Research | Open Access | Volume 9 (2): Article 73 | Published: 05 May 2026

Views: 2,074
Menu, Tables and Figures
| Variable | n | % |
|---|---|---|
| Age (years) | ||
| 15–24 | 80 | 19.8 |
| 25–34 | 263 | 65.1 |
| 35–49 | 61 | 15.1 |
| Marital status | ||
| Married | 300 | 74.3 |
| Single | 50 | 12.4 |
| Widowed | 19 | 4.7 |
| Divorced | 12 | 3.0 |
| Separated | 21 | 5.2 |
| Cohabiting | 2 | 0.5 |
| Education | ||
| No Formal Education | 10 | 2.5 |
| Primary Education | 16 | 4.0 |
| Secondary Education | 59 | 14.6 |
| Tertiary Education | 319 | 79.0 |
| Religion | ||
| Islam | 212 | 52.5 |
| Christianity | 182 | 45.0 |
| Traditional/Other | 10 | 2.5 |
| Number of Children | ||
| 0 | 88 | 21.8 |
| 1–3 | 237 | 58.6 |
| ≥4 | 79 | 19.6 |
Table 1: Sociodemographic characteristics of respondents (N = 404)
| Predictor | Current users n (%) | Non-users n (%) | cOR (95% CI) | p-value | aOR (95% CI) | p-value |
|---|---|---|---|---|---|---|
| State | ||||||
| Kano (ref) | 105/205 (51.2) | 100/205 (48.8) | 1.00 | 1.00 | ||
| Bayelsa | 117/199 (58.8) | 82/199 (41.2) | 1.36 (0.91–2.03) | 0.126 | 0.33 (0.12–0.90) | 0.030 |
| Education | ||||||
| Lower (ref)* | 58/85 (68.2) | 27/85 (31.8) | 1.00 | 1.00 | ||
| Tertiary | 164/319 (51.4) | 155/319 (48.6) | 0.49 (0.30–0.80) | 0.003 | 0.49 (0.32–0.73) | 0.001 |
| Number of children (mean ± SD) | 2.1 ± 1.4 | 2.8 ± 1.6 | 0.80 (0.72–0.89) | <0.001 | 0.71 (0.60–0.84) | <0.001 |
| Cultural acceptability | ||||||
| Yes (ref) | 52/113 (46.0) | 61/113 (54.0) | 1.00 | 1.00 | ||
| No | 85/153 (55.6) | 68/153 (44.4) | 1.47 (0.91–2.36) | 0.91 (0.54–1.53) | 0.720 | |
| Not sure | 85/138 (61.6) | 53/138 (38.4) | 1.88 (1.15–3.07) | 0.047 | 1.09 (0.98–1.23) | 0.120 |
| Religion encourages FP | ||||||
| Yes (ref) | 108/195 (55.4) | 87/195 (44.6) | 1.00 | 1.00 | ||
| No | 20/44 (45.5) | 24/44 (54.5) | 0.67 (0.35–1.29) | 0.389 | 1.06 (0.84–1.33) | 0.640 |
| Not sure | 94/165 (57.0) | 71/165 (43.0) | 1.07 (0.72–1.59) | – |
Table 2: Logistic regression of sociocultural and demographic predictors of FP use (N = 399)
| Characteristic | High knowledge (≥5 methods) n (%) | Positive attitude n (%) | Current contraceptive use n (%) |
|---|---|---|---|
| Age | |||
| 15-24 | 42 (52.5) | 58 (72.5) | 48 (60.0) |
| 25-34 | 168 (63.9) | 210 (79.8) | 148 (56.3) |
| 35-49 | 32 (52.5) | 42 (68.9) | 26 (42.6) |
| p-value | 0.124 | 0.032* | 0.089 |
| Education | |||
| Tertiary | 210 (65.8) | 248 (77.7) | 164 (51.4) |
| Secondary or lower | 32 (37.6) | 62 (72.9) | 58 (68.2) |
| p-value | <0.001* | 0.342 | 0.003* |
| Religion | |||
| Islam | 138 (65.1) | 162 (76.4) | 112 (52.8) |
| Christianity | 98 (53.8) | 142 (78.0) | 104 (57.1) |
| p-value | 0.054 | 0.712 | 0.412 |
| Parity (children) | |||
| 0 | 48 (54.5) | 68 (77.3) | 56 (63.6) |
| 1-3 | 152 (64.1) | 184 (77.6) | 138 (58.2) |
| ≥4 | 42 (53.2) | 58 (73.4) | 29 (36.7) |
| p-value | 0.142 | 0.654 | <0.001* |
| *p<0.05. High knowledge = correctly naming ≥5 modern contraceptive methods spontaneously. Positive attitude = agrees FP is beneficial AND disagrees FP encourages promiscuity. | |||
Table 3: Cross-tabulation of FP knowledge, attitudes, and practices by sociodemographic characteristics (N=404)
| Indicator | Kano (n=205) n (%) | Bayelsa (n=199) n (%) | p-value |
|---|---|---|---|
| Discussed FP with partner | |||
| Yes | 153 (74.6) | 144 (72.4) | 0.605 |
| No | 52 (25.4) | 55 (27.6) | |
| Partner approves FP | |||
| Yes | 144 (70.2) | 132 (66.3) | 0.001 |
| No | 38 (18.5) | 20 (10.1) | |
| Not sure | 23 (11.2) | 47 (23.6) | |
| Can use FP without permission | |||
| Yes | 72 (35.1) | 60 (30.2) | 0.287 |
| No | 133 (64.9) | 139 (69.8) | |
| Partner accompanied to facility | |||
| Yes | 72 (35.1) | 38 (19.1) | <0.001 |
| No | 133 (64.9) | 161 (80.9) | |
| Variable | Kano | Bayelsa | ||||
|---|---|---|---|---|---|---|
| Current users n (%) | Non-users n (%) | P value | Current users n (%) | Non-users n (%) | P value | |
| Discussed FP with Partner | ||||||
| Yes | 92 (60.1) | 61 (39.9) | <0.001 | 103 (71.5) | 41 (28.5) | <0.001 |
| No | 13 (25.0) | 39 (75.0) | 14 (25.5) | 41 (74.5) | ||
| Partner approves FP | ||||||
| Yes | 86 (59.7) | 58 (40.3) | 0.276 | 98 (74.2) | 34 (25.8) | <0.001 |
| No | 19 (50.0) | 19 (50.0) | 4 (20.0) | 16 (80.0) | ||
Table 5: Association between male partner factors and contraceptive use, stratified by state (N = 404)
| State | Predictor | AOR | 95% CI | p-value |
|---|---|---|---|---|
| Kano | Partner accompanied to facility | 6.83 | 3.16–14.76 | <0.001 |
| Discussed FP with partner | 7.45 | 2.05–27.10 | 0.002 | |
| Partner approves FP | 0.98 | 0.43–2.22 | 0.957 | |
| Autonomy to use FP | 1.71 | 0.85–3.43 | 0.131 | |
| Bayelsa | Partner accompanied to facility | 1.46 | 0.63–3.41 | 0.382 |
| Discussed FP with partner | 0.94 | 0.32–2.78 | 0.909 | |
| Partner approves FP | 2.41 | 1.34–4.31 | 0.003 | |
| Autonomy to use FP | 0.72 | 0.37–1.39 | 0.327 |
Table 6: Logistic regression: Male partner predictors of contraceptive use, by state
Fareedah Lami Abdulkadir1, Polycarp Dauda Madaki1,2,&, Halima Abdulaziz Muhammad1, Shaima Ahmad Abdel-Sadiq1,3, Bashiru Abdullahi1, Ruth Sabo Manzo4, Akilu Abdullahi1,5, Sylvia Ezenwa-Ahanene6
1Department of Public Health, Faculty of Basic and Applied Biological Sciences, Ahmadu Bello University, Zaria, Nigeria, 2Department of Veterinary Tropical Diseases, University of Pretoria, Pretoria 0110, South Africa, 3Nigerian Airforce Hospital, Kano, Nigeria, 4African Centre for Disease Control and Prevention, Addis Ababa, Ethiopia, 5Obstetrics and Gynaecology Department, Muhammad Abdullahi Wase Teaching Hospital, Kano, Nigeria, 6Nigeria Centre for Disease Control and Prevention, Abuja, Nigeria
&Corresponding author: Polycarp Dauda Madaki, Department of Public Health, Faculty of Basic and Applied Biological Sciences, Ahmadu Bello University, Zaria, Nigeria, Email: polycarp.madaki@tuks.co.za, ORCID: https://orcid.org/0009-0001-8216-9779
Received: 24 Nov 2025, Accepted: 02 May 2026, Published: 05 May 2026
Domain: Sexual and Reproductive Health
Keywords: Family planning, contraceptive use, male involvement, sociocultural factors, Nigeria
©Fareedah Lami Abdulkadir et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Fareedah Lami Abdulkadir et al., Regional disparities in family planning knowledge, attitudes, practices, and barriers among reproductive-age women in Nigeria: A comparative study of Kano and Bayelsa States. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):73. https://doi.org/10.37432/jieph-d-25-00302
