Research | Open Access | Volume 9 (1): Article 47 | Published: 16 Mar 2026
Views: 13
Menu, Tables and Figures
| Variable | Frequency | Percentage (%) |
|---|---|---|
| Age (years) | ||
| Early adolescence (13-14) | 137 | 68.8 |
| Late adolescence (15-19) | 62 | 31.2 |
| Gender | ||
| Male | 70 | 35.2 |
| Female | 129 | 64.8 |
| Class | ||
| JSS 1 | 36 | 18.1 |
| JSS 2 | 35 | 17.6 |
| JSS 3 | 44 | 22.1 |
| SSS 1 | 24 | 12.1 |
| SSS 2 | 29 | 14.6 |
| SSS 3 | 31 | 15.6 |
| Living Situation | ||
| Both Parents | 138 | 69.3 |
| Single Parents | 29 | 14.6 |
| Guardians | 32 | 16.1 |
| Access to Internet | ||
| Yes | 159 | 79.9 |
| No | 40 | 20.1 |
| Received Formal Education on SRH | ||
| Yes | 170 | 85.4 |
| No | 29 | 14.6 |
| Religion | ||
| Christianity | 174 | 87.4 |
| Islam | 25 | 12.6 |
| None | 0 | 0.0 |
| Type of School | ||
| Private | 107 | 53.8 |
| Public | 92 | 46.2 |
| Number of Siblings | ||
| None | 10 | 5.0 |
| 1–2 | 53 | 26.6 |
| 3–4 | 97 | 48.7 |
| 5 or more | 39 | 19.6 |
| Mode of Transportation | ||
| Parents own one car | 66 | 33.2 |
| Parents own multiple cars | 84 | 42.2 |
| Parents primarily use public transportation | 47 | 23.6 |
| Parents rely on others for transportation | 2 | 1.0 |
| Socioeconomic Class | ||
| High | 96 | 48.0 |
| Medium | 99 | 50.0 |
| Low | 4 | 2.0 |
| Variable | Frequency | Percentage (%) |
|---|---|---|
| Comfort discussing sexual health with peers | ||
| Very uncomfortable | 68 | 34.2 |
| Somewhat uncomfortable | 35 | 17.6 |
| Neutral | 35 | 17.6 |
| Very comfortable | 61 | 30.7 |
| Sex education taught in school | ||
| No | 20 | 10.1 |
| Yes | 179 | 89.9 |
| Importance of access to SRH services | ||
| Not important | 7 | 3.5 |
| Somewhat unimportant | 2 | 1.0 |
| Neutral | 8 | 4.0 |
| Somewhat important | 13 | 6.5 |
| Very important | 169 | 84.9 |
| Parents discussing SRH | ||
| No | 27 | 13.6 |
| Yes | 172 | 86.4 |
| Contraceptives without parental consent | ||
| No | 58 | 29.2 |
| Yes | 141 | 70.9 |
| Equal SRH education for boys & girls | ||
| No | 84 | 42.2 |
| Yes | 115 | 57.8 |
| Teenagers discussing SRH with healthcare providers | ||
| No | 36 | 18.1 |
| Yes | 163 | 81.9 |
| Variable | Frequency | Percentage (%) |
|---|---|---|
| Formal SRH education | ||
| Yes, comprehensive | 118 | 59.3 |
| Yes, limited | 69 | 34.7 |
| No, not at all | 12 | 6.0 |
| Understanding of SRH | ||
| Very good | 98 | 49.2 |
| Good | 78 | 39.2 |
| Fair | 19 | 9.5 |
| Poor | 4 | 2.0 |
| Awareness of SRH services | ||
| Yes | 45 | 22.6 |
| No | 125 | 62.8 |
| Not sure | 29 | 14.6 |
| Source of SRH information | ||
| School | 73 | 36.7 |
| Parents/Guardians | 90 | 45.2 |
| Friends | 4 | 2.0 |
| Internet/Social media | 23 | 11.6 |
| Health professionals | 7 | 3.5 |
| Others | 2 | 1.0 |
| Comfort discussing SRH with parents | ||
| Very comfortable | 69 | 34.7 |
| Comfortable | 41 | 20.6 |
| Neutral | 41 | 20.6 |
| Uncomfortable | 48 | 24.1 |
| Adequacy of school SRH info | ||
| Strongly agree | 50 | 25.1 |
| Agree | 96 | 48.2 |
| Neutral | 42 | 21.1 |
| Disagree | 7 | 3.5 |
| Strongly disagree | 4 | 2.0 |
| Importance of learning consent | ||
| Very important | 154 | 77.4 |
| Important | 31 | 15.6 |
| Neutral | 8 | 4.0 |
| Unimportant | 5 | 2.5 |
| Very unimportant | 1 | 0.5 |
| Perception of how SRH is portrayed in media/social media | ||
| Very positive | 26 | 13.1 |
| Positive | 40 | 20.1 |
| Neutral | 69 | 34.7 |
| Negative | 47 | 23.6 |
| Very negative | 17 | 8.5 |
| Barriers to SRH services (multiple) | ||
| Multiple choices | 73 | 36.7 |
| Lack of information | 74 | 37.2 |
| Stigma/Shame | 21 | 10.6 |
| Parental disapproval | 14 | 7.0 |
*Multiple responses allowed, percentages may exceed 100%.
