Research | Open Access | Volume 9 (2): Article 70 | Published: 29 Apr 2026

Views: 1,024
Menu, Tables and Figures
| Variables | Frequency (n) | Percentage (%) |
|---|---|---|
| Mother’s level of education | ||
| No formal | 211 | 47.1 |
| Primary | 111 | 24.8 |
| Secondary and higher | 126 | 28.1 |
| Mother’s marital status | ||
| Single | 14 | 3.1 |
| Married | 434 | 96.9 |
| Mother’s religion | ||
| Traditional and other | 83 | 18.5 |
| Christian | 253 | 56.5 |
| Islam | 112 | 25.0 |
| Mother’s Occupation | ||
| No | 42 | 9.4 |
| Yes | 406 | 90.6 |
| Age of youngest child (in months) | ||
| <12 | 125 | 27.9 |
| 12-23 | 125 | 27.9 |
| ≥24 | 198 | 44.2 |
| Sex of youngest child | ||
| Female | 219 | 48.9 |
| Male | 229 | 51.1 |
| Rank of youngest child | ||
| 1 | 100 | 22.3 |
| 2 | 125 | 27.9 |
| ≥3 | 223 | 49.8 |
| Mother’s knowledge of High-Impact Community-Based Intervention Packages | ||
| No | 311 | 69.4 |
| Yes | 137 | 30.6 |
| Knowledge of CR number | ||
| No | 416 | 92.9 |
| Yes | 32 | 7.1 |
| Awareness of CR services | ||
| No | 208 | 46.4 |
| Yes | 240 | 53.6 |
| Household size | ||
| ≤5 | 283 | 63.2 |
| >5 | 165 | 36.8 |
| Number of children under 5 | ||
| 1 | 263 | 58.7 |
| 2 | 157 | 35.0 |
| ≥3 | 28 | 6.3 |
| Region | ||
| North | 160 | 35.7 |
| Central | 121 | 27.0 |
| South | 167 | 37.3 |
CR: Communauty Relay
Rank of youngest child: rank of youngest child in the fraternity
Knowledge of CR number: knowledge of the telephone number of a community relay
Table 1: Sociodemographic characteristics of mothers of children under five , Benin, 2022 (n = 448)
| Variables | Community relay services (n) | cOR | 95% CI | p | |
|---|---|---|---|---|---|
| Non-use | Use | ||||
| Mother’s level of education | |||||
| Uneducated/literate | 112 | 99 | 1.0 | ||
| Primary | 65 | 46 | 1.3 | 0.8 – 2.0 | 0.348 |
| Secondary and higher | 72 | 54 | 1.2 | 0.8 – 1.8 | 0.469 |
| Mother’s marital status | |||||
| Single | 7 | 7 | 1.0 | ||
| Married | 242 | 192 | 1.3 | 0.4 – 3.7 | 0.670 |
| Mother’s religion | |||||
| Traditional and other | 51 | 32 | 2.6 | 1.4 – 4.6 | 0.002 |
| Christian | 155 | 98 | 2.5 | 1.6 – 4.0 | <0.001 |
| Islam | 43 | 69 | 1.0 | ||
| Mother’s occupation | |||||
| No | 27 | 15 | 1.5 | 0.8 – 2.9 | 0.235 |
| Yes | 222 | 184 | 1.0 | ||
| Age of youngest child (months) | |||||
| <12 | 72 | 53 | 1.0 | 0.7 – 1.6 | 0.855 |
| 12-23 | 65 | 60 | 0.8 | 0.5 – 1.3 | 0.422 |
| ≥24 | 112 | 86 | 1.0 | ||
| Sex of youngest child | |||||
| Female | 115 | 104 | 1.0 | ||
| Male | 134 | 95 | 1.3 | 0.9 – 1.9 | 0.201 |
| Rank of youngest child | |||||
| 1 | 57 | 43 | 1.0 | ||
| 2 | 80 | 45 | 1.3 | 0.8 – 2.3 | 0.285 |
| ≥3 | 112 | 111 | 0.8 | 0.5 – 1.2 | 0.260 |
| Mother’s knowledge of PIHI Com. | |||||
| No | 206 | 105 | 4.3 | 2.8 – 6.6 | <0.001 |
| Yes | 43 | 94 | 1.0 | ||
| Knowledge of CR phone number | |||||
| No | 245 | 171 | 10.0 | 3.5 – 29.1 | <0.001 |
| Yes | 4 | 28 | 1.0 | ||
| Knowledge of CR services | |||||
| No | 195 | 13 | 51.7 | 27.3 – 97.8 | <0.001 |
| Yes | 54 | 186 | 1.0 | ||
| Alcohol consumption | |||||
| No | 155 | 124 | 1.0 | ||
| Yes | 94 | 75 | 1.0 | 0.7 – 1.5 | 0.989 |
| Tobacco consumption | |||||
| No | 227 | 171 | 1.0 | ||
| Yes | 22 | 28 | 0.6 | 0.3 – 1.1 | 0.083 |
| Untorn ITNs in household | |||||
| No | 32 | 35 | 1.0 | ||
| Yes | 217 | 164 | 1.5 | 0.9 – 2.4 | 0.164 |
| Availability of latrines with hand-washing facilities | |||||
| No | 232 | 182 | 1.3 | 0.6 – 2.6 | 0.497 |
| Yes | 17 | 17 | 1.0 | ||
| Household size | |||||
| ≤5 | 161 | 122 | 1.2 | 0.8 – 1.7 | 0.465 |
| >5 | 88 | 77 | 1.0 | ||
| Number of children under 5 | |||||
| 1 | 153 | 110 | 1.0 | ||
| 2 | 79 | 78 | 0.7 | 0.5 – 1.1 | 0.118 |
| ≥3 | 17 | 11 | 1.1 | 0.5 – 2.5 | 0.796 |
| Region | |||||
| North | 58 | 102 | 1.0 | ||
| Central | 86 | 35 | 4.3 | 2.6 – 7.2 | <0.001 |
| South | 105 | 62 | 3.0 | 1.5 – 5.9 | 0.003 |
