Research | Open Access | Volume 9 (1): Article 38 | Published: 04 Mar 2026
Views: 29
Menu, Tables and Figures
| Attributes | Indicators | How it was assessed | Data collection tools |
|---|---|---|---|
| Simplicity | Structure and ease of operation | • Assessed the processes involved in the surveillance • Ease of case definition to identify OD communities • Steps of how data/reports are submitted, collated, analyzed and distributed | Records review Interview Observation |
| Flexibility | Variability of adapting to changing needs and conditions | • Modifications and new introduction to systems operation and how system adapted within 2019 to 2023 | Interview Records review |
| Acceptability | Willingness of stakeholders to participate in the process | • Reporting rates of sub districts to the district and to the region • Data completeness | Interview Records review Observation |
| Representativeness | Variability in the distribution of latrines and ODFs by councils (sub districts) | • Distribution of toilets in the communities within 2019–2023 • ODF declaration within 2019–2023 | Records review |
| Stability | Reliability of the system, and its ability to work when needed | • Resources available to collect, manage and provide data when needed • Source of funding of the operation | Interview |
| Data Quality | Completeness and validity of the data in the system | • Data completeness of baseline, triggering and end line forms • Proper documentation and reporting from 2019–2023 | Records review |
| Timelines | Mean time between triggering and declaration of ODF | • Timelines between triggering and ODF declaration • Reporting timelines for 2019–2023 | Records review Interview |
Table 1: Indicators used in assessing the system attributes
| Sub District | Number of Communities | Communities Triggered | Number of ODF Communities | Proportions (%) |
|---|---|---|---|---|
| Bongo Central | 34 | 14 | 7 | 50.0 |
| Balungu | 20 | 9 | 5 | 55.6 |
| Namoo | 33 | 13 | 9 | 69.2 |
| Soe | 17 | 7 | 5 | 71.4 |
| Beo | 22 | 8 | 4 | 50.0 |
| Zorko | 23 | 9 | 5 | 55.6 |
| Valley Zone | 19 | 6 | 2 | 33.3 |
| Total | 168 | 66 | 37 |
Table 2: Distribution of CLTS surveillance system in Subdistricts within Bongo District, 2019-2023
Dora Pakindam1, Rita Agyekumwah Asante Kusi2,3,&, Samuel Dapaa2, Charles Noora Lwanga2, Joseph Asamoah Frimpong2, Samuel Sackey2, Ernest Kenu2
1Environmental Health and Sanitation Department, Bongo, Upper East Region, 2University of Ghana, School of Public Health, Legon, Ghana, 3Food and Drugs Authority, Accra Ghana
&Corresponding author: Rita Asante Kusi: University of Ghana, School of Public Health, Legon, Ghana, Email: angeasante@yahoo.com, rita.asante@fda.gov.gh ORCID: https://orcid.org/0000-0003-1907-3667
Received: 20 Nov 2025, Accepted: 02 Mar 2026, Published: 04 Mar 2026
Domain: Environmental Health
Keywords: Sanitation, open defecation, Bongo, Ghana, latrine
©Rita Asante Kusi et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Rita Asante Kusi et al., Evaluation of the community-led total sanitation in Bongo District, Ghana, 2024. Journal of Interventional Epidemiology and Public Health. 2026; 9(1):38. https://doi.org/10.37432/jieph-d-25-00293
Introduction: Open defecation increases the spread of diarrhoea illnesses, especially among children under five years in Ghana. Community-led total sanitation (CLTS) is an intervention implemented by the Environmental Health and Sanitation Department (EHSD) to stop open defecation. We evaluated the objectives, attributes, and usefulness of the CLTS surveillance system in the Bongo District, Upper East Region, Ghana.
Methods: Adapting the Centers for Disease Control and Prevention updated guidelines for evaluating public health surveillance systems, the CLTS system was evaluated from 2019 to 2023 using a semi-structured questionnaire. Data was collected through interviews, observations and review and summarised as frequencies, proportions and text.
Results: The CLTS system was triggered in 39.3% (66/168) of communities, with 56.1% (37/66) declared Open Defecation Free (ODF). About 619 latrines were constructed over the evaluation period, with 66.7% (14/21) of stakeholders interviewed having latrines in their homes and 52.4% (11/21) having handwashing facilities. About 85.7% (18/21) of community members were aware of faeco-oral transmission of diseases. Introduction of the Basic Sanitation Information System (BaSIS) data source in 2022 did not interrupt the system’s operations. All nine key informants stated that it is easy to identify an OD and ODF community using observation. Data completeness among all seven reporting units was 89.2% (34/37), with 100% reporting. The stability of the system is compromised as it largely depends on Non-Governmental Organisations (NGOs), coupled with a lack of computers for data storage. Triggering and ODF declaration took three to six months.
Conclusion: The CLTS system was found to meet its objectives and is useful. It was acceptable, flexible, simple, with good data quality and representative. Reporting timeliness was good, with poor stability. The Government should provide budgetary support to the EHSD to effectively implement CLTS surveillance system.
About 3.4 billion people globally lacked access to improved latrines in 2022 and the situation is even worse in the Sub-Saharan African countries [1]. This situation leads to open defecation (OD) which is affecting almost one billion people worldwide and contributing to an estimated 842,000 sanitation-related deaths [2].
As of 2021, people practicing OD in Ghana were reported to be 17.7% leading to annual losses of about US$ 290 million [3]. Open defecation is more prevalent in the Northern zone of Ghana with the Upper East Region having 70.3% as the highest [4]. A major intervention for improving sanitation access is Community-Led Total Sanitation (CLTS), a non-subsidized approach that focuses on igniting a change in sanitation behavior rather than constructing toilets. This is done through a process of social awakening stimulated by facilitators from within or outside the community [5]. The goal of CLTS is to end OD and sustain an Open Defecation Free (ODF) status.