Sylvia Adanma Ezenwa-Ahanene1,2, Madaki Dauda Polycarp1,3, Oghenetega ThankGod Oweh4,&, Olaolu Bilewu1, Deinere Oweh5
1Department of Public Health, Faculty of Basic and Applied Biological Sciences, Ahmadu Bello University, Zaria, 2Nigeria Centre for Disease Control and Prevention (NCDC), Abuja, Nigeria, 3Department of Veterinary Tropical Diseases, University of Pretoria, Pretoria 0110, South Africa, 4Department of Medical Biochemistry, College of Medicine, Kaduna State University, 5Department of Sociology, Kaduna State University
&Corresponding author: Oghenetega ThankGod Oweh, Department of Medical Biochemistry, College of Medicine, Kaduna State University. Email: Oghenetega.oweh@kasu.edu.ng ORCID: https://orcid.org/0000-0002-0051-9975
Received: 02 Sept 2025, Accepted: 14 Mar 2026, Published: 16 Mar 2026
Domain: Sexual and Reproductive Health, Public Health
Keywords: Adolescents, sexual and reproductive health, knowledge, attitudes, perceptions, Abuja, Nigeria
©Sylvia Adanma Ezenwa-Ahanene et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Sylvia Adanma Ezenwa-Ahanene et al., Knowledge, attitude, and perception of sexual and reproductive health among adolescents in Abuja secondary schools. Journal of Interventional Epidemiology and Public Health. 2026; 9(1):47. https://doi.org/10.37432/jieph-d-25-00181
Introduction: Sexual and reproductive health (SRH) among adolescents remains a major challenge in Nigeria, where limited knowledge, cultural barriers, and restricted access to services hinder effective SRH education and care. This study assessed adolescents’ knowledge, attitudes, and perceptions of SRH in secondary schools within the Abuja Municipal Area Council.
Methods: This was a cross-sectional study of 199 adolescents aged 13 to 19, conducted in secondary schools within the Abuja Municipal Area Council, using multistage sampling. Data were collected using a structured, validated questionnaire that measured socio-demographic characteristics, knowledge (19 items), attitudes (13 items), and perceptions (30 items) of sexual and reproductive health. Data were analyzed using descriptive statistics (frequencies, percentages), t-tests, and correlation analysis in SPSS version 25.0.
Results: The median age of adolescents was 14 years (IQR:13-16 years). About 81.4%(162/199) had good knowledge of SRH, 64% had positive attitudes toward SRH, and 66% had positive perceptions. The main barriers to accessing SRH information were lack of information (n=116, 58.3%), stigma/shame (n=86, 43.2%), and parental disapproval (n=57, 28.6%).
Conclusion: The findings in this study support the need for the enactment of policies and interventions that will make sexual and reproductive health information and services readily accessible to the target population.
Sexual and reproductive health (SRH) plays a vital role in adolescents’ overall well-being. According to WHO, SRH refers to a state of physical, emotional, mental, and social well-being in all aspects of sexuality and reproduction [1, 2]. This includes components such as sexual health, reproductive health, family planning, maternal and child health, prevention and treatment of sexually transmitted infections (STIs), and the prevention and management of gender-based violence [3, 4].
Adolescence is a crucial period in human development, characterised by significant physical, cognitive, emotional, and social changes. WHO defines adolescence as the phase between childhood and adulthood, typically spanning the ages of 10 to 19 years [4]. Sexual and reproductive health (SRH) plays a pivotal role in the overall health and well-being of adolescents. Some consequences of inadequate access to SRH among adolescents include unwanted pregnancies, increased STIs and HIV, and unsafe abortions [5]. Despite national policies advocating for SRH services for adolescents, many face obstacles in accessing quality SRH services. Factors such as limited access to health facilities and underutilisation of services contribute to the high rate of SRH challenges among adolescents in Nigeria [6]. The poor provision of sexual and reproductive health care for adolescents is an emerging public health concern in Nigeria [7]. The inadequate provision of SRH education in secondary schools in Abuja and other parts of North Central Nigeria exacerbates challenges related to SRH[8].
Despite global recognition of the importance of adolescent SRH [9], there is a paucity of research conducted in Abuja and its environs. By considering local perspectives and diverse cultural factors, this study assessed the knowledge, attitudes and perceptions of adolescents regarding SRH in Abuja secondary schools to provide insights that may guide targeted interventions towards fostering positive SRH behaviours among adolescents.
