Research | Open Access | Volume 9 (2): Article 79 | Published: 20 May 2026

Views: 989
Menu, Tables and Figures
| Variable | Positive malaria | Negative Malaria | Total | Percentage (%) |
|---|---|---|---|---|
| Age (years) | ||||
| <25 | 51 | 97 | 148 | 37.2 |
| 25–34 | 41 | 93 | 134 | 33.7 |
| 35–44 | 17 | 54 | 71 | 17.8 |
| 45–54 | 7 | 22 | 29 | 7.3 |
| >54 | 2 | 14 | 16 | 4.0 |
| Sex | ||||
| Male | 86 | 125 | 211 | 53.0 |
| Female | 32 | 155 | 187 | 47.0 |
| Religion | ||||
| Protestant | 3 | 6 | 9 | 2.3 |
| Orthodox | 4 | 13 | 17 | 4.3 |
| Catholic | 3 | 7 | 10 | 2.5 |
| Muslim | 108 | 254 | 362 | 91.0 |
| Educational status | ||||
| Illiterate | 75 | 199 | 274 | 68.8 |
| Literate | 43 | 81 | 124 | 31.2 |
| Family size | ||||
| <5 | 106 | 256 | 362 | 91.0 |
| ≥5 | 12 | 24 | 36 | 9.0 |
| Marital status | ||||
| Single | 10 | 77 | 87 | 21.9 |
| Married | 105 | 186 | 291 | 73.1 |
| Divorced | 1 | 12 | 13 | 3.3 |
| Widowed | 2 | 5 | 7 | 1.8 |
| Residency | ||||
| Urban | 61 | 110 | 171 | 43.0 |
| Rural | 57 | 170 | 227 | 57.0 |
Table 1: Socio-demographic characteristics of study participants for malaria prevalence in the Kurmuk district, Benishangul Gumuz regional state, Ethiopia (n=398)
| Variable | Malaria Positive (%) | Malaria Negative (%) | COR (95% CI) | AOR (95% CI) | P value |
|---|---|---|---|---|---|
| Sex (ref: Female) | |||||
| Male | 86 (40.8) | 125 (59.2) | 3.33 (2.08–5.32) | 4.13 (2.48–6.87) | <0.001 |
| Female | 32 (17.1) | 155 (82.9) | 1.00 | 1.00 | |
| Place of residence (ref: Urban) | |||||
| Rural | 61 (35.7) | 110 (64.3) | 1.65 (1.07–2.55) | 2.14 (1.31–3.49) | 0.002 |
| Urban | 57 (25.1) | 170 (74.9) | 1.00 | 1.00 | |
| IRS done within last 6–12 months (ref: No) | |||||
| Yes | 3 (7.0) | 40 (93.0) | 0.16 (0.05–0.52) | 0.14 (0.04–0.49) | 0.002 |
| No | 115 (32.4) | 240 (67.6) | 1.00 | 1.00 | |
| ITN utilized (ref: No) | |||||
| Yes | 29 (20.7) | 111 (79.3) | 0.50 (0.31–0.80) | 0.58 (0.34–0.99) | 0.047 |
| No | 89 (34.5) | 169 (65.5) | 1.00 | 1.00 | |
| Distance from breeding sites (ref: >1 km) | |||||
| ≤1 km | 92 (34.7) | 173 (65.3) | 2.19 (1.33–3.60) | 1.88 (1.08–3.26) | 0.025 |
| >1 km | 26 (19.5) | 107 (80.5) | 1.00 | 1.00 | |
| Outdoor activities (ref: No) | |||||
| Yes | 103 (31.1) | 228 (68.9) | 1.55 (0.84–2.86) | 1.37 (0.68–2.73) | 0.377 |
| No | 15 (22.4) | 52 (77.6) | 1.00 | 1.00 | |
| Travel history within 30 days (ref: No) | |||||
| Yes | 68 (37.8) | 112 (62.2) | 2.04 (1.32–3.15) | 2.09 (1.29–3.40) | 0.003 |
| No | 50 (22.9) | 168 (77.1) | 1.00 | 1.00 | |
| Education (ref: Literate) | |||||
| Illiterate | 75 (27.4) | 199 (72.6) | 0.71 (0.45–1.12) | 0.77 (0.46–1.27) | 0.302 |
| Literate | 43 (34.7) | 81 (65.3) | 1.00 | 1.00 | |
| Abbreviations: COR = Crude Odds Ratio; AOR = Adjusted Odds Ratio (adjusted for all variables in the table); CI = Confidence Interval; IRS = Indoor Residual Spraying; ITN = Insecticide Treated Net | |||||
Table 2: Multivariate analysis of factors associated with malaria among clients visiting health facilities in Kurmuk district, Benishangul Gumuz Regional State, Ethiopia, 2022 (n=398)
| Breeding site | No. of dips | No. of +ve dips | Larval density | Dipper index | Species density | |||
|---|---|---|---|---|---|---|---|---|
| An. Gambiae s.l | An. coustani | An. maculipalpis | An. pharoensis | |||||
| Canal with vegetation | 10 | 2 | 28 (14.7%) | 20 | 32.1 | 7.1 | 0 | 60.7 |
| Fresh water pool | 8 | 1 | 5 (2.6%) | 12.5 | 60 | 0 | 20 | 20 |
| River margin | 10 | 7 | 91 (47.6%) | 70 | 40.7 | 25.3 | 2.2 | 30.8 |
| Discarded tire | 3 | 1 | 18 (9.4%) | 33.3 | 27.7 | 16.6 | 5.5 | 50 |
| Plastic container | 1 | 0 | 0 (0%) | 0 | 0 | 0 | 1.1 | 0 |
| Irrigation ditch | 7 | 5 | 49 (25.7%) | 71.4 | 63.2 | 32.6 | 2.0 | 2.0 |
Table 3: Malaria vector breeding habitat & species density in Kurmuk town, Benishangul Gumuz region, Ethiopia
Zalalam Olani1,&, Samrawit Solomon1,2, Tolcha Kebebew2, Solomon Kinde3, Fufa Hunduma1, Haimanot Ewunetu1, Ebsa File3, Sarah Zohdy4, Chloe Crocker4, Mame Niang4
1Saint Paul’s Hospital Millennium Medical College, School of Public Health, Addis Ababa, Ethiopia, 2Centers for Disease Control and Prevention, Addis Ababa, Ethiopia, 3Ethiopian Public Health Institute, Addis Ababa, Ethiopia, 4US Centers for Disease Control and Prevention, Atlanta, Georgia, USA
&Corresponding author: Zalalam Olani, Saint Paul’s Hospital Millennium Medical College, School of Public Health, Addis Ababa, Ethiopia, Email: zalalamolani8@gmail.com, ORCID: https://orcid.org/0000-0002-0857-7723
Received: 12 Aug 2025, Accepted: 15 May 2026, Published: 20 May 2026
Domain: Infectious Disease Epidemiology
Keywords: Human mobility, border health, malaria prevalence, Ethiopia-Sudan border
©Zalalam Olani et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Zalalam Olani et al., Cross-border human mobility and malaria prevalence in Western Ethiopia: A case of the Kurmuk District. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):79. https://doi.org/10.37432/jieph-d-25-00173
Introduction: Cross-border population movement complicates malaria control, especially for countries like Ethiopia that aim for elimination. Kurmuk District, on the Ethiopia–Sudan border, faces elevated risk due to frequent human mobility, ecological continuity, and disparities in malaria prevalence between the two countries. This study assessed the influence of cross-border human mobility on malaria prevalence and identified associated risk factors in Kurmuk, Western Ethiopia.
