Research | Open Access | Volume 9 (1): Article 42 | Published: 10 Mar 2026
Views: 29
Menu, Tables and Figures
| Health Facility | Young Adult (15-49 years) | Elderly (50 years and above) |
|---|---|---|
| Sunyani Municipal Hospital | 345 | 1078 |
| SDA Hospital | 398 | 769 |
| Bono Regional Hospital | 777 | 1191 |
| Total | 1,520 | 3,038 |
| Youth | Elderly | ||||
|---|---|---|---|---|---|
| Participant | Gender | Education Level | Participant | Gender | Education Level |
| 1 | A young male | Senior High School (SHS) or Equivalent | 15 | An elderly female | Primary School |
| 2 | A young male | Junior High School (JHS) or Equivalent | 16 | An elderly male | Postgraduate Degree |
| 3 | A young female | Primary School | 17 | An elderly male | Primary School |
| 4 | A young female | First Degree | 18 | An elderly male | Primary School |
| 5 | A young female | First Degree | 19 | An elderly female | Primary School |
| 6 | A young female | SHS or Equivalent | 20 | An elderly female | Primary School |
| 7 | A young female | First Degree | 21 | An elderly male | Junior High School (JHS) or Equivalent |
| 8 | A young male | No Educational Background | 22 | An elderly female | No Educational Background |
| 9 | A young female | SHS or Equivalent | 23 | An elderly male | No Educational Background |
| 10 | A young male | No Educational Background | 24 | An elderly female | Primary School |
| 11 | A young female | SHS or Equivalent | 25 | An elderly female | Primary School |
| 12 | A young female | First Degree | 26 | An elderly male | Postgraduate Degree |
| 13 | A young male | SHS or Equivalent | 27 | An elderly male | Primary School |
| 14 | A young female | SHS or Equivalent | 28 | An elderly male | Primary School |
Table 2: Demographic Characteristics of Participants Both the Youth and the Elderly
| Emerging Themes | Subthemes |
|---|---|
| Beliefs about the importance of hypertensive medication | Perceived Importance of Medication Adherence |
| Acknowledgment of Benefits Over Side Effects | |
| Impact of Health Education | |
| Trust in Healthcare Providers | |
| Effectiveness of hypertensive medication | Confidence in Medication’s Effectiveness |
| Belief in Reduced Risk of Complication | |
| Challenges of Adherence Despite Confidence | |
| Motivation to take hypertensive medication | Desire for a Long and Healthy Life |
| Influence of Family and Social Responsibility | |
| Education and Observational Learning | |
| Spiritual Beliefs and Personal Determination | |
| Support systems | Personal Responsibility in Health Management |
| Family and Social Support | |
| Spiritual and Self-Reliance | |
| Awareness of Consequences | |
| Alternative medication | Reliance on Medical Education |
| Trust in Hospital-Based Medication | |
| Skepticism About Alternative Medicine | |
| Potential Future Consideration of Alternative Medicine |
Ernest Osei1,&, Magdalene Afua Asiateba2
1Department of Public Health Education, Faculty of Environment and Health Education, Akenten Appiah-Menka University of Skills Training and Entrepreneurial Development, Asante Mampong, Ghana, 2Department of Public Health, School of Public Health and Allied Sciences, Catholic University of Ghana, Sunyani, Ghana
&Corresponding author: Ernest Osei, Department of Public Health Education, Faculty of Environment and Health Education, Akenten Appiah-Menka University of Skills Training, and Entrepreneurial Development, Asante Mampong, Ghana, Email: ernestosei56@gmail.com, eosei@ammusted.edu.gh ORCID: https://orcid.org/0000-0002-8536-545X
Received: 29 May 2025, Accepted: 07 Mar 2026, Published: 10 Mar 2026
Domain: Non-communicable Disease Epidemiology
Keywords: Hypertension, Medication Adherence, Perception, Elderly, Youth
©Ernest Osei et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Ernest Osei et al., Perceptions on medication adherence among the elderly and the youth with hypertension in the Sunyani municipality, Ghana. Journal of Interventional Epidemiology and Public Health. 2026; 9(1):42. https://doi.org/10.37432/jieph-d-25-00131
Introduction: Hypertension is considered to be a global health problem affecting people of all age groups. Hypertension medication adherence is a major burden in the Sunyani Municipality. The study examined the perceptions of the youth and the elderly regarding hypertensive drug adherence.
