Research | Open Access | Volume 9 (Suppl 12): Article 2 | Published: 20 Apr 2026
Views: 956
Menu, Tables and Figures
| Table 1: Selected IPC infrastructure and staffing subcomponents before and after intervention | ||
|---|---|---|
| Variable | Before intervention | After intervention |
| Built environment and infrastructure | ||
| Isolation ward fenced and cordoned off crowded areas of the hospital | Yes | Yes |
| Well ventilated | Yes | Yes |
| Regular supply of electricity and functional back-up power sources? | Yes | Yes |
| Water services available at all times and of sufficient quantity for all uses | Yes | Yes |
| Patient care (high-risk) area clearly separated from the general/administrative (low-risk) area | No | Yes |
| Separate entrances and exits for staff and patients | No | Yes |
| Dedicated space for staff to don PPE before entry into high-risk area | No | Yes |
| Dedicated area for doffing PPE with hand hygiene facility in place at the high-risk area | No | Yes |
| Any identified unidirectional workflow to prevent cross-contamination | No | Yes |
| Distance between two beds in the cohort bays more than 1 meter | Yes | Yes |
| Separate rooms for males and females | Yes | Yes |
| Staffing | ||
| Trained staff in the isolation ward | No | Yes |
| Dedicated staff assigned to preparing chlorine solution for disinfection | No | Yes |
| Dedicated cleaning staff | No | Yes |
| Dedicated IPC focal person in the ward | No | Yes |
| Daily IPC training for staff in the isolation ward | No | Yes |
| Staff trained to perform hand hygiene appropriately | No | Yes |
| Staff trained on the appropriate use of PPE | No | Yes |
| Staff trained on cleaning and disinfection of the isolation ward | Partially | Yes |
| Staff trained on healthcare waste management | Partially | Yes |
| Staff trained on safe sample packaging and transport | No | Yes |
Table 1: Selected IPC infrastructure and staffing subcomponents before and after intervention
| Table 2: Selected IPC equipment, practices and guidelines before and after intervention | ||
|---|---|---|
| Variable | Before intervention | After intervention |
| IPC equipment and materials | ||
| Functional hand hygiene stations at all points of care | No | Yes |
| Functional hand hygiene stations in general (low-risk) area | No | Yes |
| Patient-care equipment available and individualized | No | Yes |
| PPE available in different sizes and in sufficient quantity for clinical and support staff | Yes | Yes |
| Alcohol based hand rub available and adequate | Yes | Yes |
| Chlorine (powder/bleach) available and in sufficient quantity | Yes | Yes |
| Functional waste collection bins for segregation of waste at all waste generation points | No | Yes |
| Sharp boxes available at all points of care and not more than ¾ full | Yes | Yes |
| Incinerator available | Yes | Yes |
| IPC practices | ||
| Chlorine solution freshly prepared daily with the recommended formula | No | Yes |
| All surfaces in the patient care area are cleaned and disinfected twice daily | No | Yes |
| Staff wear full PPE to enter the patient care area | No | Yes |
| Waste segregated, transported and disposed of appropriately | No | Yes |
| IPC guidelines and SOPs | ||
| Clinical guidelines for the management of Lassa fever patients are available | No | No |
| SOP for Hand hygiene is available | No | No |
| SOP for cleaning and disinfection is available | No | No |
| SOP for Health care worker protection and safety is available | No | No |
| SOP for Waste management is available | No | No |
| SOP for donning and doffing PPE | No | No |
Table 2: Selected IPC equipment, practices and guidelines before and after intervention
| Table 3: IPC performance scores before and after IPC intervention | |||
|---|---|---|---|
| IPC Components | Before Intervention Score (%) | After Intervention Score (%) | Change (%) |
| Built Environment and Infrastructure | 53.2 | 86.8 | 33.6 |
| IPC Equipment and Materials | 44.7 | 89.5 | 44.8 |
| Staffing and Training | 35.0 | 91.7 | 56.7 |
| IPC guidelines/SOPs | 0.0 | 0.0 | 0.0 |
| Overall Score | 39.0 | 73.5 | 34.5 |
Table 3: IPC performance scores before and after IPC intervention

Ola Chikerendu Egbuta1&, Joseph Okoeguale2,3, Mojeed Olaitan Rafiu2,4,5, Christian Ehigbor Erohubie2,4,5, Pristar Omogbai2, Pokyes Hosea Daburum2, Jacqueline Agbukor2, Thomas Olokor2, Rita Omoafeba Esumeh2, Winifred Ambrose2, Emmanuel Illonah2, Reuben Agbons Eifediyi2,3
1Department of Community Medicine, Irrua Specialist Teaching Hospital, Irrua, Edo State, Nigeria, 2Institute of Viral and Emergent Pathogens, Control and Research, Irrua Specialist Teaching Hospital, Edo State, Nigeria, 3Department of Obstetrics and Gynaecology, Ambrose Alli University, Ekpoma, Edo State, Nigeria, 4Department of Internal Medicine, Irrua Specialist Teaching Hospital, Irrua, Edo State, Nigeria, 5Department of Medicine, Ambrose Alli University, Ekpoma, Edo State, Nigeria.