Study design and setting
This was a cross-sectional study conducted among adolescents between 13 and 19 years enrolled in junior and senior private and public secondary schools within the Abuja Municipal Area Council (AMAC) between May and August 2024. This study was conducted in the Abuja Municipal Area Council (AMAC), one of the six area councils of the Federal Capital Territory (FCT), Nigeria. AMAC is the most urbanised area council in the FCT and houses the seat of the Nigerian government. According to the FCT Universal Basic Education Board, AMAC has approximately 287 registered secondary schools, comprising 112 public (government-owned) schools and 175 private schools, with an estimated student population of over 150,000 adolescents.
Sexual and Reproductive Health (SRH) services in Abuja are available through various channels, including school-based health programs, primary healthcare centres, and youth-friendly health centres. The FCT Secondary Education Board mandates a basic Family Life and HIV Education (FLHE) curriculum in public schools, though implementation varies. Private schools often develop their own approach to SRH education. Formal SRH services accessible to adolescents include family planning services, STI testing and treatment, and antenatal care at public health facilities, typically requiring parental consent for minors. However, access is often hindered by provider biases, confidentiality concerns, and limited youth-friendly service points. Community-based organisations also provide some SRH outreach programs, though coverage remains limited.
Sampling procedure
A multistage sampling technique was employed to select study participants:
Stage 1 (Selection of schools): All secondary schools in AMAC were stratified into two strata based on ownership: public (government-owned) and private schools. Using a computer-generated random number list, 4 public schools and 4 private schools were randomly selected from the sampling frame obtained from the FCT Universal Basic Education Board. This ensured representation from both school types proportional to their distribution in the area.
Stage 2 (Selection of classes): In each selected school, a complete list of all classes (from JSS1 to SSS3) was obtained. Using simple random sampling (balloting method), two classes were selected from each school, one from junior secondary (JSS1-3) and one from senior secondary (SSS1-3) levels, to ensure representation across grade levels.
Stage 3 (Selection of students): All eligible students present in the selected classes on the day of data collection were invited to participate. For students who were absent, replacements were randomly selected from the same class on subsequent days until the required sample size was achieved. This approach minimised selection bias while ensuring adequate representation across age groups and class levels.
Sample size and study population
The sample size for this study was determined using the Cochran formula for descriptive cross-sectional studies. Based on a 95% confidence. level (Z=1.96) and a 5% margin of error (d=0.05), the calculation utilized a prevalence rate (p) of 78.8% (0.788). This prevalence represents the known level of good contraceptive knowledge among adolescents in the Federal Capital Territory, Nigeria [10]. The resulting minimum required sample size was calculated to be 257 participants.
$$
n = \frac{Z^{2} \cdot p \cdot q}{d^{2}}
= \frac{(1.96)^{2} \times 0.788 \times 0.212}{(0.05)^{2}}
\approx 257
$$
However, due to logistical constraints and school access limitations (including restricted school days, ongoing examinations, and the need to complete data collection within the school term), the number of adolescents who consented and fully completed the questionnaire was 199, representing 77.4% of the target sample. This final sample size still provides sufficient power to detect meaningful patterns in knowledge, attitudes, and perceptions of sexual and reproductive health among Abuja secondary school students.
Eligibility criteria (Inclusion and Exclusion)
Adolescents aged 13 to 19 years who were currently enrolled in selected secondary schools in AMAC, FCT, were included in the study; those who did not consent to participate or for whom parental or guardian consent could not be obtained were excluded.
Data collection
Data were collected using a structured paper-based questionnaire adapted from previously validated SRH instruments [11-13]. The tool included sections on socio-demographic characteristics, knowledge, attitudes and perceptions of SRH. The questionnaire was adopted and modified from a previously published and validated SRH survey instrument. Face and content validity were established of two experts in adolescent health and public health. The experts independently reviewed the questionnaire for: clarity and appropriateness of language for the adolescent target population (age 13-19 years), relevance of items to the study objectives and local context, comprehensiveness in covering key SRH domains (knowledge, attitudes, perceptions, barriers), and cultural sensitivity and appropriateness for the Nigerian setting. Each expert provided written feedback, which was discussed in a consensus meeting. Items were modified based on expert recommendations some questions were reworded for clarity, others were removed due to redundancy or cultural inappropriateness, and additional items were included to address identified gaps. This process ensured that the instrument appeared to measure what it intended to measure (face validity) and adequately covered all relevant aspects of adolescent SRH (content validity). The instrument was pretested among 20 students (not included in the main study) to ensure clarity and reliability.