Table 2: Bivariate analysis of non-use of Community Relay services by mothers of children under five, Benin, 2022
| Variables | aOR | 95% CI | p-value |
|---|---|---|---|
| Mother’s knowledge of PIHI Com | |||
| Yes (Reference) | 1.0 | – | – |
| No | 5.5 | 2.7 – 11.1 | <0.001 |
| Knowledge of CR services | |||
| Yes (Reference) | 1.0 | – | – |
| No | 46.7 | 23.6 – 92.3 | <0.001 |
| Region | |||
| North (Reference) | 1.0 | – | – |
| Central | 3.5 | 1.7 – 7.3 | 0.001 |
| South | 2.9 | 1.5 – 5.9 | 0.003 |
Table 3: Factors associated with non-use of Community Relay services by mothers of children under five, Benin, 2022

Kougbessi Gélase Atiogbe1,&, Nicolas Gaffan1, Emmanuel Ghislain Sopoh1, Edgard-Marius Ouendo1
1Regional Public Health Institute, University of Abomey-Calavi, Ouidah, Benin
&Corresponding author: Kougbessi Gélase Atiogbe, Regional Public Health Institute – University of Abomey-Calavi, Ouidah, Benin, Email: atigel2002@yahoo.fr ORCID: https://orcid.org/0009-0005-5726-2890
Received: 20 Aug 2025, Accepted: 24 Apr 2026, Published: 29 Apr 2026
Domain: Health Management
Keywords: Healthcare service, children under, community relay, Benin
©Kougbessi Gélase Atiogbe et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Kougbessi Gélase Atiogbe et al., Factors associated with the underutilization of Community Relay Healthcare Services by mothers in Benin. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):69. https://doi.org/10.37432/jieph-d-25-00175
Introduction: A community relay is a volunteer from the local community trained to raise awareness, provide advice, and support people by promoting health and access to healthcare services. Their role is critical in facilitating access to primary healthcare in Benin, especially in rural areas with limited health infrastructure. However, the use of their services remains suboptimal despite efforts by the Ministry of Health to strengthen their capacity, motivation, equipment, and to integrate them into health programs to improve their performance in the field. This study determined factors associated with the non-use of healthcare services provided by Community Relays.
Methods: A cross-sectional study was conducted among 448 mothers of children under five in areas covered by the High-Impact Community-Based Interventions Package (PIHI Com) selected using simple random sampling. A multistage random sampling method was used to select the participants. The data were collected using a digital form administered by investigators and analysed using logistic regression.
Results: Among the mothers surveyed, 55.6% (249/448) reported not using community relay services. Multivariate analysis revealed that not using these services was significantly associated with a lack of awareness (adjusted OR = 5.5; 95% CI: 2.7–11.1) of the PIHI Com program and the services provided by community relays. Additionally, mothers living in the central (aOR= 3.5, 95%CI = 1.7-7.3) or southern (aOR = 2.9, 95%CI = 1.5-5.9) regions were less likely to use these services than those living in the northern region.
Conclusion: Enhancing communication strategies and aligning services with local needs may increase the utilization of community-based services, ultimately contributing to the reduction of maternal and child mortality.
Strengthening healthcare systems is fundamental to achieving universal health coverage, as it ensures efficient, sustainable, and equitable delivery of health services [1–3]. In response to persistent shortages and unequal distribution of human resources for health, task-shifting from professional health workers to community health workers (CHWs) has been increasingly promoted as an effective strategy to improve primary healthcare delivery [4,5]. Since the Alma-Ata Declaration, CHWs have been recognised as essential intermediaries between communities and formal health systems [6].