Methods: A mixed-methods cross-sectional study was conducted from December 2021 to February 2022. Health facility attendees were tested for malaria by microscopy and interviewed about travel history and risk factors. Entomological surveys identified local vectors. Qualitative data on travel patterns came from eight key informant interviews.
Results: Among 398 participants, 118 (29.6%) tested positive for malaria. Being male (aOR = 4.1; 95%CI: 2.48–6.87), rural residence (aOR = 2.1; 95%CI: 1.31–3.49), recent travel (aOR = 2.1; 95%CI: 1.29–3.40), and living within 1 km of mosquito breeding sites (aOR = 1.9; 95% CI: 1.08–3.26) were significantly associated with having malaria. Protective factors were use of insecticide-treated nets (ITN) (aOR = 0.6; 95% CI: 0.34–0.99) and indoor residual spraying (IRS) (aOR = 0.1; 95% CI: 0.04–0.49). Coverage was 45.2% for ITNs and 28.6% for IRS. Anopheles gambiae s.l. was the dominant vector (49.5%). Qualitative findings showed that adults, especially merchants and religious travellers, frequently cross into Sudan during the dry season.
Conclusion: High malaria prevalence in this border district, driven by cross-border mobility and suboptimal vector control, threatens national elimination efforts. Strategies must include targeted interventions for mobile populations, cross-border collaboration, and improved ITN/IRS coverage.
Malaria is a vector-borne disease that is transmitted by Anopheles mosquitoes. It is one of the leading causes of mortality and morbidity in many developing countries [1]. The World Malaria Report of 2020 showed about 215 million cases of malaria, and 94% of these malaria cases were reported from the WHO African region [2].
Ethiopia has put updated malaria control measures into practice to control and eventually eliminate malaria. In recent decades, two malaria prevention interventions, indoor residual spraying (IRS) and insecticide-treated bed nets (ITNs), have been responsible for averting more cases of malaria than any other tool [2]. Malaria distribution in Ethiopia is a climatic and topographic “patchwork.” Transmission is intense in the hot, low-lying areas below 1,500 meters, unstable in the mid-altitude highlands [1,500-2,500m], and negligible in the cool highlands above 2,500 meters, where temperatures are too low for the parasite to develop. This stratification, driven by altitude-controlled temperature, is essential for targeting control efforts effectively [3,4].
Human mobility is a well-established factor in malaria transmission, particularly in regions pursuing elimination. Studies using malaria case data and migration patterns confirm that countries with high migration often have high infection rates. To effectively control and eliminate malaria, especially in cross-border contexts, it is essential to incorporate human movement into public health strategies. A detailed travel history is crucial for identifying the likely geographic origin of a malaria infection [5]. Understanding the role of human mobility in malaria transmission is critical for developing the dynamic interventions needed to achieve the WHO’s 2030 elimination goals [2,6,7]. This study assessed the malaria burden associated with human migration in the Kurmuk border district of Ethiopia and Sudan and examined environmental factors influencing malaria incidence.
Study area
Kurmuk district, situated in the Benishangul-Gumuz Region of western Ethiopia, occupies a strategically important position, sharing an extensive international border with Sudan to the north and west. The district’s geographical characteristics feature significant elevation variations that create diverse microclimates and ecological zones, with a predominantly hot tropical monsoon climate marked by distinct seasonal variations. Annual temperatures typically range between 19°C (66°F) and 39°C (103°F), creating favourable conditions for disease transmission throughout much of the year. The landscape is characterized primarily by natural vegetation, with extensive forest cover and grasslands supporting agricultural activities and livestock rearing.
Economically, the district relies mainly on subsistence farming of sorghum and maize, complemented by traditional gold mining operations that attract migrant labour and contribute to significant population mobility. Healthcare services are provided through three main health facilities Horazahabe Health Centre, Dulshetaul Health Centre, and Famatsera Health Center, which serve as crucial access points for malaria diagnosis and treatment. This combination of climatic conditions, cross-border location, economic activities involving population movement, and limited healthcare infrastructure establishes Kurmuk as a high-priority district for malaria control interventions and underscores its significance in Ethiopia’s broader malaria elimination efforts.
Kurmuk District is a geographically isolated border area with limited road infrastructure, periodic security concerns, and a highly mobile population. Conducting a community‑based household survey would have required extensive logistical coordination, including travel to dispersed rural kebeles, securing permissions from multiple administrative and traditional authorities, and managing safety risks near the international border. The three health centres Horazahabe, Dulshetaul, and Famatsera serve as the primary points of care for the majority of the district’s population and provided a secure, accessible, and practical site for systematic recruitment.
