Research | Open Access | Volume 9 (1): Article 43 | Published: 10 Mar 2026
Views: 62
Menu, Tables and Figures
| Province | District | Incidence rate/1000 live births (%) | ||||
|---|---|---|---|---|---|---|
| 2019 % (n/N) | 2020 % (n/N) | 2021 % (n/N) | 2022 % (n/N) | 2023 % (n/N) | ||
| Tete | Macanga | 2.2 (21/9,768) | 0.0 (0/9,209) | 0.0 (0/6,788) | 0.0 (0/8,276) | 0.0 (0/7,740) |
| Chifunde | 1.1 (7/6,559) | 0.0 (0/8,921) | 0.0 (0/7,277) | 0.0 (0/7,796) | 0.0 (0/8,310) | |
| Cidade de Tete | 1.1 (14/12,809) | 0.0 (0/12,495) | 0.0 (0/16,021) | 0.0 (0/18,087) | 0.0 (0/21,836) | |
| Manica | Tambara | 1.2 (3/2,417) | 0.0 (0/2,285) | 0.0 (0/2,574) | 0.0 (0/2,448) | 0.0 (0/2,551) |
| Macossa | 0.0 (0/2,572) | 1.1 (3/2,728) | 0.0 (0/2,777) | 0.0 (0/2,873) | 0.0 (0/2,925) | |
| Guro | 0.0 (0/5,068) | 0.0 (0/5,063) | 1.2 (6/5,179) | 1.8 (10/5,460) | 0.0 (0/5,355) | |
| Sussundenga | 0.0 (0/8,192) | 0.0 (0/8,435) | 0.0 (0/8,852) | 1.4 (13/9,409) | 0.0 (0/9,298) | |
| Nampula | Memba | 0.0 (0/10,397) | 1.0 (11/10,751) | 0.0 (0/14,514) | 0.0 (0/14,646) | 0.0 (0/15,266) |
| Mecufi | 0.0 (0/2,465) | 2.0 (5/2,465) | 1.2 (3/2,546) | 0.0 (0/2,727) | 0.0 (0/2,669) | |
| Zambézia | Luabo | 0.0 (0/1,779) | 0.0 (0/1,864) | 1.6 (3/1,919) | 0.0 (0/2,372) | 0.0 (0/2,674) |
Table 1: Districts with tetanus incidence rate ≥1/1000 live births in Mozambique, 2019 – 2023
| Attributes | Evaluation Criteria | Results and classification |
|---|---|---|
| Acceptability | It will be acceptable if the number of districts reporting cases including “0 cases” out of the total number of districts in the country is ≥90% | 86% (139/161). Rating: Not acceptable |
| Data quality | The system will be considered to be of good quality if the percentage of completion of the 19 mandatory variables (date of receipt of the form, date of notification, date of investigation of the case, date of birth, sex, age, place of birth, material used to cut the cord, mother was vaccinated, vaccination status before delivery, case classification, the baby was normal at birth, cried well, stopped sucking after 2 days, muscle stiffness, spasm, opisthotonus) is ≥ 90%. | 17 variables reached ≥95% One variable reached 93% and one variable 92% Rating: Good quality |
| Will be considered of good quality if all the variables in the database correspond to those in the investigation form | 14 variables of the database are not included in the investigation form Rating: Poor quality. The final data quality rating was intermediate, as it meets one of the criteria | |
| Stability | It will be stable if the dependence on the functioning of the system is mostly on the state fund, otherwise it will not be stable. | Yes, the system works mainly with state funds. Rating: Stable |
| Representativeness | Level of installation of the neonatal tetanus surveillance system in Mozambique, if national level (all districts) stable, if some districts, not stable. | Surveillance is installed in all districts. Rating: Representative |
| Reporting of institutional and non-institutional births. If information is reported on institutional and non-institutional births, it is representative; if only one group is reported it is not representative. | The system collects information on institutional and non-institutional births. Rating: Representative The system was considered representative because it meets both criteria. | |
| Utility | Data from the NNT surveillance system is used to estimate incidence and mortality rates. It will be useful if it captures data on deaths and new cases. | Yes – the database captures deaths and new cases. Rating: Useful |
| The data is used to identify areas at high risk of neonatal tetanus. It will be useful if the data collected allows the calculation of neonatal tetanus incidence rates. | Yes – through incidence rate by district. Rating: Useful | |
| It will be useful if the data collected allows the evaluation of the effect of the interventions. | Coverage of mothers whose children were confirmed with NNT was 46% (245/533). Rating: Useful | |
| It will be useful if the data collected is used to design strategies that support the elimination of TMN in Mozambique. | Yes, they allow for guiding vaccination campaigns. Rating: Useful |
* VAT2+: two or more doses of anti-tetanus vaccination; NNT: neonatal tetanus.