In Benin, child mortality remains high, with 55 deaths per 1,000 live births before age one and 125 before age five [7]. The country also faces a severe shortage of qualified health professionals, with only 9 per 10,000 inhabitants compared to the WHO-recommended threshold of 23, alongside a health service utilisation rate of 61.3% [8]. To address these challenges, the Ministry of Health has progressively implemented the High-Impact Community-Based Intervention Package (PIHI Com) since 2011, focusing on evidence-based interventions to reduce maternal, neonatal, and child mortality [9].
The PIHI Com comprises scientifically proven interventions delivered nationwide through two components: the basic high-impact package of interventions and the complementary high-impact package of interventions, in addition to routine health facility activities [10]. At the community level, PIHI Com includes interventions targeting childhood illness management, hygiene and nutrition promotion, and improved access to preventive and curative care.
With support from the West African Health Organization (WAHO), Benin documented the community-level implementation of PIHI in 2014, identifying promising practices for dissemination across ECOWAS countries. Community relays were introduced to extend health services to households, particularly in remote and underserved areas [11]. They play a central role in PIHI Com by supporting disease prevention and treatment, promoting health behaviours, conducting awareness activities, collecting health data, and strengthening links between communities and health facilities [12,13].
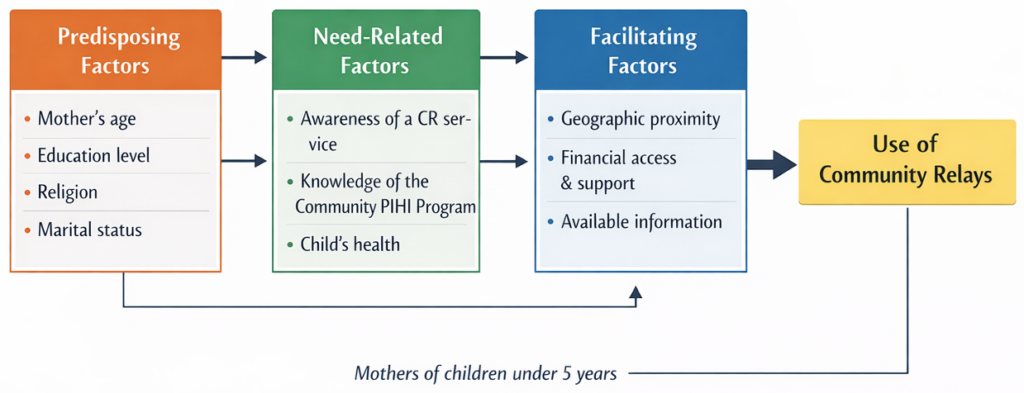
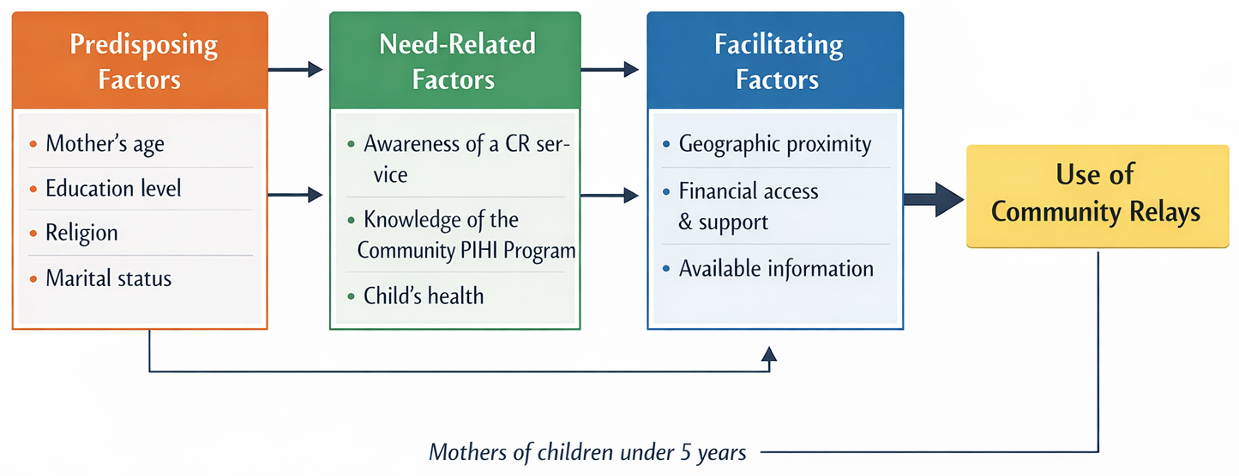
Despite the availability of community-based health services through PIHI Com, barriers to the utilisation of services provided by community relays persist. The lack of empirical evidence on factors influencing service use limits informed and context-sensitive policy development. This study, therefore, determined factors associated with the use of community relay healthcare services by mothers of children aged 0 to 5 years. The conceptual framework guiding the study, drawing on Andersen’s Behavioral Model of Health Services Use and highlighting the role of community relays in facilitating access to and utilization of health services within the study setting.