A randomized controlled trial in rural Ghana on impact of subsidies in ODF communities observed substantial differences in sanitation outcomes between subsidy and control communities at end line [6]. Another study in rural Ghana found that 75% of ODF communities did not meet Ghana’s ODF requirements [7]. Evaluation of CLTS surveillance system is crucial in tailoring intervention leading to the achievement of ODF communities. Bongo is among the districts with high open defecation rates in Upper East Region ranging from 81.7% to 89.6% [8]. We evaluated the implementation of CLTS surveillance system in Bongo District of the Upper East Region from 2019 to 2023 to determine if the system’s objectives are being met, assess its usefulness and attributes.
Evaluation design
We conducted a cross-sectional study to evaluate the CLTS surveillance system in Bongo District between the periods of 2019 and 2023. The CDC Updated Guidelines for Evaluating Public Health Surveillance Systems, were adapted for the evaluation [9], which was conducted from May 7 to June 14, 2024. We described the attributes and effectiveness of the community-led total sanitation surveillance system in the Bongo District of the Upper East Region from 2019 to 2023 employing interviews, observation and a retrospective document review.
Evaluation setting
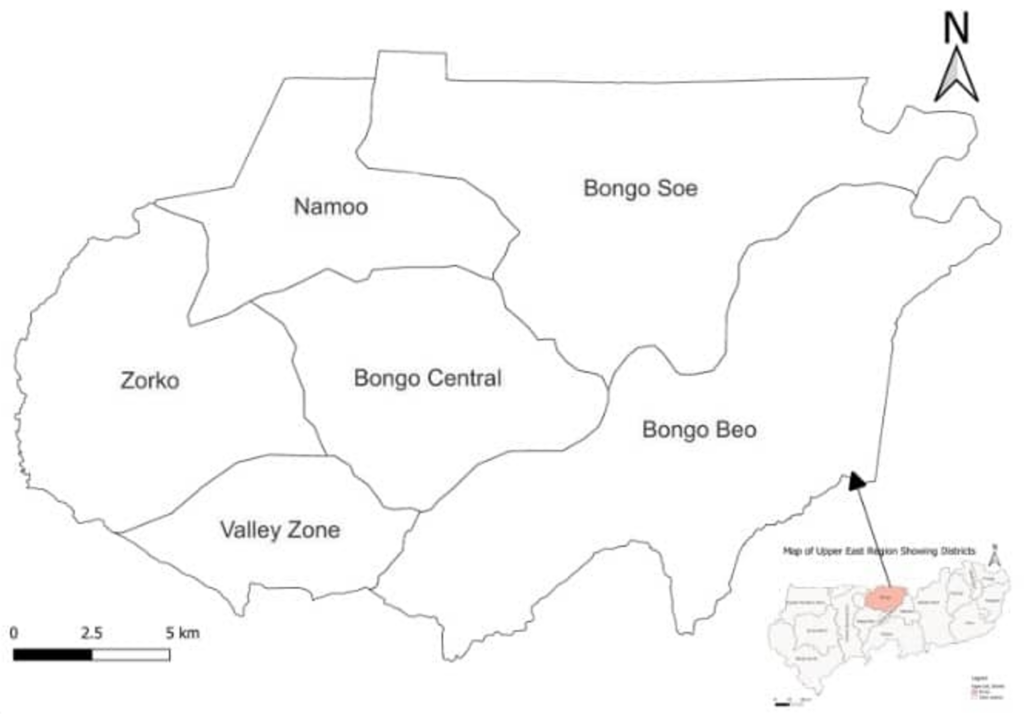
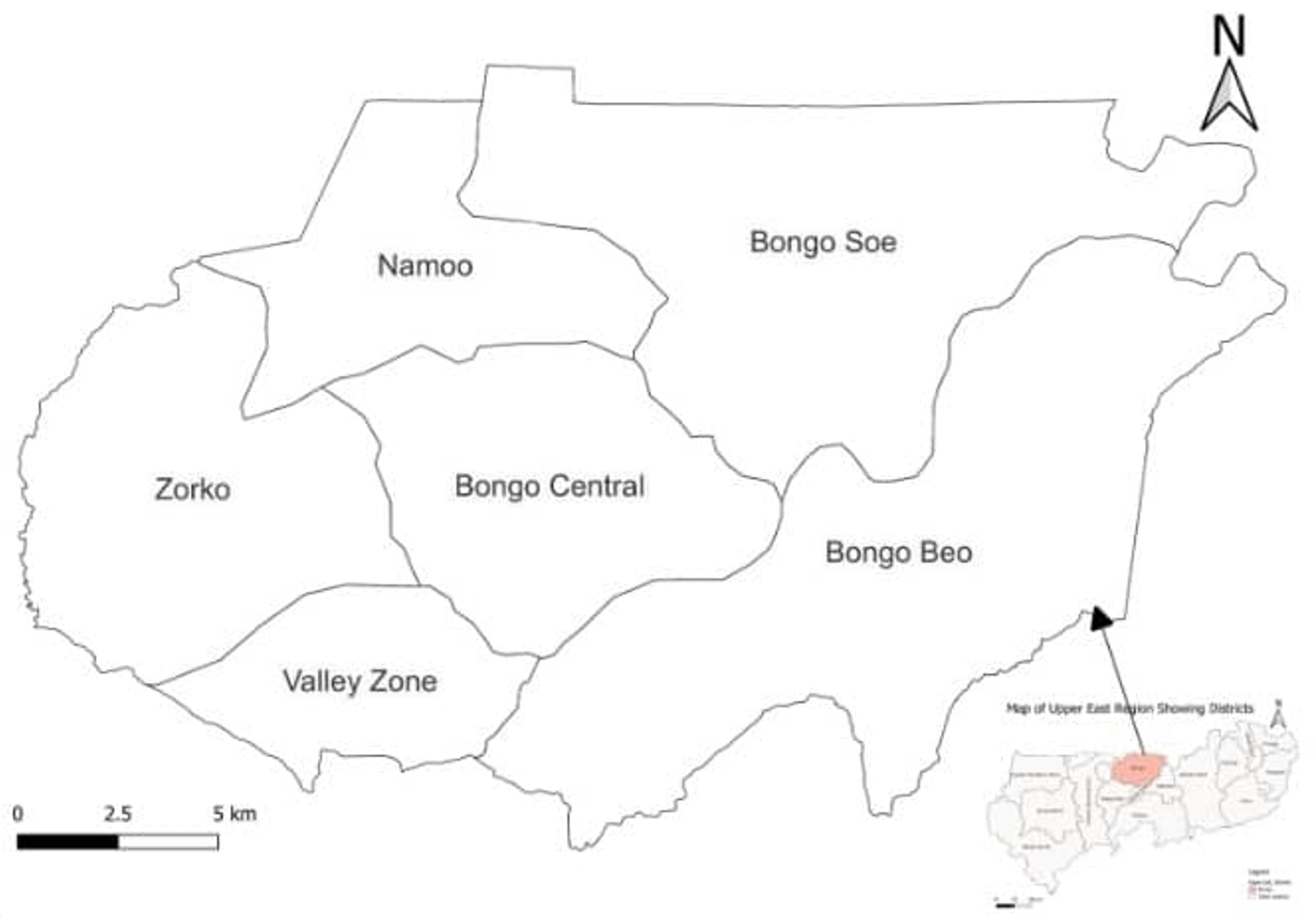
Bongo District (Figure 1) is one of the fifteen (15) districts in the Upper East Region of Ghana with Bongo as its capital. The district shares boundaries with Burkina Faso to the North, Kassena-Nankana Municipality and Kassena-Nankana West District to the West, Bolgatanga Municipality to the Southwest, and Nabdam District to the southeast. Bongo District’s estimated population was 120,254, with females constituting 63,334 (52.7%) based on the 2021 