Outbreak Investigation | Open Access | Volume 9 (2): Article 65 | Published: 17 Apr 2026

Views: 1,391
Menu, Tables and Figures
| Variable | Number | Attack rate (%) | Prevalence OR (95% CI) |
|---|---|---|---|
| All cases | 45 | 45/135 (33.33) | |
| Sex | |||
| Female | 5 | 5/25 (20) | 1 |
| Male | 40 | 40/110 (36.36) | 2.7 (1.31–3.04) |
| Age class* (years) | |||
| 18–28 | 11 | 11/31 (35.48) | 1 |
| 29–39 | 17 | 17/53 (32.08) | 1.5 (0.9–4.2) |
| 40–50 | 10 | 10/29 (34.48) | 2.1 (1.8–3.4) |
| 51 and + | 7 | 7/22 (31.82) | 2.2 (1.7–3.5) |
| Concerned prison | |||
| Prison 1 | 18 | 18/49 (36.73) | 1 |
| Prison 2 | 14 | 14/42 (33.33) | 2.9 (0.8–11.1) |
| Prison 3 | 13 | 13/44 (29.54) | 2.1 (0.5–8.2) |
Table 1: Characteristics of mpox cases during the mpox outbreak in 3 military prisons in Kinshasa, DRC, October 2024 to January 2025
| Variable | Number (%) | Median (range) |
|---|---|---|
| Symptoms | ||
| Fever | 42 (93.3) | |
| Skin rashes | 45 (100.0) | |
| Myalgia | 40 (88.9) | |
| Physical asthenia | 37 (82.2) | |
| Lymphadenopathy | 29 (64.4) | |
| Hospitalization | 45 (100.0) | |
| Length of hospitalization (days) | 10 (5–12) | |
| Incubation period (days) | 8 (6–11) | |
| Scab samples collected | 88 (65.2) | |
| Blood samples collected | 88 (65.2) | |
| Scab samples positive for mpox | 45/88 (51.1) | |
| Blood samples positive for mpox | 26/88 (29.5) | |
Table 2 : Clinical and laboratory characteristics of mpox cases during the mpox outbreak in 3 military prisons in Kinshasa, DRC, October 2024 to January 2025 (n = 45)
Table 3: Mpox safety and prevention measures implemented in three prisons. n=45. mpox outbreak in 3 military prisons in Kinshasa, DRC, October 2024 to January 2025
| Classification | Considerations for the prevention of mpox | Recommended changes to the prison |
|---|---|---|
| Structural | Reduce the density of people in the prison | Stop accepting too many visitors to the prison |
| *Stagger visiting hours by increasing the number of visiting shifts | ||
| Stop adding new people to the prison and release prisoners with sentences for release already pronounced | ||
| Reduce the number of people around meals | ||
| Maintain physical distancing when entering and leaving the prison | *Use of larger doors for entry and exit | |
| Functional | Maintaining physical distancing during calls and plenary sessions within the confines of the plot housing the prisons | Reduce the number of speakers per session and per workspace |
| Use of virtual means to conduct certain meetings | ||
| Isolate suspected detainees (symptomatic of mpox) | Investigate and collect all suspected cases in the prison | |
| Isolate any suspected case on site then with mpoxTC | ||
| Compliance with infection prevention and control measures | Installation of hand hygiene devices at observation points | |
| *Regular cleaning and disinfection of surfaces | ||
| Wearing of appropriate PPE, including face masks, by all officers and officials in the lockup | ||
| Socio-economic | People in detention living in densely populated and highly interactive communities | Educate people in detention about general preventive measures when they leave the prison |
Table 3: Mpox safety and prevention measures implemented in three prisons during the outbreak in 3 military prisons in Kinshasa, DRC, from October 2024 to January 2025


Levis Kengea Amisi1,2,&, Winnie Bikoki Masamba3, Vally Temuangudi Ndumbi4, Angele Mavinga Wumba5, Anthony Mutombe Mbuyi2,5, Jean Jacques Kalume Kape5, Jean Claude Bungiena Nsinga2,5
1Kokolo Health Zone, Military Health Corps, Kinshasa, Democratic Republic of Congo, 2School of Public Health, University of Kinshasa, Kinshasa, Dem. Rep. of Congo, 3Central Military Hospital, Military Health Corps, Kinshasa, Democratic Republic of Congo, 4Type A Operational Medical Centre of the 113 Ndolo Air Base, Military Health Corps, Kinshasa, Democratic Republic of Congo, 5Military Health Corps, Kinshasa, Democratic Republic of Congo
&Corresponding author: Levis Kengea Amisi, Kokolo Health Zone, Military Health Corps, Kinshasa, Democratic Republic of Congo, Email: drlevisamisi@gmail.com, ORCID: https://orcid.org/0009-0007-0966-7783
Received: 19 Sep 2025, Accepted: 15 Apr 2026, Published: 17 Mar 2026
Domain: Field Epidemiology
Keywords: Mpox outbreak, Congestion and physical distancing, Public health response, Democratic Republic of Congo
©Levis Kengea Amisi et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Amisi Kengea Levis et al., Mpox outbreak in a confined population in Kinshasa, Democratic Republic of Congo, October 2024 to January 2025 . Journal of Interventional Epidemiology and Public Health. 2026; 9(2):65. https://doi.org/10.37432/jieph-d-25-00198
Introduction: In October 2024, an alert was issued at a military prison in Kinshasa, Democratic Republic of the Congo, of a possible mpox outbreak among the detainees. We invested the alert to confirm the outbreak, institute control measures, and prevent further escalation of the situation, given the confined nature of the prison.