Study design and setting
This study employed a cross-sectional design. The study was conducted in the PIHI Com intervention zones in Benin. More broadly, Benin is a country in the West African sub-region, covering an area of 114,763 km² [14]. In administrative terms, Benin is divided into twelve departments, which constitute the highest administrative level of the country: Alibori, Atacora, Atlantique, Borgou, Collines, Couffo, Donga, Littoral, Mono, Ouémé, Plateau, and Zou. These departments are further subdivided into 77 communes (municipalities) [14]. Three of which have a special status (Cotonou, Porto-Novo, and Parakou) due to their highly urbanized character. The 77 communes are divided into 546 arrondissements (sub-municipal administrative units), comprising a total of 5,295 villages and neighbourhoods (Figure 1) [14]. All departments, except Couffo, were included in the PIHI Com program, which was implemented in specific localities of each county. The study’s implementation was guided by Andersen’s model (Figure 2)
Study population
The study population included mothers with at least one child aged less than five years who had been residing for at least two years in the PIHI Com intervention zones in Benin. The mothers who had declined to provide consent were excluded.
Sampling procedure
A multistage random sampling strategy was employed.
Sampling of the village: Benin’s administrative structure is composed of departments, communes (municipalities), arrondissements (sub-municipal administrative units), and villages/neighborhoods. Within each department, a simple random selection of one commune that had benefited from PIHI Com interventions was conducted. This selection was based on the mapping of PIHI Com interventions and implementing partners. The Couffo department was excluded from the study because it had not benefited from PIHI Com interventions. Subsequently, within each selected commune, one arrondissement was randomly selected, followed by the random selection of one village or one urban neighbourhood. In total, eleven villages or urban neighbourhoods were selected: Arbonga, Koutatiegou, Zoungbomè, Bonkora, Gbowele, Kodowari, Kowegbo, Doguia, Tanzoun, Okoffin, and Hounviguèli.
Sampling of participants: In each village/neighbourhood, the houses to be visited were selected using random route sampling. The random walk method was used because the community context did not allow for a comprehensive and up-to-date household survey. This method involves choosing a random starting point within a defined area, then following a predefined route (for example, moving in a randomly chosen direction) and selecting households at fixed intervals—such as every 3rd or 5th dwelling. Within each selected household, one eligible participant is then chosen using a simple rule. Standardized procedures were applied to limit selection bias. In each selected house, all mothers with at least one child under five were eligible to participate. If an eligible mother was absent from home, no replacement was made, and the survey continued with the next household according to the defined route. The data collectors then continued visiting houses sequentially until the target number of participants was reached in each village or city district. The minimum sample size was estimated using Schwartz’s formula, assuming a prevalence of 50%, a 5% margin of error, and a 95% confidence level [15]. The sample size calculation determined that a minimum of 385 people should be surveyed. To anticipate potential losses due to incorrectly completed, incomplete, or unusable questionnaires, 50 additional individuals were surveyed. Therefore, the target was to survey at least 435 mothers, which equates to an average of around 40 mothers per village. Ultimately, a total of 448 mothers were included in the study.
Variables
Dependent variable
The dependent variable was the utilization of community relay (CR) services by mothers of children under five. A mother was considered to have used CR services if she had either received a visit from a community relay during the three months preceding the survey, as part of routine home visits, or if she had sought CR services the last time her child was ill. This outcome was coded as a binary variable, with “0” indicating use of CR services and “1” indicating non-use.
Independent variables
The independent variables considered in this study covered sociodemographic, behavioural, and household characteristics. Maternal characteristics were education level (no formal education, primary, secondary or higher), marital status (single, married), religion (traditional and other, Christianity, Islam), profession (yes, no), and alcohol or tobacco consumption (yes, no). Child-related variables included the age of the youngest child in months (<12, 12–23, ≥24), sex of the youngest child (female, male), and birth rank (1, 2, ≥3). Knowledge-related factors encompassed the mother’s awareness of the PIHI Com program (yes, no), knowledge of a community relay’s phone number (yes, no), and knowledge of available CR services (yes, no). Household and environmental variables included the presence of untorn insecticide-treated bed nets (ITNs) (yes, no), the availability of a latrine with a handwashing facility (yes, no), household size (≤5, >5), number of children under five (1, 2, ≥3), and region of residence (south, center, north).