housing and population census[10]. Parts of the district are rocky terrain and serve as hidden places for open defecation. CLTS is being implemented in 30 communities across the seven area councils, namely Bongo Central, Valley Zone, Beo, Namoo, Balungu Zorko and Soe. The district has 25 Environmental Health Officers with 60% (15/25) currently trained on CLTS.
Operations of the CLTS surveillance system
The goal of CLTS is to end open defecation (OD) and sustain an open defecation-free (ODF) status. An OD community is any community where people defecate in open places, such as bushes, fields, water bodies, forest among others, rather than using a latrine or toilet, whereas an ODF community refers to any community with no visible sign of open defecation, with at least 80% of households having latrines and hand washing facilities [7]. CLTS facilitators attempt to trigger collective behaviour change by encouraging and motivating people to confront the impact of community-wide open defecation. To facilitate a community to achieve ODF status the following CLTS stages need to be followed;
Resources required for CLTS operations include motorbikes, computers, smartphones, tablets, fuel, financial resources, vehicles and personnel.
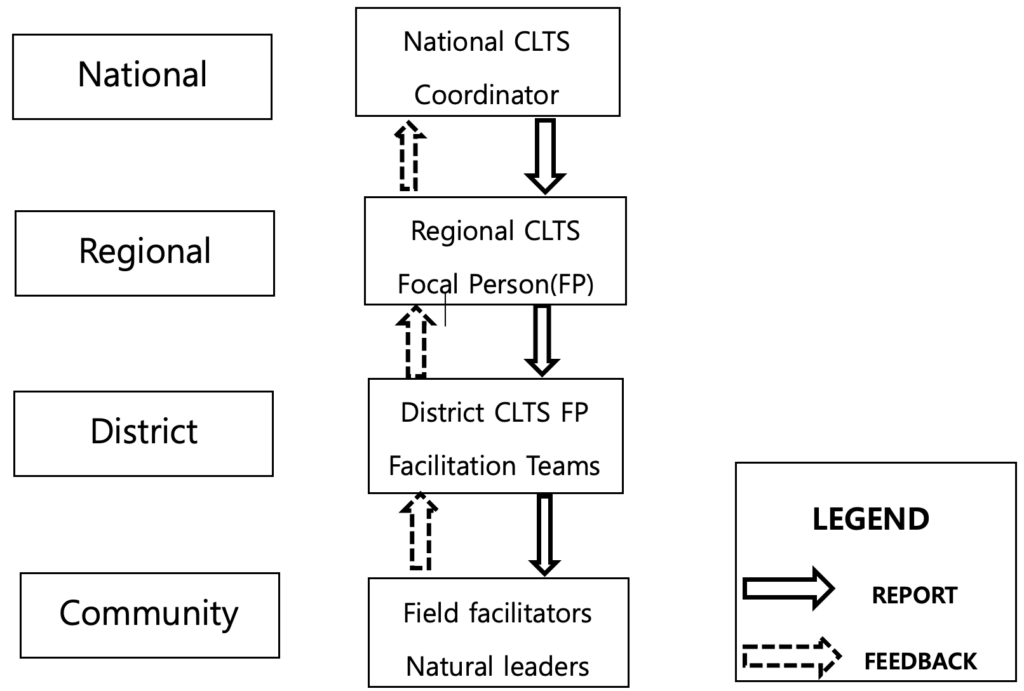
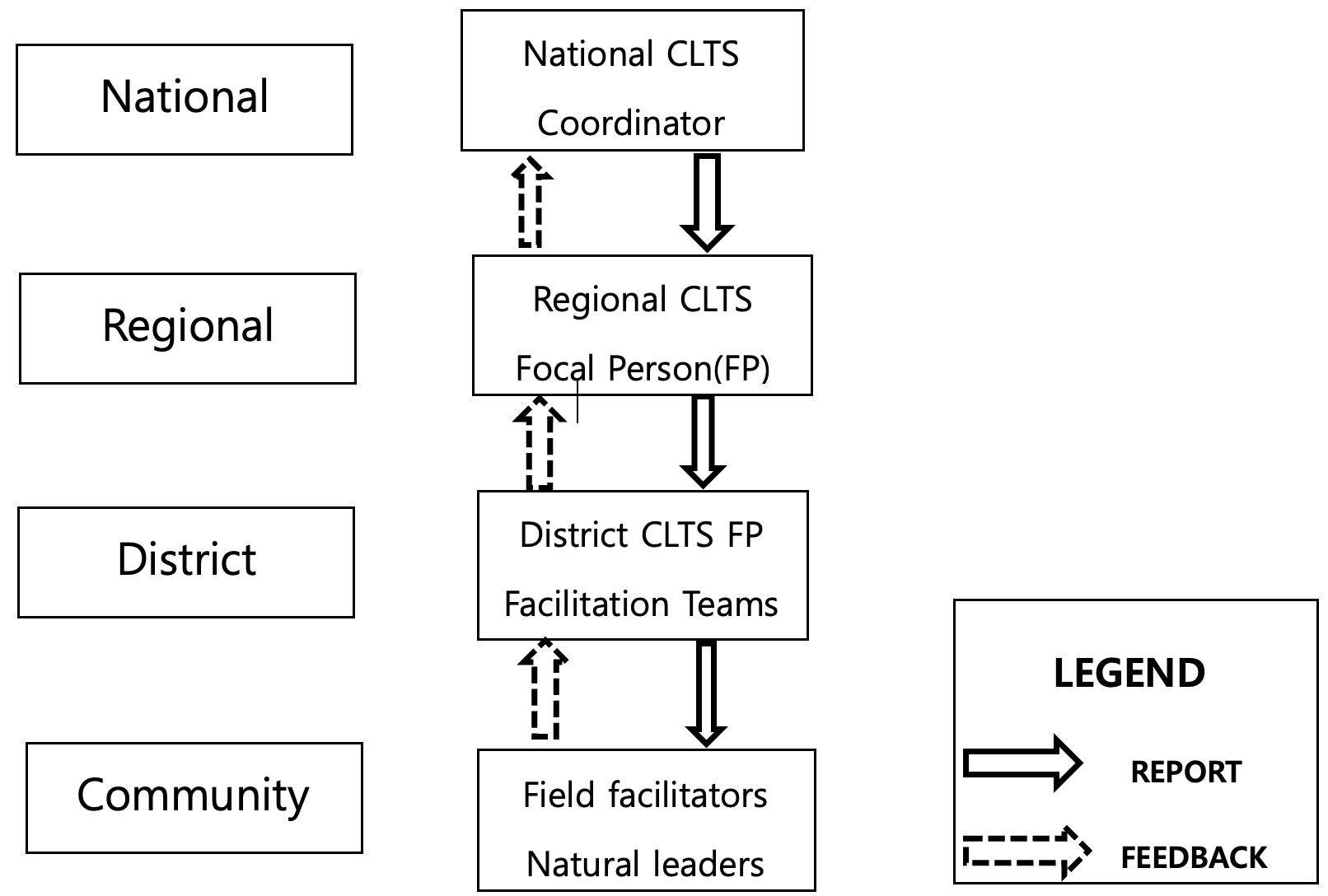
The baseline form used in the data collection process of the operations has two main parts: the community population and WASH related information and household demographic, population and WASH related information. Two copies of the form are usually made after filling it completely. One is kept at the sub district/ community level by the facilitator, another goes to the District Environmental health office (paper-based forms). The district submit to the region monthly or quarterly using the BaSIS which is then validated by Monitoring and