![Figure 2: Overall distribution of neonatal tetanus data in Mozambique, 2019-2023 [*TNN: neonatal tetanus, RN: newborn, Confirmed: suspected cases of NNT* that meets three criteria: 1) Newborn* who was born well, with normal ability to suck and cry during the first two days of life; 2) stopped sucking normally between 3rd and 28th day of life; 3) developed convulsions, muscle rigidity, opisthotonus or one of these. Discarded: suspected case of NNT that presents some clinical criteria, but does not meet all the requirements for confirmation. Unclassified: suspected case of TNN not investigated or with insufficient information to confirm or rule out.]](https://afenet-journal.org/wp-content/uploads/2026/03/Screenshot-2026-03-10-at-11.47.03.png)
José Vasco Jemusse1,& ,Taiobo Martins Jamal2, Domingos Guihole2, Érika Valeska Rossetto3, Adilson Fernando Bauhofer4, Áuria Ribeiro Banze1
1Programa de Formação em Epidemiologia de Campo, Moçambique, Instituto Nacional de Saúde, Maputo, Moçambique, 2Departamento de Vigilância em Saúde, Ministério da Saúde, Maputo, Moçambique, ³Instituto Nacional de Saúde, Maputo, Moçambique, 4Programa de Formação em Epidemiologia de Campo, Moçamb
&Corresponding author: José Vasco Jemusse, Field Epidemiology Training Program, National Health Institute, Mozambique. Email: jose.jemusse@ins.gov.mz, josevjemusse2@gmail.com ORCID: https://orcid.org/0009-0001-2467-6377
Received: 06 Oct 2025, Accepted: 06 Mar 2026, Published: 10 Mar 2026
Domain: Maternal and Child Health
Keywords: Surveillance system, tetanus, neonatal, Mozambique
©José Vasco Jemusse et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: José Vasco Jemusse et al., Evaluation of the neonatal tetanus surveillance system in Mozambique, 2019-2023. Journal of Interventional Epidemiology and Public Health. 2026; 9(1):43. https://doi.org/10.37432/jieph-d-25-00223
Introduction: Neonatal tetanus (NT) remains a public health problem in low- and middle-income countries. In several countries, surveillance systems for NT are not well established, and the incidence is not well known. The aim of this study was to evaluate the surveillance system for neonatal tetanus.
Methods: This evaluation was conducted in Mozambique, from 2019 to 2023, using the guidelines of Centers for Disease Control and Prevention for evaluating public health surveillance systems. The system’s utility, its acceptability and data quality attributes were evaluated. Acceptability was considered adequate if ≥ 90% of districts, including those reporting “0 cases”, submitted reports. Data quality was considered good if completeness of the mandatory fields reached ≥ 90% and database variables matched the investigation form, intermediate if only one criterion was met, and poor if neither was met. Usefulness was evaluated by the system’s ability to identify high-risk areas through incidence rates.