Collecting and processing data
Prior to data collection, survey agents and supervisors received training on the study context, objectives, and data collection procedures. The questionnaire was adapted from validated instruments, the Demographic and Health Surveys (DHS) and Multiple Indicator Cluster Surveys (MICS), and has been contextualised to the study with specific items on community health workers [7]. The structured digital form comprised sections on the sociodemographic, behavioural, and household characteristics. It was designed and deployed using Kobo Toolbox. The form was delivered by specially trained investigators. A pretest was conducted to ensure clarity and relevance of the tool with 20 households not included in the final sample, which allowed for refinement and finalisation of the data collection instrument.
Data analysis
Statistical analyses were performed using STATA software, version 15. Quantitative variables were summarized as means with standard deviations when normally distributed, and as medians with interquartile ranges when distributions were skewed. Categorical variables were described using frequencies and percentages. To identify factors associated with non-use of CR services, bivariate logistic regression analyses were first performed. Variables with a p-value < 0.20 in the bivariate analysis were subsequently entered into a multivariate logistic regression model. A stepwise backward selection procedure was applied to retain variables with a significance threshold of 5%. Model validity and performance were assessed through multicollinearity diagnostics, the likelihood ratio test, the Hosmer–Lemeshow goodness-of-fit test, classification tables (confusion matrix), and receiver operating characteristic (ROC) curve analysis with estimation of the area under the curve (AUC). Results are presented in tables and figures.
Ethical considerations
The study received approval No. 530/CLERB-UP/P/SP/R/SA from the Local Ethics Committee for Biomedical Research of the University of Parakou, Benin. Administrative authorizations were obtained prior to the commencement of the study. Ethical standards were strictly adhered to, including measures to ensure anonymity and confidentiality. A detailed information sheet was provided to all potential participants, and verbal informed consent was obtained individually before data collection. Consent was obtained using a form designed for this purpose, duly signed by the respondents. Those who could not read or write received an explanation from the investigator and had their signature replaced by their fingerprint.
Basic characteristics of the study population
A total of 448 mothers of children under five were enrolled in the study (Table 1). Nearly half of the participants (47.1%, 211/448) had no formal education. The majority were married (96.9%), and more than half identified as Christian (56.5%). The mean age of the children was 22.3 ± 14.5 months, while the mean age of the mothers was 27.3 ± 5.7 years. Regarding behavioural and knowledge-related characteristics, less than one-third of mothers (30.6%) were aware of the PIHI Com program, and only 7.1% reported knowing the telephone number of a community relay. Just over half (53.6%) were able to identify at least one service provided by the community relays. By region, 37.3% resided in the southern part of the country, 27.0% in the central region, and 35.7% in the north.
Among the mothers surveyed, 55.6% (249/448) reported not using community relay services. The bivariate analysis examined the association between each independent variable and the non-use of community relay (CR) services. Mothers practicing traditional religions and other (OR = 2.6, 95% CI: 1.4–4.6) and Christianity (OR = 2.5, 95% CI: 1.6–4.0) were more likely not to use CR services compared to Muslim mothers. Lack of knowledge of the PIHI Com program (OR = 4.3, 95% CI: 2.8–6.6), unawareness of a CR’s phone number (OR = 10.0, 95% CI: 3.5–29.1), and unfamiliarity with CR services (OR = 51.7, 95% CI: 27.3–97.8) were associated with non-use. Regionally, mothers residing in the central (OR = 4.3, 95% CI: 2.6–7.2) and southern (OR = 3.0, 95% CI: 1.5–5.9) regions were less likely to use CR services than those in the north (Table 2).
In the adjusted model, three factors remained significantly associated with the non-use of CR services (Table 3). Mothers with limited knowledge of the PIHI Com program were less likely not to use CR services. Specifically, mothers who reported being aware of the program but could not name any PIHI service were 5.5 times less likely to not use CR services (adjusted OR = 5.5; 95% CI: 2.7–11.1). Similarly, mothers unable to identify at least one service provided by a community relay were at substantially higher risk of non-use (adjusted OR = 46.7, 95% CI: 23.6–92.3). Additionally, residing in the central (adjusted OR = 3.5, 95% CI: 1.7–7.3) or southern regions (adjusted OR = 2.9, 95% CI: 1.5–5.9) was associated with higher odds of non-use compared to the northern region.
Model Diagnostics and Validation
Multicollinearity Assessment
Multicollinearity among variables was assessed using the Variance Inflation Factor (VIF). Three variables (religion, knowledge of at least one community relay service, and awareness of the Community PIHI program) are not collinear, as all VIF values were below 5.