evaluation officers (Figure 2). Variables collected both manually (paper-based) and electronically (BaSIS) during the process include the number of houses, number of households, population of the household and gender of the occupants. The number of households with toilets are also recorded to enable facilitators to know the extent of open defecation or sanitation coverage and the number of household toilets needed to achieve ODF. Other information include sources of water supply, health facilities, schools, etc. to identify other Water Sanitation and Hygiene (WASH) related needs or interventions of the communities. This is done by field facilitators who are mostly Environmental Health Officers. This data is taken as baseline information and updated during monitoring and finalized as end line after successful CLTS implementation. This information or data is collected only in triggered communities.
Data collection
Data on CLTS (from 2019 to 2023) were manually and electronically collected at the regional, district and community levels. Thirty stakeholders, which included nine key informants at the regional and district level and 21 other stakeholders at the community level, were selected. These stakeholders, which include community members, opinion leaders, field facilitators, CLTS focal persons, and Environmental Health Officers, were purposively selected at the regional, district and across six communities. Three of the purposively selected communities were triggered communities (Azangabisi, Yindongo and Feo-Kunkoa) and three ODF communities (Asaloko, Abelenzanga and Bongo-Tingre). Participants were selected due to their key role in the ODF communities and the operation of the surveillance system. Stakeholders engaged were above 18years, residents in the selected community and of sound mind and excluded mentally challenged individuals.