Method: The researchers conducted in-depth interviews among the elderly and the youth diagnosed with hypertension on medication adherence. A purposive sampling approach was used to select both the elderly and the youth diagnosed with hypertension. The researchers then conducted 28 in-depth interviews comprising 14 youth and 14 elderly who have been diagnosed with hypertension on medication adherence. The data were transcribed, coded, arranged, and analysed to determine categories and themes.
Results: The study indicated that both the young and elderly respondents regarded the main motives for medication adherence are to control hypertension and avoiding complications. Also, the most critical elements in adherence to medication concern trust in health care providers, family support, and positive consideration of the health benefits of the medicine, including stability of symptoms of hypertension and blood pressure. While both age groups valued the education support from health care providers, some youths preferred that this support be complemented with other online resources.
Conclusion: Although hypertensive youth and elderly patients from Sunyani recognised the importance of adherence, both groups were adherent. Identification of age-specific adherence barriers and supportive relationships may strengthen adherence, especially among younger patients. There is a great likelihood that benefits arising from tailored interventions on adherence may improve long-term health outcomes across age groups.
Hypertension is considered to be a global health problem affecting people in all age groups. It’s also one of the highest risk factors for cardiovascular diseases, stroke, and renal failure [1]. The prevalence of hypertension is increasing globally, and it is estimated that one billion people worldwide have hypertension [2, 3]. Global number increases daily: 20% of adults >25 years are hypertensive. Over 1.56 billion people will be hypertensive by the end of 2025. Hypertension is one of the leading causes of death in adults in Sub-Saharan Africa. Ghana’s estimates account for about a tenfold increase in the number of persons reporting to hospitals with hypertension between 1988 and 2007. In Ghana, the prevalence of hypertension is estimated to be 255, and it is one of the leading causes of morbidity and mortality [4].
Poor medication adherence is a common problem in both the elderly and youth with hypertension, leading to poor health outcomes, increased healthcare costs, and a reduction in quality of life [5]. The rates of non-adherence have been noted as 38.4% and 22.3% in young and older adults, respectively. Younger adults have been found to report higher rates of both unintentional and intentional non-adherence compared to older adults [6]. Among patients with mild and moderate hypertension, lifestyle modifications, constant monitoring for about 3-6 months, and medications are required to control the blood pressure. In patients with severe hypertension, however, both lifestyle modifications and medicines are required to control it. When these lifestyle modifications and prescribed medicines are adhered to every day of their life, hypertension might be controlled, and the benefits of controlled blood pressure might be realized [7, 8].
Medication adherence is crucial for the management of hypertension, and it involves following the prescribed medication regimen, including taking the medication at the right time and in the right dose. Non-adherence to medication is a significant problem, and it is associated with poor health outcomes and increased healthcare costs.
On the other hand, if patients adhere to their prescribed anti-hypertensive treatment regimens daily, blood pressure may be controlled, and these patients could lead relatively normal lives. Cardiovascular and renal disease and strokes (cerebrovascular incidents) could be avoided if hypertensive patients’ blood pressure levels are controlled. Healthcare professionals could play a major part in helping patients achieve and maintain hypertension control through providing effective health education [9, 10].
In Ghana, it is estimated that 93.3% of hypertensive patients do not adhere to their medication [11]. Data from the Sunyani Municipal Health Directorate shows that from 2020 to 2022, the prevalence of hypertension among the youth aged 18 to 35 was 1520 per 10, 000 population while the elderly aged 50 and above recorded 3038 per 10, 000 population [12] and medication adherence among hypertensive clients is low as there is an increased number in hypertension comorbidities in the Municipality. Hypertension medication adherence is a major burden in the Sunyani Municipality. Understanding the level of medication adherence for both the youth and the elderly is crucial for developing effective interventions to improve medication adherence and ultimately reduce the burden of hypertension-related complications in this population. Therefore, this study sought to provide an answer to the question: What are the perceptions of the youth and the elderly regarding hypertensive medication adherence in the Sunyani Municipality? The findings of this study could inform policy and practice aimed at improving hypertension management and reducing the burden of hypertension-related morbidity and mortality in the region.
