Research | Open Access | Volume 9 (1): Article 52 | Published: 26 Mar 2026
Views: 54
Menu, Tables and Figures
| Variable | Frequency (%) |
|---|---|
| Age (years) | |
| ≤ 35 | 31 (15) |
| > 35 | 175 (85) |
| Gender | |
| Male | 47 (23) |
| Female | 159 (77) |
| Work experience of CHWs (years) | |
| < 5 | 43 (21) |
| 5–10 | 36 (17) |
| > 10 | 127 (62) |
| Level of education completed | |
| Primary | 44 (21) |
| Secondary | 121 (59) |
| Tertiary | 41 (20) |
| Have you heard about mpox | |
| Yes | 202 (98) |
| No | 4 (2) |
| Have you received any specific training related to mpox | |
| Yes | 61 (30) |
| No | 141 (70) |
Table 1: Characteristics of community health workers assessed for knowledge, attitudes and practices regarding mpox, Mbarara City, Uganda, February 2025 (N=206)
| Items* | N (%) |
|---|---|
| 1. How is mpox transmitted? | 132 (65) |
| 2. Are there specific treatments for mpox? | 141 (70) |
| 3. Do you know how to detect mpox cases in your community? | 163 (81) |
| 4. Do you know the procedure for reporting a suspected mpox case? | 172 (85) |
| 5. Are you aware of the specific health facilities to which you should refer suspected mpox cases in your community? | 194 (96) |
| 6. Do you have access to the contact information of health facilities for mpox referrals in your community? | 175 (87) |
| *Responses to the items indicate only the “yes” category | |
Table 2: Community health workers’ knowledge regarding mpox in Mbarara City, Uganda, February 2025 (n=202)
| Items | N (%) |
|---|---|
| 1. How serious do you think the threat of mpox is for the community’s health and well-being? | 158 (78) |
| 2. How confident are you in your ability to identify and manage a suspected mpox case? | 176 (87) |
| 3. Do you think the community is well-prepared to prevent the spread of mpox? | 123 (61) |
| 4. How would you rate your personal belief in the effectiveness of mpox prevention measures (e.g., vaccination, hand washing)? | 180 (89) |
| 5. Do you feel supported by local health authorities in your role as a CHWs in preventing mpox? | 138 (68) |
Table 3: Community health workers’ attitudes toward mpox in Mbarara City, Uganda, February 2025 (n=202)
| Item | N (%) |
|---|---|
| Have you been involved in community education or awareness activities about mpox? | 143 (71) |
| Do you actively refer suspected mpox cases to higher health facilities? | 55 (27) |
| How regularly do you report suspected mpox cases to health authorities? | 51 (25) |
| Do you conduct home visits to educate households on mpox prevention? | 59 (29) |
Table 4: Community health workers’ responses to practices regarding mpox in Mbarara City, Uganda, February 2025 (n=202)
| Variable | Knowledge | COR (95% CI) | AOR (95% CI) | |
|---|---|---|---|---|
| Good (%) | Poor (%) | |||
| Age (years) | ||||
| ≤35 | 22 (17) | 8 (11) | Ref | |
| >35 | 107 (83) | 65 (89) | 1.7 (0.7–3.9) | 0.7 (0.2–1.9) |
| Gender | ||||
| Male | 28 (22) | 18 (25) | Ref | |
| Female | 101 (78) | 55 (75) | 1.9 (0.8–4.5) | 0.6 (0.3–1.6) |
| Work experience of CHWs (years) | ||||
| <5 | 53 (71) | 38 (72) | Ref | |
| 5–10 | 22 (29) | 15 (28) | 0.9 (0.4–2.1) | 1.1 (0.5–2.8) |
| >10 | 54 (50) | 20 (34) | 1.1 (0.4–2.6) | 1.0 (0.4–2.3) |
| Level of education completed | ||||
| Secondary | 78 (79) | 43 (69) | Ref | |
| Primary | 21 (21) | 19 (31) | 1.6 (0.8–3.3) | 0.8 (0.4–1.7) |
| Tertiary | 30 (28) | 11 (20) | 0.7 (0.3–1.5) | 1.5 (0.6–3.5) |
| Have you received any specific training related to mpox reporting and referral | ||||
| No | 77 (39) | 64 (93) | Ref | |
| Yes | 52 (61) | 9 (7) | 4.8 (2.1–10) | 5 (2.2–11) |
| Ref: reference; COR: crude odds ratios; AOR: adjusted odds ratios; CI: confidence interval | ||||
Table 5: Multivariable logistic regression analysis on factors associated with knowledge toward mpox among community health workers in Mbarara City, Uganda, February 2025
| Variable | Attitude | cOR (95% CI) | aOR (95% CI) | |
|---|---|---|---|---|
| Positive | Negative | |||
| Age (years) | ||||
| ≤35 | 1 (5) | 29 (16) | Ref | |
| >35 | 20 (95) | 152 (84) | 3.8 (0.5–30) | 0.3 (0.03–2.9) |
| Gender | ||||
| Male | 39 (22) | 7 (33) | Ref | |
| Female | 142 (78) | 14 (67) | 0.5 (0.2–1.5) | 0.4 (0.1–1.4) |
| Work experience of CHWs (years) | ||||
| <5 | 80 (71) | 11 (73) | Ref | |
| 5–10 | 33 (29) | 4 (27) | 0.5 (0.1–3.2) | 1.1 (0.3–4.3) |
| >10 | 68 (46) | 6 (35) | 0.3 (0.1–1.5) | 0.9 (0.2–3.8) |
| Level of education completed | ||||
| Secondary | 109 (77) | 12 (60) | Ref | |
| Primary | 32 (23) | 8 (40) | 0.8 (0.3–2.9) | 0.6 (0.2–1.9) |
| Tertiary | 40 (27) | 1 (13) | 0.6 (0.2–1.8) | 4.3 (0.5–37) |
| Have you received any specific training related to mpox reporting and referral | ||||
| No | 124 (69) | 17 (81) | Ref | |
| Yes | 57 (31) | 4 (19) | 1.9 (0.6–6.1) | 0.9 (0.9–5.0) |
| Mpox knowledge | ||||
| Poor | 56 (31) | 17 (81) | Ref | |
| Good | 125 (69) | 4 (19) | 9.9 (3.1–29) | 9 (2.6–30) |
| Ref: reference; cOR: crude odds ratios; aOR: adjusted odds ratios; CI: confidence interval | ||||
Table 6. Factors associated with attitude toward mpox among community health workers in Mbarara City, Uganda, February 2025