Study design and period
The study was conducted from December 2021 to February 2022. The study utilized a mixed-methods approach. Quantitative data on malaria prevalence and risk factors were collected via structured questionnaires and microscopic blood examination. Entomological data on malaria vectors were gathered through larval and adult mosquito collections. Qualitative insights into community travel patterns were obtained through key informant interviews.
Study population
The source population for this study consisted of all adult residents (aged 18 years and above) of Kurmuk district in the Benishangul Gumuz region of Ethiopia during the study period. The study population included people who visited health centers in the Kurmuk area of the Benishangul Gumz Regional State from December 1/2021 to February 30/2022. The study included consenting adults (≥18 years) who were conscious, willing, and seeking medical care at the participating health facilities. Pregnant mothers and children under the age of 18 were excluded from this study. This decision was made for two primary reasons: first, to focus on the highly mobile adult population, particularly adult males, who are identified as key drivers of malaria transmission and importation in border regions due to their travel patterns for work and trade; and second, to streamline the ethical and procedural protocols for this initial study, as involving minors and pregnant women requires additional safeguards and consent processes.
Sample size and sampling procedure
The sample size was determined using two statistical approaches, and the larger value was selected to ensure adequate power for both prevalence estimation and identification of associated risk factors. First, the single population proportion formula was applied to estimate the minimum sample size required for malaria prevalence, using a previously reported prevalence rate of 22.2% from Dembiya district, North-Western Ethiopia [8]. With a 95% confidence level (Z = 1.96) and a 5% margin of error, the calculated sample size was 264. After adding a 10% non-response rate, the sample size became 290.
Second, for the specific objective of identifying factors associated with malaria prevalence, the double population proportion formula was used, guided by prior studies. Using Epi Info™ version 7 (StatCalc), sample sizes were computed for each key risk factor, including ITN utilisation, presence of stagnant water, ITN availability, house spraying, and travel away from home, based on proportions and odds ratios from a study conducted in Mizan-Aman Town and its catchment area, Southwest Ethiopia [9]. Assumptions included a 95% confidence level, 80% power, and a 1:1 ratio between exposed and unexposed groups. The largest sample size obtained from these calculations was 398 (for the variable ITN utilization). After accounting for a 10% non-response rate, the final sample size was 438. Since this was larger than the 290 derived from the single proportion formula, it was selected as the study sample size and proportionally distributed across the study population at each health centre.
Sampling procedure
A systematic random sampling technique was employed to select participants at each of the three health centres. The total sample size (N=438) was proportionally allocated to each health centre based on its respective catchment populations. The sampling frame consisted of all consecutive adult patients (≥18 years) attending the outpatient department (OPD) at each health center during the study period. The sampling interval (k) was calculated daily for each facility by dividing the average daily patient flow (obtained from health center records). On each day of data collection, a starting point was randomly selected between 1 and k. Thereafter, every kth patient was invited to participate in the study after initial triage. This process continued each day until the pre-allocated sample size for each health centre was reached. Eligible patients who declined to participate were recorded as non-respondents, and the next kth patient was approached.
Data collection tools and procedures
After providing informed consent, participants who were systematically recruited via the process described above underwent a face-to-face interview using a structured questionnaire. Participants were asked about recent travel history, destinations, purposes of travel, and border crossings. Key informant interviews supplemented these data by providing contextual understanding of community-wide travel patterns, seasonal trends, and economic or social drivers of mobility.
Immediately following the interview, a blood sample was collected by a trained laboratory technician from each consenting participant for parasitological examination. Blood samples were collected via finger-prick.
Laboratory data collection and analysis
Malaria diagnosis followed WHO guidelines, with a quality control protocol where all positive slides and a random sample of negatives were re-checked at a regional reference laboratory.
Entomological survey
Methods and site selection
Potential mosquito breeding habitats were identified through preliminary field surveys targeting sites consistent with the ecological preferences of malaria vectors, including natural features such as river margins and freshwater pools, as well as artificial containers like cisterns, wells, tyres, and plastic containers. From these, six confirmed breeding habitats were systematically sampled using standard 350 ml dippers (up to 10 dips per site) or plastic pipettes for confined areas. Collected larvae and pupae were reared to adulthood in the laboratory and identified to species using morphological keys.
Adult Anopheles mosquitoes were collected indoors using CDC light traps positioned 1.5 meters above the ground near sleeping spaces from 18:00 to 06:00 hours. Households for trapping were purposively selected within 2 km of identified larval habitats to evaluate the spatial link between breeding sites and indoor vector presence. Captured mosquitoes were transported, euthanised, and identified using standard taxonomic keys.
Description of larval habitats and sampling of Anopheles
To detect the invasive malaria vector Anopheles stephensi, which breeds in man-made water containers, a comprehensive survey of potential larval habitats was conducted in Kurmuk town. Sites examined included concrete cisterns, wells, irrigation ditches, discarded tyers, plastic containers, freshwater pools, and interrupted river margins.
From a total of six identified larval habitats, Anopheles larvae and pupae were collected. Standard 350 ml dippers were used to take 10 dips per site where possible, while plastic pipettes were employed in smaller, confined breeding sites. All collected larvae were transported to the laboratory, reared to adulthood, and identified to species level using standard morphological keys [10,11].
Adult Anopheles mosquito collection
Adult Anopheles mosquitoes were collected using CDC light traps set from 18:00 to 06:00 hours. Traps were positioned 1.5 meters above the ground near sleeping spaces protected by long-lasting insecticidal nets (LLINs). Captured mosquitoes were transported to the laboratory in plastic collection cups, euthanised by freezing, and identified to species level using standard morphological keys.
Data quality management
Malaria diagnostics were performed by an expert laboratory technologist at the regional laboratory and the three health centres. Before testing began, internal quality assurance (IQA) was conducted using the standard 2016 WHO IQA checklist [12]. To ensure diagnostic accuracy, all positive slides and a random sample of 14% of negative slides underwent cross-verification at the Benishangul Gumuz Regional State Public Health Laboratory Institute. All procedures followed standard operating protocols, utilizing appropriate quality control materials for both thick and thin blood films. Collected data underwent thorough cleaning, coding, and entry. Entomological data were analyzed by a senior entomologist from the Ethiopian Public Health Institute (EPHI), with verification performed by a counterpart from the US Centres for Disease Control and Prevention (CDC).