Results: The NT surveillance system, in the acceptability attribute, found that 86.3% of districts reported cases. Field completeness reached 92%. However, when comparing the variables in the database and the investigation form, it was found that there are 14 variables in the database that are not included in the investigation form. The usefulness of the surveillance system was confirmed by the identification of 10 high-risk districts with a neonatal tetanus incidence rate of one or more per 1000 live births.
Conclusions: The surveillance system for neonatal tetanus in Mozambique demonstrated weaknesses in acceptability and intermediate data quality but proved useful for guiding public health policies.
Tetanus is an infectious disease caused by the bacteria Clostridium tetani [1]. Transmission occurs indirectly when an open wound on the skin comes into contact with a surface contaminated with the bacteria [2]. The diagnosis is clinical and does not require laboratory confirmation [3,4]. It is a vaccine-preventable disease.
Neonatal tetanus is described as the occurrence of tetanus during the first 28 days of a newborn’s life [5], which manifests as progressive difficulty in sucking, excessive crying, with or without opisthotonus, muscular hypertonia, hyperreflexia, muscle rigidity, and/or spasms [3,6]. In settings with limited resources and inadequate medical care, the case fatality rate of neonatal tetanus can reach as high as 100%. However, with access to basic medical care, this rate can be reduced by half, and with intensive care, it can be further decreased to 10–20% [7,8].
The prevention of neonatal tetanus relies on the vaccination of pregnant women and women of childbearing age, combined with hygienic delivery practices and proper umbilical cord care. Furthermore, robust surveillance systems are critical for promptly detecting cases and identifying gaps in immunization and safe delivery practices, enabling timely preventive interventions [3,9,10].
The World Health Organization estimated that approximately 24,000 newborns died from neonatal tetanus worldwide in 2021, reflecting an 88% reduction from the 200,000 deaths reported in 2000[11]. However, the global burden of tetanus remains significant, particularly neonatal tetanus, in some underdeveloped countries [12]. Global tetanus elimination is defined as an annual rate of < 1 case per 1000 live births in each district or similar administrative unit of a country [10].
In Mozambique, the neonatal tetanus mortality rate was reduced by almost half, falling from 54 deaths per 1000 live births in 1997 to 24 deaths per 1000 live births in 2018 [13]. According to the global tetanus elimination agenda, Mozambique considered maternal and neonatal tetanus eliminated since 2010 [14]. Mozambique has implemented a neonatal tetanus surveillance system to identify neonatal tetanus cases early and prevent the emergence of new cases. Additionally, the system aimed to identify high-risk areas to guide tetanus vaccination campaigns for pregnant women and women of childbearing age. It also seeks to measure progress by district towards the elimination of neonatal tetanus and monitor the state of elimination [15]. This study aimed to evaluate the performance of Mozambique’s neonatal tetanus surveillance system between 2019 and 2023.
We evaluated the epidemiological surveillance system for neonatal tetanus in Mozambique from 2019 to 2023, following the U.S. Centers for Disease Control and Prevention (CDC) Updated Guidelines for Evaluating Public Health Surveillance Systems: Recommendations from the Guidelines Working Group 2001[16]. In this study, we analyzed all reported cases of neonates with suspected tetanus obtained from a secondary database of the national neonatal tetanus surveillance system, covering January 1, 2019, to December 31, 2023, provided by the Ministry of Health. We evaluated the usefulness of the system, along the qualitative attributes (data quality and acceptability) and quantitative attributes (representativeness and stability) [16]. Bibliographic and documentary reviews were conducted to describe the surveillance system. Attributes were evaluated using pre-established criteria and defined according to the attribute specificity and score-based classification.
Description of the neonatal tetanus surveillance system in Mozambique
Neonatal tetanus is a notifiable disease in Mozambique, and its surveillance system forms part of the Integrated Disease Surveillance and Response (IDSR) strategy. This system facilitates interoperability with the Expanded Vaccination and Maternal Health Program for children and tracks the implementation of its interventions.