Methods: An outbreak investigation team was constituted. A suspected case of mpox was defined as any person in the prisons presenting a fever (temperature ≥ 38°C) or an acute fever accompanied by symptoms of mpox, or any person presenting one or more maculopapular rashes or crusts between October 2024 and December 30, 2024. We conducted an active search for suspected mpox cases, identified and tested the contacts. We conducted environmental analyses and identified gaps in surveillance, as well as infection prevention and control (IPC) measures present in the prison.
Results: Of the 135 people detained in the prisons, 88 detainees (65.18%) were tested as part of active case finding and contact tracing, and 45 of the 88 suspected cases (51.13%) tested positive for mpox. The median age of the positive patients was 41 years (1st Quartile 24 years – 3rd Quartile 46 years). An outbreak of mpox was confirmed, introduced by a new inmate from outside the prison. All new intake of inmates was stopped to relieve congestion and allow for a certain degree of physical distancing among inmates. Visitors were also prevented from further interactions with the inmates as a control measure to prevent escalations. Preventive measures were instituted, congestion was relieved, and infected cases were treated as per existing protocol.
Conclusion: An outbreak of mpox was confirmed in the prisons. The crowded prisons, combined with ineffective preventive measures, probably facilitated the spread of the outbreak. We recommended strengthening the surveillance measures, improving health preventive measures, and vaccinating the community outside of the prisons in the Health Zone and inmates and personnel in the prisons.
In Africa, the mpox epidemic continues to spread in different countries, including the Democratic Republic of Congo, South Africa, Ivory Coast, Kenya, Liberia, Nigeria, Uganda, the Central African Republic, Burundi, Rwanda and most recently, Senegal. In the DRC, mpox is now considered a major epidemic at the national level, affecting several provinces, including Kinshasa, with more than 102,176 cases, involving both subclades Ia and Ib. The focus of the control has been improving surveillance, isolation and treatment of cases and vaccination, especially among the general population and some key populations. The result of the control of efforts has been variable due to security challenges, socio-cultural dynamics and limited geographical and financial access to early treatment.
In October 2024, the authorities in one of the three military prisons in Kinshasa, Democratic Republic of Congo, issued an mpox alert, informing of a suspected case of mpox for four days. After the investigation, it was noticed that the detainee had passed through two military prisons. There were 136 detainees in confinement, 135 had become contacts, and many had become suspects. A one health team was deployed with the objective to confirm the outbreak, characterise the outbreak epidemiologically, clinically and environmentally and advise on control strategies and policy implications.
Study design and setting
We conducted a descriptive cross-sectional study to confirm and describe the outbreak. The study took place at the Gombe, Matete and Ngaliema military prisons in Kinshasa from October to December 2024. They were densely populated with poor sanitation practices among the inmates. These prisons were within the Kokolo health district, a strategic zone for health monitoring with an mpox treatment centre (mpoxTC).
The Kokolo Health Zone (HZ) is one of the 35 HZ of the Kinshasa Provincial Health Division and one of the military units of the Military Health Corps (MHCor), with 32 health care facilities scattered throughout the city-province of Kinshasa. This HZ has extensive experience in managing previous epidemics, including measles, cholera, and COVID-19, with a specific treatment centre set up for the response [1].