Data analysis
Quantitative data were entered into Epi-Info v7.2.1.0 and analyzed using SPSS v20. Results were presented through descriptive and inferential statistics, including text, tables, and figures. Bivariate logistic regression identified candidate variables (p < 0.25) for the final multivariable logistic regression model. Model fitness was assessed using the Hosmer-Lemeshow test, and variables with p < 0.05 in the multivariable analysis were considered significant risk factors for malaria. Multicollinearity among independent variables was assessed using the Variance Inflation Factor (VIF). All VIF values were below 2.5, indicating no substantial multicollinearity.
A binary logistic regression analysis was performed on the variables, which included socio-demographic factors and risk factors. Eight variables, including sex, residency area, IRS in residence, ITN residence, having travel history, living home distance from larval habitat breeding sites, outdoor activities, and educational status, were candidate variables for the final model. In the binary logistic regression analysis, variables with P-values equal to or less than 0.25 were identified for the multiple logistic regression analysis.
After potential confounders were controlled, all variables that showed a statistically significant association during the binary logistic regression analysis were included in the multiple logistic regression analysis. These characteristics have a significant association with malaria, according to the results of the multiple logistic regression analysis (P-value 0.05)
Qualitative data collection and sampling
Semi-structured key informant interview guides were developed to explore cross-border malaria and human mobility. The development process included: a targeted literature review on mobility and malaria risk in border settings; a conceptual framework addressing who travels, why, when, where, and how; expert review by epidemiologists, a qualitative methodologist, and an entomologist; and pilot testing with two community members, which led to minor wording adjustments and the addition of probes on religious travel and mining-related mobility
A qualitative study was conducted in the Kurmuk district to describe the community’s travelling patterns. Key informants were selected using a purposive sampling technique to ensure the inclusion of individuals with expert knowledge of population mobility from diverse sectors. The selection criteria required participants to hold a relevant leadership or expert position for at least one year and have direct knowledge of community travel patterns.
We recruited eight key informants, representing the following sectors: health (a health extension worker, the head of the district health office, and two health office experts), trade (the head of the trade office), transport (the head of the transport office), religion (a religious leader), and community leadership (a community leader). Recruitment continued until thematic saturation was reached, meaning that subsequent interviews no longer yielded new information or themes related to travel patterns.
The interviews were transcribed into Amharic, translated into English, and then coded and analyzed thematically using NVIVO version 12.
Thematic analysis
We conducted inductive thematic analysis following Braun and Clarke’s six-phase framework. Two authors independently read all transcripts, performed line-by-line coding in NVivo 12, and met iteratively to develop and refine a codebook. Codes were grouped into categories, then synthesised into broader themes; disconfirming evidence was actively sought. Final themes were defined and illustrated with quotations.
Trustworthiness