Knowledge was assessed through items on awareness, legal consent age, STI identification, fertility awareness, prevention methods, contraception purpose and methods, and HIV transmission myths. Correct answers were assigned 1 point; incorrect or “don’t know” answers received 0 points. For questions with multiple correct responses, each correct response earned one point. The total knowledge score (range 0-19) was categorized as: Poor knowledge (0-9) and Good knowledge (10-19). The initial plan to categorise into three levels (excellent, good, poor) was revised to a dichotomous classification (poor vs. good) to simplify analysis and improve statistical power for subgroup comparisons. Attitude was measured using Likert-scale items that assessed respondents’ evaluative judgments and predispositions toward SRH, including: (1) comfort discussing SRH with peers (reflecting social attitudes), (2) perceived importance of SRH education and services (reflecting value-based attitudes), and (3) views on contraceptive access and equity (reflecting policy attitudes). Perception was measured via items that assessed respondents’ subjective interpretations and understanding of their SRH experiences and environment, including: (1) adequacy of received education (reflecting perceived quality of instruction), (2) sources of SRH information (reflecting perceived accessibility), (3) comfort discussing SRH with parents (reflecting perceived family communication dynamics), and (4) views on media portrayals of SRH issues (reflecting perceived external messaging). While both domains included items about “comfort,” the attitude items focused on general disposition toward SRH discussions with peers, whereas perception items focused on the specific experience of family communication about SRH. For both scales, higher scores indicated more positive attitudes/perceptions, with reverse scoring for negatively worded items. Total attitude scores (range 0-13) were categorised as Negative/Neutral (0-8) and Positive (9-13). Total perception scores (range 0-30) were categorised as Negative/Neutral (0-20) and Positive (21-30).
Socioeconomic status (SES) was assessed using a composite index adapted from the Family Affluence Scale, incorporating: (1) parental car ownership (0 = no car, 1 = one car, 2 = multiple cars), (2) access to internet at home (0 = no, 1 = yes), (3) number of siblings (0 = 5 or more, 1 = 3-4, 2 = 1-2, 3 = none), and (4) type of school attended (0 = public, 1 = private). Scores were summed (range 0-8) and categorized as: Low SES (0-3 points), Medium SES (4-6 points), and High SES (7-8 points).
Data analysis
Quantitative data were tabulated appropriately to facilitate statistical analysis. Basic descriptive statistics such as frequency and percentages were calculated and used to summarise the data and analysis was done using SPSS version 25.0. Student t-test and ANOVA were used for comparing the mean differences in continuous outcome variables across two or more independent groups while correlation analysis was used to check for the strength and direction of the relationships between the continuous variables.
In addition, outcome variables (knowledge, attitude, and perception) were dichotomized as follows: knowledge (poor vs. good), attitude (negative/neutral vs. positive), and perception (negative/neutral vs. positive). Binary logistic regression analysis was performed to identify factors associated with good knowledge, positive attitude, and positive perception. Variables with p<0.20 in bivariate analysis were entered into multivariate logistic regression models. Adjusted odds ratios (aOR) with 95% confidence intervals were calculated, and statistical significance was set at p<0.05.
Data availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available due to privacy and ethical restrictions concerning sensitive information from minor participants.
Ethical considerations
The research protocol, including the consent process and all materials, was reviewed and approved by the National Health Research Ethics Committee of the Federal Capital Territory, Abuja (Approval: FHREC/2024/01/087).
Consent process: For participants younger than 18 years, parental or guardian consent was obtained through a two-step process: (1) Information sheets and consent forms were sent home with students for parents/guardians to review, which explained the study purpose, procedures, confidentiality measures, and the voluntary nature of participation; (2) Parents/guardians who agreed to their child’s participation signed the consent form and returned it via the student. On data collection day, these students provided written assent after having the study explained to them in age-appropriate language. Participants aged 18 years and above provided independent, written informed consent. All participants were informed that they could withdraw at any time without consequences. Participation was entirely voluntary, and no incentives were provided. All data were anonymised at entry to ensure confidentiality, given the sensitive nature of the topics.
Socio-demographic characteristics of respondents
The sample had more females (64.8%, 129/199) than males (35.2%, 70/199). The mean age of respondents was 14.6 ± 1.8 years (range: 13-19 years), with the majority (48.2%, 96/199) aged 13 years. Most were in JSS3 (22.1%, n=44), lived with both parents (69.3%, n=138), had internet access (79.9%, n=159), received formal SRH education (85.4%, n=170), were Christian (87.4%, n=174), and attended private schools (53.8%,n=107). The higher proportion of female respondents (64.8%, n=129) may reflect differences in class composition or participation patterns (Table 1). Most of the adolescents fell within the medium (n = 99, 50%) socioeconomic class, and the rest fell into the high (n = 96, 48%) and low (n = 4, 2%) socioeconomic classes, respectively.