An mpox TC at the Kokolo HZ has been set up to provide holistic care (medical, psychological and nutritional care) for all mpox detainees in the city of Kinshasa, as well as for mpox cases among military personnel and/or their dependents and/or civilians living in the vicinity of military camps or preferring a military healthcare facility. This mpox care site is therefore specific, as it is located in a military HZ, specifically in a military camp.
Case definition
Suspected case of mpox was defined as “any person in the cell presenting with fever (T° ≥ 38 °C) or acute fever accompanied by one of the other symptoms of mpox (adenopathy, myalgia, physical asthenia, rashes), or any person presenting only one or more smallpox-like rashes between October 2024 and December 30, 2024.” The national coordination of mpox response defines a probable case as a deceased or untraceable case for which no laboratory results for mpox could be obtained, but which subsequently generated suspected or confirmed cases. In other words, it is a patient who, for clinical and/or epidemiological reasons, has a very high probability of being infected with the mpox virus, but whose infection has not been laboratory confirmed. A confirmed case is a suspected case of mpox for which a laboratory test (PCR) is positive. A non-case is a suspected case of mpox for which the laboratory test (PCR) is negative [1].
Community engagement and prison visit
We engaged with political and administrative authorities through physical and virtual meetings to obtain firsthand information on the nature of the situation, obtain their consent, and obtain authorisation to collect data as part of the epidemic response. A special mpox case management site was immediately set up not far from the prison, with a detachment of the health district’s response team. The general public was also engaged through media and health education on the causes of mpox, established potential risk factors, and means of prevention using community outreach systems. After completing the initial administrative procedures, we visited the prison to determine the exact number of inmates and to assess the security environment and preventive measures, overcrowding procedures in the prisons, and visitor reception. We also reviewed plans to prevent mpox transmission in prisons.
Active case search and contact tracing
During the same period of October 2024, the Kokolo HZ response team immediately launched an active search for mpox cases and case investigation, as well as an environmental assessment to confirm the outbreak, assess it in the prisons, identify the mode and drivers of transmission and implement the necessary management and response measures. The three prisons initially held 136 male and female inmates. The inmates came from all over Kinshasa. The prison was overcrowded, and the number of inmates continued to increase. There was no infirmary or health personnel dedicated solely to the three prisons. Patients of all types in the prisons were transferred to the Central Military Hospital for treatment. However, for mpox, as during the COVID-19 period, a specific mpoxTC was set up within the Kokolo Health Zone, specifically within the enclosure housing the prison, until the end of the epidemic.
We obtained data on demographic characteristics, periods, signs and symptoms, and potential risk factors for contracting the disease. The samples were sent to the National Institute of Biomedical Research (NIBR) laboratory for testing for mpox by Real Time-PCR (RT-PCR). We identified all contacts, including household contacts and visitors of both the suspected and confirmed cases, who were followed for 21 days through community relays (Core for short). All patients who tested positive received treatment for mpox until recovery, and non-cases were treated for other health problems they had, and were then transferred to the central military hospital or other non-mpox health facility.
Contact follow-up was carried out for 21 days, and the number of follow-up days was calculated based on the last day of contact with a confirmed mpox case. The contacts were discharged on the 21st day of follow-up, according to the national protocol [2-5]. As soon as a contact developed any clinical sign, their status was changed to that of a suspected case, and they benefited from investigation, contact listing and decontamination of the places visited by the latter (pavilions, rooms or offices in the enclosure of the prison). The health district health team collected data on all test results from the contacts of the first mpox case, as well as other agents and officials of the prison. The addresses and telephone numbers of the 28 external contacts at the prison were also obtained from the visitor registers and from the suspected or confirmed cases themselves.
Environmental investigations
Beginning in October, authorities from the Military Health Corps (MHCor) and the Kokolo health district inspected prisons several times, investigated detention conditions, and interviewed both inmates and prison officials to detect any illnesses in the 21 days prior to the onset of suspected signs of mpox. They examined the addresses and backgrounds of inmates before their arrival at the prison. Samples of scabs and blood samples were available whenever inmates became suspects.
The assessment of infection prevention and control was based on the number of inmates, the presence of handwashing kits, separate facilities for the sick and the healthy, as well as the cleanliness of these sanitary facilities.