Credibility was enhanced through investigator triangulation (dual coding) and peer debriefing; preliminary findings were validated with the district health office. Transferability was supported by thick contextual description. An audit trail (raw transcripts, coding files, NVivo project) ensured dependability. Reflexivity was maintained through team discussions and bracketing of prior assumptions.
Ethical consideration
The Institutional Review Board (IRB) of St. Paul’s Hospital Millennium Medical College (SPHMMC) gave ethical approval. The implementation of the study was also given written approval by the Benishangul Gumuz Regional Health Bureau. Before being asked to sign a consent form and participate in an interview, each study participant received an overview of the study’s goals. In order to safeguard confidentiality, study participant data were kept private and used without any personal information.
Socio-demographic characteristics of the participants
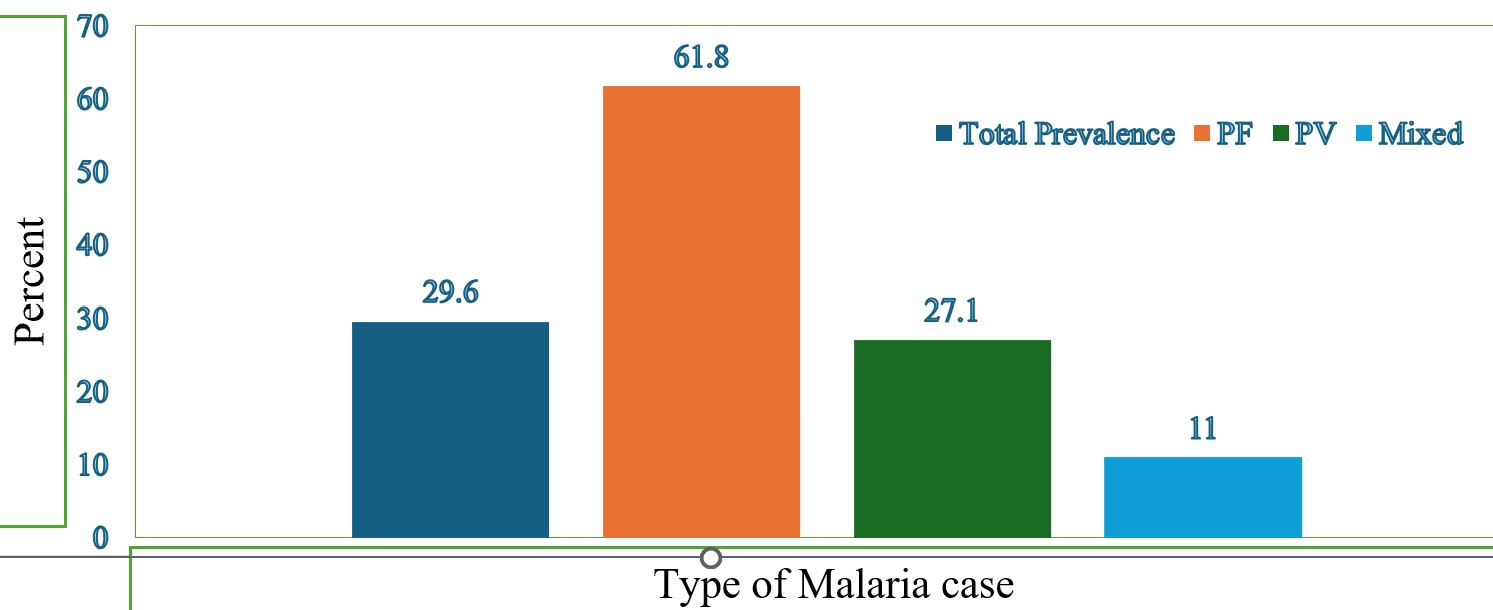
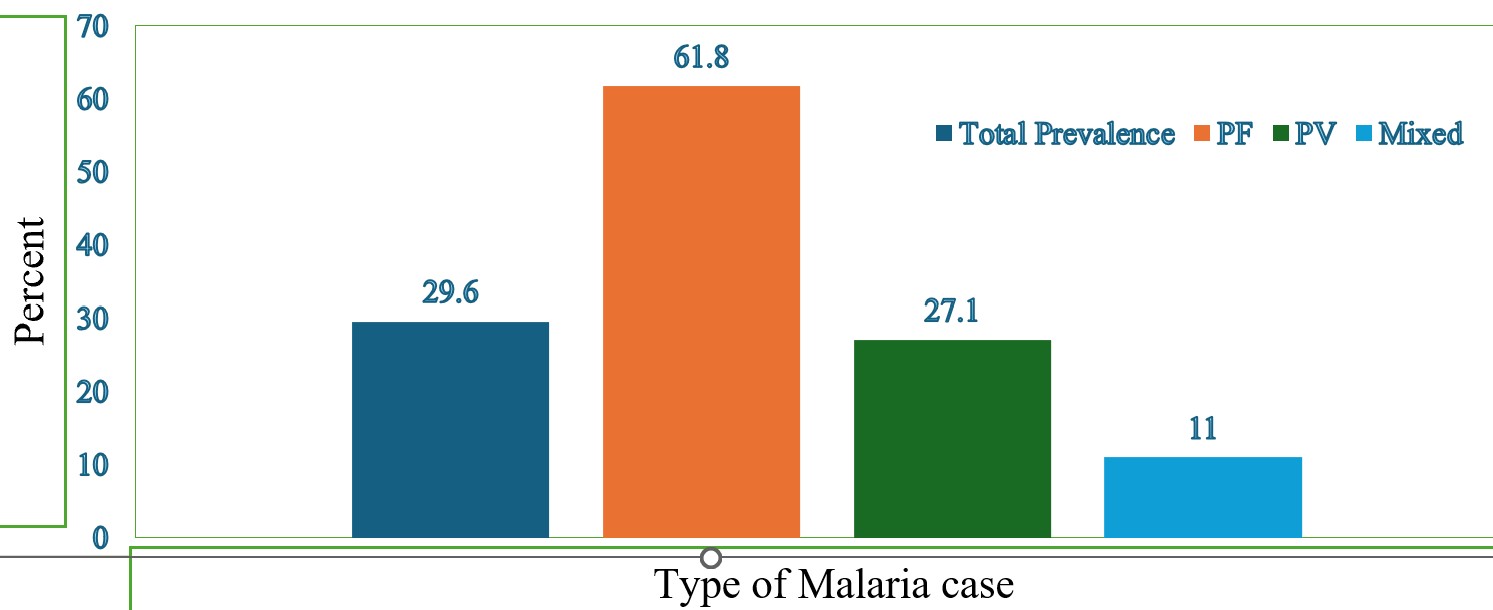
The study included a total of 398 individuals, with ages ranging from 18 to 69 years. The mean age was 29 years, with a standard deviation of approximately ±10.9 years. One hundred eighteen (118, 29.5%) of the 398 study participants had malaria parasite infections (Table 1), including 73 (61.8%) with Plasmodium falciparum, 32 (27.11%) with Plasmodium vivax, and 13 (11%) with both (Figure 1).
Possible risk factors for malaria infection
In this regard, the risk of malaria infection was four times greater in men (aOR = 4.1; 95%CI: 2.48 – 6.80). Rural living individuals are twice as likely as urban participants to have a malaria incidence (aOR=2.2; 95%CI: 1.33-3.50, Table 2). Those individuals using ITNs are 42% less likely to be infected by malaria than those who are not using it, with (aOR=0.6; 95%CI: 0.33 – 0.92), and participants whose house had IRS within the last six to twelve months are 85.7% less likely to acquire malaria than those who did not have IRS at their home with (aOR=0.1, 95%CI: 0.12 – 0.52). According to this study, those who live less than 1 km from mosquito larval breeding areas have an increased risk of contracting malaria by 1.8 times compared to those who live farther away (aOR=1.8; 95%CI: 1.11 – 3.32). The quantitative survey found that 29.4% of participants had travelled recently. In the overall sample, recent travel history was associated with higher odds of malaria infection (aOR=2.1; 95% CI: 1.33–3.42) compared to non-travellers. To specifically assess cross-border risk, we analyzed the subset of travellers (n=117). Among them, the prevalence of malaria was 48.1% in those who crossed into Sudan, compared to 28.6% in those who travelled only within Ethiopia. In a logistic regression model controlling for age and sex, cross-border travel to Sudan was associated with a 2.3-fold increased odds of malaria infection compared to domestic travel only (aOR = 2.3; 95%CI: 1.15– 4.61).
Entomological findings
A total of 191 Anopheles mosquito larvae were collected from six larval breeding habitats. The Anopheles larval density within each positive breeding site was calculated by counting the number of larvae per litre. High larval densities were found in the river margin, 91 (47.6%), and irrigation ditches, 49 (25.7%).
Anopheles species composition and abundance
A total of 212 female Anopheles mosquitoes were collected in Kurmuk district kebeles using Adult & larval collection methods. Among the collected mosquitoes, the highest number of Anopheles belonged to An. gambiae s.l.(49.5%), followed by An. pharoensis (26.4%), An. coustani s.l (20.7%), An. maculipalpis (2.8%), while the lowest density belonged to An. demeilloni (0.47%). The majority, 90.1% were collected from larval breeding habitats Table 3. The rest collected mosquitoes, 9.9% were from indoor collections using CDC light traps.