Likelihood ratio test
The regression table shows that the probability associated with the likelihood ratio test statistic is statistically significant (p-value < 0.05), indicating that the model is globally significant. Additionally, the model presents a moderate pseudo R² (49.04%), which, although of limited interpretability, suggests acceptable explanatory power.
Hosmer–Lemeshow Goodness-of-Fit Test
The model fits the data well, as the p-value is greater than 0.05.
Confusion Matrix / Classification Table
The classification table summarizes the model’s ability to correctly classify observations using a 0.5 threshold, by comparing the predicted values (classified) from the logistic model with the observed values (true). The model correctly predicted 85.0% of individuals in their original group. It also demonstrates a good balance between sensitivity (78.3%) and specificity (93.5%).
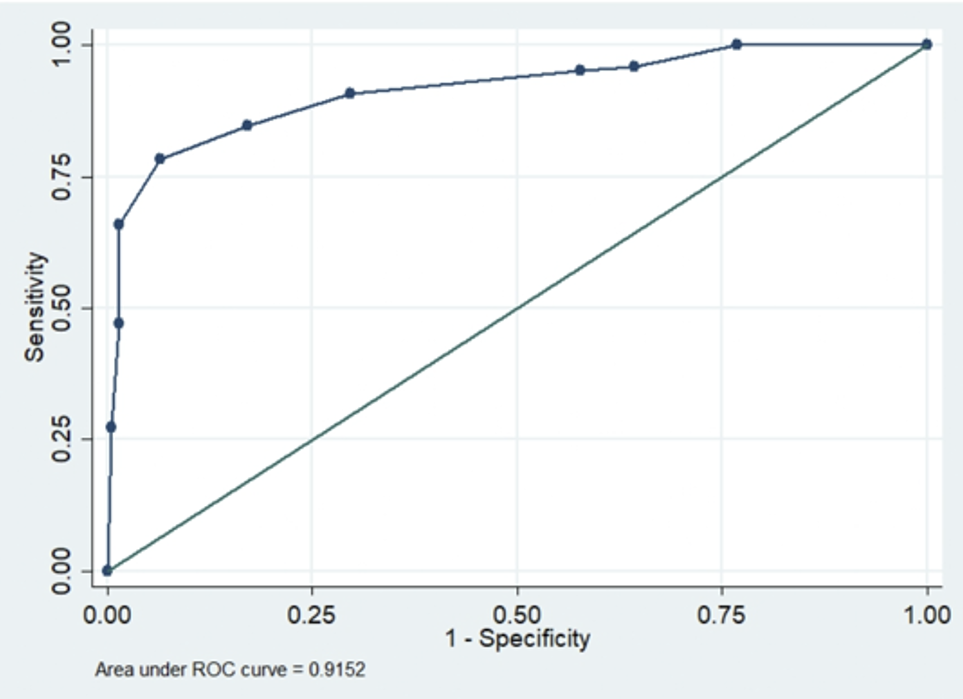
ROC Curve and Area Under the Curve (AUC)
The ROC curve allows visualisation of the model’s ability to discriminate between the two groups of the dependent variable. The area under the curve (AUC) provides a measure of this discriminative ability. In this analysis, the AUC is 0.915, which is greater than 0.9, indicating excellent discrimination between the two groups (Figure 3). Overall, these diagnostics indicate that the model is adequate and can be reliably used for the interpretation of results.
We found that mothers who had never heard of the PIHI Com program or were unable to name at least one service provided by community relays were significantly less likely to utilize their services. This situation suggests that mere exposure to the program does not guarantee effective uptake of its services. Limited or superficial knowledge of the PIHI Com content may hinder understanding of the role of community relays, reduce the perceived usefulness of the services offered, and consequently limit their utilization. These findings highlight persistent challenges related to communication and awareness surrounding community health interventions.
According to the definition by Renaud (2020), health communication is “a strategic intervention to improve health through planned activities aimed at changing individual behaviors and modifying the physical, economic, and social environment [16].” This concept is central to the successful implementation of community-based initiatives. In this context, a study by Lokossou et al. (2019) demonstrated a progressive improvement in community relay performance and key health indicators between 2010 and 2014, as these actors increasingly engaged in educational sessions and promoted the PIHI Com interventions [17]. This suggests that consistent communication and gradual community familiarization with both the PIHI Com program and the role of community relays may enhance service uptake and integration.
Similarly, a World Health Organization (2021) framework on health systems’ contribution to health security emphasizes the lack of awareness and communication regarding the importance of health systems among decision-makers, policymakers, and communities [18]. This reinforces our finding that strengthening communication efforts is critical to enhancing community engagement and uptake of health services.
Studies by Fourn et al. (2001) have shown that underutilization of healthcare services in rural areas may also be due to the limited availability of services at times that are convenient for the population [19]. For instance, farmers often leave home early, before services open, and return late, after facilities are closed. While this factor was not directly observed in our study, differences in service accessibility may partly explain why mothers did not use community relay services, depending on the point of care referenced.