Sample size, sampling and Laboratory testing
All 136 inmates from three military prisons were included in this study. All samples were collected from vesicular skin lesions using sterile forceps and swabs. Samples were transported by laboratory technicians of the Kokolo health district in triple packaging to the National Institute of Biomedical Research, where they were RT-PCR and sequencing were done. The positive as well as the negative results were given by the laboratory.
Data analysis
The linelist was analysed in Microsoft Excel and Stata version 14.0. For quantitative data (length of hospitalisation, incubation period, time from contact to the onset of the first suspected signs of mpox), given the abnormal distribution, the median with its range was calculated. The frequency and the proportion of cases were estimated. The attack rates (AR) were estimated for each prison. Prevalence odds ratios (OR) and 95% confidence intervals (95% CI) were calculated for different variables. The chi-square test was used to compare proportions between groups, with p considering α=5%. The results are presented in table form.
Ethical considerations
Approval letter N° 630/CNES/BN/PMMF/2025 of 16/02/2025 by the National Health Ethical Committee, although the outbreak investigation was considered a response to a public health emergency for which approval was granted by the Kokolo Health District Health Services. Consent was obtained during the mpox response from all individuals whose samples were collected for laboratory testing and stayed available for the present study. The samples were collected for laboratory testing in the best interest of individuals and society as a whole. Permission was also sought from local stakeholders and prison management before conducting the tests and visiting the prison. Permission was also sought from the relevant authorities to access the data from the line list used.