Community mobility and reason for travel
From the community’s perspective, the whole community, especially adults (>18 years( community travels more than other age groups. Merchants/marketers travel more than other individuals from Kurmuk district to other districts or across the Sudan border. Some key informants interviewed who identified as merchants were the most mobile in the community.
”…The most mobile group of people are merchants. They cross the border in quest of fresh markets, commodities to trade, and financial gain…”. (Trade office head)
“Other key informants were identified as religious personnel who travel and cross the Sudan border. ”… (religious leader)
“Religious people travelling are often a way to fulfil their spiritual obligations and deepen their faith…” religious leader
Locations of origin and next destination, most common destinations
Key informants in Kurmuk district pointed out that the places of origin of travellers are Asossa town, Metekel town, Kurmuk town, Horazeb kebele in Kurmuk district, Shetahul kebele in Kurmuk district, Hode kebele found in Kurmuk district, and Kamashi town, which are the starting points or origins of travel in the region
”….The places of origin for travel include Horazeb, Shetahul, Hode, and Asossa. These locations offer unique experiences and cultural insights for those who visit…”(transport office and health office head)
The most common next destination places were Kamashi Kurmuk Sudan and Asossa town.
”… Sudan, Kurmuk, and Asossa Town are all popular destinations for travellers seeking adventure and cultural immersion. Asossa Town, located in western Ethiopia, is a vibrant hub of culture and commerce….”(Community leaders)
Seasonal and temporal travel trends
Winter was reported as the highest season for travelling. On Thursdays and Sundays, the community movement convened frequently for marketing. They would congregate to sell their handcrafted wares and advance their cause at the neighbourhood farmer’s market.
“…Thursday and Sunday are the most popular days for crossing; it is also possible to cross on other days of the week with less traffic..” (Trade office head and HEW).
These two days are the busiest for border crossings, as many people travel to buy goods and products that are cheaper in the neighbouring country.
Directions of community travel
According to the key informants, there are various directions of travel in the study area. The major directions indicated by the key informants were from Kurmuk to Asossa, Kurmuk to Metekel, Ethiopian Kurmuk district to Kurmuk, Sudan, from Shetahul kebele to Horazeb kebele, located in Kurmuk district; from Kurmuk town to Horazeb kebele, which is the mining area; from the eastern part of the country to the western part, vice versa; and outside the country, from Sudan to Kurmuk district of Ethiopia, which is a point of entry.
”… Some individuals embark on journeys from Kurmuk to Asossa, while others travel from Kurmuk to Metekel. Additionally, some people make their way from Kurmuk to Sudan. These directions of travel highlight the interconnectedness of our district and the importance of transportation in facilitating movement and commerce….” (Transport office head)
The most common means/mode of transport
Key informants indicated that the most common means of transportation are by foot, vehicles such as motorcycles, mini-buses, buses and cars. Cars, buses, and mini -buses all qualify as modes of transportation.
“…Due to its smaller size and ability to fit through tight streets and alleyways, mini buses are ideal for smaller groups of people who want to travel together…”(Transport office Head and Health extension workers
Synthesis of travel patterns: Triangulating quantitative and qualitative data
The integration of quantitative and qualitative data reveals a consistent pattern of mobility linked to malaria risk. The quantitative survey found that 29.4% (117/398) of all participants had travelled recently. Among these travellers, the history of travel was a significant risk factor for malaria (AOR=2.093). The qualitative interviews with key informants provide context for this finding, identifying merchants/marketers and religious travellers as the most mobile groups and confirming Sudan as a primary destination. This synergy suggests that cross-border travel is a key behaviour underlying the high prevalence of malaria in Kurmuk.
Analysis of travel histories from the survey revealed that a significant proportion of the study participants were actively engaged in cross-border movement. Of the 117 participants with a recent travel history, 52 (44.4% of travellers, or 13.1% of the total study population) reported having crossed the border into Sudan within the past month. This quantitatively confirms that cross-border mobility is a common behaviour within our study population from Kurmuk district, justifying the focus on cross-border health.
To directly assess the risk associated with cross-border movement, we analyzed a subset of participants who reported any travel in the last 30 days (n=117). Among these travellers, those who reported crossing into Sudan had a significantly higher prevalence of malaria (48.1%) compared to those who travelled only within Ethiopia (28.6%). In a binary logistic regression model controlling for age and sex, cross-border travel to Sudan was associated with 2.3-fold increased odds of malaria infection compared to domestic travel only (AOR = 2.30; 95% CI: 1.15 – 4.58).
Malaria remains a significant public health challenge in Ethiopia, with transmission dynamics influenced by a complex interplay of factors including vector ecology, human behaviour, and environmental conditions. This study, conducted in the strategically important border district of Kurmuk, provides critical insights into the local epidemiology of malaria and identifies key drivers of transmission that extend beyond national borders. Specifically, the finding that travel history, especially cross-border movement, significantly increases malaria risk points to the role of imported infections. This pattern is supported by historical economic data [13] and epidemiological reports indicating that Eastern Sudan states experience sustained, high malaria transmission, establishing a scenario where frequent travel from high-transmission areas in Sudan to Kurmuk facilitates continuous parasite importation.
The observed malaria prevalence of 29.6% in our study population substantially exceeds national averages reported for Ethiopian adults, highlighting Kurmuk as a high-burden area requiring intensified interventions. The variation in prevalence compared to other studies in Ethiopia and sub-Saharan Africa [13-20] likely reflects differences in ecological settings, transmission seasons, and study methodologies. The predominance of Plasmodium falciparum (61.8%) aligns with national trends and underscores the continued challenge posed by this potentially fatal species.
Our multivariate analysis identified several significant risk factors that collectively paint a picture of malaria transmission dynamics in this border region. Male participants demonstrated a four-fold higher risk of malaria infection compared to females (AOR=4.132; 95% CI: 2.48-6.873), a finding consistent with multiple studies across Ethiopia [21-24]. This gender disparity likely reflects differential exposure patterns, with men more frequently engaged in outdoor occupations and nighttime activities that increase their contact with mosquito vectors.