Introduction: Family planning (FP) is crucial for maternal and child health, yet Nigeria has one of the lowest modern contraceptive prevalence rates globally, with marked regional disparities. Factors influencing low contraceptive prevalence include socio-cultural norms, religious beliefs, and geopolitical variations across Nigeria’s six geopolitical zones. In Kano State (Northwest), conservative gender norms and religious interpretations discourage contraception, while Bayelsa State (South-South) has relatively more liberal attitudes toward modern FP. This study compared FP knowledge, attitudes, practices, and barriers among reproductive-age women in Kano State (Northwest, predominantly Muslim) and Bayelsa State (South-South, predominantly Christian), and examined the influence of male partners and socio-cultural factors on contraceptive use.
Methods: A comparative cross-sectional study was conducted among 404 women aged 15-49 years (205 from Kano, 199 from Bayelsa) using multistage sampling. Data were collected through interviewer-administered structured questionnaires and analyzed using SPSS version 25. Descriptive statistics, chi-square tests, and binary logistic regression were employed, with statistical significance set at p<0.05.
Results: FP awareness was nearly universal (98.5%), with no significant difference between states. However, knowledge scores were significantly higher in Kano (Mean=4.60, SD=2.79) than Bayelsa (Mean=3.68, SD=2.24; p<0.001). Current contraceptive use was 47.3% in Kano versus 52.7% in Bayelsa (p=0.126). Partner accompaniment to facilities (OR=3.03, 95% CI:1.75-5.25, p<0.001) and spousal discussion (OR=2.37, 95% CI:1.14-4.95, p=0.021) significantly predicted use. Paradoxically, Kano women reported higher cultural/religious acceptance but lower actual use. Main barriers were fear of side effects (29.1%) and desire for more children (24.2%)
Conclusion: Despite near-universal awareness, a clear knowledge practice gap persists, particularly in Kano, where higher knowledge does not translate into higher contraceptive use. Male partner involvement especially accompaniment to health facilities and spousal communication emerged as key drivers of uptake. Fear of side effects and the desire for more children remain the main barriers. These findings highlight the need for context-specific, culturally sensitive interventions that actively engage men and address misconceptions about contraceptive side effects.
Family planning (FP) is a cornerstone of reproductive health and has a crucial role in preventing maternal and child mortality, improving the health of women, and promoting sustainable development. The United Nations Population Fund (UNFPA) promotes all pregnancies being wanted, all births being safe, and all young people’s potential being fulfilled, while World Health Organization (WHO) identifies FP as central to achieving universal access to sexual and reproductive health services and the Sustainable Development Goals (SDGs) [1, 2]. By enabling couples and individuals to choose the number and timing of their offspring, FP benefits health, social, and economic benefits [3, 4]. Globally, FP prevents approximately 30% of maternal deaths and 10% of childhood deaths by enabling optimal birth spacing and reducing high‑risk pregnancies, consistent with evidence showing that scaling up contraceptive use can avert 32% of maternal deaths and nearly 10% of childhood deaths [1, 4, 5]. The 2030 Agenda for Sustainable Development explicitly includes universal access to sexual and reproductive health services under SDG target 3.7, recognizing FP as a cost‑effective public health intervention with proven demographic and socioeconomic dividends [1].
Despite such benefits, contraceptive use in Nigeria remains low, particularly among northern states such as Kano, compared to southern states such as Bayelsa. Nigeria, with a population exceeding 200 million, has one of the highest fertility rates in Africa and a modern contraceptive prevalence rate (mCPR) of about 15% among married women [6-8]. Substantial regional disparities exist across states, with markedly lower contraceptive use in northern states such as Kano compared with southern states such as Bayelsa [7, 8].These vary based on socio-cultural values, religious beliefs, and gender relations that greatly influence reproductive decisions. Large families are widely seen in the northern part of Nigeria as a representation of wealth, strength, and God’s blessing, particularly among Hausa and Fulani people [9]. Religious views also generate resistance, with Islamic clerics objecting to FP on the grounds that it interferes with God’s will, while the Roman Catholic Church maintains opposition to artificial contraception[9, 10]. Beyond religious affiliations, specific doctrinal interpretations and the influence of religious leaders substantially shape community norms around contraception. In northern Nigeria, some Islamic scholars equate FP with Western cultural imperialism and interference with divine will, while in the south, certain Christian denominations maintain ambivalent positions some Pentecostal churches encourage “fruitfulness” while others support child spacing for maternal health [10, 11]. This nuanced influence of religious leadership, rather than mere religious affiliation, warrants careful examination
Male involvement in reproductive decision-making is another critical determinant of contraceptive use. In patriarchal settings such as northern Nigeria, men dominate household decisions, including reproductive decisions, but can fail to receive FP education themselves, thereby limiting women’s access [12]. Evidence from south-western Nigeria shows that the women whose husbands/partners participated in reproductive health decisions were more likely to utilize modern contraceptives [13]. On the other hand, in the majority of southern states, relatively more egalitarian gender norms give women a greater degree of control over reproductive health decisions [13].
Religious and cultural beliefs also shape FP attitudes at the community level. Islamic leaders in Kano frequently discourage contraception, associating it with sin or Western intrusion, while in Bayelsa Christian attitudes are more diverse and sometimes more accepting of modern use of contraceptives.[7, 9, 14] These differences underscore the value of culturally sensitive and gender-responsive interventions to increase FP use.