The surveillance system in Mozambique was established shortly after independence in 1976, and this is the first evaluation of the attribute-based neonatal tetanus surveillance system. Neonatal tetanus surveillance system in Mozambique is a national, case-based, passive surveillance system. This surveillance is guided by the Integrated Disease Surveillance and Response Manual, Neonatal Tetanus Norms and Procedures, and WHO guidance documents on neonatal tetanus. However, there is no national manual to guide this surveillance.
Mozambique’s neonatal tetanus surveillance system aims to ensure the early detection and confirmation of cases, prevent avoidable deaths, identify high-risk areas, and guide vaccination strategies for women of reproductive age, thereby supporting sustained elimination efforts. The system covers all live births, with suspected cases defined as newborns who develop tetanus-like illness or die from unknown causes within the first 28 days of life. Surveillance activities are coordinated nationally by an epidemiologist and supported by routine surveillance staff and government funding through the Department of Health Surveillance
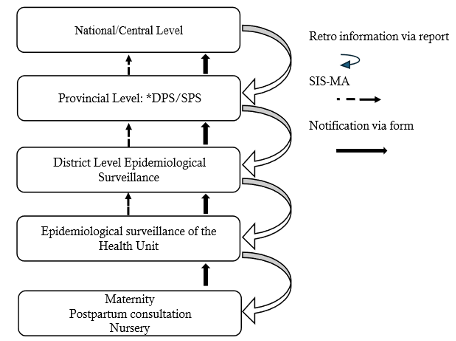
When a community suspects a case, they send the case to the health unit where the case is evaluated in the maternity ward. The doctors and/or nurses assess the case base on the signs and symptoms and notify the epidemiological surveillance unit of the health unit immediately (within 24 hours) if they suspect NT and then investigation is done by filling the case investigation form and making the final classification according to the clinical criteria and sending the form to the district. The district sends the form to the province, and finally, the province sends it to the central level. And at the end of each year, feedback is sent in the form of a report (Figure 1).
Case Definitions
Confirmation of neonatal tetanus cases was based exclusively on clinical criteria, using the national standard case definition for neonatal tetanus. Cases were confirmed as clinically compatible during case investigation when all three criteria were met: (1) the newborn was healthy at birth and able to suck and cry normally during the first two days of life; (2) the newborn was unable to suck normally between days 3 and 28 of life; and (3) the newborn developed one or more clinical signs consistent with neonatal tetanus, including convulsions, muscle rigidity, or opisthotonos. Case confirmation was performed through review of surveillance reports by trained surveillance officers at health facility, district, and provincial levels, based on clinical assessments documented by the managing clinicians.
Discarded case: A suspected case of neonatal tetanus (NNT) that, after investigation, does not meet the clinical criteria for confirmation or has an alternative diagnosis [8,11].
Unclassified: A suspected neonatal tetanus case not investigated or with insufficient information to confirm or rule out [8,11].
Data source and collection
Data for this study were obtained from the national neonatal tetanus surveillance system coordinated by the Ministry of Health of Mozambique, which routinely collects data from all public health facilities nationwide through the continuous notification of suspected cases. Case notification, investigation, and classification follow the guidelines in use within the country. All suspected cases undergo detailed investigation and clinical verification prior to final classification.
As this is a routine surveillance system, it is expected that a substantial proportion of initially suspected cases will not be confirmed following investigation. Considering that final classification occurs at the central level and that data are reported by multiple health facilities with varying levels of staff qualification, some variability in data completeness and in the application of the case definition may occur during the reporting process. Consequently, not all reported suspected cases are expected to fully meet the case definition criteria and are therefore classified as non-confirmed cases.
Attributes evaluated
Acceptability: reflects the willingness of individuals and/or organizations to participate in the surveillance system [16]. In the context of neonatal tetanus surveillance, this attribute was defined by the willingness of districts to report cases, including ‘0’ cases, according to the national surveillance design. For the assessment, the percentage of districts reporting cases, including “0 cases”, was calculated as a proportion of all districts in Mozambique. The system was considered acceptable if ≥90% of districts reported; otherwise, it was deemed unacceptable.