Study design and setting
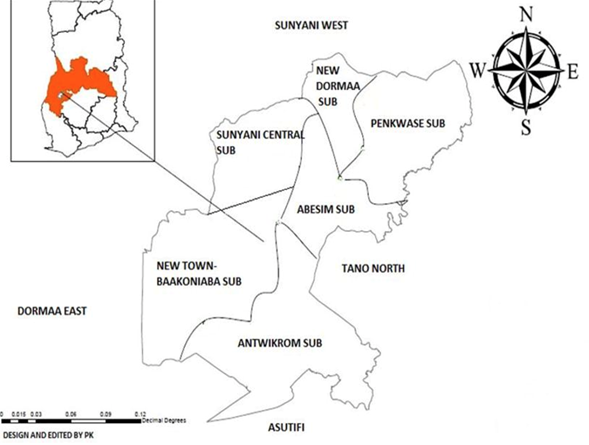
A qualitative study using a semi-structured interview guide was conducted to collect data through face-to-face interviews. The study was conducted in the Sunyani Municipality. The Sunyani Municipality is one of the oldest districts created and one of the twenty-seven administrative districts in the then Brong Ahafo Region of Ghana [13]. It has Sunyani as its municipal capital and is now the Bono Regional Capital. The district lies between Latitudes 70 20’N and 70 05’N and Longitudes 20 30’W and 2010’W and shares boundaries with Sunyani West District to the North, Dormaa District to the West, Asutifi District to the South, and Tano North District to the East [13] (Figure 1). There are effective economic and social interactions with the neighboring districts, which promote resource flow among this district [2]. The Municipality has more women of reproductive age, according to a health survey by the Municipal Health Directorate (MHD). The Municipal Health Directorate (MHD) is responsible for the health administration and coordination of activities of all health providers within the district. It owes its vision to improving the quality of health delivery in the Municipality. It has 35 health facilities and 34 functional Community-based Health Planning and Services (CHPS) zones in the six sub-municipalities.
Study population
The population of this study comprises hypertension patients in the Sunyani Municipality. In this study, hypertension is defined as the clinically diagnosed persistent elevated blood pressure on multiple occasions using standardized measurement techniques such as medical history, physical examination, and basic tests in a health facility. The hypertensive patients were individuals with medical records in a health facility in the Municipality.
The total population of individuals living in the Sunyani Municipality is 193,595. As of the end of 2022, Sunyani Municipal had 4558 patients per 10,000 population living with hypertension from the ages of 18 to 70 and above [13]. Out of the 193,595 population, 1520 per 10,000 population are young adults aged from 18 to 49 years, while the remaining 3038 per population are older adults aged above 50 years (Table 1). The World Health Organization defined the youth as individuals between the ages of 15 and 24 years. For this study, the youth were defined as individuals aged between the ages of 18 and 49 years to help capture young adults and middle-aged adults as well. Therefore, the youth for this study were adults aged 18 to 49 years, and the elderly aged 50 and above. The interviews were carried out with young and elderly hypertensive patients in the Sunyani municipality of Ghana.
Inclusion criteria
People who were clinically diagnosed with hypertension by confirming that their blood pressure (BP) is persistently elevated on multiple occasions, using standardised measurement techniques, and ruling out secondary causes with history, exam, and basic tests such as blood pressure measurement, and were above 18 years of age in any of the hospitals in the Sunyani Municipality were included in the study.
Exclusion criteria
HIV/AIDS patients or those on AR T treatment who have been diagnosed with hypertension were excluded from the study because the focus is on individuals with hypertension without underlying conditions.
Sample size and sampling technique
A purposive sampling technique was employed to sample people who were clinically diagnosed with hypertension from 18 years and above in any of the hospitals in the Sunyani Municipality as participants. Participants with hypertension records at the health facilities were considered for this study. Purposive sampling was employed to select specific participants who possess particular characteristics relevant to the research question. The twenty-eight patients who took part in this study were determined based on the saturation point during the face-to-face in-depth interviews.
Data collection instrument
Qualitative data were collected through in-depth individual interviews using an interview guide, and twenty-eight in-depth interviews were conducted. The interview was designed to obtain respondents’ perceptions on various questions relating to hypertension medication adherence. The interview guide enabled the researcher to cover the main topics and categories while giving space to explore issues that emerged during the interview. The interview guide was organized into parts with questions that helped to answer the various research questions formulated for the study. In a qualitative interpretivism framework, research based on interviews often seeks to penetrate social life beyond appearance and manifest meaning. Interpretivism is a research framework that focuses on understanding how people make sense of their social world, emphasising meanings, experiences, and perspectives rather than objective measurement or universal laws. Interpretivism maintains that reality is socially created and subjective, meaning that what is real depends on people’s interpretations, shared meanings, language, and culture. Instead of trying to discover general laws like in positivism, interpretivism attempts to understand how distinct individuals or groups perceive and interpret particular events.