While previous studies have examined individual factors influencing contraceptive use in Nigeria, few have adopted a comparative design that directly contrasts regions with markedly different socio-cultural, religious, and demographic contexts using identical methodology. To address this gap, the present study selected Kano and Bayelsa States based on three predefined criteria. First, the states represent extreme contrasts in contraceptive prevalence reported in the 2023-2024 Nigeria Demographic and Health Survey (NDHS), with substantially lower contraceptive use in the North-West compared with the South-South region [15]. Second, the states are significantly different in terms of their socio-cultural and religious backgrounds, as Kano is mainly filled with Hausa-Fulani ethnic groups where Islamic faith prevails, and Bayelsa mainly with Ijaw ethnic groups with Christian beliefs. Such different cultural and religious settings have been revealed to influence the reproductive norms, fertility preferences, and the acceptance of modern contraception [10, 16]. Third, the states are geographically distinct geopolitical areas (North-West vs. South-South) that would allow analyzing regional inequalities in reproductive health indicators in Nigeria. By selecting these contrasting contexts, this study aims to maximize analytical contrast and provide deeper insights into how socio-cultural, religious, and gender dynamics influence FP knowledge, attitudes, practices, and barriers among reproductive-age women in Nigeria.
In Kano State, family planning programs face implementation challenges including limited male engagement in reproductive health services, conservative religious interpretations discouraging modern contraceptive use, and gender norms that restrict women’s independent access to health facilities. Conversely, Bayelsa State benefits from relatively higher female literacy rates, more active community-based distribution of contraceptives through NGOs, and greater acceptance of modern FP methods among Christian-dominated communities, though misconceptions about side effects remain prevalent [17-19].
This study was guided by an adapted version of the Socio-Ecological Model (SEM) combined with the Theory of Planned Behavior (TPB). The SEM conceptualizes that individual behaviors (such as contraceptive use) are influenced by multiple interacting levels: (1) individual factors (knowledge, attitudes, age, parity, education, occupation), (2) interpersonal factors (male partner involvement including discussion, approval, accompaniment, and women’s autonomy), (3) community factors (cultural norms regarding family size, religious beliefs about contraception, community perceptions of contraception), and (4) health system factors (access to facilities, affordability of services) [20]. The TPB complements this framework by suggesting that behavioral intention (to use contraception) is shaped by attitudes toward the behavior (beliefs about whether FP is beneficial or encourages promiscuity), subjective norms (perceived social pressure from partner, family, and community), and perceived behavioral control (women’s autonomy to use contraceptives without partner’s permission)[21]. In this study, the primary outcome (current contraceptive use) is hypothesized to be directly influenced by male partner involvement at the interpersonal level, while knowledge (individual level) and cultural/religious beliefs (community level) operate through attitudes and perceived norms. The comparative design between Kano and Bayelsa States allows examination of how different socio-ecological contexts produce different patterns of family planning knowledge, attitudes, practices, and barriers.
Study design and setting
A community-based comparative cross-sectional study design was employed. This design was selected to enable simultaneous data collection from two geographically and culturally distinct populations, allowing for direct comparison of FP indicators using identical instruments and procedures.
The study was conducted in Kano State (Northwest Nigeria) and Bayelsa State (South-South Nigeria). Kano has a population of around 16.2 million, which is Muslim and Hausa-Fulani dominated, and has conservative gender norms and little utilization of contraceptives. Bayelsa has a population of around 2.3 million and is predominantly Christian and Ijaw with relatively higher levels of acceptance towards modern FP. These two states were purposively selected based on three predefined criteria: (1) extreme contrast in reported contraceptive prevalence from the most recent NDHS, (2) distinct socio-cultural and religious compositions (Islamic/Hausa-Fulani vs. Christian/Ijaw), and (3) geopolitical representation (Northwest vs. South-South). This purposive selection is to maximize the contrast in exposure variables and enable meaningful comparative analysis of how socio-cultural contexts shape FP outcomes [15].
Study population
The study population comprised women of reproductive age (15-49 years) who had resided in the selected communities for at least six months preceding data collection. Eligibility criteria included: (1) women aged 15-49 years, (2) married, cohabiting, or in a recognized partnership (including widowed, divorced, or separated women who could report on partner influence from their most recent relationship), (3) permanent resident in the study community, and (4) willingness to provide informed consent.
Exclusion criteria were: (1) women with cognitive or physical impairments that prevented them from providing informed responses, (2) critically ill individuals unable to complete the interview, and (3) those who declined participation after receiving study information
Sample size determination
The sample size needed was calculated using Cochran’s formula:
\[ n = \frac{Z^2 \cdot P \cdot (1 – P)}{d^2} \]
Where:
Z = 1.96 (95% confidence level)
P=0.368 [22]
d=0.05(error margin).
\[ n = \frac{(1.96)^2 \times 0.368 \times (1 – 0.368)}{(0.05)^2} \approx 357 \]
This gave a sample size of 357. To account for 10% non-response, at least 397 participants were required, approximately 400 individuals (200 each from the two states).
The estimated sample size was 400 participants (200 per state). However, the actual study achieved 404 respondents: 205 from Kano State and 199 from Bayelsa State. This slight discrepancy occurred because during household selection in one ward in Kano State, the sampling interval calculation yielded a slightly higher number of eligible households than anticipated, resulting in additional eligible women who consented to participate. In one ward in Bayelsa State, three selected households had no eligible women present after three visits and were replaced according to the sampling protocol with the next households in the sequence. No attrition occurred during data collection as all approached eligible women who provided informed consent completed the full interview. The sample size achieved (N=404) exceeds the minimum required sample of 397 (calculated to account for 10% non-response).
Sampling technique
A multistage sampling technique was employed, with identical procedures applied in both states to ensure methodological comparability.
Stage 1: Selection of Local Government Areas (LGAs): In each state, three Local Government Areas were purposively selected to capture variation in population density and settlement patterns. The selection ensured representation of both predominantly urban and rural communities within each state.
Stage 2: Selection of wards: From each selected LGA, three wards were selected using simple random sampling (balloting). This resulted in nine wards per state and a total of eighteen wards across the two states.
Stage 3: Selection of households: Within each selected ward, households were selected using systematic sampling. A central point in the community was identified as the starting location, after which every nth household was approached. The sampling interval (n) was determined by dividing the estimated number of households in the ward by the required number of households to be surveyed. Sampling intervals ranged from approximately 5 to 10 households depending on population density. The first household was selected by generating a random number between 1 and n, after which every nth household was approached. Households that were vacant or had no eligible respondent were skipped, and the next household in the sampling sequence was selected.