Data quality: reflects the completeness and validity of the data recorded in the public health surveillance system [16]. To assess this attribute, we verified the completeness of the mandatory variables in suspected cases, considering ≥90% as good quality and <90% as poor quality. We also assessed the consistency between the database variables and the investigation form, which was considered good if all database variables corresponded to those in the form. Overall, data quality was classified as good if both criteria were met, intermediate if only one criterion was met, and low if neither was met.
Stability: refers to the ability of the surveillance system to operate continuously and reliably, ensuring the availability of information critical to public health [16]. Given the strong influence of financial sustainability on system stability, this attribute was assessed through a document review.
A document review was conducted of official documents from the Department of Health Surveillance (DVS), including annual operational plans and annual reports. These documents were analyzed to determine the main source of funding for the neonatal tetanus surveillance system and to assess the level of implementation of planned activities and the execution of allocated funds. The surveillance system was considered stable when its operations were predominantly funded by government resources.
Representativeness: this attribute ensures that the surveillance system adequately represents the monitored population [16]. It was assessed by the level of installation of the neonatal tetanus surveillance system in Mozambique (national – all districts or partially some districts) and the capacity to report institutional and non-institutional births, if it reports all births and at all levels it is representative, otherwise it is not representative. The neonatal tetanus surveillance system operates within the integrated disease surveillance framework and includes community-based surveillance. Local actors, including traditional healers, community leaders, and traditional midwives, serve as trained community focal points to identify suspected neonatal tetanus cases occurring outside health facilities and refer them to the nearest health unit for notification and care. This approach helps capture cases that develop after discharge or that seek care outside formal health services.
Utility: determines the relevance and usefulness of surveillance data for public health action and health policy development [16]. The utility of the system assessed whether the data in the system could be used to calculate the incidence and mortality rate of neonatal tetanus, to identify high-risk areas through incidence by district and percentage of non-institutionalised births, and to evaluate the interventions of the Expanded Vaccination Program through the coverage rate of two or more doses of anti-tetanus vaccine.
Ethical considerations
The study was approved by the Institutional Bioethics Committee for Health at the Faculty of Medicine and Maputo Central Hospital (CIBS-FM&HCM, No. 16/2025). The data were obtained from the surveillance system without direct contact with participants and with authorization from the Ministry of Health. To ensure confidentiality and anonymity, all identifiable information, including the names of newborns and parents, was removed. Access to the database was limited to the research team, and the data was stored on the investigator’s secure drive and encrypted.
Data Description of the Neonatal Tetanus Surveillance System in Mozambique (2019 – 2023)
Between 2019 and 2023, 1,492 suspected cases of neonatal tetanus were registered in Mozambique, but 56 of these were duplicates, which were removed. After data cleaning, 1,436 cases were preliminarily analysed. Of these, 67.1% (964 cases) were in the recommended age range (3–28 days) for suspected neonatal tetanus, whereas 32.9% (472 cases) were outside this range.
In the final analysis, 964 cases were included. Of these, 50.3% were male, and 49.7% were female. Of the cases, 55.3% (533/964) were confirmed, of which 50.3% (268/533) were male, 39.6% (382/964) were discarded, and 5.1% (49/964) were unclassified (Figure 2).
Attribute evaluation results
Acceptability: The percentage of districts reporting cases was 86.3% (139/161), below the proposed criterion of 90% of districts for neonatal tetanus reporting. Accordingly, this attribute was classified as not acceptable (Table 2).