A semi-structured questionnaire adapted from CDC’s Updated Guidelines for Evaluating Public Health Surveillance Systems was used for face-to-face interviews for all stakeholder including observation of the system’s operations. Data on CLTS from all six area councils and Bongo town council were extracted from the Bongo District Environmental Health unit CLTS file, and BaSIS (Basic Sanitation Information System) using a paper-based checklist. Variables extracted included the number of ODF communities and the number of household latrines in the ODF communities. Data on baseline (sanitation situations before implementation of CLTS) and end-line (outcome of CLTS intervention) were also reviewed and abstracted.
Validity checks, data cleaning
The data analysed were obtained from an established routine system that incorporates several built-in data quality and validation procedures. These include the use of structured data collection tools and predefined reporting formats across all reporting sites. Data were subjected to verification at multiple levels, including community-level checks for completeness and consistency, district/regional review prior to submission, and national-level validation during data collation and analysis. Microsoft Excel 2013 was used to clean data for analysis, which involved correcting the year formatting, removal of duplicate records and data inconsistencies.
Data analysis
The evaluation was conducted by adapting the CDC’s updated guidelines for evaluating public health surveillance system, seven attributes: simplicity, flexibility, data quality, acceptability, representativeness, timeliness and stability, usefulness and the ability of the system to achieve its objectives were evaluated. Microsoft Excel 2013 was used to generate frequencies and proportions for quantitative data. Assessment indicators (Table 1) for quantitative attributes, like data quality, utilised the proportion of records with missing or incomplete fields, while the proportion of reporting councils was used in the assessment of representativeness. The qualitative data gathered were analysed by a direct content analysis approach. Qualitative feedback from key informants and routine reporting performance indicators, including discussion of the system functionality, reporting interruptions, and how surveillance outputs informed public health decision-making, were used in the assessment of qualitative attributes like simplicity, acceptability, stability and usefulness (Table 1). The results were presented in text, tables and graphs.
Assessment of system objectives
The objectives of the system are to construct and maintain a hygienic latrine, to stop open defecation and break the chain of feco-oral diseases. Indicators include the number of latrines, the number of ODF communities and knowledge on feco-oral transmission.
Records review of hardcopy documents kept at the Environmental Health and Sanitation department, and electronic database on Basic Sanitation Information System (BaSIS) was used in the assessment of the number of ODF recorded over the 5year period. System objectives such as latrine construction, usage and maintenance as well as open defecation free communities was reviewed from the Environmental Health unit CLTS file and the designated database, BaSIS. Records on triggering (community defecation map and action plan) were reviewed for awareness creation assessment by the system to break the chain of feco-oral transmission. Face-to-face interviews were also used to assess the awareness of community members on feco-oral transmission of diseases.
Assessment of system attributes
The Centers for Disease Control and Prevention guidelines for assessing a public health surveillance system were used in assessing the system’s attributes. The developed questionnaire was used to answer and describe seven attributes relevant to the CLTS surveillance system (Table 1).