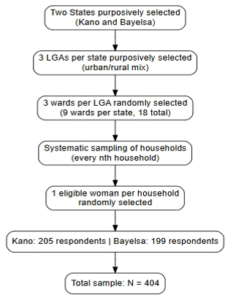
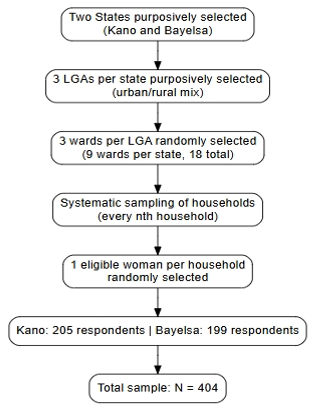
Stage 4: Selection of respondents: Within each selected household, one eligible woman of reproductive age was invited to participate in the study. In households where more than one eligible woman was present, one respondent was selected randomly. If no eligible woman was available in a selected household, the next household in the sampling sequence was approached. To ensure proportional representation, the number of households sampled in each ward was allocated using probability proportional to size based on estimated ward populations. This ensured that wards with larger populations contributed proportionally more respondents to the study sample. Figure 1 illustrates the multistage sampling procedure from population to final respondents
Operational definitions
For this study, the following operational definitions were adopted:
FP knowledge: Measured using an 8-item index where respondents were asked to name modern contraceptive methods spontaneously (unaided recall). Each correctly named method scored 1 point. Methods assessed included: pills, injectables, implants, intrauterine device (IUD), condoms, withdrawal method, lactational amenorrhea, and other methods. Total knowledge scores ranged from 0 to 8, with higher scores indicating greater knowledge.
FP attitude: Measured using Likert-scale questions assessing: (1) ‘Do you believe family planning is beneficial to couples?’ with responses ranging from strongly agree to strongly disagree; (2) ‘Do you think family planning encourages promiscuity?’ with responses from strongly agree to strongly disagree; and (3) ‘Do you think family planning goes against your religious belief?’ with responses from strongly agree to strongly disagree. Positive attitudes were defined as agreeing/strongly agreeing that FP is beneficial, disagreeing/strongly disagreeing that FP encourages promiscuity, and disagreeing/strongly disagreeing that FP goes against religious beliefs.
Contraceptive use: Defined as self-reported current use of any modern contraceptive method (pills, injectables, implants, IUD, condoms, or lactational amenorrhea) at the time of survey. Traditional methods (withdrawal method, rhythm method) were recorded but analyzed separately as non-modern methods.
Data collection instruments
Quantitative data were collected using a standardized interviewer-administered questionnaire, developed on Google Forms and pre-tested for reliability in similar communities. Cronbach’s alpha coefficients of ≥0.7 were achieved, signifying internal consistency. The questionnaire collected socio-demographics, knowledge, attitudes, influence of the male partner, cultural and religious beliefs, and FP practices and barriers. The pre-test was conducted among 20 women (10 per state) with similar characteristics in communities not included in the main study. Feedback from pre-testing led to minor rewording of ambiguous questions and confirmation of average interview duration (25-30 minutes)
Data collection procedure
Data was collected by trained enumerators who were given two-day training on interviewing, ethical practice, and data quality. Informed consent was obtained prior to data collection. Field supervision and real-time checks for consistency ensured data quality. Data quality was ensured through multiple measures: standardized two-day training of all enumerators covering interview techniques and ethical conduct, daily field supervision with spot-checks on 10% of completed questionnaires, real-time review of submissions for completeness and consistency, and double-data entry verification for a random sample of 10% of questionnaires
Data analysis
Quantitative data were entered into and processed using SPSS version 25. Frequencies and percentages were computed for all categorical variables, including socio-demographic characteristics, knowledge of FP methods, sources of information (analyzed using multiple response frequencies), attitudes, male partner influence, cultural beliefs, and barriers.
Bivariate analysis: Chi-square (χ²) tests were used to examine associations between categorical variables, particularly comparing Kano and Bayelsa States on key outcomes. Fisher’s exact test was applied where expected cell counts were <5. An independent samples t-test was conducted to compare mean knowledge scores between states.
Multivariate analysis: Binary logistic regression was performed to identify predictors of current contraceptive use. Variables were coded as follows: current contraceptive use (0=no, 1=yes); state (0=Kano, 1=Bayelsa); education (0=none/primary/secondary, 1=tertiary); number of children (continuous); partner accompaniment (0=no, 1=yes); spousal discussion (0=no, 1=yes); autonomy (0=no, 1=yes); partner approval (0=no, 1=yes/unsure); cultural acceptability (0=not acceptable, 1=acceptable/unsure); religious encouragement (0=no, 1=yes/unsure). Multicollinearity among independent variables was assessed using variance inflation factor (VIF), with all variables below the threshold of concern (VIF<10). Adjusted odds ratios (AOR) with 95% confidence intervals (CI) were reported. Statistical significance was set at p<0.05 (two-tailed). Comparisons were also made across regions in Kano and Bayelsa.
The chi-square test was chosen for bivariate comparisons because all primary outcome variables (current contraceptive use, partner approval, partner accompaniment) are categorical. Fisher’s exact test was applied where any expected cell count was less than 5. The independent samples t-test was used to compare mean knowledge scores between Kano and Bayelsa because knowledge score is a continuous variable and the two groups are independent. Levene’s test for equality of variances was used to assess whether variances were equal between the two states. Effect size was calculated using Cohen’s d. Binary logistic regression was selected for multivariate analysis because the primary outcome variable (current contraceptive use) is dichotomous (yes/no). Variables were entered into the logistic regression model using the enter method (simultaneous entry) because all variables were selected a priori based on a literature review. The variance inflation factor (VIF) was used to assess multicollinearity among independent variables. The Hosmer-Lemeshow goodness-of-fit test was used to assess model calibration. Nagelkerke R-squared values are reported to indicate the proportion of variance explained by the models
Ethical Considerations
Ethical approval was obtained from the Kano State Ministry of Health (NHREC/17/03/2018) and Bayelsa State Ministry of Health (BY/SMOH/HPRS/HP22/VOL.1/2025). Informed consent was obtained from all participants with guarantees of confidentiality and anonymity. Participation was voluntary, and respondents reserved the right to withdraw at any time. All methods were performed in accordance with relevant guidelines and regulations, including the Helsinki Declaration of 1975, as revised in 2013, on ethical principles for medical research involving human subjects.
Sociodemographic characteristics of respondents
A total of 404 participants were surveyed, with 205 (50.7%) from Kano and 199 (49.3%) from Bayelsa. The majority (65.1%) were aged 25-34 years, and 74.3% were married. Nearly four-fifths (79.0%) had a tertiary education. Islam was the predominant religion (52.5%), followed by Christianity (45.0%). More than half (58.6%) had 1-3 children, while 21.8% reported no children Regarding occupation, civil servants constituted the largest group (41.1%), followed by students (16.1%), traders (12.4%), private sector employees (7.9%), housewives (8.2%), self-employed individuals (7.7%), unemployed (3.7%), artisans (1.2%), and others (1.7%) (Table 1).