Data quality in the database: The data quality of the surveillance system was considered intermediate because it met only one of the criteria. The completeness of the fields for mandatory variables (date of receipt of the form, date of notification, date of case investigation, date of birth, sex, age, place of birth, material used to cut the cord, mother vaccinated, vaccination status before delivery, case classification, baby was normal at birth, cried well, stopped sucking after 2 days, muscle rigidity, spasm, opisthotonus) reached 92%, meeting the criteria for data completeness (≥90%). However, when comparing the variables in the database with those in the investigation form, 14 variables (received date, case investigated date, nearest health facility, medical number, date of response for supplemental, date of response, district code, reporting district, case number, town/city, address, facility, mother given protection dose of TT within 3 mothers of report and supplemental immunization within same locality as the case) were identified in the database that were not included in the form. This discrepancy likely occurred because, at the time the database was created, the investigation forms were already in use, and a corresponding form aligned with the database was not updated, which contributes to poor data quality. Of these variables, three were filled in outside the form, while the remaining 11 were left empty in the database.
Stability: To conduct neonatal tetanus activities, the surveillance system is dependent on the state budget for its operations. Currently, neonatal tetanus surveillance does not have a specific partner, but the system continues to operate and meet its objectives, with support from other programs for supervision and training activities. On this criterion, the system is stable (Table 2).
Representativeness: The neonatal tetanus surveillance system is implemented in all districts and health units, capturing information on both institutional and non-institutional births. Based on these two criteria, the system was considered representative (Table 2).
Utility: The utility of this surveillance system identified 10 districts across four provinces (Manica, Tete, Nampula, and Zambézia), four of which are in Manica Province, with a neonatal tetanus incidence ≥1 per 1,000 live births. The highest numbers of cases were reported in the following districts: in 2019, Macanga District (Tete Province) reported 21 cases with an incidence of 2.2 per 1,000 live births; in 2020, Mecúfi District (Nampula Province) recorded 5 cases at 2.0 per 1,000 live births; in 2021, Luabo District (Manica Province) reported 3 cases corresponding to 1.6 per 1,000 live births; and in 2022, Guro District (Manica Province) reported 10 cases corresponding to 1.8 per 1,000 live births (Table 1). Of the 533 suspected cases of neonatal tetanus, mother of 245 cases received two or more doses of tetanus vaccine, and the coverage was 46% (245/533) versus ≥ 80% predicted by vaccination program (Table 2).
This is the first evaluation of the neonatal tetanus surveillance system in Mozambique since its creation in 1976. In Yemen, the neonatal surveillance system was evaluated a decade after its creation (2021 versus 2009) [17]. According to the World Health Organization, the neonatal tetanus surveillance system should be evaluated every five years [15], however, both Mozambique and Yemen have not complied with this recommendation.
This evaluation revealed that all variables from the investigation form are included in the database. However, the database contains additional variables that are not part of the form, which contributed to inconsistence and affected the quality, analysis and stability of the data. When the database was created, the investigation forms were already in use, however, a corresponding form aligned with the database was not updated, probably due to lack of funding. Centers for Disease Control and Prevention recommends that the variables in the database must be the same as those in the notification/investigation form [18].
The findings of this evaluation on the acceptability of the neonatal tetanus surveillance system were low, showing similarity to the results found in a study carried out in Yemen [17], which indicated an average acceptability of 64%, rating the system with a similar weight. Although the study in Yemen used interviews to assess acceptability, both studies did not find a good rating for the acceptability of the neonatal tetanus surveillance system. This shows that, in both Yemen and Mozambique, the surveillance system has an acceptability below the level considered good.
The low acceptability found in neonatal tetanus surveillance in Mozambique reflect similar challenges previously faced by Uganda [19]. To improve the integrated disease surveillance and response system, Uganda implemented several effective measures such as, training in integrated surveillance which increased the capacity of technicians in data analysis from 47% in 2004 to 54% in 2016, strengthening feedback increased communication between the different levels of health, rising from 55% in 2004 to 87% of health facilities receiving regular feedback in 2016 which culminated in technician motivation, engagement and improved data [19]. Uganda also formed district epidemic response committees, improving outbreak reporting from 46% to 58% in 2016 [19]. These strategies can be adapted to improve the system under evaluation in Mozambique.