The strong protective effects of both indoor residual spraying (IRS) and insecticide-treated net (ITN) use emphasize the continued importance of these core vector control interventions. Participants reporting IRS implementation within the previous 6-12 months showed an 85.7% reduction in malaria risk (AOR=0.143; 95% CI: 0.042-0.488), while ITN users experienced a 42% risk reduction (AOR=0.58; 95% CI: 0.339-0.992). These findings are supported by studies from Nigeria, Sudan, and various Ethiopian regions [25-29], confirming that proper implementation of these interventions remains crucial for malaria control.
Environmental and behavioral factors further contributed to transmission risk. Rural residents faced twice the risk of urban dwellers (AOR=2.139; 95% CI: 1.310-3.492), consistent with findings from Togo, Nigeria, and other Ethiopian studies [30-32]. This urban-rural disparity likely reflects differences in housing quality, environmental management, and proximity to breeding sites. Indeed, participants living within 1 km of mosquito breeding habitats demonstrated a 1.8-fold increased risk (AOR=1.878; 95% CI: 1.081-3.262), corroborating evidence from multiple settings [28,33-35] that proximity to larval habitats significantly enhances exposure risk.
The integration of entomological and human mobility data provides particularly valuable insights for understanding cross-border transmission dynamics. The predominance of An. gambiae s.l. (49.5%) as the primary vector aligns with findings from Burkina Faso, Gambella, and Asossa district, Ethiopia [36-38], confirming the presence of efficient malaria vectors in the region. Crucially, our study demonstrates that human mobility significantly drives transmission, with recent travellers showing twice the infection risk of non-travellers (AOR=2.093; 95% CI: 1.288-3.401). This finding is consistent with a meta-analysis of sub-Saharan African studies [39] and other Ethiopian research [21,23], highlighting travel as a major contributor to malaria epidemiology.
The triangulation of quantitative and qualitative data strengthens our understanding of how mobility patterns fuel transmission. The quantitative finding that travelers face elevated risk is contextualized by qualitative interviews identifying merchants and marketers as the most mobile group, frequently crossing into Sudan for trade. This pattern is supported by historical economic data [12] describing Kurmuk as a traditional cross-border market hub. The convergence of these data streams suggests that a substantial portion of malaria burden in Kurmuk relates to transmission networks extending across the Ethiopia-Sudan border.
The high prevalence of malaria (29.6%), coupled with the finding that over half of the positive cases had a recent travel history and the qualitative data identifying Sudan as a common destination for merchants, suggests that human mobility is a key driver of malaria in Kurmuk. Furthermore, the qualitative report of increased travel in the dry season/winter aligns with the timing of our data collection (December-February), potentially capturing a peak transmission risk facilitated by movement. The qualitative findings identified the dry season (approximately November to February, locally referred to as “winter”) as the period of most frequent cross-border travel, primarily for commerce. Our study was conducted during this exact high-mobility season (December to February). The high malaria prevalence (29.6%) we observed likely reflects an elevated transmission intensity fueled by this seasonal surge in human movement. This synchronicity suggests that the dry season is a critical window for malaria transmission in this border region, primarily due to human mobility patterns that facilitate parasite importation and spread, rather than climatic factors favoring mosquito breeding.
Among environmental factors, proximity to anopheline breeding habitats was a significant predictor of infection, consistent with the known ecology of major vectors like An. gambiae s.l. This finding underscores the critical role of local aquatic habitats in sustaining transmission. The district’s hot tropical climate, riverine landscape, and irrigation ditches create perennial breeding opportunities, making environmental management a vital complementary strategy to human-targeted interventions.
The triangulation of data provides compelling evidence for the role of human mobility. The high prevalence of malaria (29.6%), the significant association between recent travel and infection (aOR=2.1), and the qualitative identification of frequent cross-border travel for trade collectively indicate that a substantial portion of the malaria burden in Kurmuk is sustained by the importation of parasites through human movement, particularly across the border with Sudan.
Limitations of the study
This study has limitations that should be considered when interpreting the findings. First, the collection during a single season precludes assessment of seasonal variations in malaria transmission. Second, key behavioural data, such as bednet ownership and use, relied on self-reporting without independent verification, potentially introducing recall or social desirability bias. Third, while microscopy remains the standard for clinical malaria diagnosis in Ethiopia, its use without molecular confirmation (e.g., PCR) may have resulted in underestimation of true prevalence due to undetected low-parasite-density and subclinical infections. Fourth, the entomological investigation did not include insecticide resistance testing for key vectors such as An. stephensi, limiting the evaluation of potential resistance-driven transmission dynamics. Further research incorporating longitudinal monitoring, molecular diagnostics, and vector resistance profiling is needed to better understand transmission dynamics and optimize intervention strategies in this border region.
Fifth, the health facility‑based sampling may introduce selection bias. Participants seeking care at health centres likely differ from the general population they are symptomatic, have higher health‑seeking behaviour, and may overestimate true malaria prevalence. Findings are therefore not generalizable to asymptomatic or non‑care‑seeking adults in the community. Future studies should incorporate community‑based surveys to validate these findings.
This study reveals a high and persistent malaria burden in the Kurmuk border district, with a prevalence of 29.6% that starkly contrasts with Ethiopia’s national elimination targets.
The key drivers of this burden were identified through the triangulation of quantitative and qualitative data. Travel history particularly cross-border movement to Sudan by merchants emerged as a primary driver of transmission, confirming human mobility as a central factor. This risk is compounded by intense local transmission of P. falciparum by the dominant vector An. gambiae s.l., alongside suboptimal coverage and utilization of protective measures such as LLINs and IRS. The typical risk profile a mobile adult male residing in a rural area near mosquito breeding sites highlights a specific population acting as a conduit for malaria importation and sustained transmission.
These findings carry important implications for malaria control strategy. They underscore that in strategic border regions like Kurmuk, standard interventions alone are insufficient. Transmission is sustained through a combination of cross-border importation and localized ecological factors, presenting a distinct threat to national elimination progress.
Therefore, achieving elimination in this region requires targeted, collaborative recommendations. Success hinges on; enhancing cross-border surveillance and data-sharing mechanisms with Sudan; providing tailored health education and access to chemoprophylaxis for high-risk travelers such as merchants; and intensifying efforts to improve the coverage, quality, and utilization of LLINs and IRS. Addressing the complex interplay between human mobility and vector ecology is paramount for safeguarding national and regional health security.