Knowledge of family planning (FP)
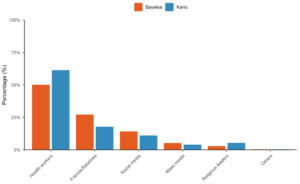
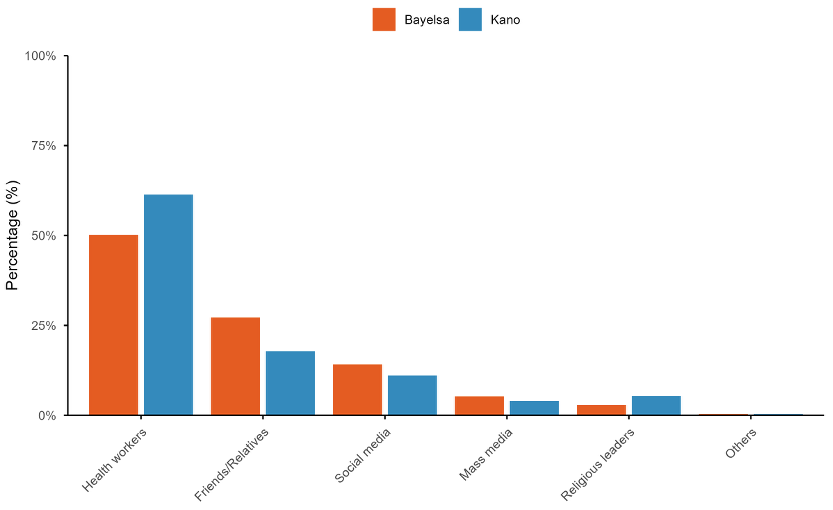
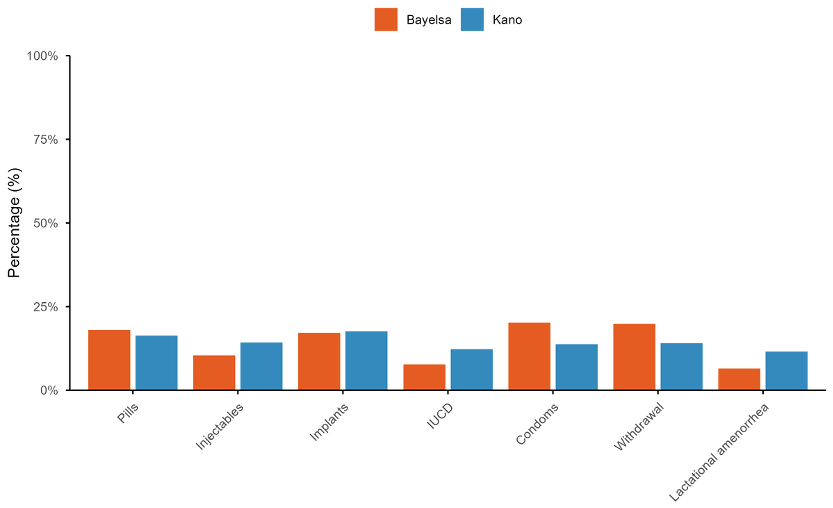
Almost all respondents (98.5%) had heard of FP, with no significant variation between states (χ²=0.001, p=0.971). Health workers were the most frequently cited source of information (82.6%), followed by relatives/friends (33.2%) and social media (18.9%). Figure 2 shows the sources of FP information disaggregated by state, revealing notable differences: Kano respondents relied more heavily on health workers (90.1% vs. 72.4% in Bayelsa), while Bayelsa respondents reported higher use of friends/relatives (39.3% vs. 26.1%) and social media (20.4% vs. 16.3%). Overall, 55.0% of respondents reported currently using a method of FP, while 45.0% were not currently using any method. Figure 3 presents knowledge of specific modern contraceptive methods by state. Implants were the most widely known method in Kano (80.2%), whereas condoms and withdrawal were more commonly known in Bayelsa (72.6% and 71.6%, respectively). Largest inter-state differences were observed for injectables (65.3% in Kano vs. 37.6% in Bayelsa) and lactational amenorrhea (53.0% vs. 23.4%).
Knowledge scores were significantly higher among Kano respondents (Mean=4.60, SD=2.79) than Bayelsa respondents (Mean=3.68, SD=2.24) ; independent samples t-test showed a mean difference of 0.924 (95% CI: 0.426-1.422), t (397) =3.65, p<0.001, Cohen’s d=0.365 . Among current users, implants were the most used method (26.0% of all respondents), followed by pills (10.6%), withdrawal method (10.1%), condoms (7.4%), injectables (3.0%), and IUCD (2.2%). Lactational amenorrhea and other methods were used by 0.2% and 5.4% respectively. Notably, 34.9% of all respondents reported using no method.
Attitudes toward family planning
Regarding attitudes toward family planning, the majority of respondents (90.8%) agreed or strongly agreed that family planning is beneficial to couples. Specifically, 163 respondents (40.3%) agreed and 204 (50.5%) strongly agreed that FP is beneficial, while 24 (5.9%) were neutral, 11 (2.7%) disagreed, and 2 (0.5%) strongly disagreed. Regarding the belief that family planning encourages promiscuity, 110 respondents (27.2%) agreed and 40 (9.9%) strongly agreed, representing 37.1% of all respondents. Additionally, 138 (34.2%) were neutral, 74 (18.3%) disagreed, and 42 (10.4%) strongly disagreed. Regarding religious beliefs about FP, 29 respondents (7.2%) agreed and 17 (4.2%) strongly agreed that family planning goes against their religious beliefs (11.4% combined), while 107 (26.5%) were neutral, 186 (46.0%) disagreed, and 65 (16.1%) strongly disagreed. Willingness to use contraceptives in the future showed that 298 respondents (73.8%) answered yes, 66 (16.3%) answered maybe, and 40 (9.9%) answered no.
Cultural and religious beliefs
Cultural acceptance of limiting family size was reported by 28.0% of women and was significantly associated with FP use (χ²=6.126, p=0.047). Among women who reported that limiting family size was culturally acceptable, 46.0% were current contraceptive users compared with 55.6% where it was considered not acceptable and 61.6% among those unsure (Table 2). In contrast, religious encouragement of contraceptives (p=0.389) was not significantly related to use. Multivariate logistic regression analysis (Table 2) showed that state of residence, education, and parity significantly predicted FP use. Women in Bayelsa had lower odds of contraceptive use compared with those in Kano (aOR=0.33, 95% CI: 0.12–0.90, p=0.030).
Sociodemographic correlates of knowledge, attitudes, and practices
To further characterize the study population, cross-tabulations of key FP outcomes with sociodemographic characteristics were examined (Table 3). Higher knowledge scores (≥5 methods known) were more common among women with tertiary education (72.4%) compared with those with secondary or lower education (27.6%, p<0.001). Positive attitudes toward FP (agreeing FP is beneficial while disagreeing it encourages promiscuity) were most prevalent among women aged 25-34 years (68.2%) and lowest among those aged 35-49 years (12.1%, p=0.032). Current contraceptive use varied significantly by parity: among women with no children, 63.6% were current users; among women with 1-3 children, 58.2%; and among women with ≥4 children, 36.7% (p<0.001). No significant associations were found between current use and religion (p=0.412) or occupation (p=0.218).
Male partner influence
Spousal discussion, partner’s approval, accompaniment to facilities, and autonomy were examined. While 73.5% reported discussing FP with their partners, only 68.3% stated that their partners approved. Partner disapproval was significantly more common in Kano than Bayelsa, whereas accompaniment to facilities was significantly higher in Kano (Table 4).