Data collection procedure
The qualitative data were collected from both the elderly and the youth diagnosed with hypertension on medication adherence. Our interview guide was piloted with two elderly and two youth outside the study area. The researcher, assisted by two research assistants, conducted the interviews using the interview guide, which contained several open-ended questions. The interview guide helped us ensure that all the essential aspects of medication adherence regarding hypertension were comprehensively covered during each interview section. After that, all the necessary changes were made to the interview guide. The interviews were conducted in the Bono and other local languages of the participants and translated into English where necessary until saturation was reached, where no new information was being revealed from the interviews.
Data analysis
The audio-recorded interviews were first transcribed verbatim into a Microsoft Word document. These transcripts were then analyzed using thematic analysis. This involved the preliminary identification of broad themes from the transcripts, which were later developed into coded themes. In constructing the themes, we considered statements of meaning that were repeated with some regularity in the relevant data. These themes were verified and coded by independent coders to enhance the reliability of the findings. Data collection and analysis went hand in glove as the researchers progressively refined their interviews and observations, testing emerging conclusions. The interview transcripts were later imported into NVivo version 12 for detailed analysis. A codebook was developed that outlined the key themes of the study, with major themes being organised in a tree and free nodes. Using this codebook, the researchers independently coded the transcripts and cross-verified the coding. The identified themes and sub-themes are elaborated upon below, supported by respondent quotes.
Ethical considerations
Ethical clearance was sought from the Kintampo Health Research Centre Institutional Ethics Committee with study ID Number: KHRCIEC/2024-07 before the commencement of the study. Written consent was obtained from each participant before being included in the study. All information collected from the survey was kept confidential and safe. The anonymity and confidentiality of the study subjects were also ensured by assigning numerical codes instead of names without any personal identifiers in the data collection, analysis, and the findings. Participants were informed that participation was voluntary and based on their willingness, and they had the right to withdraw from the study at any point. Participants were also informed that participating in this study is voluntary and, therefore, they have the right to participate or refuse to participate in the study. The researchers verbally explained to the participants that whatever information was given was not going to be disclosed to the media or any other person who was not related to the study.
The sample for this study comes from a broad section, consisting of 14 youths and 14 elderly. The youth in this study fall between the ages of 18 and 49 years, with varying educational backgrounds ranging from no formal education up to postgraduate level. The elderly in this study fall within the age brackets of 50 to 70 years, mostly with primary education, although a number of them have no formal education (Table 2). The study consists of young adults of 14 participants, divided into 6 males and 8 females. The ages range from 18 to 35 years, thus predominantly falling into young adulthood. Levels of education among participants, 3 males and 3 females, have completed Senior High School (SHS) or its equivalent, while 4 participants are females with a first degree. One male participant had completed Junior High School (JHS), while one female participant reported completion of primary school. Two males reported no formal educational background. This makes for a good demographic profile since the diversity automatically guarantees a rich variation in perspectives due to the differentiated nature of age, gender, and years of schooling.
The ages of the adult participants were between 50 and 70 years. The gender distribution is almost even, with 8 males and 6 females. As for education, participants are mostly at a level where 9 have completed only primary school, indicating relatively low formal education in the group. One participant reported having gone to Junior High School or its equivalent, while two have gone to pursue postgraduate degrees. Two participants had received no formal education at all. Thus, the sample represented a wide variety of educations, though the majority had received limited formal education.
Emerging themes
Five main themes were identified: Beliefs about the importance of hypertensive medication, the effectiveness of hypertensive medication, motivation to take hypertensive medication, support systems, and alternative medication (Table 3).
Beliefs regarding the importance of hypertensive medication
Both the elderly and the youth shared their beliefs about the importance of hypertensive medication. All of the participants believe that taking their hypertensive medication as prescribed is important for their overall health because it will help them restore their health. One of the participants added that taking their hypertensive medication as prescribed is important.
“I believe, but taking the medication is not easy for me” (Participant 27, an elderly male).
Almost all of the participants pointed out that the importance of taking their hypertensive medication cannot be overemphasized. They believe taking their medications regularly will reduce their risk of having other complications associated with the disease. The respondents added that they strongly believe that it is important to be taking their hypertensive medications.
“…initially, when I was not yet diagnosed with the disease, I was not feeling well every day, but since I got to know and was put on medication, I am now getting better” (Participant 3, a young female).
Owing to the belief in the importance of taking hypertensive medications, both the youth and the elderly believed that the benefits of taking their hypertensive medication outweighed any potential side effects. Some participants disclosed that they understand that if they don’t adhere to their medications, their condition will get more complicated.