&Corresponding author: Ola Chikerendu Egbuta, Irrua Specialist Teaching Hospital, Irrua, Edo State, Nigeria; Email: olaegbutac@gmail.com ORCID: https://orcid.org/0000-0001-6520-3245
Received: 24 Nov 2025, Accepted: 16 Apr 2026, Published: 20 Apr 2026
Domain: Infectious Disease Epidemiology
Keywords: Lassa fever, Infection Prevention and Control, Outbreak, Healthcare Worker
©Ola Chikerendu Egbuta et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Ola Chikerendu Egbuta et al., Improving infection prevention and control during a Lassa fever outbreak: Experience from a military hospital in Nigeria. Journal of Interventional Epidemiology and Public Health. 2026; 9(Suppl 12):2. https://doi.org/10.37432/jieph-d-25-00301
Introduction: Lassa fever remains a serious public health threat in Nigeria, with annual outbreaks affecting healthcare workers due to inadequate Infection Prevention and Control (IPC) measures. As of March 2024, the country had reported 806 confirmed cases and 150 deaths, including 32 infections among healthcare workers. An outbreak at a Nigerian military hospital resulted in four deaths, three of whom were healthcare workers. In response, a multidisciplinary emergency team from the Irrua Specialist Teaching Hospital (ISTH) was deployed to assess existing IPC facilities and implement rapid IPC interventions.
Method: A targeted intervention was conducted from 27th February to 29th March 2024. IPC facilities and practices within the isolation ward were assessed using a checklist adapted from the World Health Organisation 2017 IPC Assessment Framework and the Nigeria Centre for Disease Control and Prevention Guidelines on infection prevention and control for viral haemorrhagic fevers. Structural modifications were undertaken to reduce transmission risks and facilitate effective barrier nursing. Comprehensive training sessions were provided to staff, focusing on Lassa fever transmission, hand hygiene, appropriate use of personal protective equipment, environmental disinfection, waste disposal and chlorine preparation.
Result: Initial assessment revealed that the isolation ward scored 39.0%, which improved to 73.5% post-intervention. Key improvements included the demarcation of high and low risk zones, the establishment of donning and doffing areas, and the installation of hand hygiene stations at strategic points. Three confirmed cases were admitted, treated with intravenous ribavirin and supportive care, and subsequently discharged without further deaths. No additional health worker infections occurred.
Conclusion: The IPC intervention implemented was associated with a reduction in the risk of hospital-based transmission of Lassa fever at the Military hospital. Sustained investment in IPC infrastructure and personnel training is essential in ensuring effective responses to future outbreaks.
Lassa fever is an acute viral haemorrhagic disease caused by the Lassa virus, an arenavirus endemic in West Africa[1,2] . Transmission occurs primarily through contact with food or household items contaminated by the excreta, urine or saliva of Mastomys natalensis rats. Secondary human-to-human transmission involving direct contact with blood or bodily fluids of infected persons may occur, especially within healthcare settings [2,3]. The disease poses a significant public-health burden, with an estimated 100000 – 300000 infections and approximately 5000 deaths occurring annually in the West African region [4,5]. Nigeria accounts for a substantial proportion of this burden, with year-round transmission and seasonal outbreaks occurring during the dry season, from November to March [6,7].