When analyzed by state, attitudes differed markedly. Among Kano respondents, 92.2% (189/205) agreed or strongly agreed that FP is beneficial compared with 89.4% (178/199) in Bayelsa (p=0.342). Regarding promiscuity beliefs, 41.0% (84/205) of Kano women believed FP encourages promiscuity (agree/strongly agree) compared with 33.2% (66/199) of Bayelsa women (p=0.089). Concerning religious beliefs, 13.2% (27/205) of Kano women agreed FP goes against their religious beliefs compared with 9.5% (19/199) of Bayelsa women (p=0.214). Bivariate analysis showed significant associations between several partner-related factors and current contraceptive use, with notable regional variations. Discussing FP with a partner was strongly associated with use in both states (p<0.001). Partner approval was associated with use in Bayelsa (p<0.001) but not in Kano (p=0.276, Table 5). Partner accompaniment to health facilities was associated with use in both states, though the effect was more pronounced in Kano (80.6% vs. 35.3%) than in Bayelsa (78.9% vs. 54.0%).
Binary logistic regression stratified by state revealed distinct regional patterns (Table 6). In Kano, partner accompaniment (AOR=6.83, p<0.001) and spousal discussion (AOR=7.45, p=0.002) strongly predicted contraceptive use. In Bayelsa, only partner approval was significant (AOR=2.41, p=0.003). Autonomy to use contraception without permission was not significant in either state.
Barriers to family planning (FP)
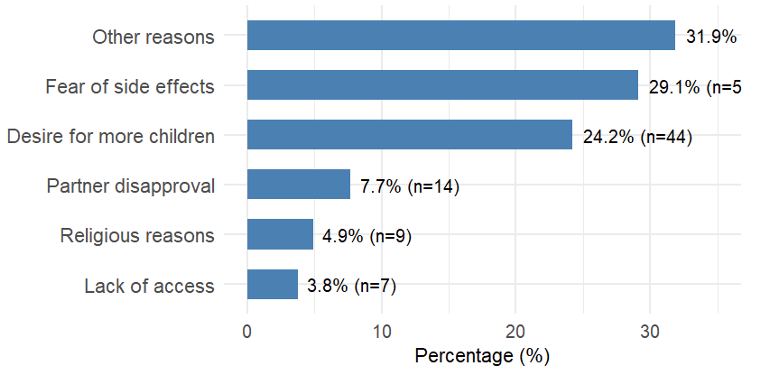
Most respondents (73.5%) lived within 30 minutes of a facility, and 87.1% reported that services were affordable. Access barriers were more common in Kano, though not statistically significant. Among the 182 non-users, the main reasons cited were fear of side effects (29.1%), desire for more children (24.2%), and husband’s/partners’s disapproval (7.7%, Figure 4). Side effects most reported were menstrual irregularities, weight gain, headache, and back pain.
Summary of regional differences
Comparisons between Kano and Bayelsa showed no significant differences in current FP use (47.3% vs. 52.7%, p=0.126) or willingness to use FP (p=0.224). However, cultural and religious views differed markedly: acceptance of limiting children was higher in Kano (68.1% vs. 31.9%, p<0.001), and religious encouragement of contraceptives was more common in Kano (62.1% vs. 37.9%, p<0.001).
From the logistic regression analysis examining sociodemographic and cultural predictors of contraceptive use (Table 2), women with tertiary education had lower odds of contraceptive use compared with those with lower education levels (AOR=0.49, 95% CI: 0.32-0.73, p=0.001). For each additional child a woman had, the odds of contraceptive use decreased (AOR=0.71, 95% CI: 0.60-0.84, p<0.001). Cultural acceptability of limiting family size was significantly associated with contraceptive use (χ²=6.126, df=2, p=0.047). Religious encouragement of modern contraceptives was not significantly associated with use (p=0.389). Women’s autonomy to use contraceptives without partner permission was not significantly associated with use (p=0.885).
The current study evaluated FP knowledge, attitudes, practice, and barriers among reproductive-age women in Kano and Bayelsa States, Nigeria. The findings revealed the presence of similarity and regional differences, where male partner support, socio-cultural beliefs, and perceived barriers impacted the use of contraceptives.
Knowledge and utilization of family planning (FP)
FP knowledge approached universality, according to national estimates of the 2023-24 Nigeria Demographic and Health Survey [15]. Implants, oral pills, and condoms were the most widely known strategies, in line with previous research that these remain the dominant forms of contraceptive awareness in Nigeria [24]. Women in Kano had significantly higher levels of knowledge scores than women in Bayelsa, possibly because they had a stronger reliance on health workers as a primary source of information. This concurs with evidence that health workers remain the most effective and most trusted source of FP communication in sub-Saharan Africa [24].
Despite this high awareness, contraceptive use remained low, particularly in Kano, this finding aligns with the 2023-24 Nigeria Demographic and Health Survey which reported modern contraceptive prevalence of 1.2% in Kano compared to 27.8% in Bayelsa among married women [15]. Our study found higher prevalence in both states (47.3% in Kano, 52.7% in Bayelsa), likely reflecting our sample’s higher educational attainment (79% tertiary) compared with general populations, suggesting that education may attenuate but not eliminate regional disparities in FP use[25].
Knowledge alone could not guarantee use, particularly where there were social and cultural constraints on women’s decision-making power. Similar knowledge-practice gaps have been documented in studies from northern Nigeria [22, 23] and other sub-Saharan African settings [24], underscoring that information alone is insufficient to drive behavior change in contexts with strong sociocultural constraints.
Attitudes toward family planning (FP)
Although most of the respondents perceived FP as good, more than one-third still saw it as encouraging promiscuity. Similar misconceptions have been observed elsewhere in Nigerian settings, where FP is often framed in terms of culture or morality [26]. It is such perceptions that result in stigma and opposition and emphasize the need for education programs that are culture-sensitive and dispel misinformation while highlighting FP’s health and economic benefits.
Male partner influence
Male partners were central to decision-making around contraceptives. Partners’ accompaniment to locations and couple discussions were strong predictors of FP uptake, affirming evidence that male participation strengthens where men are hegemonic [17]. Surprisingly, while disapproval was higher in Kano, men in this state were also more likely to escort their wives to locations, suggesting a paradox. This ‘accompaniment paradox’ may reflect a model of gatekeeper accompaniment where men maintain control by personally supervising their wives’ access to services rather than granting autonomous decision-making authority. Similar dynamics have been observed in conservative Muslim communities in Nigeria [18, 19, 27].
Cultural and religious beliefs
Cultural and religious environments played a significant role in FP attitudes. The women in Kano were likely to validate cultural and religious support for contraception, and skepticism was the situation in Bayelsa. With every additional child, the likelihood of FP use declined, reflecting deep-rooted pronatalist values [26]. This finding aligns with studies from other Nigerian settings where larger family size is associated with lower contraceptive use due to cultural preferences for many children [28, 29]. The association between higher parity and lower contraceptive use may also reflect that women who have achieved their desired family size may be older and potentially facing reduced fecundity.
Interestingly, women with a tertiary education had lower odds of modern method contraceptive use, a finding that could reflect postponement of childbearing plans without corresponding modern method adoption [25].