The utility assessment demonstrates that the neonatal tetanus surveillance system in Mozambique is useful in identifying high-risk districts and critical gaps in maternal vaccination coverage. While the surveillance system generates actionable evidence to guide elimination efforts, the translation of this evidence into interventions and policies depends on programmatic decision-making, resource availability, and implementation capacity, which are beyond the direct scope of the surveillance system itself. These findings also suggest that neonatal tetanus may still be present in Mozambique and highlight the urgent need for a new study to assess the current status of elimination efforts in the country. Similar results were found in 2010 by a joint team from WHO, UNICEF and the Expanded Program of Vaccination (EPV) of the Mozambican Ministry of Health, which found 11 high-risk districts in the first phase of the assessment to validate neonatal tetanus elimination [14], which motivated them to conduct a more in-depth study that allowed neonatal tetanus to be declared eliminated in the country.
Study limitations
One limitation encountered during the evaluation was related to the assessment of timeliness, specifically the calculation of the interval between case notification and case investigation. This limitation arose from the structure of the case investigation form, which uses a single field to record both the date of notification and the date of investigation in the database. Consequently, it was assumed that all reported cases were investigated on the same day, which may have biased the interpretation of the timeliness attribute. An additional limitation relates to the interpretation of the non-updating of the case investigation form. The term “probably lack of funding,” used in the discussion, reflects the absence of documented evidence formally explaining why the form was not updated at the time the database was developed. Although neonatal tetanus is a priority disease in Mozambique and is included among the ten notifiable diseases with weekly reporting through the National Epidemiological Bulletin, some post-validation activities, including the updating of investigation instruments, faced operational and financial constraints, limiting the ability to draw definitive conclusions regarding the underlying causes.
The results of this evaluation show that the neonatal tetanus surveillance system in Mozambique is both representative and stable. However, it demonstrates weakness in data quality and acceptability, characterized by intermediate data quality and low level of acceptability. These findings reinforce the need for priority interventions, including awareness-raising activities targeting health professionals, continuous capacity-building, and strengthening feedback mechanisms is also essential to improve adherence to the standard case definition by reporting personnel, thereby reducing misclassification and the reporting of cases outside the defined neonatal period. In addition, it is essential to update the case investigation form to ensure greater consistency and standardization of the information generated, thereby contributing to improved case reporting across all districts.
Despite these challenges, the surveillance system has proven useful for identifying high-risk districts and critical gaps in maternal immunization coverage. While it generates actionable evidence to guide elimination efforts, the translation of this evidence into interventions and policies depends on programmatic decision-making, resource availability, and implementation capacity, which are beyond the direct scope of the surveillance system.
Recommendations
It is recommended that a national surveillance manual of neonatal tetanus be developed to guide the implementation of this surveillance, that the variables in the database be harmonized with those in the case investigation form, and that an in-depth prevalence study be conducted in the districts identified with an incidence rate ≥ 1 per 1000 live births, particularly in the provinces of Manica, Tete and Cabo Delgado to assess the current status of neonatal tetanus elimination.
What is already known about the topic
What this study adds
This study has been supported by the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) through the Centers for Disease Control and Prevention (CDC). The findings and conclusions in this paper are those of the author(s) and do not necessarily represent the official position of the funding agencies.