Ethical considerations
Ethical approval with reference: GHS – ERC: 023/05/24 was obtained from the Ghana Health Service Ethics Review Committee. Permission was obtained from the Regional and District Environmental Health and Sanitation offices. Informed consent was obtained orally from individual respondents, and they were assured of confidentiality. Passwords were used to protect files of data and personal identifiers removed.
Socio-demographic of respondents
A total of 30 stakeholders, involving 10 community leaders, 10 community members, one community health volunteer (community level) and nine Environmental Health Officers (includes five field facilitators), were interviewed on the CLTS surveillance system in the Bongo District. The community members were made up of household heads or their representatives with a median age of 33 and interquartile range (IQR) (26 -41) years, with males constituting 19 (63.3%).
Assessment of system objectives
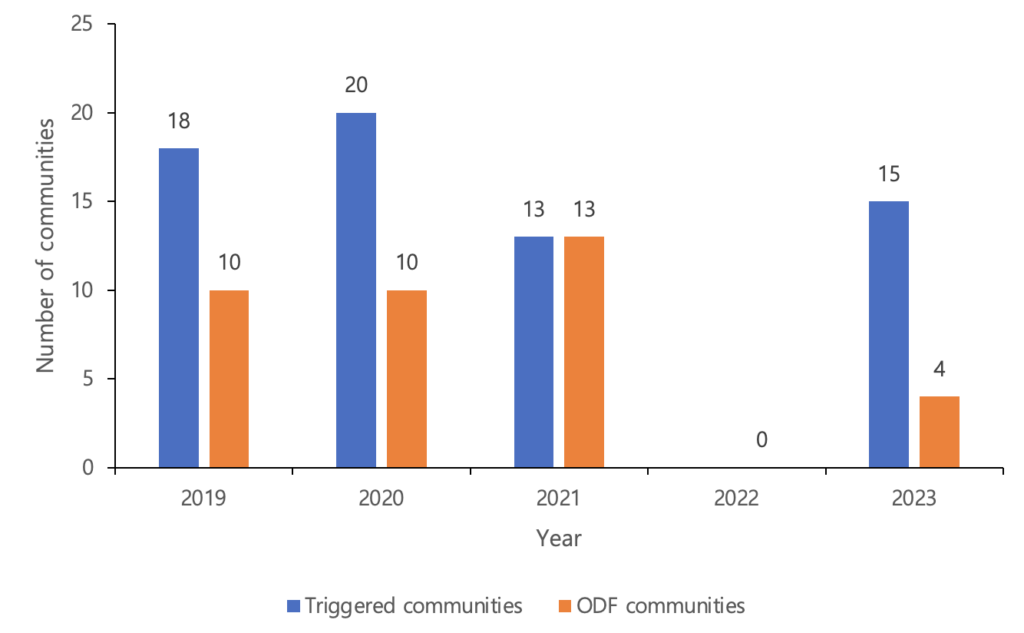
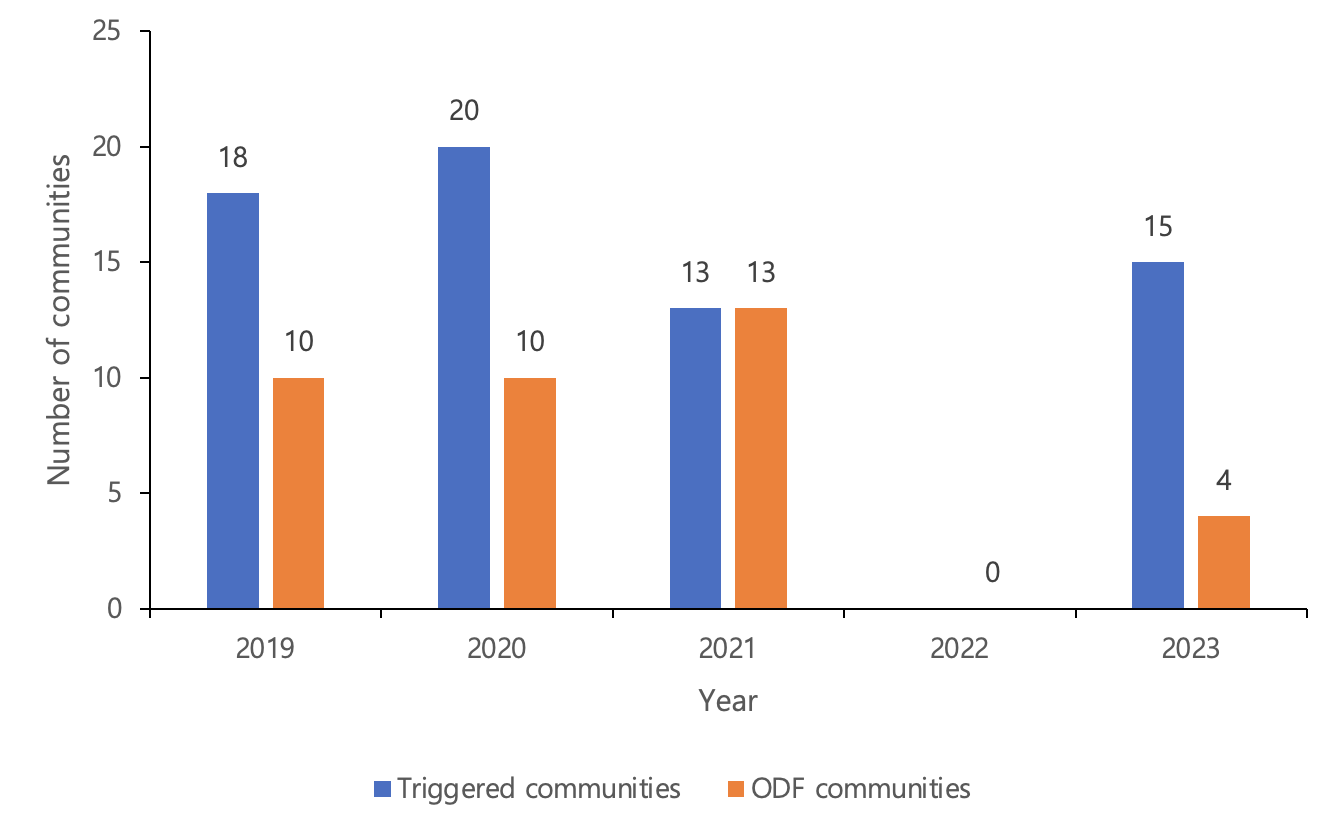
The objectives of the system are to construct and maintain hygienic latrine, to stop open defecation and break the chain of feco-oral diseases. Within the evaluation period, a total of 619 latrines were constructed in the district. About 66.7% (14/21) of stakeholders interviewed at the community level have latrines in their homes, and 52.4% (11/21) had hand washing facilities by their latrines. From 2019 to 2023, about 56.1% (37/66) of the triggered communities in Bongo District were declared ODF. In assessing the break in feco-oral transmission of diseases, about 85.7% (18/21) of respondents at the community level acknowledged that open defecation was a major source of diseases, hence admitted to the importance of CLTS in reducing feco-oral transmission of diseases in the communities. Communities triggered and declared ODF during the evaluation period (Figure 3).
Assessment of system attributes
Simplicity
All nine (100%) Environmental Health Officers stated that it is easy to identify an OD community using set criteria, and through the same observation, a community can be identified as ODF. All five field facilitators knew the processes of the CLTS surveillance system and stated that it takes an average of seven minutes to fill a paper-based form, while an average of five minutes is used to fill the BaSIS software. The data is collated at the sub-district/community level and disseminated to the district monthly. The district analyses and disseminates to the region and nationally on a quarterly basis. The electronic data collection tools have made it easier for dissemination to the next level once validated by a Monitoring and Evaluation Officer.
Flexibility
There have been changes in the data collection tools from paper-based to electronic-based over the past years. Two electronic data collection tools, ODK and BaSIS, were introduced in 2015 and 2021. Additional information added to the data collection tool includes household water supply and storage, and daily expenditure. These inclusions did not affect the system operations and its objectives, but rather made the system more efficient. The majority, 78% (7/9) of Environmental health officers who directly operate the system, indicated it is easier to operate the system now than before.
Acceptability
Field workers and District Interagency Coordinating Committee on Sanitation (DICCS) members expressed their preparedness and readiness towards the system operations. The six area council reporting units sent complete reports to the district with 100% reporting rates and 85% timeliness. All 21 people interviewed at the community level advocated for all the communities to be included in the CLTS operations.