The first mpox case was a detainee incarcerated in October 2024. He first developed a fever four days before, for which he was given two paracetamol tablets for each episode when he passed through the first prison. Myalgia and rashes appeared two days after he was transferred to the second prison, followed by physical asthenia two days after, the day the alert was triggered in the third prison. The first case presented with fever, physical asthenia, myalgia, rash, and lymphadenopathy within seven days of arrival at the third prison. He had no contact with any other known case of mpox or with anyone suffering from any eruptive illness, and no other case of mpox had previously been recorded in these prisons.
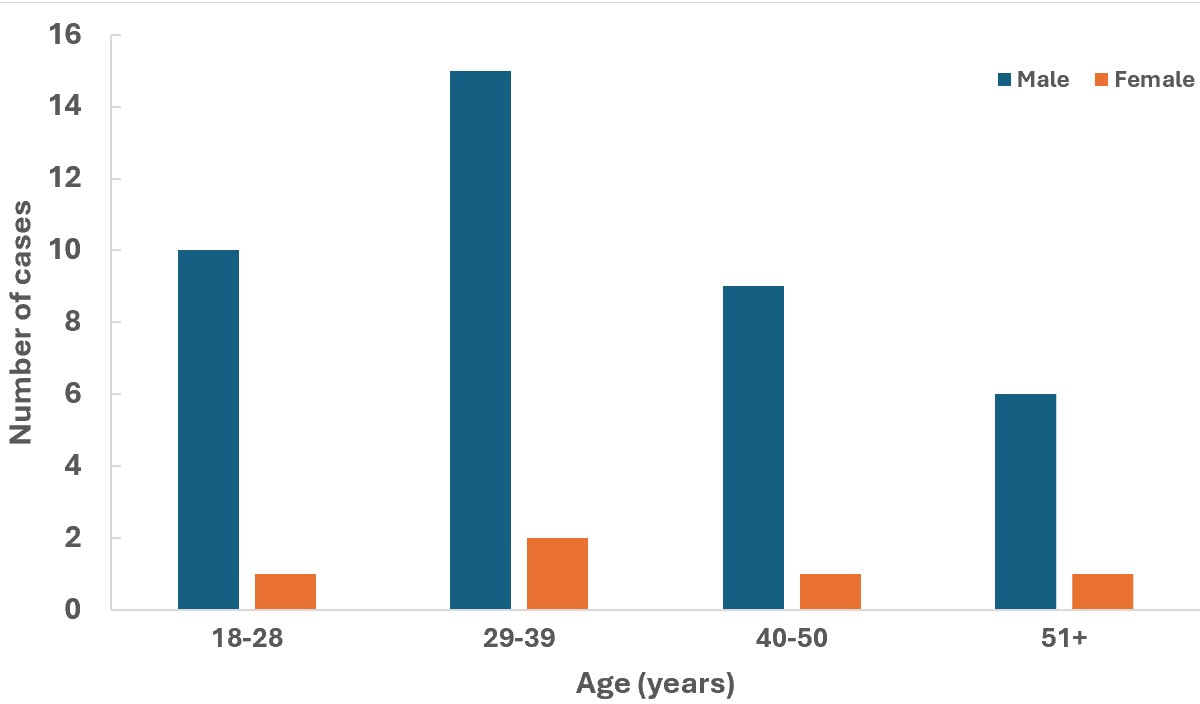
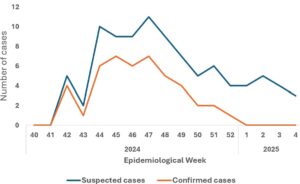
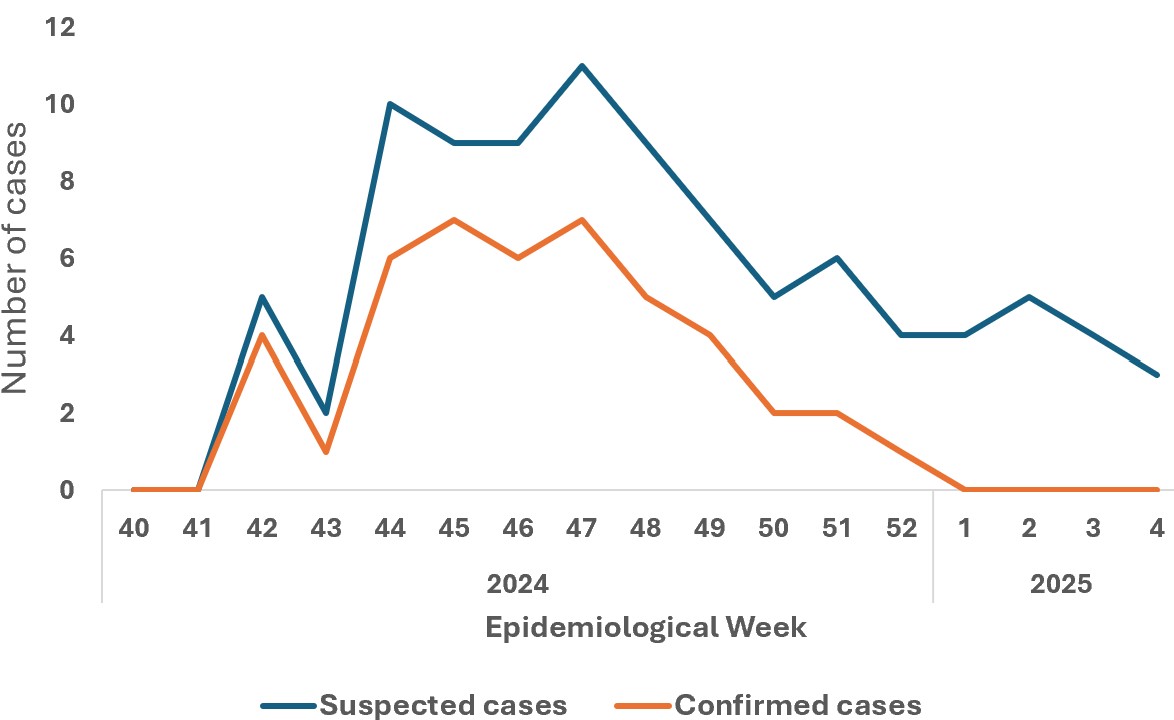
The 135 inmates (100%), contacts of the first mpox case, were followed up within 21 days. One hundred and ten (81.48%) of them were men. The case definition could be applied to 88 inmates (65.18%, 95%CI: 42.43-88.21%) who had become suspected cases or symptomatic, forty-five of these 88 samples; or 51.14% (95%CI: 37.24-64.32%) were confirmed mpox among which 40 (88.89%, 95%CI: 76.23-92.65%) were male and 17 (37.78% 95%CI: 26.46-48.41%) aged 29 to 39 years (Figure 1). The overall attack rate among inmates was 33.33% (95%CI: 24.75-45.28%). The age and sex distribution of mpox inmates with higher attack rates differed from that of mpox inmates with lower attack rates (Table 1). The epidemiological weeks of confirmation of mpox diagnosis for the 45 cases are presented in Figure 2. The number of cases has been steadily increasing, starting in week 41 of 2024, peaking in week 47 of the same year and decreasing in the first week of 2025 (Figure 2).