Healthcare facilities are often significantly affected during these outbreaks, as healthcare workers face heightened risks of infection, especially in facilities where infection prevention and control (IPC) measures are inadequate [8–10]. Factors such as limited access to personal protective equipment (PPE), poor adherence to standard precautions, and substandard infrastructure contribute to preventable disease transmission [8]. Effective IPC measures encompassing correct hand hygiene techniques, environmental cleaning and disinfection, the appropriate use of PPE, waste management, regular training, and proper patient screening, placement, and isolation are essential for interrupting transmission of viral haemorrhagic fevers and protecting healthcare workers [11]. Purpose-built isolation units for managing highly infectious diseases such as Lassa fever are a cornerstone of IPC. These units feature clearly defined high- and low-risk zones, secure access controls, separate entry and exit points for staff and patients, dedicated staff areas, well-ventilated rooms, reliable water supply, easy-to-clean surfaces, and capacity for expansion, all designed to minimise transmission risks to healthcare workers and the wider community [11]. However, many healthcare facilities in Nigeria lack such infrastructure and struggle to maintain effective IPC systems, particularly during outbreaks, due to resource constraints and limited institutional capacity [12–14].
As of March 2024, Nigeria had reported 806 confirmed cases of Lassa fever and 150 associated deaths, including 32 infections among healthcare workers [15]. Among the affected health institutions was a Nigerian military hospital that experienced an outbreak that resulted in four deaths, three of which occurred amongst healthcare workers. In response, a multidisciplinary emergency team from Irrua Specialist Teaching Hospital (ISTH), Edo State, was deployed to provide technical support. The team assessed existing IPC facilities, implemented rapid IPC interventions, and supported clinical case management within the isolation ward of the hospital. This article describes the IPC interventions implemented and the impact on IPC performance of the isolation ward of the affected military hospital.
The Irrua Specialist Teaching Hospital emergency team conducted a rapid IPC intervention in the isolation ward of a Nigerian military hospital between 27th February and 29th March 2024 during a Lassa fever outbreak.
Study setting
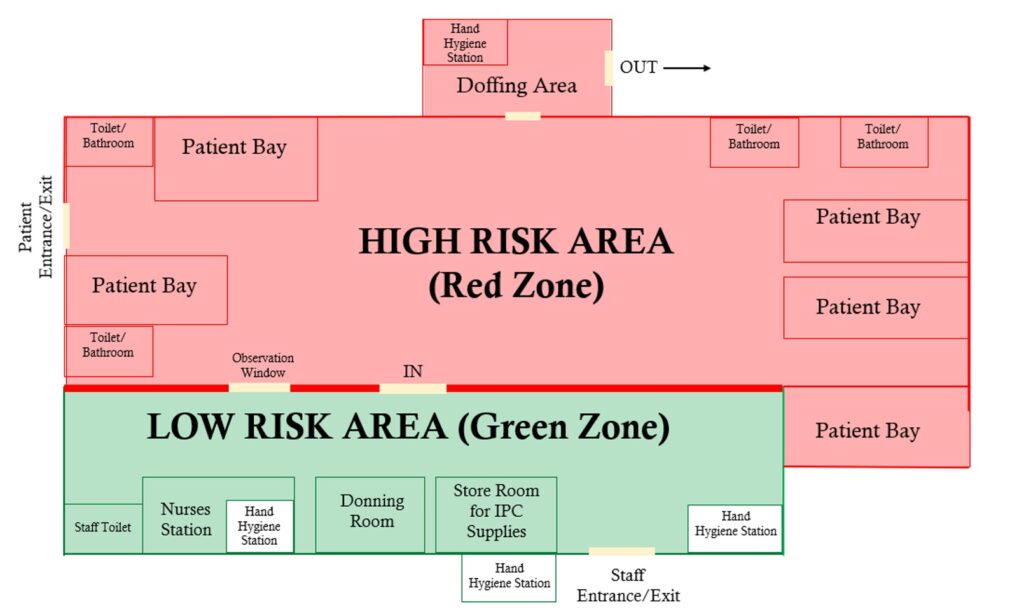
The hospital is a 600-bed tertiary healthcare facility providing clinical, laboratory and radiological services to military personnel and members of neighbouring communities. The isolation ward is a 25-bed facility comprising 5 separate bays designed for patient cohorting. It is fenced and situated away from the rest of the hospital to limit access and reduce the risk of disease transmission. Before intervention, the ward lacked clearly defined high-risk (patient care) and low-risk (nursing office/general) areas, and there were no designated areas for donning and doffing PPEs. These deficiencies increased the risk of cross-contamination between patients and staff.