Representativeness
The system is represented in all six area councils and the Bongo town council (Table 2). At the community level, triggered communities, every house is represented, and at the household level, everyone (male and female) is included.
Stability
All staff of the Environmental Health and Sanitation Unit (EHSU), who operate the system, are paid by the Government of Ghana. Funding for the system operations is largely dependent on Non-Governmental Organizations (NGOs). The system’s operation in 2022 was halted due to a lack of funding. Resulting in zero triggering and zero declaration of ODF. The system is not integrated into other operations of the EHSU. There is only one computer at the district office of EHSU. Some officers are not trained in the CLTS surveillance system.
Data quality
From 2019 to 2023, a total of 66 communities were triggered and 37 declared ODF, but data on the baseline for two communities that were declared ODF were missing, with no community name for one community. Percentage completeness for the ODF declaration form electronic data storage on communities was 89.2% (34/37). Monitoring progress data was difficult to extract and time-consuming due to the volume of papers. Inconsistency was observed in district and regional level data, coupled with variations in key variables such as the classification of ODF communities and observed ODF communities. Out-of-range values for the recorded date and duplicates were also observed.
Timeliness:
It takes an average of 3-6 months to trigger and declare a community as ODF. Though there are no stipulated timelines for reporting, sending reports to the next level was done daily, monthly and quarterly by officers in charge of data transmission. There was 100% reporting rate by officers from 2019 to 2023. Feedback to two officers in 2023 after data validation was delayed for about four days. However, it is ideal to expect the feedback within 24 hours.
Assessing the usefulness of the system
The surveillance data is used by DICCS and Regional Interagency Coordinating Committee on Sanitation (RICCS for verification of about 37 ODF communities. A mechanised borehole was constructed in the Asaloko community by Water Aid Ghana in 2020 after their declaration in 2019 as ODF to aid in their water supply in ensuring sustainability of the status.
The evaluation of the CLTS surveillance system in Bongo District was done to determine if the system meets its objectives and assess the usefulness and attributes of the system. There has been an increase in construction and usage of latrines in Bongo due to CLTS intervention, with more than two-thirds of households having and using household latrines in triggered communities. Another study reported that CLTS intervention in a community was approximately two times more likely to increase the rate of latrine ownership [11]. It has also been reported that the CLTS approach impacts on sanitation quality by reducing the practice of open defecation [7]. This fulfils the primary goal of preventing open defecation and cutting off feco-oral transmission of diseases with evidence of handwashing facilities in the communities. This contradicts similar studies, which found a gross unavailability of hand washing facilities both before CLTS (95.8%) and after CLTS (93%) [12].
The system was found to have triggered OD communities to take action in providing household latrines. This led to a change in the status of many communities being declared ODF. Though the number of ODF communities had increased, it was observed that some communities could not meet the expected 80% household latrine target for declaration, and hence were not declared. This might be a result of inadequate funding to subsidize the construction of CLTS latrines. It can also be due to the rocky terrain of the district, making latrine construction difficult in some of the communities. This situation might result in an increase in open defecation, water pollution, and disease outbreaks such as cholera and typhoid, among others, which will hinder the progress of the CLTS program from achieving its objectives of stopping open defecation and breaking the chain of feco-oral transmission diseases.
CLTS data was used to determine the sanitation coverage of the district and the region. Developmental partners and other NGOs interested in water, sanitation and hygiene (WASH) activities also used the data for implementation of other WASH programs as a measure of sustainability, considering the little or no support from the assembly and/or the government. This implies that CLTS communities stand the chance of getting other WASH interventions after successful implementation if need be.
A reliable source of funding is required to ensure that the CLTS surveillance keeps running to be able to achieve the United Nations (UN) SDGs goal six, which declares the importance of achieving “clean water and sanitation for all” [13]. As observed from the evaluation of the system in Bongo District, the funding source for CLTS surveillance is mainly from non-governmental organisations (NGOs) like the United Nations Children’s Fund (UNICEF) and other donor partners. District environmental health offices are responsible for coordination, triggering, follow-up, and monitoring. However, NGOs are de facto CLTS implementers due to resource constraints, though local government plays a supporting role in most stages of the system. Due to financial, human and material resource constraints, there was a system breakdown in all 12 months of 2022, resulting in no triggering and declaration. It started again in the latter part of 2023 with the intervention of Water Aid Ghana and Global Communities. This situation made the majority of respondents express fears of a future breakdown when donor support ceases.
It can be deduced from the users that the system was simple, as the flow of information across all levels of the surveillance system, including the timeliness of submitting baseline forms, was not a challenge. Issues such as information required to detect OD communities are easy to obtain and ascertain through observation in the communities. This conforms with the evaluation of the measles surveillance system in Ga West Municipality, which realized the system was simple as key surveillance officers demonstrated understanding of the case definition and its application [14]. The electronic data collection tools have made it easier for dissemination to the next level once validated by a Monitoring and Evaluation Officer. This conforms with the evaluation of the cholera surveillance system in Kumasi Metropolis, which found that reporting and feedback are done through electronic media such as WhatsApp, e-mails, among others, which makes reporting easier [15].
There has been a modification to the data collection tools from paper-based to electronic forms. Other indicators have been added to make it more sensitive and effective in assessing community status. These inclusions did not interfere with the system’s operations and its objectives, but they made the system more efficient. Majority of environmental health officers directly operating the system indicated that modifications to the system have made it easier to operate the system now than before. This is consistent with another evaluation of the cholera surveillance system at Osu Klotey which was found to be flexible [16]. On the contrary, the malaria surveillance system evaluation at Adaklu in the Volta Region found that the introduction of a protocol on testing all suspected cases partially affected the flexibility of the system [17]. The flexibility of the system has increased efficiency, reduced cost and time for data collection.