The median time from contact to the onset of the first suspected signs of mpox in mpox cases was 8 days (range, 6–11 days). The median length of hospitalisation was 10 days (range, 5–12 days). Males were 2.7 times (95% CI: 1.3–3) more likely to be affected than females. Inmates aged 18–28 years had the highest attack rate (35.48%) and were 1.3 times (95% CI: 0.26–3.92) more likely to have confirmed mpox than inmates aged 51 years and older, who had the lowest attack rate (31.82%), but the difference is not statistically significant.
Attack rates for inmates in the three prisons ranged from 29.54% to 36.73% (X2 = 10.2; p =0.24). The first prison had more mpox cases, 18 (36.73%), compared to the other two with 14 (33.33%) and 13 (29.54%), respectively, but this difference was not statistically significant. The main symptoms of the cases were skin rashes (case definition: 100%), fever (93.33%), myalgia (88.89%), physical asthenia (82.22%) and lymphadenopathy (64.44%) (Table 2).
Eighty-eight suspected cases of mpox (65.18%) provided scab and blood samples. Forty-five of them returned positive for mpox (51.14%) following scab sampling, and twenty-six returned positive (29.54%) following blood sampling. There were no cases of mpox with genital rashes, and the laboratory had only mentioned subclade Ia and no sexual transmission form of mpox. All positive cases had been treated with topicals, antibiotics, zinc and symptomatic treatment of cases, with satisfactory follow-up. There was no further increase in cases unrelated to the mpox epidemic in the three prisons during this study period. The rapid increase and decrease of the epidemic, the single peak despite the promiscuity and overcrowding in the prisons as well as the nonobservance of hygiene and infection prevention and control (IPC) measures in the prison enclosures as well as the halt in the increase in new mpox cases confirmed by the laboratory suggest an epidemic of community origin brought by a new inmate who had just been put in prison (Figure 2).
Contact tracing
The total number of contacts of the initial case outside the cell has not been established with precision, apart from the 28 visitors recorded. However, the 135 co-inmates were followed up: 88 of them were tested as suspects and 45 tested mpox positive (Figure 2). All were treated and monitored until their recovery, in accordance with national guidelines. Actions included raising awareness among the 135 inmates, vaccination during the response (only 69 accepted, lacking full confidence in the vaccine and fearing for their lives as prisoners), decontaminating the prison, actively searching for suspected cases, providing regular psychosocial support, and conducting contact tracing for 21 days.
Environmental investigations
The authorities of the military health corps and those of the Kokolo Health Zone noted persistent and serious violations of hygiene and IPC rules. The relevant findings regarding the mpox epidemic in the military dungeons were that handwashing kits were unavailable from the prisons, and sanitation was not up to standard in these prisons, with no vaccinated prisoners or prison authorities.
Coordination
A multisectoral approach was used for the investigation and response to the outbreak. In addition to the Ministry of Public Health, Hygiene and Social Security, the Ministry of National Defense and Veterans Affairs (through the Military Health Corps), the Ministry of Justice, and the Provincial Division of Public Health and Hygiene were involved, with support from the Public Health Emergency Operations Center (PHEOC) through the Incident Management System (IMS), which had coordinated the response. Data from local health authorities were shared through provincial health authorities with the national IMS.
Environmental, safety and preventive assessment
Safety and prevention measures were put in place in prisons as soon as cases were identified during the epidemic (Table 1). At the time of the assessment, the prison had no sinks, let alone running water, soap, or hand dryers at the entrances. Only the mpoxTC agents next to the prison scrupulously observed infection prevention and control (IPC) measures by wearing masks, washing their hands regularly, and applying hydroalcoholic gel when necessary. Gloves were systematically worn and changed after each patient, as well as the systematic wearing of gowns and boots at the mpoxTC. The mpoxTC next to the prison was divided into two compartments to separate suspected cases from confirmed cases. Within each compartment, there were also two compartments to separate male and female subjects.
Surveillance
Prison management indicated that it had implemented measures prior to this incident to prevent staff contamination. These measures included educating all staff about the causes and symptoms of mpox, identifying risk factors, and implementing a reporting system in the logbook, based on prison activities. Unfortunately, according to our assessment, hand hygiene measures, such as hydroalcoholic solutions and handwashing stations, were not visible at observation points. The identity of all persons entering the prison or its grounds was verified and recorded after the start of the intervention. Management indicated that all observed measures had been implemented before the first cases of mpox were confirmed. The health district intervention team, therefore, came to support the prison management to ensure compliance with all these outstanding measures, which are nevertheless known.