What is already known about the topic
What this study adds
We would like to express our heartfelt appreciation to the School of Public Health at St. Paul’s Hospital Millennium Medical College for their unwavering support for this research. Next, We’d like to express our heartfelt gratitude to the CDC POPCAB mini-grant project for providing us with funding to perform this study.
ZO: Conceptualization, formal analysis, investigation, methodology, project administration,
supervision, writing – original draft; SS: Conceptualization, data curation, supervision, validation; TK: Conceptualization, funding acquisition, supervision and validation; SK: Data curation and investigation; FH: Writing – review & editing; HE: Conceptualization and supervision; EF: Conceptualization, data curation; SZ: Validation, visualization, writing – review & editing; CC: Writing – original draft; MN: Resources and visualization.
| Variable | Positive malaria | Negative Malaria | Total | Percentage (%) |
|---|---|---|---|---|
| Age (years) | ||||
| <25 | 51 | 97 | 148 | 37.2 |
| 25–34 | 41 | 93 | 134 | 33.7 |
| 35–44 | 17 | 54 | 71 | 17.8 |
| 45–54 | 7 | 22 | 29 | 7.3 |
| >54 | 2 | 14 | 16 | 4.0 |
| Sex | ||||
| Male | 86 | 125 | 211 | 53.0 |
| Female | 32 | 155 | 187 | 47.0 |
| Religion | ||||
| Protestant | 3 | 6 | 9 | 2.3 |
| Orthodox | 4 | 13 | 17 | 4.3 |
| Catholic | 3 | 7 | 10 | 2.5 |
| Muslim | 108 | 254 | 362 | 91.0 |
| Educational status | ||||
| Illiterate | 75 | 199 | 274 | 68.8 |
| Literate | 43 | 81 | 124 | 31.2 |
| Family size | ||||
| <5 | 106 | 256 | 362 | 91.0 |
| ≥5 | 12 | 24 | 36 | 9.0 |
| Marital status | ||||
| Single | 10 | 77 | 87 | 21.9 |
| Married | 105 | 186 | 291 | 73.1 |
| Divorced | 1 | 12 | 13 | 3.3 |
| Widowed | 2 | 5 | 7 | 1.8 |
| Residency | ||||
| Urban | 61 | 110 | 171 | 43.0 |
| Rural | 57 | 170 | 227 | 57.0 |
| Variable | Malaria Positive (%) | Malaria Negative (%) | COR (95% CI) | AOR (95% CI) | P value |
|---|---|---|---|---|---|
| Sex (ref: Female) | |||||
| Male | 86 (40.8) | 125 (59.2) | 3.33 (2.08–5.32) | 4.13 (2.48–6.87) | <0.001 |
| Female | 32 (17.1) | 155 (82.9) | 1.00 | 1.00 | |
| Place of residence (ref: Urban) | |||||
| Rural | 61 (35.7) | 110 (64.3) | 1.65 (1.07–2.55) | 2.14 (1.31–3.49) | 0.002 |
| Urban | 57 (25.1) | 170 (74.9) | 1.00 | 1.00 | |
| IRS done within last 6–12 months (ref: No) | |||||
| Yes | 3 (7.0) | 40 (93.0) | 0.16 (0.05–0.52) | 0.14 (0.04–0.49) | 0.002 |
| No | 115 (32.4) | 240 (67.6) | 1.00 | 1.00 | |
| ITN utilized (ref: No) | |||||
| Yes | 29 (20.7) | 111 (79.3) | 0.50 (0.31–0.80) | 0.58 (0.34–0.99) | 0.047 |
| No | 89 (34.5) | 169 (65.5) | 1.00 | 1.00 | |
| Distance from breeding sites (ref: >1 km) | |||||
| ≤1 km | 92 (34.7) | 173 (65.3) | 2.19 (1.33–3.60) | 1.88 (1.08–3.26) | 0.025 |
| >1 km | 26 (19.5) | 107 (80.5) | 1.00 | 1.00 | |
| Outdoor activities (ref: No) | |||||
| Yes | 103 (31.1) | 228 (68.9) | 1.55 (0.84–2.86) | 1.37 (0.68–2.73) | 0.377 |
| No | 15 (22.4) | 52 (77.6) | 1.00 | 1.00 | |
| Travel history within 30 days (ref: No) | |||||
| Yes | 68 (37.8) | 112 (62.2) | 2.04 (1.32–3.15) | 2.09 (1.29–3.40) | 0.003 |
| No | 50 (22.9) | 168 (77.1) | 1.00 | 1.00 | |
| Education (ref: Literate) | |||||
| Illiterate | 75 (27.4) | 199 (72.6) | 0.71 (0.45–1.12) | 0.77 (0.46–1.27) | 0.302 |
| Literate | 43 (34.7) | 81 (65.3) | 1.00 | 1.00 | |
| Abbreviations: COR = Crude Odds Ratio; AOR = Adjusted Odds Ratio (adjusted for all variables in the table); CI = Confidence Interval; IRS = Indoor Residual Spraying; ITN = Insecticide Treated Net | |||||
| Breeding site | No. of dips | No. of +ve dips | Larval density | Dipper index | Species density | |||
|---|---|---|---|---|---|---|---|---|
| An. Gambiae s.l | An. coustani | An. maculipalpis | An. pharoensis | |||||
| Canal with vegetation | 10 | 2 | 28 (14.7%) | 20 | 32.1 | 7.1 | 0 | 60.7 |
| Fresh water pool | 8 | 1 | 5 (2.6%) | 12.5 | 60 | 0 | 20 | 20 |
| River margin | 10 | 7 | 91 (47.6%) | 70 | 40.7 | 25.3 | 2.2 | 30.8 |
| Discarded tire | 3 | 1 | 18 (9.4%) | 33.3 | 27.7 | 16.6 | 5.5 | 50 |
| Plastic container | 1 | 0 | 0 (0%) | 0 | 0 | 0 | 1.1 | 0 |
| Irrigation ditch | 7 | 5 | 49 (25.7%) | 71.4 | 63.2 | 32.6 | 2.0 | 2.0 |