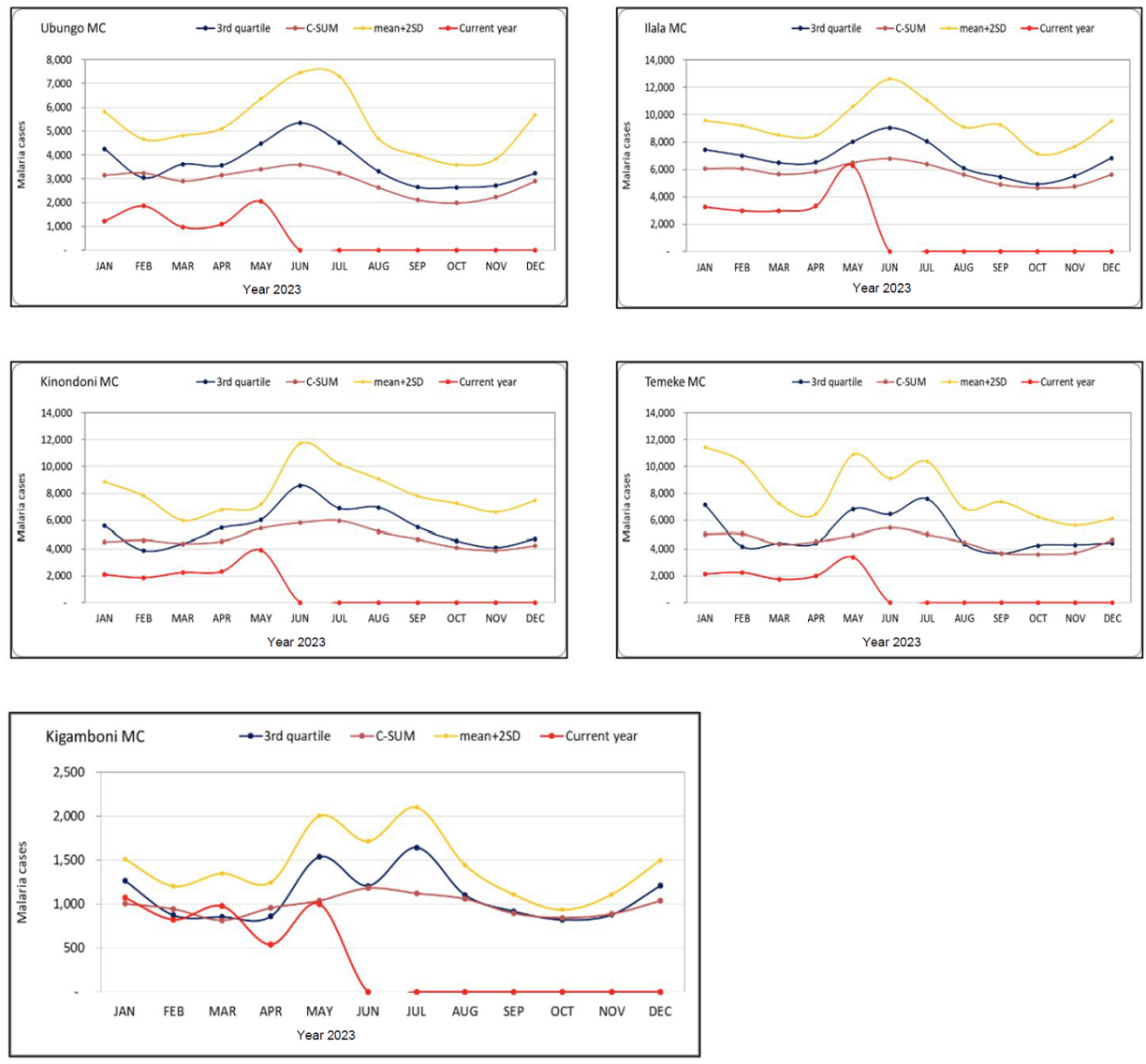
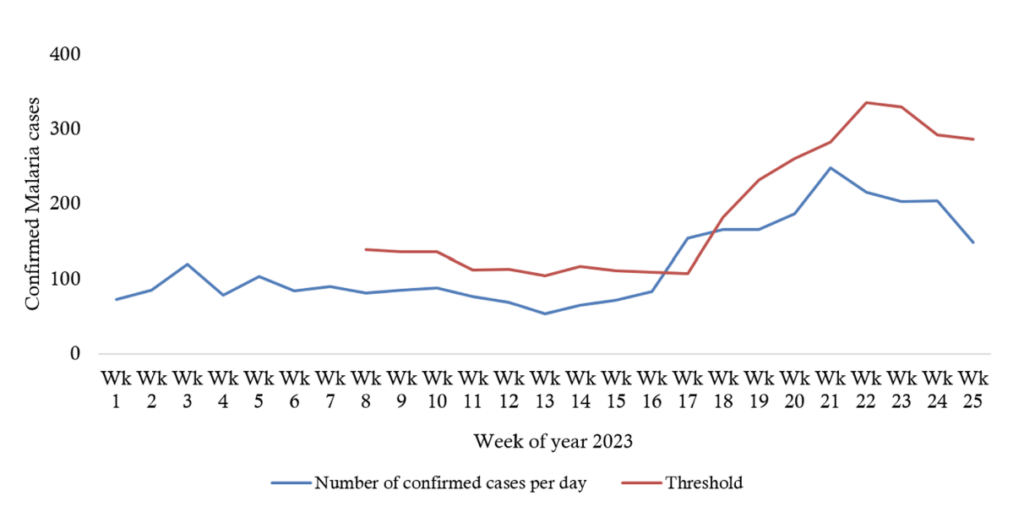
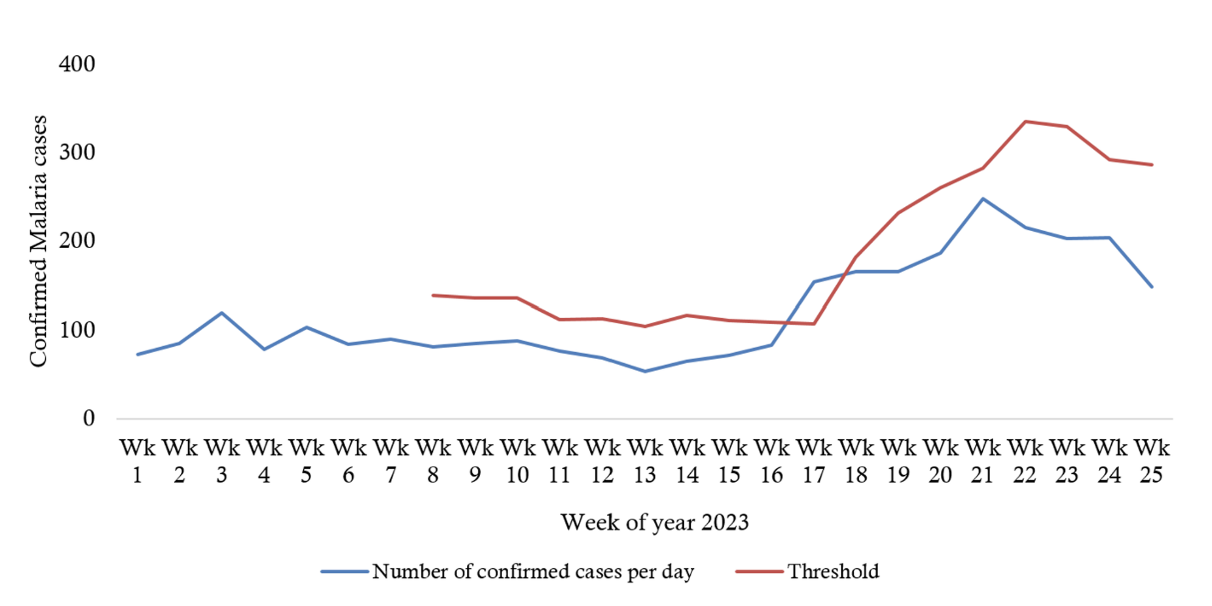
Analysis of confirmed OPD malaria cases data extracted from DHIS2 shows that the number of malaria cases in all councils of Dar es Salaam for the period of January to May 2023 is below the thresholds that indicate no outbreak of Malaria in Dar es Salaam (Figure 3). The seasonality analysis was conducted by comparing data collected between January and June from the previous year historical data and the current year (2023). The findings revealed an increase in malaria cases during May and June, as indicated by observations at the cumulative sum of malaria outbreak thresholds which was below the 3rd quantile outbreak limit (Figure 3). The threshold was calculated by using CUSUM method shows that from 1st January to 23rd June 2023 there were increase of malaria confirmed cases. A high peak noted at month of May 2023. Furthermore, it was noted that there was high peak above the threshold of malaria cases noted at 17th week of year 2023 (Figure 4).
Comparison of malaria cases in January to June 2021 to 2023
The t-test showed a significant decrease by year 2021 as compared to year 2022 in the mean of malaria cases from (1165, 95%CI:1161.92, 1168.08) to (861,95%CI: 857.78, 864.22) cases, p<0.05 respectively. No significant increase in malaria cases in comparison of year 2022 and 2023 (Table 2).
According to our findings, there was a rise in confirmed malaria cases from January to June 2023, with a high peak recorded at 17th week of 2023. Males and younger adults accounted for majority of cases. Laboratory positivity rates showed an upward trend, reaching 6% in May 2023. Despite higher cases in May 2023 compared to previous years, t-test statistical analysis did not confirm an outbreak. Increase of malaria clinical cases were noted during specific months.