New entries into the prisons were stopped
Given the high number of cases recorded and the risk of infecting other inmates, the authorities of the prisons temporarily suspended the admission of new inmates. With the support of the provincial health division, the situation was quickly brought under control. Of the 69 people vaccinated, three fell ill three days later (two of them) and one of the three four days later. All inmates who tested positive were excluded from the trial programs until their recovery, in accordance with national guidelines (Table 3).
We confirmed an outbreak of mpox in the three prisons in Kinshasa, and the outbreak was believed to be due to poor infection prevention and control practices in the facility. Generally, there is less concern for people in detention and inmates, even if the country or region is already in an outbreak, which constitutes a weakness in the response that can perpetuate the epidemic. Being held in an overcrowded prison during the mpox outbreak put inmates at significant risk of contracting mpox. No cases were observed among visitors. Of the 135 contacts in the prisons, the majority (65.19%) became suspects. They were distributed among three prisons, with the majority in the first cell, where a prevalence was noted. Thus, from an epidemiological perspective, being in an overcrowded prison during the mpox outbreak appears to be the most likely driver of this epidemic. Confirmation of the diagnosis of mpox from cases in the community confirms this finding, as the virus is circulating in the city of Kinshasa [6-11]. Half of the suspected cases 51.14% were positive.
Environmental surveys corroborate our epidemiological findings and revealed serious gaps in compliance with hygiene and infection prevention and control measures in the three prisons. Both the index case and the secondary cases of mpox were recorded in the prisons, not beforehand. This suggests that the outbreak was introduced into the prisons by newly incarcerated inmate, followed by the spread of mpox within the prisons.
The attack rates for the tables ranged from 29.54% to 36.73%, with no statistically significant differences. Since each prison had more than 10 cases, it is more likely that the outbreak was brought by a newly arrived inmate. Contamination occurred through direct and indirect contact; there were no cases with subclade Ib. Non-compliance with hygiene and IPC measures, as well as overcrowding in the cells, could facilitate the spread of mpox in the cells.
Our results are consistent with those of other prison epidemics and closed places [8,11]. It is also a biologically plausible vector for the etiological agent, mpox. The exposure in question preceded the illness. Community contamination, followed by the decision to detain in the cells were positively associated with the illness. Detention in the cells was positively associated with contamination for mpox, and this association was strong for all three cells. The main symptoms of the patients were rash, fever, myalgia, and lymphadenopathy, with a hospital stay of 5-12 days. Scab and blood samples were taken for reverse transcriptase PCR confirmation of the disease. The additional cases confirm the hypothesis that detention in the cells was the vector of the epidemic.
The national level responsible for the response (PHEOC through the IMS), the Kinshasa Provincial Health Division, the Military Health Corps, and the central office of the Kokolo Health Zone were informed of the epidemic and subsequently investigated the origin of the mpox contamination before and during detention. Thorough investigations were conducted for each case.
The team recommended strengthening surveillance system, raising awareness among all inmates and prison staff about the causes and symptoms of mpox and prevention methods, identifying risk factors and implementing a reporting system in the registry, vaccinating all the community out of the prisons and all consenting inmates, decontaminating according to the patient’s course, identifying and reducing the number of visitors to the prisons, stopping new entries to the prisons, and all inmates who tested positive were excluded from court programs until their recovery in accordance with national guidelines. Structural and operational deficiencies in the prisons were identified, and prison management was supported in correcting them.
Limitation
Information bias is likely, particularly after incarcerated individuals are detained, accompanied by ongoing legal proceedings that were halted due to the epidemic. Prolonged laboratory turnaround times and the stigma associated with the mpox outbreak may have facilitated the spread of the virus, particularly from inmates in the incubation period to uninfected individuals [1-3]. Furthermore, the perceived stigma surrounding suspected cases compromised contact tracing efforts, as those affected were often reluctant to interact with investigation teams and provide accurate information.
The main objectives of this study were to confirm the epidemic, identify the mode of transmission and put in place appropriate control measures. We see in that study that an inmate has passed in three different prisons and brought mpox, all inmates were listed as contacts and followed up within 21 days, two-thirds of the contacts became suspect to mpox but only half among them were confirmed mpox cases by the laboratory with RT-PCR and sequencing. Fighting back in closed spaces requires a lot of discipline and good organization and it is necessary to isolate all suspected cases and carry out all Public Health actions and momentarily stop the arrival of new people in these closed places until the normal situation is restored, then make a new assessment before new measures to be taken.