“The side effects are minor, which I can overlook, so the focus is getting better by taking my medication as prescribed” (Participant 1, a young male).
Half of the participants disclosed that they have seen some changes so far, and their blood pressure (BP) is stable nowadays. They said that they have to continually take their medications to prevent a relapse of the hypertension.
“I understand that not adhering to my medications can increase the risk of complications of my condition. I may get a stroke or heart disease” (Participant 24, an elderly female).
Almost all the participants indicated that they have been educated on the negative impact of not taking their drugs. They also indicated that whenever they do not take their drugs, they feel weak and sedated, and they are unable to involve themselves in any daily activities. Some of the participants added that they understand that some of the medication has side effects, so they should report any side effects.
“…I am also aware that I may get complications if I don’t take my medications as prescribed” (Participant 3, a young female).
All of the participants stated that they have developed a positive attitude towards incorporating hypertensive medication into their daily routine. A few of the participants added that they have developed trust in their healthcare providers’ recommendation to take their hypertensive medication as prescribed. Some of them disclosed that it is important to take their hypertension medication because it helps to reduce their high blood pressure to normal pressure to control their hypertension.
“I am trying to adhere even though taking the medication is not easy for me ” (Participant 21, an elderly male).
“I have to develop a positive attitude in order not to relapse” (Participant 2, a young male).
Most of the participants stated that they honestly trust their healthcare providers’ recommendations because they have helped them manage their condition incredibly. Some of the participants added that they have to be strong and positive-minded to stick to the required prescription and timelines. Some of the participants indicated that they believe in their healthcare providers.
“…because I was not feeling well some time ago, but when I came, they were able to find out my blood pressure was high, and they helped in maintaining my blood pressure at normal levels, and I have maintained a strong will to stay on course” (Participant 20, a young male).
The majority of the participants mentioned that the healthcare providers are very trustworthy and serious practitioners. Some of them added that they trust their healthcare providers 100 per cent because they know they will give them the best care to prevent any complications.
A few of the participants also stated similarly that they trust the health professionals because it was in that hospital that they were diagnosed with hypertension, and so they believe they are doing well in managing their condition.
“On a scale of 1-5, I will rate their preference as 4 because I trust them because they know best about my condition” (Participant 1, a young male).
“They have educated me well enough not to relapse” (Participant 20, an elderly male).
In a nutshell, both the youth and the elderly held the perception that taking their hypertensive medication as prescribed was important for their overall health. As a result, both groups believed that the benefits of taking their hypertensive medication outweighed any potential side effects, and they have developed a positive attitude toward incorporating hypertensive medication into their daily routine and have also developed trust in their healthcare providers’ recommendation to take their hypertensive medication as prescribed.
Effectiveness of hypertensive medication
The study sought respondents’ (both the youth and elderly) perception of how confident they were in the effectiveness of their hypertensive medication in controlling their blood pressure, as well as how adhering to their hypertensive medication reduces their risk of complications related to hypertension. On the same views, both the elderly and the youth indicated that they were confident in the effectiveness of their hypertensive medication in controlling their blood pressure and thus adhering to hypertensive medication to reduce the risk of complications. About half of them added that they are confident because they can see improvement in their condition.
A few of them also indicated that, in their opinion, adhering to their hypertensive medication reduces the risk of complications related to hypertension.
“…because when I take my medication regularly for some time now, I feel healthy” (Participant 8, a young male).
The participants in a similar view indicated that they are confident in the effectiveness of their medications because they know their healthcare provider knows the best. Besides, when they were not taking the medication, they experienced severe headaches and body weakness, but when they started to take their medications again, they felt fine. Some of them stated that with the education they received at the clinic regarding their medications, they knew they would be fine.
“My healthcare providers have educated me that when I refuse to take my medications, it will get worse, and I trust them because they have been helpful” (Participant 21, an elderly female).
The majority of the participants believe that the medication given is the best, and they know that with time, it will help improve their health condition by reducing other associated complications.
“…Hmm, it’s not easy though I take just two medications, I find it difficult to adhere, but I am confident that by taking my medication everything will be fine and there will be no complications” (Participant 20, an elderly male).
This means that both the youth and elderly have similar perceptions of how confident they were in the effectiveness of their hypertensive medication in controlling their blood pressure, as well as how adhering to their hypertensive medication reduces their risk of complications related to hypertension. Thus, the respondents shared that they were confident in the effectiveness of their hypertensive medication in controlling their blood pressure. Also, the youth and elderly respondents expressed a positive opinion in terms of adhering to hypertensive medication to reduce their risk of complications.