IPC assessment and scoring
The baseline and post-intervention IPC assessments were conducted using an observational checklist adapted from the World Health Organisation IPC Assessment Framework (IPCAF) and the Nigeria Centre for Disease Control and Prevention (NCDC) Guidelines on Infection Prevention and Control for Viral Haemorrhagic Fevers [11,16]. Four key components were assessed, including the built environment and infrastructure, IPC equipment and materials, staffing and training and IPC guidelines/SOPs for the isolation ward. A total of 53 indicators were used to assess IPC performance. Each indicator was scored as 5 (meets requirement), 2.5 (partially meets requirement) and 0 (does not meet requirement). The component and overall scores were calculated as percentages using the formula:
\[
\frac{\text{Total Points Achieved}}{\text{Total Possible Points}} \times 100
\]
and categorised as inadequate (0 – 24%), basic (25 – 49%), intermediate (50 – 74%) and advanced (> 74%). The baseline assessment was conducted within the first two days of deployment, while the post-intervention assessment was conducted over one week before the end of the emergency response. To ensure scoring consistency, both assessments were conducted by the same assessment team.
The intervention
Key interventions were designed and implemented based on gaps identified during the baseline assessment, including:
Data on patient outcomes were extracted from clinical case notes.
Ethical consideration
This study was conducted as part of a formally designated emergency outbreak response activity by the Irrua Specialist Teaching Hospital, Edo State, under the authority of the Federal Ministry of Health. Since the intervention was a response to a public health emergency, no ethical approval was sought from an Institutional Review Board or Ethics Committee. Permission to use anonymised clinical data was obtained verbally from the management of the military hospital. Informed consent was obtained from all patients at discharge for the use of their clinical data for reporting purposes, and confidentiality was maintained for all patient data.
Baseline findings
Table 1 shows selected IPC infrastructure and staffing sub-components before and after IPC intervention. At baseline (before intervention), the isolation ward was fenced and well-ventilated with water services available at all times. However, major deficiencies across key areas were identified. The built environment lacked functional demarcation between the patient care area and general/administrative area; there were no dedicated donning and doffing areas, trained staff were not available in the isolation ward, and there was no dedicated IPC focal person (Table 1). Table 1 also showed that before intervention, staff were not appropriately trained on hand hygiene, the appropriate use of PPE and safe sample packaging and transport. Table 2 shows selected IPC equipment, practices and guidelines before and after intervention. At baseline, PPE, alcohol-based hand rub, and chlorine were available in sufficient quantities. However, there were no functional hand hygiene stations at points of care or in the general area, and staff did not wear full PPE to enter the patient care area. There were no available guidelines on the management of Lassa fever patients, hand hygiene, donning and doffing of PPE and cleaning and disinfection of the isolation ward.
Post-intervention findings
Following implementation of the interventions, the overall IPC performance score improved from 39.0% (basic) at baseline to 73.5% (Intermediate), with a 34.5% improvement in percentage score (Table 3). The built environment and infrastructure improved from 53.2% (intermediate) to 86.8% (advanced) after structural modifications, while staffing and training improved from 35.0% (basic) to 91.7% (advanced). However, the percentage score of the IPC guidelines/SOP component remained at 0.0% (inadequate) before and after intervention, as no written ward-specific IPC guidelines or SOPs were developed during the intervention period, despite the introduction and implementation of practical IPC measures. Specific improvements in IPC included:
Case management and outcomes
During the intervention period, three confirmed cases of Lassa fever aged 30 -55 years were admitted into the isolation ward. All received intravenous ribavirin and supportive therapy and were discharged alive. No new health worker infections were recorded during the post-intervention phase.
Challenges
The response was constrained by limited financial resources, the unavailability of written IPC guidelines, and staff shortages. Despite these challenges, multidisciplinary collaboration and continuous supervision sustained IPC compliance throughout the response.