What is already known about the topic
What this study adds
We are grateful to the command of the Military Health Corps and the Kokolo Health Zone, and to the staff of the mpox treatment center in the Kokolo Health Zone and authorities of the prison for their authorizations and support. We also thank all the staff and service providers of the mpox treatment center in the Kokolo Health Zone for their cooperation.
Amisi Kengea Levis and Ndumbi Temuangudi Vallhy conceptualised the study. Amisi Kengea Levis, Masamba Bikoki Winnie and Ndumbi Temuangudi Vally were responsible for literature and data acquisition. Amisi Kengea Levis, Wumba Mavinga Angele, Mbuyi Mutombe Anthony, Kape Kalume Jean Jacques and Nsinga Bungiena Jean Claude contributed to the literature review, analysis and data interpretation. AMISI KENGEA Levis, Nsinga Bungiena Jean Claude, Kape Kalume Jean Jacques Pamphyle, Mbuyi Mutombe Anthony, Wumba Mavinga Angele and Ndumbi Temuangudi Vally drafted the initial manuscript. Amisi Kengea Levis and Masamba Bikoki Winnie developed the second draft. All authors contributed to the final version of the manuscript, approved the final draft, and agreed to be accountable for all aspects of the work.
| Variable | Number | Attack rate (%) | Prevalence OR (95% CI) |
|---|---|---|---|
| All cases | 45 | 45/135 (33.33) | |
| Sex | |||
| Female | 5 | 5/25 (20) | 1 |
| Male | 40 | 40/110 (36.36) | 2.7 (1.31–3.04) |
| Age class* (years) | |||
| 18–28 | 11 | 11/31 (35.48) | 1 |
| 29–39 | 17 | 17/53 (32.08) | 1.5 (0.9–4.2) |
| 40–50 | 10 | 10/29 (34.48) | 2.1 (1.8–3.4) |
| 51 and + | 7 | 7/22 (31.82) | 2.2 (1.7–3.5) |
| Concerned prison | |||
| Prison 1 | 18 | 18/49 (36.73) | 1 |
| Prison 2 | 14 | 14/42 (33.33) | 2.9 (0.8–11.1) |
| Prison 3 | 13 | 13/44 (29.54) | 2.1 (0.5–8.2) |
| Variable | Number (%) | Median (range) |
|---|---|---|
| Symptoms | ||
| Fever | 42 (93.3) | |
| Skin rashes | 45 (100.0) | |
| Myalgia | 40 (88.9) | |
| Physical asthenia | 37 (82.2) | |
| Lymphadenopathy | 29 (64.4) | |
| Hospitalization | 45 (100.0) | |
| Length of hospitalization (days) | 10 (5–12) | |
| Incubation period (days) | 8 (6–11) | |
| Scab samples collected | 88 (65.2) | |
| Blood samples collected | 88 (65.2) | |
| Scab samples positive for mpox | 45/88 (51.1) | |
| Blood samples positive for mpox | 26/88 (29.5) | |
Table 3: Mpox safety and prevention measures implemented in three prisons. n=45. mpox outbreak in 3 military prisons in Kinshasa, DRC, October 2024 to January 2025
| Classification | Considerations for the prevention of mpox | Recommended changes to the prison |
|---|---|---|
| Structural | Reduce the density of people in the prison | Stop accepting too many visitors to the prison |
| *Stagger visiting hours by increasing the number of visiting shifts | ||
| Stop adding new people to the prison and release prisoners with sentences for release already pronounced | ||
| Reduce the number of people around meals | ||
| Maintain physical distancing when entering and leaving the prison | *Use of larger doors for entry and exit | |
| Functional | Maintaining physical distancing during calls and plenary sessions within the confines of the plot housing the prisons | Reduce the number of speakers per session and per workspace |
| Use of virtual means to conduct certain meetings | ||
| Isolate suspected detainees (symptomatic of mpox) | Investigate and collect all suspected cases in the prison | |
| Isolate any suspected case on site then with mpoxTC | ||
| Compliance with infection prevention and control measures | Installation of hand hygiene devices at observation points | |
| *Regular cleaning and disinfection of surfaces | ||
| Wearing of appropriate PPE, including face masks, by all officers and officials in the lockup | ||
| Socio-economic | People in detention living in densely populated and highly interactive communities | Educate people in detention about general preventive measures when they leave the prison |