Data on every household in a triggered community is represented on the CLTS surveillance system. CLTS is operational in all the sub-districts in Bongo District because all the sub-districts practice OD, and the surveillance system needs to cover the whole district to ensure sanitation for all. Though the system is operational in all the sub-districts, representativeness in proportions is not the same due to the acceptability rate at the sub-district level and the rocky terrain of some communities, which makes it difficult for latrine construction using locally available materials. However, there are alternatives like construction of latrines on raised platforms to avoid digging into rocky ground, use of prefabricated containers that can be placed on the surface, eliminating the need for excavation and among others.
The data quality of the surveillance system is quite high due to the completeness of forms and evidence of data validation by the use of data collection tools (BaSIS) and excel spread sheet template. These data validation tools have unique identification for each community and this helps to identify ODF communities from OD communities. Good data quality helps in analysing CLTS data for decision-making. An evaluation of the measles surveillance system done in Ga West Municipality indicates high form completeness and estimated data quality found to be about 86% [14], contrary to a 60% completeness for the cholera surveillance system in Kumasi Metropolis [15].
The high acceptability of the system could be attributed to stakeholder engagement during the triggering process. This attracts attention and action of diverse stakeholder groups towards reduced risk of diseases, improved hygiene, dignity, pride and convenience among others. The willingness of all community members to undertake the CLTS is indicative of their full understanding of the importance of latrine construction and ODF for public health and wellbeing.
There is no set timeliness for submitting reports; however, the introduction of the electronic data collection tool (BaSIS) enables the submission of community baseline data to be done daily. This may be due to the fact that BaSIS has made data transmission easier and can be done in the field or from any location. This is consistent with an evaluation of measles surveillance system at Ga West Municipality that found the mode of reporting through the use of telephone, e-mail and other means of communication further simplifying the system [14].
Limitation
The limitations acknowledged include the relatively small sample size (30 stakeholders), which may limit the breadth of perspectives captured, although participants were purposively selected to represent key stakeholder groups involved in the community-led sanitation intervention. Additionally, the evaluation was conducted in a single district, which may limit the generalizability of the findings to other settings with different socio-cultural, environmental, or institutional contexts.
We also note the potential for response and social desirability bias, as data were collected through stakeholder interviews and discussions where participants may have emphasized positive experiences or outcomes. Nevertheless, observations and records review were also employed to validate responses received.
The surveillance system was found to partially meet its set objectives of building and maintaining hygienic latrines that help improve sanitation. The system was found to be acceptable, flexible, simple, with good data quality and representative. Timeliness was good; however, there were challenges with system stability. The system was found to be useful in promoting WASH activities in the district.
A total of ten Environmental Health Officers were trained (two days) on the protocol for CLTS verification and certification during the evaluation period as a public health action. The Bongo District Assembly Management should provide budgetary support to the Environmental Health and Sanitation Unit for computers, motor bikes and fuel for effective implementation of CLTS surveillance system as well as organize further training for officers to build capacity for the system’s stability and attainment of more ODF.
What is already known about the topic
What this study adds
The authors would like to acknowledge the Management of the Upper East Regional Environmental Health Office, Environmental Health office, Officers of the Bongo District and the Ghana Field Epidemiology and Laboratory training Programme (GFELTP). We also want to thank Mr. Charles Yinbil Awuni, Mr. Juventius Awinsone Asayuure and Mr. Mumuni Abdulai for their support throughout the field work.
DP and RAK conceptualized the analysis and designed the protocol. DP did the data collection, cleaning, analysis, and interpretation. DP, RAK, SD and SS contributed to data analysis and interpretation. DP, RAK, GA, CNL, JAF, SS and EK contributed to the original draft and revising of the manuscript. All the authors read and approved of this final manuscript.
| Attributes | Indicators | How it was assessed | Data collection tools |
|---|---|---|---|
| Simplicity | Structure and ease of operation | • Assessed the processes involved in the surveillance • Ease of case definition to identify OD communities • Steps of how data/reports are submitted, collated, analyzed and distributed | Records review Interview Observation |
| Flexibility | Variability of adapting to changing needs and conditions | • Modifications and new introduction to systems operation and how system adapted within 2019 to 2023 | Interview Records review |
| Acceptability | Willingness of stakeholders to participate in the process | • Reporting rates of sub districts to the district and to the region • Data completeness | Interview Records review Observation |
| Representativeness | Variability in the distribution of latrines and ODFs by councils (sub districts) | • Distribution of toilets in the communities within 2019–2023 • ODF declaration within 2019–2023 | Records review |
| Stability | Reliability of the system, and its ability to work when needed | • Resources available to collect, manage and provide data when needed • Source of funding of the operation | Interview |
| Data Quality | Completeness and validity of the data in the system | • Data completeness of baseline, triggering and end line forms • Proper documentation and reporting from 2019–2023 | Records review |
| Timeliness | Mean time between triggering and declaration of ODF | • Timelines between triggering and ODF declaration • Reporting timelines for 2019–2023 | Records review Interview |
| Sub District | Number of Communities | Communities Triggered | Number of ODF Communities | Proportions (%) |
|---|---|---|---|---|
| Bongo Central | 34 | 14 | 7 | 50.0 |
| Balungu | 20 | 9 | 5 | 55.6 |
| Namoo | 33 | 13 | 9 | 69.2 |
| Soe | 17 | 7 | 5 | 71.4 |
| Beo | 22 | 8 | 4 | 50.0 |
| Zorko | 23 | 9 | 5 | 55.6 |
| Valley Zone | 19 | 6 | 2 | 33.3 |
| Total | 168 | 66 | 37 |