Motivation to take hypertensive medication
Perceptions of factors that motivated the youth and the elderly respondents to take their hypertensive medications regularly were not different. Both age groups of respondents shared similar confidence in their ability to overcome any barriers or challenges that may hinder their hypertensive medication adherence. Among the motivational factors are to have a long and healthy life, to avoid future complications, to receive constant health education from healthcare providers, and others. Some youth respondents shared that seeing elderly patients queuing for their medications motivates them to take their medications seriously and regularly to avoid being on drugs when they are old. The majority of the participants indicated that they want to have a long and healthy life, so adhering to their medication will increase their chances of living long, healthy lives. Some of them stated that they think they may get heart disease or stroke, so it motivates them to take their medications regularly.
“To avoid future complications such as heart disease and stroke, I adhered to the recommendations given by my healthcare providers” (Participant 4, a young female).
More than half of the participants indicated that the education they received at the clinic motivates them to adhere to their medications.
“I believe I will come back to my normal health after ingesting the drugs because my condition is hereditary, but my mother is perfectly well after taking in the drugs” (Participant 10, a young male).
Most of the participants indicated that when they see people with stroke or heart disease, they are motivated to take their medications so that they will not get stroke or heart disease. A few of them stated that they don’t want to be a burden to their children, so that they may have to take care of me, so this motivates them to take their medications regularly.
“My children are my everything to me, and I will do everything to sustain my life to take care of my children” (Participant 15, an elderly female).
“My health and work. I want to live long to take care of my children and grandchildren” (Participant 19, a young female).
“My family, especially my children, keep me motivated” (Participant 23, an elderly male).
Most of the participants were confident in their ability to overcome any barriers that may hinder their hypertensive medication adherence. Some of the participants were confident because they knew that adherence would help reduce the risk of their conditions getting complicated. With determination and the support from family and the nurses, they are hopeful that they will be okay.
“I’m self-motivated, so I have made it my point to keep myself healthy” (Participant 4, a young female).
Some of the participants believe in the hypertensive medication, and because of that, they have been recording average BP every 2 months on visits. Some participants also attributed their ability to overcome any barriers or challenges to prayers and belief in God. Some believe that with the help of God, they can overcome any barriers or challenges hindering their hypertensive medication adherence.
“Yes, I am very confident. I keep trying, and with the help of God, I will adhere strictly” (Participant 19, a young female).
Support systems
In terms of support systems, participants were asked whether they considered taking their hypertensive medication as a personal responsibility or if there existed support systems that encouraged them to adhere. Both age groups affirmed that they considered taking their hypertensive medication as a personal responsibility, even though they had other support systems that encouraged them to adhere. The majority of the participants disclosed that their health is a personal responsibility because the medication is helping to improve their health, and as such, they have to adhere to it. Some of the participants admitted that, because the condition may worsen if medications are not taken seriously, they sometimes get support from their families in terms of reminding them to take their medication.
“…Yes, because it is my health which is being affected if I do not adhere. The support from the healthcare providers and my family is meant to motivate” (Participant 20, an elderly male).
“I think I am responsible for taking care of myself” (Participant 19, an elderly female).
Although not all age groups of respondents had support systems in place, the study ascertained that all the respondents, regardless of age group, believed that taking their hypertensive medication was a personal responsibility. Most of them indicated that they want their health back to normal. They have taken it as their responsibility long ago; otherwise, they would have died.
“I have no one to support in any way; it is just myself, and with God, I am good” (Participant 20, an elderly male).
Most of the participants further indicated that even if they get support and they don’t take it upon themselves to manage their condition, they will still get complications. Others added that if their condition gets worse, they will suffer, and so they have to take it upon themselves to manage the condition. The changes are very positive and, for that matter, they do not hesitate to take their medication.
“I have taken it as my responsibility to manage my condition. I don’t have any support system; I just try to do it myself “ (Participant 8, a young male).
Alternative medication
Perceptions of respondents on alternative medications were also sought. Respondents were asked whether they were actively seeking information and resources to enhance their knowledge about hypertensive medication and adherence, as well as whether they were considering alternative medication, such as traditional herbs, rather than hospital medication. The study found that the majority of the youth and the elderly were not actively seeking information and resources to enhance their knowledge about hypertensive medication and adherence. However, they relied on the medical education provided by their healthcare providers. We are always asked about the progress of our condition and how stable it is becoming from the healthcare providers, and we deem it to be stable enough.