Knowledge of sexual and reproductive health
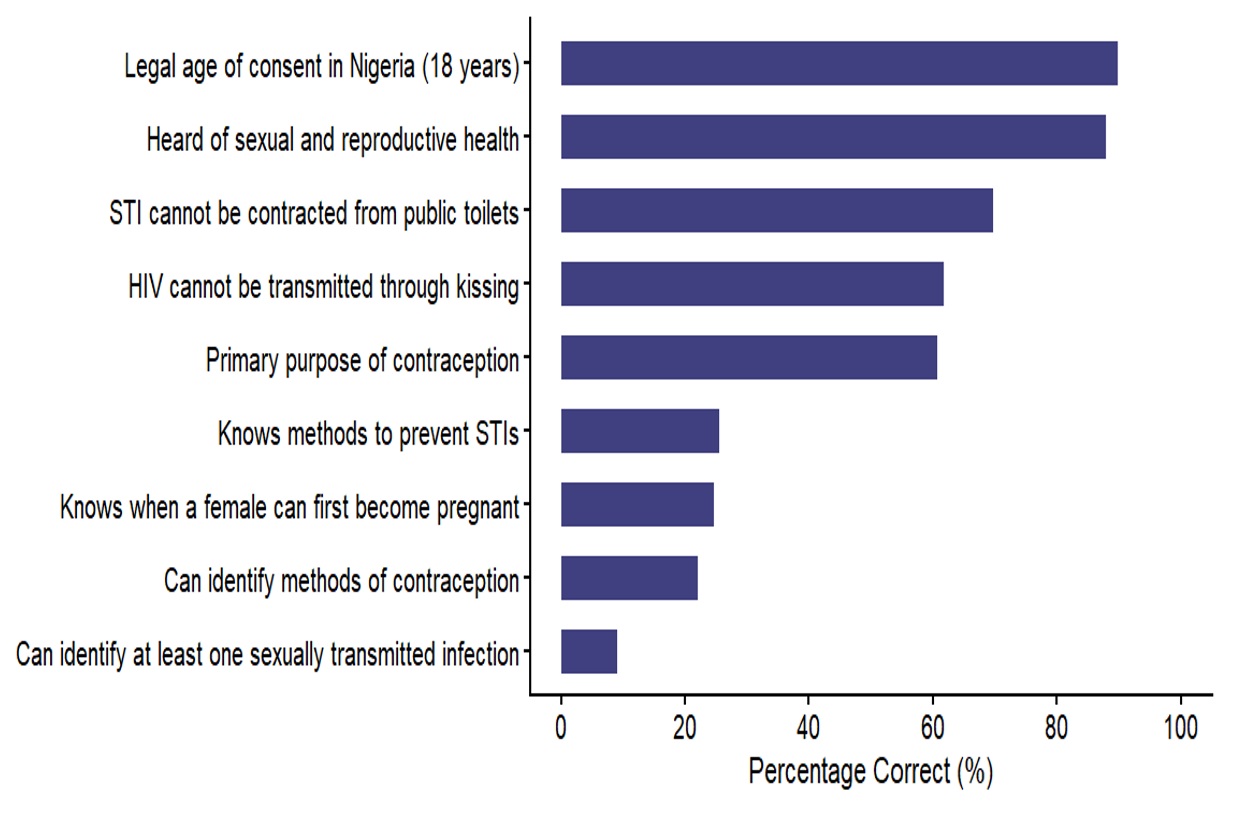
We found that 87.9% (n=175) of the respondents had prior knowledge of sexual and reproductive health. The majority of the respondents (89.9%, n=179) correctly identified 18 years as the legal age for consent. Most of the respondents (69.8%, n=139) correctly identified at least one STI, while 2.0% (n=4) failed to identify any STI. A small proportion of the respondents (24.6%, n=49) correctly identified the age range at which a female can first become pregnant. There was moderate awareness of STI prevention, with 64.8% (n=129) of the respondents identifying at least one correct method. One-third of the respondents (30.2%, n=60) believed that STIs could be contracted from public toilets, and 38.2 %(n=76) of the respondents wrongly noted that HIV transmission was possible through kissing. Most of the respondents (60.8%, n=121) correctly identified prevention of pregnancy as the primary purpose of contraception, with the majority of the respondents (51.3%, n=102) able to identify only one contraceptive method (Figure 1).