This study demonstrates that rapid, well-coordinated infection prevention and control interventions can significantly improve the preparedness and response capacity of a military hospital isolation ward during a Lassa fever outbreak. The baseline assessment revealed substantial gaps across infrastructure, staffing, IPC equipment, and practices, consistent with findings from other Nigerian healthcare facilities, where there is weak IPC governance, poor IPC practices, and inadequate isolation facility design [10,17–19]. These gaps pose a major public health risk by increasing the occupational exposure of healthcare workers to Lassa fever and amplifying outbreaks within communities.
The improvement in the overall IPC performance of the isolation ward from 39% to 73.5% shows that rapid improvements can be achieved in resource-constrained settings when interventions are well-coordinated and supported by strong technical leadership. This experience confirmed that targeted environmental modifications, such as establishing clearly defined high-risk and low-risk zones and dedicated donning and doffing areas, are essential for reducing cross-infection and improving staff safety in suboptimal isolation units. Furthermore, improvements in hand hygiene and barrier nursing practices were associated with a reduced risk of exposure, as demonstrated by the absence of new healthcare worker infections during active case management.
A key lesson from this intervention is the critical role of continuous hands-on training. The increase in staffing and training domain from 35% to 91.7% illustrates how regular IPC drills, mentorship and close supervision are associated with improved staff competence, confidence and adherence to IPC standards. This finding is consistent with previous studies, which demonstrate that frequent practical training significantly improved adherence to hand hygiene, PPE use, and waste management [20–22].
Despite these gains, the absence of written IPC guidelines/SOPs in the isolation ward before and after the intervention was a significant gap which poses a risk to long-term sustainability. Written IPC guidelines are recognised as a core component of effective IPC programmes, ensuring standardised patient care, establishing clear procedures for IPC practices, and serving as essential tools for staff training and monitoring [23]. Without formal written guidelines or SOPs in the ward, improvements achieved during the emergency response may diminish once external support ceases or staffing changes occur. Adapting existing NCDC Lassa fever case management and IPC guidelines into ward-level SOPs would present a practical and cost-effective approach to addressing this gap.
Sustaining these IPC gains will further require strengthened governance structures and reliable resource allocation. Establishing a functional IPC team and appointing ward focal persons to oversee the implementation and periodic review of SOPs, as well as monitoring and evaluation of IPC practices, will enhance accountability [24,25]. Continuous training, particularly short hands-on refresher training during routine clinical activities and regular supportive supervision, will strengthen IPC compliance. Given the challenge of limited funding, incorporating IPC supplies and maintenance of IPC infrastructure into the recurrent budget of the hospital may be necessary to ensure uninterrupted availability of essential IPC materials and their maintenance.
The deployment of the Irrua Specialist Teaching Hospital outbreak response team under the authority of the Nigerian Federal Ministry of Health provided essential technical expertise, onsite training, supervision, and mobile diagnostic support. This collaboration strengthened the effectiveness and coordination of the response and improved the preparedness of the military healthcare facility for future outbreaks.
Study limitations
This study was conducted as part of an emergency outbreak response in a single military hospital, which limits the generalisability of the findings to other settings with different capacities or organisational structures. The assessment relied primarily on observation of the IPC system, which may introduce observer bias. This bias was minimised by the use of a standardised checklist adapted from the WHO and NCDC guidelines for infection prevention and control, and findings were cross-validated by an assessment team. Furthermore, because the study focused on rapid outbreak response, improvements were measured immediately after the intervention; therefore, the long-term sustainability of these gains could not be assessed.
The targeted IPC interventions, including infrastructural modification, regular staff training and strengthened routine IPC practices, were associated with rapid improvements in isolation ward performance, a reduction in occupational exposure and the absence of healthcare worker infections during a Lassa fever outbreak in a military hospital. However, sustaining these improvements beyond the outbreak period requires long-term institutional commitment. Continued investment in functional IPC infrastructure, development of ward-specific SOPs, establishment of functional IPC team and ward focal persons, regular personnel training, and uninterrupted supply of essential IPC materials are important in ensuring effective responses to future outbreaks. Strengthening collaboration between hospitals alongside dedicated government funding will further enhance national outbreak preparedness for Lassa fever and other highly infectious diseases.