Moreover, our study found that mothers residing in the central and southern regions of Benin were significantly less likely to use CR services than those in the north. This geographical disparity may be explained by differences in the intensity of program implementation, the availability and visibility of community relays (CRs), or the presence of alternative, more accessible healthcare services in certain areas. Conversely, in northern regions, which are often characterized by more limited formal healthcare services, CRs may play a more central role and be more frequently utilized by communities. This may be attributed to the greater concentration of health centers and hospitals in the south and center, which might lead mothers to bypass community relays in favor of more formal health structures. Additionally, the relatively urban context of southern and central areas may contribute to a weaker integration of CRs within the community health framework. In the scientific literature, Ahmed et al found that, in urban settings, ASCs reported more difficulties in engaging with and gaining people’s trust due to the absence of clear community leadership, a busy lifestyle, large-scale employment trends, and the availability of private healthcare professionals [20].
To foster stronger links between community members and CRs, it is important to encourage participatory health promotion approaches. Communities should be supported in conducting their own health diagnoses to identify the changes needed to improve collective health outcomes. A study by Okuga et al. (2015) in Uganda showed that CRs were highly valued by their communities and considered important contributors to maternal and neonatal health at the local level [21]. Adapted the implementation of relational actions to regional realities to enable equity of action.
Limitations
This study has some limitations. Due to its cross-sectional design, it does not allow the establishment of a causal relationship between the identified factors and the outcome. Despite efforts to standardize the procedures, the random walk approach may limit the representativeness of participants in the sample. In addition, recall bias and social desirability bias associated with certain questions in the data collection tool may have led to an overestimation or underestimation of the frequency of participants’ behaviors. To mitigate these biases, rigorous sampling procedures were implemented, data collectors received comprehensive training, the recall period was limited to three months, and anonymity as well as neutrality in question wording were ensured.
In summary, the non-utilization of community relay (CR) services is strongly influenced by both informational and geographical factors. Limited awareness and insufficient understanding of the PIHI Com program significantly reduce mothers’ likelihood of using CR services, highlighting the gap between program exposure and effective service uptake. In addition, regional disparities in utilization suggest unequal implementation and reliance on CRs across the country, with lower use in central and southern regions compared to the north. These findings underscore the need to strengthen community sensitization, improve communication on the scope of services offered by CRs, and ensure more equitable program implementation across regions to enhance the utilization of community-based healthcare services.
What is already known about the topic
What this study adds
We would like to express our gratitude to Dr Annonciat Semevo Aviansou for the constructive comments that have enriched this article. We are grateful to Eloïc Lenox Atindegla for the relevance of his assessments and the support provided, which have greatly enriched the quality of this work.
All authors critically reviewed the manuscript, and approved the final version for publication. AKG conceptualized and designed the study, organized and supervise data collection, performed data analysis, and drafted the initial manuscript. GN interpreted the results and undertook substantial revisions to finalize the manuscript. SEG and OEMD provided expert supervision, while offering critical guidance on methodology and reviewing the manuscript.