The results showed that 81.4% (n=162) of respondents had good knowledge of SRH. The mean knowledge score was 10.12 ± 3.42 out of a possible 19 points. There was a statistically significant difference in mean knowledge scores between early adolescents (13-14 years) and late adolescents (15-19 years). Late adolescents had significantly higher knowledge scores (mean = 12.84 ± 2.91) compared to early adolescents (mean = 8.12 ± 2.67); t(197) = -19.50, p < 0.001, 95% CI (-5.09, -4.15). This indicates that knowledge of SRH improves with age. As illustrated in Figure 1, the highest proportion of correct responses was observed for awareness of SRH (87.9%) and knowledge of the legal age of consent (89.9%). However, significant knowledge gaps were evident: only 24.6% correctly identified when a female can first become pregnant, and 38.2% incorrectly believed HIV could be transmitted through kissing. Misconceptions about STI transmission from public toilets persisted in 30.2% (n=60) of respondents
Attitudes toward sexual and reproductive health
Table 2 shows the assessment of the ease with which the respondents discussed SRH with their parents and guardians. The results showed that 34.2% (n=68) of respondents felt very uncomfortable, 17.6% (n = 35) were somewhat uncomfortable, 17.6% (n = 35) were neutral, and 30.7% (n = 61) felt very comfortable. Most of the respondents, 89.9% (n = 179), believe that teenagers should be given information about sexual health by their parents, while 10.1% (n = 20) of them disagreed. On the other hand, 84.9% (n = 169) of respondents feel that including sexual health education in the school curriculum is very important, while some people feel it is somewhat important (6.5%), neutral (4.0%), somewhat unimportant (1.0%) or not important (3.5%). The assessment showed that most respondents (n = 127, 64%) demonstrated a positive attitude toward sexual and reproductive health. A smaller proportion (n = 68, 34%) displayed a neutral attitude, while only a very small fraction (2%, n=4) expressed negative attitudes toward SRH.
Perceptions of Sexual and Reproductive Health
Most of the respondents (59.3%, n=118) reported that they have received comprehensive formal SRH education, while 34.7% felt their education was limited, and 6.0% (n =12) did not receive any SRH education at all (Table 3). Assessment of the sufficiency of the respondents’ SRH education showed that 49.2% (n = 98) rated it as very good, 39.2% (n = 78) as good, 9.5% (n = 19) as fair, and 2.0% (n=4) as poor. A significant majority of adolescents (n = 125, 62.8%) do not know where to find confidential SRH services in their community. However, 22.6% (n = 45) are aware of where to access these services, while 14.6% (n = 29) are not sure. The primary sources of SRH information as indicated by the respondents were school (n = 73, 36.7%), parents/guardians (n = 90, 45.2%), friends (n = 4, 2.0%), internet/social media (n = 23, 11.6%), health professionals (n = 7, 3.5%), others (n = 2, 1.0%). The ease of discussing SRH topics with parents or guardians varied, with 34.7% (n = 69) feeling very comfortable and 20.6% (n = 41) feeling just comfortable. However, 24.1% (n = 48) felt uncomfortable, and 20.6% (n=41) were neutral about it. The adequacy of information about SRH in the school was assessed, with 48.2% (n = 96) agreeing that it was adequate and 25.1% (n = 50) strongly agreeing on the adequacy. A part of the respondents (3.5%) disagreed, (n = 4, 2.0%) strongly disagreed, and 21.1% (n = 42) were neutral about it. A total of 154 (77.4%) respondents think it is very important to learn about sexual consent and boundaries, 31 (15.6%) think it is important, 5 (2.5%) think it is unimportant, (0.5%, n=1) think it is very unimportant, and 8 (4.0%) are neutral about it. Among the respondents, 26 (13.1%) have a very positive perception about the portrayal of SRH in the media and social media, 40 (20.1%) have a positive perception, 69 (34.7%) feel neutral, 47 (23.6%) have a negative perception, and 17 (8.5%) have a very negative perception about it. Calculation of perception using the adopted scoring system showed that 65 (32.7%) had a positive perception. The mean perception score was 16.68 ± 4.21 out of a possible 30 points, indicating a generally neutral perception overall.
Barriers to accessing SRH information and services
Barriers to accessing SRH information and services were assessed using a multiple-response question (participants could select all that applied). The most frequently cited barrier was lack of information (n=116, 58.3% of respondents), followed by stigma or shame (n=86, 43.2%), parental disapproval (n=57, 28.6%), fear of confidentiality breach (n=53, 26.6%), cultural or religious beliefs (n=27, 13.6%), lack of access to services (n=4, 2.0%), and other barriers (n=6, 3.0%). These findings highlight that informational, social, and systemic barriers collectively impede adolescents’ access to SRH services
This study assessed the knowledge, attitudes, and perceptions of sexual and reproductive health among adolescents in Abuja secondary schools. The main findings reveal that while the majority of adolescents have good knowledge and positive attitudes toward SRH, significant knowledge gaps persist, particularly regarding STI identification, fertility awareness, and contraceptive methods. Additionally, multiple barriers limit access to SRH information and services, with a lack of information being the most prevalent.
The finding that 87.9% of adolescents have heard about SRH suggests that awareness campaigns and school-based programs have achieved reasonable penetration in urban Abuja. This elevated awareness corresponds with the overall trend noted by Chandra-Mouli et al. [9]. However, awareness alone is insufficient, as evidenced by the significant knowledge gaps in STI identification and fertility awareness.