“…not really because I believe the drugs taken are sufficient” (Participant 24, a young female).
The few who were in one way or another seeking information and resources to enhance their knowledge about hypertensive medication and adherence did so through social media and the internet. They were youth-dominated. Some participants shared that at times, on social media and during teachings at the clinic. Others said they just read on the internet and the teachings at the clinic.
“I searched online frequently to update myself every time” (Participant 9, a young female).
Also, the majority of the study’s participants, irrespective of age, did not consider alternative medications such as herbal medicine or traditional medicine. Thus, the perceptions of the majority of the participants were similar to alternative medications for hypertension treatment.
“No… I don’t have trust in traditional medicine’’ (Participant 10, a young male).
“I have not thought of it yet” (Participant 19, an elderly female).
Some of them stated that they had experienced the damaging side effects because it happened to their relatives. A few of them stated they have trust in the hospital-based system. Others also think that the medication given by healthcare professionals is the best.
“For now, no, the medication given to me at the clinic is better” (Participant 16, a young male).
Some of them stated they were not sure for now, but the medication given to them at the clinic is helping them. A few of them also added that people have become corrupt nowadays, and they might do anything to get money without thinking of the health implications for others. Notwithstanding, a few of the youth had thought of considering herbal medications but had yet to try them .
“I have thought about it. Maybe in the future, I will consider an alternative if the condition remains the same” (Participant 10, a young male).
Some of the participants also indicated that they sometimes believe that alternative medicine, such as traditional medicine or herbal medicine, could help, but they have yet to try it. A few of them indicated that if their blood pressure remains normal, they will not consider alternative medicine unless it becomes highly unstable. A few of the elderly who had tried alternative medicine shared that it was not helpful and would prefer the hospital medication to any alternative medicine. Others disclosed that they, at times, do herbal remedies but cannot tell whether it is good or not. Few openly stated that herbal remedies are not very helpful.
“I prefer hospital medicine because its side effects are known, unlike herbal medicines’’ (Participant 18, an elderly female).
In the study, there was a very strong consensus from the participants that it’s important to adhere to prescribed treatments irrespective of age. The youth and the elderly both realized that taking medication as prescribed was the key to their health and helped in preventing complications that might have resulted from hypertension. Participants reported positive changes in health since the commencement of medication and indicated that the side effects were far outweighed by the benefits. There was a central theme of trust in health providers and confidence in the health providers’ competence, and several responses reflected insights about the management of the condition.
These motivating factors for adherence included the desire to live long and healthily, familial responsibilities, and a fear of future complications such as heart disease or stroke. Although most of the participants viewed taking medication as a matter of personal responsibility, they still appreciated the support of family and health professionals. It is amazing that only some tried complementary remedies or looked for additional information besides what was recommended by the health professional; in general, the attitude confirms confidence in traditional medicine.
Emphasis on medication adherence to hypertensive drugs was identified as central by the respondents when it comes to the management of health and the prevention of complications, irrespective of their age. This evidence is therefore supported by the work of Khayyat et al., [5] in stating that adherence is critical to better health outcomes, healthcare cost containment, and improvement in quality of life.
The participants very much appreciated the educational support concerning the risks of poor adherence and how best to manage minor side effects [14, 15]. It was also the case that trust in the competence of health professionals and their advice acted as a necessary enabling factor, whereby participants communicated confidence in adherence. Regarding treatment effectiveness, participants, irrespective of age, believed that medicines would help in controlling blood pressure and lowering risks. Relieved symptoms of diseases further reinforced such confidence, as was also revealed by Gomis-Pastor [16], who found adherence to be indicative of healthy behaviour and a good quality of life.
Motivation for adherence was variable; younger patients were motivated by the commitment of older patients, not wanting to be on lifelong medication, whereas others did not want to develop severe conditions such as heart disease or stroke.
Furthermore, it was observed that both age groups always refilled their medication prescription before it ran out, even though they often experienced difficulties or side effects that made it challenging to adhere to the medication regimen. However, both the elderly and the youth always felt confident that taking their medication would effectively manage their hypertension and always had a support system (family, friends, healthcare provider) that encouraged and reminded them to take their medication. Both the elderly and the youth always believed that sticking to their medication regimen is crucial for maintaining their overall health, so they found it easy to incorporate taking their medication into their daily routine and often took their hypertension medication as prescribed.