What is already known about the topic
What this study adds
OCE, JO and RAE conceptualised the study. OCE, PO, PHD, JA, TO, ROE, WA and EI conducted the IPC assessment and interventions. JO, MOR and CEE supervised the IPC assessment and interventions. OCE prepared the first draft of the manuscript, and JO, MOR, CEE participated in manuscript writing and review to ensure intellectual content. All authors read and approved the final version of the manuscript.
| Table 1: Selected IPC infrastructure and staffing subcomponents before and after intervention | ||
|---|---|---|
| Variable | Before intervention | After intervention |
| Built environment and infrastructure | ||
| Isolation ward fenced and cordoned off crowded areas of the hospital | Yes | Yes |
| Well ventilated | Yes | Yes |
| Regular supply of electricity and functional back-up power sources? | Yes | Yes |
| Water services available at all times and of sufficient quantity for all uses | Yes | Yes |
| Patient care (high-risk) area clearly separated from the general/administrative (low-risk) area | No | Yes |
| Separate entrances and exits for staff and patients | No | Yes |
| Dedicated space for staff to don PPE before entry into high-risk area | No | Yes |
| Dedicated area for doffing PPE with hand hygiene facility in place at the high-risk area | No | Yes |
| Any identified unidirectional workflow to prevent cross-contamination | No | Yes |
| Distance between two beds in the cohort bays more than 1 meter | Yes | Yes |
| Separate rooms for males and females | Yes | Yes |
| Staffing | ||
| Trained staff in the isolation ward | No | Yes |
| Dedicated staff assigned to preparing chlorine solution for disinfection | No | Yes |
| Dedicated cleaning staff | No | Yes |
| Dedicated IPC focal person in the ward | No | Yes |
| Daily IPC training for staff in the isolation ward | No | Yes |
| Staff trained to perform hand hygiene appropriately | No | Yes |
| Staff trained on the appropriate use of PPE | No | Yes |
| Staff trained on cleaning and disinfection of the isolation ward | Partially | Yes |
| Staff trained on healthcare waste management | Partially | Yes |
| Staff trained on safe sample packaging and transport | No | Yes |
| Table 2: Selected IPC equipment, practices and guidelines before and after intervention | ||
|---|---|---|
| Variable | Before intervention | After intervention |
| IPC equipment and materials | ||
| Functional hand hygiene stations at all points of care | No | Yes |
| Functional hand hygiene stations in general (low-risk) area | No | Yes |
| Patient-care equipment available and individualized | No | Yes |
| PPE available in different sizes and in sufficient quantity for clinical and support staff | Yes | Yes |
| Alcohol based hand rub available and adequate | Yes | Yes |
| Chlorine (powder/bleach) available and in sufficient quantity | Yes | Yes |
| Functional waste collection bins for segregation of waste at all waste generation points | No | Yes |
| Sharp boxes available at all points of care and not more than ¾ full | Yes | Yes |
| Incinerator available | Yes | Yes |
| IPC practices | ||
| Chlorine solution freshly prepared daily with the recommended formula | No | Yes |
| All surfaces in the patient care area are cleaned and disinfected twice daily | No | Yes |
| Staff wear full PPE to enter the patient care area | No | Yes |
| Waste segregated, transported and disposed of appropriately | No | Yes |
| IPC guidelines and SOPs | ||
| Clinical guidelines for the management of Lassa fever patients are available | No | No |
| SOP for Hand hygiene is available | No | No |
| SOP for cleaning and disinfection is available | No | No |
| SOP for Health care worker protection and safety is available | No | No |
| SOP for Waste management is available | No | No |
| SOP for donning and doffing PPE | No | No |
| Table 3: IPC performance scores before and after IPC intervention | |||
|---|---|---|---|
| IPC Components | Before Intervention Score (%) | After Intervention Score (%) | Change (%) |
| Built Environment and Infrastructure | 53.2 | 86.8 | 33.6 |
| IPC Equipment and Materials | 44.7 | 89.5 | 44.8 |
| Staffing and Training | 35.0 | 91.7 | 56.7 |
| IPC guidelines/SOPs | 0.0 | 0.0 | 0.0 |
| Overall Score | 39.0 | 73.5 | 34.5 |