This limited understanding aligns with results reported by Mekie et al. [12], This awareness-knowledge disconnect indicates that current SRH education may be superficial, focusing on terminology rather than a comprehensive understanding. The practical implication is that adolescents may engage in sexual activity believing they are informed, while lacking critical knowledge about pregnancy risk and STI prevention. This places them at continued risk for unintended pregnancies and infections despite high awareness levels [14]. Policy modifications should therefore shift from awareness-focused campaigns to competency-based education that ensures adolescents can apply SRH knowledge in real-world situations
The study revealed that 64% of respondents had a positive attitude toward SRH, while 34% were neutral and 2% had negative attitudes. Comfort levels when discussing sexual health with parents or guardians varied considerably, with 34.2% feeling very uncomfortable. This variation agrees with the report of Jonas et al.[15], who highlight the importance of trust and confidentiality in SRH service utilization.
The overwhelming support for parental involvement and school-based SRH education indicates that adolescents themselves recognise the value of comprehensive SRH education from multiple sources. This contradicts the assumption that young people prefer to learn about SRH exclusively from peers or media. The finding suggests that current barriers to parent-adolescent communication are not due to adolescent resistance but rather to systemic and cultural barriers that could be addressed through parent education programs and communication skills training. Schools should leverage this student support to strengthen their SRH curricula, while policymakers should recognize that expanding school-based SRH education aligns with adolescent preferences and may improve utilization.
Regarding perceptions, about half reported receiving comprehensive formal SRH education, while about a third felt their education was limited, and 6.0% received none. A concerning finding was that nearly two-thirds of adolescents do not know where to find confidential SRH services in their community. This lack of awareness represents a critical barrier to service utilisation, as adolescents cannot access services they do not know exist [16].
The primary sources of SRH information were parents/guardians and schools, highlighting the crucial role of both home and educational institutions in SRH education. This aligns with Fatemi et al. [17], who emphasise the importance of integrating SRH education within both school curricula and community efforts. The finding that 34.7% of respondents felt very comfortable discussing SRH with parents, while 24.1% felt uncomfortable, suggests that parent-adolescent communication about SRH needs strengthening.
The predominance of informational barriers despite high awareness levels reveals a critical paradox: adolescents know that SRH information exists but cannot access specific, actionable information when needed. This suggests that SRH information is not available in accessible, age-appropriate, and confidential formats at the point of need. The high prevalence of stigma/shame indicates that social norms continue to stigmatise adolescent SRH discussions, even in urban settings. This likely discourages help-seeking behaviour and may explain why 62.8% of respondents did not know where to find confidential SRH services. Parental disapprova as a barrier suggests that family-level interventions are needed to complement school-based programs. Policy responses should therefore address multiple levels: improving confidential service access points, community stigma reduction campaigns, and family communication programs [18].
A surprising finding was that most respondents belonged to medium or high socioeconomic classes, yet the correlation between socioeconomic status and SRH outcomes was generally weak. This suggests that in urban Abuja, exposure to SRH information through schools, media, and peers may be relatively universal, transcending socioeconomic boundaries. However, the slight tendency for higher socioeconomic status to be associated with less positive attitudes suggests potential cultural or educational differences that warrant further investigation [17].
Another noteworthy finding was the limited impact of cultural or religious beliefs as barriers to accessing SRH information (only 1.5% cited this as a primary barrier). This is unexpected given Nigeria’s culturally diverse and religious society and may be attributable to the urban setting of the study, where metropolitan lifestyles may moderate traditional influences on the study population.
The discrepancy between high awareness of SRH and poor knowledge of specific reproductive health facts suggests that current SRH education may be superficial and needs to be deepened. This finding underscores the importance of moving beyond awareness-raising to comprehensive, age-appropriate education that addresses specific knowledge gaps. The positive correlation between age and knowledge, attitude, and perception scores indicates that as adolescents grow, they develop more positive SRH outcomes. This suggests that earlier interventions, targeted at younger adolescents, could be particularly beneficial in establishing positive SRH knowledge and attitudes from an early age.
The study findings revealed that despite the demonstration of good awareness and knowledge of sexual and reproductive health, there are still some significant gaps in knowledge and misconceptions persists especially regarding STI transmission, methods of contraception and infection. Most of the adolescents don’t know where to access SRH services and do not feel comfortable discussing SRH with their parents. As age increases, knowledge, attitudes and perceptions also improve, which demonstrates the need for earlier age-specific interventions. It would be beneficial to improve school-based SRH-education, adolescent and parent communication, and ensure availability and accessibility to SRH services to address these gaps.