Although religion itself did not forecast contraceptive use, religious approval as observed was regionally diverse. This is in line with findings that context-dependent meanings of religious doctrine, rather than membership in a denomination, have stronger influence on reproductive practice [26]. Similar findings have been reported in Ethiopia, where Muslim women expressed religious approval of child spacing but faced husband opposition as the primary barrier [30]. This highlights that religious doctrine alone does not determine behavior; rather, its interpretation within local power structures matters more.
Barriers to family planning (FP)
Side effects and having more children were the predominant barriers, consistent with studies in other regions of Nigeria and other African countries [31]. A systematic review of 28 studies in sub-Saharan Africa found that fear of side effects was the most prevalent barrier to contraceptive use followed by menstrual irregularities and weight gain [30]. This consistency across settings suggests the need for improved counseling that addresses these concerns realistically while offering method-mixing options. Institutional challenges such as affordability and distance were less prevalent in general but varied geographically. Infrastructural issues were elevated in Kano women, while behavioral concerns, particularly side effects and childbearing desires, were elevated in Bayelsa women. These findings necessitate region-specific interventions-improving healthcare provision in Kano and improving counseling facilities in Bayelsa.
Regional differences
The gap between Bayelsa and Kano captures the complex interplay of culture, religion, and gender dynamics. While knowledge was the same, Bayelsa women reported higher contraceptive use with more ambivalence about cultural or religious support. In contrast, Kano women reported greater agreement with cultural and religious support but lower use, suggesting that male disapproval and restrictive norms can stifle practice. This only highlights the importance of addressing intra-household relationships and societal norms in FP programming [7]. This finding contrasts with nationally representative NDHS data, which reported substantially higher modern contraceptive prevalence in Bayelsa compared with Kano [15]. This likely reflects our sample’s higher educational attainment (79% tertiary) compared with general populations, suggesting that education may attenuate but not eliminate regional disparities in FP use. Similar patterns have been observed in comparative studies of Ethiopian regions, where educated women in conservative areas demonstrated knowledge levels comparable to women in liberal regions but faced persistent structural barriers to uptake [28].
Limitations
There are strengths to this study. The design adopted a comparative, cross-sectional approach between two opposite states with the same methodology that allowed analyzing the regional determinants of FP use. The dimensions of male partner influence, which were used in the sample size (N=404) were sufficient to perform multivariate analysis and the multiple dimensions of male partner influence (discussion, approval, autonomy, and accompaniment) used gave the opportunity to assess gender dynamics in making contraceptive decisions more comprehensively.
But a few limitations are to be considered. First, cross-sectional design prevents causal inference; while partner accompaniment is associated with contraceptive use, we cannot determine directionality. Second, the purposive selection of only two states limits generalizability to other Nigerian contexts. The sample was highly educated (79.0% tertiary), not representative of general populations where female literacy is approximately 40% in Kano and 70% in Bayelsa; findings may not apply to less-educated, rural, or marginalized women. Third, self-reported data may be subject to social desirability and recall bias, particularly in Kano where FP is more stigmatized. The questionnaire did not measure household wealth, media exposure, or health system factors (provider attitudes, commodity availability). Fourth, small subgroup sizes (divorced, n=12; widowed, n=19) prevented stratified analyses. When mapped to our research flow (Figure 1), specific limitations arose at different stages. At the sampling stage, purposive selection of only two states and over-representation of tertiary-educated women (79.0%) limit generalizability. At the study design stage, the cross-sectional design prevents causal inference. At the measurement stage, self-reported data may introduce social desirability bias, particularly in Kano. At the analysis stage, small subgroup sizes (divorced n=12, widowed n=19) prevented stratified analyses, and low Nagelkerke R-squared values (0.235, 0.130) indicate unmeasured confounders. Future longitudinal, qualitative, and representative surveys oversampling less-educated populations are recommended, along with health systems research in underserved northern states.
The comparison of knowledge, attitudes, and practices between reproductive-age women in Kano and Bayelsa States (not necessarily generalizable to all Nigerian states) revealed the following:
Knowledge: Significantly higher in Kano (mean=4.60, SD=2.79) than Bayelsa (mean=3.68, SD=2.24); independent samples t-test showed a mean difference of 0.924 (95% CI: 0.426-1.422, p<0.001).
Attitudes: Overall, 90.8% of respondents agreed FP is beneficial, but 37.1% believed FP encourages promiscuity. Only 11.4% believed FP goes against their religious beliefs. Willingness to use contraceptives was high (73.8% answered yes).
Practices: No statistically significant difference in current contraceptive use between Kano and Bayelsa (p=0.126).
Analysis of research findings: High levels of knowledge and favourable attitudes are not always accompanied by high contraceptive use, as demonstrated by Kano women who had significantly higher knowledge scores, but lower (though not significantly lower) contraceptive use compared with Bayelsa women. This knowledge-practice gap persists despite nearly universal awareness (98.5% had heard of FP). Male partner involvement emerged as the strongest predictor of contraceptive use: women whose partners accompanied them to health facilities had 3.03 times higher odds of using contraception (95% CI: 1.75-5.25, p<0.001), and women who discussed FP with their partners had 2.37 times higher odds (95% CI: 1.14-4.95, p=0.021). Partner approval was also a significant predictor (AOR=1.58, 95% CI: 1.03-2.44, p=0.037). Women’s autonomy to use contraceptives without partner permission was not significantly associated with use (p=0.974), indicating that in this context, partner involvement matters more than women’s independent decision-making. The main barriers to contraceptive use among non-users were fear of side effects and desire for more children, rather than lack of access or cost. These findings confirm that increased knowledge and awareness do not guarantee increased contraceptive use; rather, contraceptive use is strongly influenced by partner involvement and addressing misconceptions about side effects.
Recommendations
Based on the findings, the following are recommended steps:
For the Federal Ministry of Health and National Primary Health Care Development Agency (NPHCDA): Strengthen FP education through culturally responsive mass media campaigns targeting both women and men to dispel the myth that FP encourages promiscuity.
For State Ministries of Health (Kano and Bayelsa) and international non-governmental organizations (e.g., UNFPA): Implement couple-based FP counseling interventions that directly engage male partners, given that partner accompaniment and spousal discussion were the strongest predictors of contraceptive use.
For health facility managers, FP coordinators, and service providers at primary and secondary health facilities: Train FP counselors to proactively address fear of side effects (the primary barrier for non-users) through realistic counseling on expected side effects, management strategies for common side effects, and method-switching options.
For Kano State Primary Health Care Development Agency and local government health authorities specifically: Address male disapproval of FP through community dialogue sessions with religious leaders, imams, and community gatekeepers, while simultaneously improving facility accessibility.
For Bayelsa State Ministry of Health and Bayelsa State Primary Health Care Board specifically: Focus on enhanced counseling services to address fear of side effects and misconceptions about promiscuity and strengthen community-based distribution of contraceptives.
Future research directions
Based on the findings and limitations of this study, the following areas are recommended for future research
What is already known about the topic
What this study adds
The authors acknowledge the support of the Department of Public Health, Faculty of Basic and Applied Biological Sciences, Ahmadu Bello University, Zaria, for providing academic guidance throughout this research. We also thank the community leaders, data collectors, and study participants in Kano and Bayelsa States for their cooperation.