The peak malaria transmission observed in May 2023 strongly correlates with seasonal rainfall patterns and massive construction activities in Dar es Salaam that increased mosquito breeding sites. Similar finding observed in a study conducted in nine African countries revealed seasonal fluctuation of Malaria cases [11]. Higher rainfall creates breeding conditions for Anopheles mosquitoes by increasing stagnant water pools. Interestingly, additional peaks in number of clinical cases were observed at the end of January, early and late April and late May. These findings differ from a previous study conducted in Morogoro region, which reported malaria case peaks in April and July [12]. These differences may be due to the fact that Morogoro and Dar es Salaam experience the rainy season differently. Historical malaria trends in Dar es Salaam from January to June 2021–2023 further support the seasonality of infections. Comparing these data with previous years suggests fluctuating epidemic risks, though overall case counts remained below the defined epidemic threshold. The malaria trends in Dar es Salaam appear consistent with findings in Kenya, where seasonal transmission intensifies from April to June, corresponding with rainfall peaks [13].
We noted that laboratory-confirmed malaria positivity rates steadily increased from January to June 2023, reaching approximately 6% in May 2023. The alignment between laboratory trends and outpatient confirmed cases suggests strong consistency in diagnostic detection. We found a significant decrease in malaria cases between 2021 and 2022. However, no significant differences were observed between 2021 and 2023 or between 2022 and 2023. This suggests intermittent progress in malaria control efforts, but not substantial long-term reductions. However, the resurgence of cases in 2023 implies challenges in maintaining long-term malaria reduction strategies. A broader comparison with malaria trends in Uganda and Rwanda suggests a similar pattern where short-term reductions are followed by periodic transmission spikes [14,15]. This reinforces the necessity for sustained malaria intervention strategies beyond seasonal control efforts.
This investigation had several limitations including, the use of previously recorded malaria data, limiting control over data completeness and quality. Incompleteness in DHIS2 and missing standardized line list data may affect the data accuracy. The seasonal variations may introduce bias in trend interpretation. Additionally, dependence on DHIS2 records and laboratory registers means cases outside formal health systems may be missed. The strength of this study including public and private facilities enhances representation of malaria burden.
This study found an increase in malaria cases, peaking on 17th week of 2023. Men and young adults bore a higher malaria burden. Laboratory positivity rates closely mirrored the rise in OPD confirmed cases. Although seasonal spikes were observed, the findings did not confirm the occurrence of an outbreak. Missing standardized line lists and seasonal variability may have introduced bias in trend interpretation, and cases outside formal health systems may have been underrepresented. The study underscores the need for improved malaria surveillance. Targeted prevention efforts, aligned with seasonal transmission trends, could further enhance malaria control in the region.
Recommendations
We recommend that NMCP strengthen malaria surveillance to improve data completeness, enhance outbreak detection and support targeted prevention efforts based on seasonal transmission trends.
What is already known about the topic
What this study adds
| Characteristics | Frequency | Proportion (%) |
|---|---|---|
| Age Group | ||
| 0-<2 | 78 | 2.7 |
| 2-<5 | 118 | 4.0 |
| 5-<19 | 463 | 15.7 |
| 19-<45 | 1681 | 57.0 |
| ≥45 | 608 | 20.6 |
| No age specified | 44 | 1.5 |
| Gender | ||
| Male | 1884 | 63.0 |
| Female | 1108 | 37.0 |
| District | ||
| Ilala | 1578 | 52.7 |
| Kinondoni | 912 | 30.5 |
| Kigamboni | 284 | 9.5 |
| Temeke | 218 | 7.3 |
| Months 2023 | ||
| January | 401 | 13.4 |
| February | 344 | 11.5 |
| March | 332 | 11.1 |
| April | 400 | 13.4 |
| May | 871 | 29.1 |
| June | 644 | 21.5 |
| t-Test: Paired Two Sample for Means | Year 2021 | Year 2022 | Year 2022 | Year 2023 | Year 2021 | Year 2023 |
|---|---|---|---|---|---|---|
| Mean | 1165 | 861 | 861 | 1285.5 | 1165 | 1285.5 |
| Variance | 17296 | 13980.8 | 13980.8 | 826063.1 | 17296 | 826063.1 |
| 95% CI for the mean | (1161.92, 1168.08) | (857.78, 864.22) | (857.78, 864.22) | (1265.21, 1305.79) | (1161.92, 1168.08) | (1265.21, 1305.79) |
| Observations | 6 | 6 | 6 | 6 | 6 | 6 |
| P(T≤t) two-tail | 0.005 | 0.265 | 0.751 | |||