| Province | District | Incidence rate/1000 live births (%) | ||||
|---|---|---|---|---|---|---|
| 2019 % (n/N) | 2020 % (n/N) | 2021 % (n/N) | 2022 % (n/N) | 2023 % (n/N) | ||
| Tete | Macanga | 2.2 (21/9,768) | 0.0 (0/9,209) | 0.0 (0/6,788) | 0.0 (0/8,276) | 0.0 (0/7,740) |
| Chifunde | 1.1 (7/6,559) | 0.0 (0/8,921) | 0.0 (0/7,277) | 0.0 (0/7,796) | 0.0 (0/8,310) | |
| Cidade de Tete | 1.1 (14/12,809) | 0.0 (0/12,495) | 0.0 (0/16,021) | 0.0 (0/18,087) | 0.0 (0/21,836) | |
| Manica | Tambara | 1.2 (3/2,417) | 0.0 (0/2,285) | 0.0 (0/2,574) | 0.0 (0/2,448) | 0.0 (0/2,551) |
| Macossa | 0.0 (0/2,572) | 1.1 (3/2,728) | 0.0 (0/2,777) | 0.0 (0/2,873) | 0.0 (0/2,925) | |
| Guro | 0.0 (0/5,068) | 0.0 (0/5,063) | 1.2 (6/5,179) | 1.8 (10/5,460) | 0.0 (0/5,355) | |
| Sussundenga | 0.0 (0/8,192) | 0.0 (0/8,435) | 0.0 (0/8,852) | 1.4 (13/9,409) | 0.0 (0/9,298) | |
| Nampula | Memba | 0.0 (0/10,397) | 1.0 (11/10,751) | 0.0 (0/14,514) | 0.0 (0/14,646) | 0.0 (0/15,266) |
| Mecufi | 0.0 (0/2,465) | 2.0 (5/2,465) | 1.2 (3/2,546) | 0.0 (0/2,727) | 0.0 (0/2,669) | |
| Zambézia | Luabo | 0.0 (0/1,779) | 0.0 (0/1,864) | 1.6 (3/1,919) | 0.0 (0/2,372) | 0.0 (0/2,674) |
| Attributes | Evaluation Criteria | Results and classification |
|---|---|---|
| Acceptability | It will be acceptable if the number of districts reporting cases including “0 cases” out of the total number of districts in the country is ≥90% | 86% (139/161). Rating: Not acceptable |
| Data quality | The system will be considered to be of good quality if the percentage of completion of the 19 mandatory variables (date of receipt of the form, date of notification, date of investigation of the case, date of birth, sex, age, place of birth, material used to cut the cord, mother was vaccinated, vaccination status before delivery, case classification, the baby was normal at birth, cried well, stopped sucking after 2 days, muscle stiffness, spasm, opisthotonus) is ≥ 90%. | 17 variables reached ≥95% One variable reached 93% and one variable 92% Rating: Good quality |
| Will be considered of good quality if all the variables in the database correspond to those in the investigation form | 14 variables of the database are not included in the investigation form Rating: Poor quality. The final data quality rating was intermediate, as it meets one of the criteria | |
| Stability | It will be stable if the dependence on the functioning of the system is mostly on the state fund, otherwise it will not be stable. | Yes, the system works mainly with state funds. Rating: Stable |
| Representativeness | Level of installation of the neonatal tetanus surveillance system in Mozambique, if national level (all districts) stable, if some districts, not stable. | Surveillance is installed in all districts. Rating: Representative |
| Reporting of institutional and non-institutional births. If information is reported on institutional and non-institutional births, it is representative; if only one group is reported it is not representative. | The system collects information on institutional and non-institutional births. Rating: Representative The system was considered representative because it meets both criteria. | |
| Utility | Data from the NNT surveillance system is used to estimate incidence and mortality rates. It will be useful if it captures data on deaths and new cases. | Yes – the database captures deaths and new cases. Rating: Useful |
| The data is used to identify areas at high risk of neonatal tetanus. It will be useful if the data collected allows the calculation of neonatal tetanus incidence rates. | Yes – through incidence rate by district. Rating: Useful | |
| It will be useful if the data collected allows the evaluation of the effect of the interventions. | Coverage of mothers whose children were confirmed with NNT was 46% (245/533). Rating: Useful | |
| It will be useful if the data collected is used to design strategies that support the elimination of TMN in Mozambique. | Yes, they allow for guiding vaccination campaigns. Rating: Useful |
* VAT2+: two or more doses of anti-tetanus vaccination; NNT: neonatal tetanus.