FLA designed the study, coordinated data collection, and contributed to data analysis and manuscript drafting. PDM supervised the study, interpreted the findings, and led manuscript revision. HAM, SAAS, BA, RSM, SA and AA collectively contributed to data collection, literature review, data analysis support, and critical review of the manuscript. All authors approved the final version.
| Variable | n | % |
|---|---|---|
| Age (years) | ||
| 15–24 | 80 | 19.8 |
| 25–34 | 263 | 65.1 |
| 35–49 | 61 | 15.1 |
| Marital status | ||
| Married | 300 | 74.3 |
| Single | 50 | 12.4 |
| Widowed | 19 | 4.7 |
| Divorced | 12 | 3.0 |
| Separated | 21 | 5.2 |
| Cohabiting | 2 | 0.5 |
| Education | ||
| No Formal Education | 10 | 2.5 |
| Primary Education | 16 | 4.0 |
| Secondary Education | 59 | 14.6 |
| Tertiary Education | 319 | 79.0 |
| Religion | ||
| Islam | 212 | 52.5 |
| Christianity | 182 | 45.0 |
| Traditional/Other | 10 | 2.5 |
| Number of Children | ||
| 0 | 88 | 21.8 |
| 1–3 | 237 | 58.6 |
| ≥4 | 79 | 19.6 |
| Predictor | Current users n (%) | Non-users n (%) | cOR (95% CI) | p-value | aOR (95% CI) | p-value |
|---|---|---|---|---|---|---|
| State | ||||||
| Kano (ref) | 105/205 (51.2) | 100/205 (48.8) | 1.00 | 1.00 | ||
| Bayelsa | 117/199 (58.8) | 82/199 (41.2) | 1.36 (0.91–2.03) | 0.126 | 0.33 (0.12–0.90) | 0.030 |
| Education | ||||||
| Lower (ref)* | 58/85 (68.2) | 27/85 (31.8) | 1.00 | 1.00 | ||
| Tertiary | 164/319 (51.4) | 155/319 (48.6) | 0.49 (0.30–0.80) | 0.003 | 0.49 (0.32–0.73) | 0.001 |
| Number of children (mean ± SD) | 2.1 ± 1.4 | 2.8 ± 1.6 | 0.80 (0.72–0.89) | <0.001 | 0.71 (0.60–0.84) | <0.001 |
| Cultural acceptability | ||||||
| Yes (ref) | 52/113 (46.0) | 61/113 (54.0) | 1.00 | 1.00 | ||
| No | 85/153 (55.6) | 68/153 (44.4) | 1.47 (0.91–2.36) | 0.91 (0.54–1.53) | 0.720 | |
| Not sure | 85/138 (61.6) | 53/138 (38.4) | 1.88 (1.15–3.07) | 0.047 | 1.09 (0.98–1.23) | 0.120 |
| Religion encourages FP | ||||||
| Yes (ref) | 108/195 (55.4) | 87/195 (44.6) | 1.00 | 1.00 | ||
| No | 20/44 (45.5) | 24/44 (54.5) | 0.67 (0.35–1.29) | 0.389 | 1.06 (0.84–1.33) | 0.640 |
| Not sure | 94/165 (57.0) | 71/165 (43.0) | 1.07 (0.72–1.59) | – |
| Characteristic | High knowledge (≥5 methods) n (%) | Positive attitude n (%) | Current contraceptive use n (%) |
|---|---|---|---|
| Age | |||
| 15-24 | 42 (52.5) | 58 (72.5) | 48 (60.0) |
| 25-34 | 168 (63.9) | 210 (79.8) | 148 (56.3) |
| 35-49 | 32 (52.5) | 42 (68.9) | 26 (42.6) |
| p-value | 0.124 | 0.032* | 0.089 |
| Education | |||
| Tertiary | 210 (65.8) | 248 (77.7) | 164 (51.4) |
| Secondary or lower | 32 (37.6) | 62 (72.9) | 58 (68.2) |
| p-value | <0.001* | 0.342 | 0.003* |
| Religion | |||
| Islam | 138 (65.1) | 162 (76.4) | 112 (52.8) |
| Christianity | 98 (53.8) | 142 (78.0) | 104 (57.1) |
| p-value | 0.054 | 0.712 | 0.412 |
| Parity (children) | |||
| 0 | 48 (54.5) | 68 (77.3) | 56 (63.6) |
| 1-3 | 152 (64.1) | 184 (77.6) | 138 (58.2) |
| ≥4 | 42 (53.2) | 58 (73.4) | 29 (36.7) |
| p-value | 0.142 | 0.654 | <0.001* |
| *p<0.05. High knowledge = correctly naming ≥5 modern contraceptive methods spontaneously. Positive attitude = agrees FP is beneficial AND disagrees FP encourages promiscuity. | |||
| Indicator | Kano (n=205) n (%) | Bayelsa (n=199) n (%) | p-value |
|---|---|---|---|
| Discussed FP with partner | |||
| Yes | 153 (74.6) | 144 (72.4) | 0.605 |
| No | 52 (25.4) | 55 (27.6) | |
| Partner approves FP | |||
| Yes | 144 (70.2) | 132 (66.3) | 0.001 |
| No | 38 (18.5) | 20 (10.1) | |
| Not sure | 23 (11.2) | 47 (23.6) | |
| Can use FP without permission | |||
| Yes | 72 (35.1) | 60 (30.2) | 0.287 |
| No | 133 (64.9) | 139 (69.8) | |
| Partner accompanied to facility | |||
| Yes | 72 (35.1) | 38 (19.1) | <0.001 |
| No | 133 (64.9) | 161 (80.9) | |
| Variable | Kano | Bayelsa | ||||
|---|---|---|---|---|---|---|
| Current users n (%) | Non-users n (%) | P value | Current users n (%) | Non-users n (%) | P value | |
| Discussed FP with Partner | ||||||
| Yes | 92 (60.1) | 61 (39.9) | <0.001 | 103 (71.5) | 41 (28.5) | <0.001 |
| No | 13 (25.0) | 39 (75.0) | 14 (25.5) | 41 (74.5) | ||
| Partner approves FP | ||||||
| Yes | 86 (59.7) | 58 (40.3) | 0.276 | 98 (74.2) | 34 (25.8) | <0.001 |
| No | 19 (50.0) | 19 (50.0) | 4 (20.0) | 16 (80.0) | ||
| State | Predictor | AOR | 95% CI | p-value |
|---|---|---|---|---|
| Kano | Partner accompanied to facility | 6.83 | 3.16–14.76 | <0.001 |
| Discussed FP with partner | 7.45 | 2.05–27.10 | 0.002 | |
| Partner approves FP | 0.98 | 0.43–2.22 | 0.957 | |
| Autonomy to use FP | 1.71 | 0.85–3.43 | 0.131 | |
| Bayelsa | Partner accompanied to facility | 1.46 | 0.63–3.41 | 0.382 |
| Discussed FP with partner | 0.94 | 0.32–2.78 | 0.909 | |
| Partner approves FP | 2.41 | 1.34–4.31 | 0.003 | |
| Autonomy to use FP | 0.72 | 0.37–1.39 | 0.327 |