Though a few of the participants sought further information from social media, most relied on healthcare provider education and felt this was sufficient. There was also little interest in alternative treatments, with prior experiences of herbal remedies proving disastrous for many; thus, many had trust in care based within the hospital setting. This supports Teshome et al., [17], who reported that partial knowledge about the disease and lack of reliable alternatives are among the variables that affect hypertensive patients’ adherence attitude. Generally, this study underlines that perceived benefits, family support, provider trust, and tailored education play a determining role in promoting sustained adherence.
This study provides an understanding of the perceptions of both the youth and the elderly regarding their adherence to medication for hypertension. Although hypertensive youth and elderly patients from Sunyani recognized the importance of adherence, both groups were non-adherent. Identification of age-specific adherence barriers and supportive relationships may strengthen adherence, especially among younger patients. Both acknowledge that continuous medication serves best to maintain health, control blood pressure, and prevent complications such as heart disease and stroke. Therefore, trust in health care providers and family support were identified as strong motivational factors; this proves the powerful influence of a supportive milieu on health behaviors. Additionally, there was limited interest in alternative treatments, particularly herbal remedies, both because prior negative experiences had occurred and because of the belief in in-hospital treatment.
Furthermore, the participants made use, for the most part, of the medical education provided by the providers, although the youth expressed a partial desire to learn more about their condition using online resources. The findings suggest that effective hypertensive management requires constant education on the part of the patient, supportive relationships, and access to available resources. This is how one can battle barriers in the form of side effects and knowledge gaps, which, together with enhancing adherence, will reinforce the idea of hypertensive management among the youth as well as the elderly.
What is already known about the topic
What this study adds
| Health Facility | Young Adult (15-49 years) | Elderly (50 years and above) |
|---|---|---|
| Sunyani Municipal Hospital | 345 | 1078 |
| SDA Hospital | 398 | 769 |
| Bono Regional Hospital | 777 | 1191 |
| Total | 1,520 | 3,038 |
Table 2: Demographic Characteristics of Participants Both the Youth and the Elderly
| Youth | Elderly | ||||
|---|---|---|---|---|---|
| Participant | Gender | Education Level | Participant | Gender | Education Level |
| 1 | A young male | Senior High School (SHS) or Equivalent | 15 | An elderly female | Primary School |
| 2 | A young male | Junior High School (JHS) or Equivalent | 16 | An elderly male | Postgraduate Degree |
| 3 | A young female | Primary School | 17 | An elderly male | Primary School |
| 4 | A young female | First Degree | 18 | An elderly male | Primary School |
| 5 | A young female | First Degree | 19 | An elderly female | Primary School |
| 6 | A young female | SHS or Equivalent | 20 | An elderly female | Primary School |
| 7 | A young female | First Degree | 21 | An elderly male | Junior High School (JHS) or Equivalent |
| 8 | A young male | No Educational Background | 22 | An elderly female | No Educational Background |
| 9 | A young female | SHS or Equivalent | 23 | An elderly male | No Educational Background |
| 10 | A young male | No Educational Background | 24 | An elderly female | Primary School |
| 11 | A young female | SHS or Equivalent | 25 | An elderly female | Primary School |
| 12 | A young female | First Degree | 26 | An elderly male | Postgraduate Degree |
| 13 | A young male | SHS or Equivalent | 27 | An elderly male | Primary School |
| 14 | A young female | SHS or Equivalent | 28 | An elderly male | Primary School |
Source: Field Data, 2023
| Emerging Themes | Subthemes |
|---|---|
| Beliefs about the importance of hypertensive medication | Perceived Importance of Medication Adherence |
| Acknowledgment of Benefits Over Side Effects | |
| Impact of Health Education | |
| Trust in Healthcare Providers | |
| Effectiveness of hypertensive medication | Confidence in Medication’s Effectiveness |
| Belief in Reduced Risk of Complication | |
| Challenges of Adherence Despite Confidence | |
| Motivation to take hypertensive medication | Desire for a Long and Healthy Life |
| Influence of Family and Social Responsibility | |
| Education and Observational Learning | |
| Spiritual Beliefs and Personal Determination | |
| Support systems | Personal Responsibility in Health Management |
| Family and Social Support | |
| Spiritual and Self-Reliance | |
| Awareness of Consequences | |
| Alternative medication | Reliance on Medical Education |
| Trust in Hospital-Based Medication | |
| Skepticism About Alternative Medicine | |
| Potential Future Consideration of Alternative Medicine |