| Variables | Frequency (n) | Percentage (%) |
|---|---|---|
| Mother’s level of education | ||
| No formal | 211 | 47.1 |
| Primary | 111 | 24.8 |
| Secondary and higher | 126 | 28.1 |
| Mother’s marital status | ||
| Single | 14 | 3.1 |
| Married | 434 | 96.9 |
| Mother’s religion | ||
| Traditional and other | 83 | 18.5 |
| Christian | 253 | 56.5 |
| Islam | 112 | 25.0 |
| Mother’s Occupation | ||
| No | 42 | 9.4 |
| Yes | 406 | 90.6 |
| Age of youngest child (in months) | ||
| <12 | 125 | 27.9 |
| 12-23 | 125 | 27.9 |
| ≥24 | 198 | 44.2 |
| Sex of youngest child | ||
| Female | 219 | 48.9 |
| Male | 229 | 51.1 |
| Rank of youngest child | ||
| 1 | 100 | 22.3 |
| 2 | 125 | 27.9 |
| ≥3 | 223 | 49.8 |
| Mother’s knowledge of High-Impact Community-Based Intervention Packages | ||
| No | 311 | 69.4 |
| Yes | 137 | 30.6 |
| Knowledge of CR number | ||
| No | 416 | 92.9 |
| Yes | 32 | 7.1 |
| Awareness of CR services | ||
| No | 208 | 46.4 |
| Yes | 240 | 53.6 |
| Household size | ||
| ≤5 | 283 | 63.2 |
| >5 | 165 | 36.8 |
| Number of children under 5 | ||
| 1 | 263 | 58.7 |
| 2 | 157 | 35.0 |
| ≥3 | 28 | 6.3 |
| Region | ||
| North | 160 | 35.7 |
| Central | 121 | 27.0 |
| South | 167 | 37.3 |
| Variables | Community relay services (n) | cOR | 95% CI | p | |
|---|---|---|---|---|---|
| Non-use | Use | ||||
| Mother’s level of education | |||||
| Uneducated/literate | 112 | 99 | 1.0 | ||
| Primary | 65 | 46 | 1.3 | 0.8 – 2.0 | 0.348 |
| Secondary and higher | 72 | 54 | 1.2 | 0.8 – 1.8 | 0.469 |
| Mother’s marital status | |||||
| Single | 7 | 7 | 1.0 | ||
| Married | 242 | 192 | 1.3 | 0.4 – 3.7 | 0.670 |
| Mother’s religion | |||||
| Traditional and other | 51 | 32 | 2.6 | 1.4 – 4.6 | 0.002 |
| Christian | 155 | 98 | 2.5 | 1.6 – 4.0 | <0.001 |
| Islam | 43 | 69 | 1.0 | ||
| Mother’s occupation | |||||
| No | 27 | 15 | 1.5 | 0.8 – 2.9 | 0.235 |
| Yes | 222 | 184 | 1.0 | ||
| Age of youngest child (months) | |||||
| <12 | 72 | 53 | 1.0 | 0.7 – 1.6 | 0.855 |
| 12-23 | 65 | 60 | 0.8 | 0.5 – 1.3 | 0.422 |
| ≥24 | 112 | 86 | 1.0 | ||
| Sex of youngest child | |||||
| Female | 115 | 104 | 1.0 | ||
| Male | 134 | 95 | 1.3 | 0.9 – 1.9 | 0.201 |
| Rank of youngest child | |||||
| 1 | 57 | 43 | 1.0 | ||
| 2 | 80 | 45 | 1.3 | 0.8 – 2.3 | 0.285 |
| ≥3 | 112 | 111 | 0.8 | 0.5 – 1.2 | 0.260 |
| Mother’s knowledge of PIHI Com. | |||||
| No | 206 | 105 | 4.3 | 2.8 – 6.6 | <0.001 |
| Yes | 43 | 94 | 1.0 | ||
| Knowledge of CR phone number | |||||
| No | 245 | 171 | 10.0 | 3.5 – 29.1 | <0.001 |
| Yes | 4 | 28 | 1.0 | ||
| Knowledge of CR services | |||||
| No | 195 | 13 | 51.7 | 27.3 – 97.8 | <0.001 |
| Yes | 54 | 186 | 1.0 | ||
| Alcohol consumption | |||||
| No | 155 | 124 | 1.0 | ||
| Yes | 94 | 75 | 1.0 | 0.7 – 1.5 | 0.989 |
| Tobacco consumption | |||||
| No | 227 | 171 | 1.0 | ||
| Yes | 22 | 28 | 0.6 | 0.3 – 1.1 | 0.083 |
| Untorn ITNs in household | |||||
| No | 32 | 35 | 1.0 | ||
| Yes | 217 | 164 | 1.5 | 0.9 – 2.4 | 0.164 |
| Availability of latrines with hand-washing facilities | |||||
| No | 232 | 182 | 1.3 | 0.6 – 2.6 | 0.497 |
| Yes | 17 | 17 | 1.0 | ||
| Household size | |||||
| ≤5 | 161 | 122 | 1.2 | 0.8 – 1.7 | 0.465 |
| >5 | 88 | 77 | 1.0 | ||
| Number of children under 5 | |||||
| 1 | 153 | 110 | 1.0 | ||
| 2 | 79 | 78 | 0.7 | 0.5 – 1.1 | 0.118 |
| ≥3 | 17 | 11 | 1.1 | 0.5 – 2.5 | 0.796 |
| Region | |||||
| North | 58 | 102 | 1.0 | ||
| Central | 86 | 35 | 4.3 | 2.6 – 7.2 | <0.001 |
| South | 105 | 62 | 3.0 | 1.5 – 5.9 | 0.003 |
| Variables | aOR | 95% CI | p-value |
|---|---|---|---|
| Mother’s knowledge of PIHI Com | |||
| Yes (Reference) | 1.0 | – | – |
| No | 5.5 | 2.7 – 11.1 | <0.001 |
| Knowledge of CR services | |||
| Yes (Reference) | 1.0 | – | – |
| No | 46.7 | 23.6 – 92.3 | <0.001 |
| Region | |||
| North (Reference) | 1.0 | – | – |
| Central | 3.5 | 1.7 – 7.3 | 0.001 |
| South | 2.9 | 1.5 – 5.9 | 0.003 |