What is already known about the topic
What this study adds
| Variable | Frequency | Percentage (%) |
|---|---|---|
| Age (years) | ||
| Early adolescence (13-14) | 137 | 68.8 |
| Late adolescence (15-19) | 62 | 31.2 |
| Gender | ||
| Male | 70 | 35.2 |
| Female | 129 | 64.8 |
| Class | ||
| JSS 1 | 36 | 18.1 |
| JSS 2 | 35 | 17.6 |
| JSS 3 | 44 | 22.1 |
| SSS 1 | 24 | 12.1 |
| SSS 2 | 29 | 14.6 |
| SSS 3 | 31 | 15.6 |
| Living Situation | ||
| Both Parents | 138 | 69.3 |
| Single Parents | 29 | 14.6 |
| Guardians | 32 | 16.1 |
| Access to Internet | ||
| Yes | 159 | 79.9 |
| No | 40 | 20.1 |
| Received Formal Education on SRH | ||
| Yes | 170 | 85.4 |
| No | 29 | 14.6 |
| Religion | ||
| Christianity | 174 | 87.4 |
| Islam | 25 | 12.6 |
| None | 0 | 0.0 |
| Type of School | ||
| Private | 107 | 53.8 |
| Public | 92 | 46.2 |
| Number of Siblings | ||
| None | 10 | 5.0 |
| 1–2 | 53 | 26.6 |
| 3–4 | 97 | 48.7 |
| 5 or more | 39 | 19.6 |
| Mode of Transportation | ||
| Parents own one car | 66 | 33.2 |
| Parents own multiple cars | 84 | 42.2 |
| Parents primarily use public transportation | 47 | 23.6 |
| Parents rely on others for transportation | 2 | 1.0 |
| Socioeconomic Class | ||
| High | 96 | 48.0 |
| Medium | 99 | 50.0 |
| Low | 4 | 2.0 |
| Variable | Frequency | Percentage (%) |
|---|---|---|
| Comfort discussing sexual health with peers | ||
| Very uncomfortable | 68 | 34.2 |
| Somewhat uncomfortable | 35 | 17.6 |
| Neutral | 35 | 17.6 |
| Very comfortable | 61 | 30.7 |
| Sex education taught in school | ||
| No | 20 | 10.1 |
| Yes | 179 | 89.9 |
| Importance of access to SRH services | ||
| Not important | 7 | 3.5 |
| Somewhat unimportant | 2 | 1.0 |
| Neutral | 8 | 4.0 |
| Somewhat important | 13 | 6.5 |
| Very important | 169 | 84.9 |
| Parents discussing SRH | ||
| No | 27 | 13.6 |
| Yes | 172 | 86.4 |
| Contraceptives without parental consent | ||
| No | 58 | 29.2 |
| Yes | 141 | 70.9 |
| Equal SRH education for boys & girls | ||
| No | 84 | 42.2 |
| Yes | 115 | 57.8 |
| Teenagers discussing SRH with healthcare providers | ||
| No | 36 | 18.1 |
| Yes | 163 | 81.9 |
| Variable | Frequency | Percentage (%) |
|---|---|---|
| Formal SRH education | ||
| Yes, comprehensive | 118 | 59.3 |
| Yes, limited | 69 | 34.7 |
| No, not at all | 12 | 6.0 |
| Understanding of SRH | ||
| Very good | 98 | 49.2 |
| Good | 78 | 39.2 |
| Fair | 19 | 9.5 |
| Poor | 4 | 2.0 |
| Awareness of SRH services | ||
| Yes | 45 | 22.6 |
| No | 125 | 62.8 |
| Not sure | 29 | 14.6 |
| Source of SRH information | ||
| School | 73 | 36.7 |
| Parents/Guardians | 90 | 45.2 |
| Friends | 4 | 2.0 |
| Internet/Social media | 23 | 11.6 |
| Health professionals | 7 | 3.5 |
| Others | 2 | 1.0 |
| Comfort discussing SRH with parents | ||
| Very comfortable | 69 | 34.7 |
| Comfortable | 41 | 20.6 |
| Neutral | 41 | 20.6 |
| Uncomfortable | 48 | 24.1 |
| Adequacy of school SRH info | ||
| Strongly agree | 50 | 25.1 |
| Agree | 96 | 48.2 |
| Neutral | 42 | 21.1 |
| Disagree | 7 | 3.5 |
| Strongly disagree | 4 | 2.0 |
| Importance of learning consent | ||
| Very important | 154 | 77.4 |
| Important | 31 | 15.6 |
| Neutral | 8 | 4.0 |
| Unimportant | 5 | 2.5 |
| Very unimportant | 1 | 0.5 |
| Perception of how SRH is portrayed in media/social media | ||
| Very positive | 26 | 13.1 |
| Positive | 40 | 20.1 |
| Neutral | 69 | 34.7 |
| Negative | 47 | 23.6 |
| Very negative | 17 | 8.5 |
| Barriers to SRH services (multiple) | ||
| Multiple choices | 73 | 36.7 |
| Lack of information | 74 | 37.2 |
| Stigma/Shame | 21 | 10.6 |
| Parental disapproval | 14 | 7.0 |
*Multiple responses allowed, percentages may exceed 100%.