Patrick Kwizera1,&, Richard Migisha1, Hannington Katumba1, Charity Mutesi1, Emmanuel Mfitundinda1, Owens Joyce Kobusingye1, Loryndah Olive Namakula1, Emmanuel Okiror Okello1, Abraham Muhwezi2, Dansan Atim3, Ivan Lukabwe1, Lilian Bulage1, Benon Kwesiga1, Alex Riolexus Ario1
1Uganda Public Health Fellowship Program-Uganda National Institute of Public Health, Kampala, Uganda, 2Department of Community Health, Faculty of Medicine, Mbarara University of Science and Technology, Uganda, 3Ministry of Health, Kampala, Uganda
&Corresponding author: Patrick Kwizera, Uganda Public Health Fellowship Program, Uganda National Institute of Public Health, Kampala, Uganda, Email: pkwizera@uniph.go.ug
Received: 29 Nov 2025, Accepted: 21 Mar 2026, Published: 26 Mar 2026
Domain: Infectious Disease Epidemiology
Keywords: Mpox, Knowledge, Attitude, Practices, Uganda
©Patrick Kwizera et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Patrick Kwizera et al. Knowledge, attitudes, and practices of community health workers regarding Mpox in Mbarara City, Uganda, February 2025. Journal of Interventional Epidemiology and Public Health. 2026; 9(1):52. https://doi.org/10.37432/jieph-d-25-00305
Introduction: Mpox is a re-emerging zoonotic viral disease with significant public health implications due to its potential for human-to-human transmission and outbreaks in urban areas. Community health workers (CHWs) play a critical role in surveillance, case detection, and health education; however, their preparedness for mpox control is not well documented. This study assessed the knowledge, attitudes, and practices (KAP) of CHWs regarding mpox transmission, detection, reporting, and referral in Mbarara City, February 2025.
Methods: We conducted a cross-sectional study in Mbarara City, southwestern Uganda, from February 1–15, 2025. Eligible participants were CHWs aged ≥18 years with at least one year of experience. Those unavailable during data collection were excluded. Using simple random sampling, CHWs were selected from a list of all CHWs across city wards. A self-administered, researcher-developed questionnaire comprising 26 mpox-related KAP items was used. Knowledge was assessed using 11 items, attitude with 5 items, and practice with 7 items, each worth 1 point. Scores >60% were classified as good knowledge, positive attitude, or good practices. Multivariate logistic regression was used to identify KAP-associated factors.
Results: Among 206 CHWs, 159 (77%) were female, and 127 (62%) had >10 years of experience. Four participants had not heard about mpox. In total, 64% (129/202) of participants had good knowledge, 90% (181/202) had positive attitudes, and seven (3%) demonstrated good practices. Regarding practices, 143 (73%) engaged in health education, 55 (28%) referred suspected cases, and 51 (26%) consistently reported to health authorities when a suspected case was identified. Having attended mpox-specific training (aOR=5.0; 95%CI: 2.2–11) and having good knowledge (aOR=9.0, 95%CI: 2.6–30) were significantly associated with a positive attitude.
Conclusion: While most CHWs showed positive attitudes about mpox, just about two-thirds had good knowledge. Serious gaps remain in case referral and reporting. Targeted CHWs training and mentorship could improve outbreak response effectiveness.
Mpox (formerly known as monkeypox) is a re-emerging zoonotic viral disease with human-to-human transmission occurring through close contact with infected persons or bodily fluids [1–3]. The incubation period ranges from 1–21 days, with most patients developing symptoms within seven days of exposure [4,5]. Mpox gained global attention following outbreaks in several countries. In response to increasing case counts, including notable outbreaks in the Democratic Republic of the Congo, the World Health Organization declared mpox a Public Health Emergency of International Concern (PHEIC) on August 14, 2024 [6].
Uganda confirmed its first human mpox cases on July 24, 2024. By November 30, 2024, a total of 745 PCR‐confirmed infections had been reported across 52 districts, including nearly 200 cases among children and adolescents [7]. Urban centers later became epicentres of transmission; for example, Mbarara City’s caseload rose from 92 in December 2024 to 123 in January 2025. This urban shift underscored critical gaps in prevention, early detection, and timely response.
Community health workers (CHWs) are essential for disease surveillance, case identification, and community education; however, their preparedness for mpox control has not been evaluated. Gaps in CHWs knowledge, attitudes, and practices (KAP) may contribute to delayed reporting and suboptimal outbreak response.
Previous KAP studies on emerging infections, including COVID-19 and Ebola, have demonstrated that adequate knowledge and positive attitudes among healthcare workers enhance adherence to infection prevention measures [8,9]. However, data on CHWs’ knowledge, attitudes and practices regarding mpox in Uganda remain limited. Addressing this gap will provide insights to guide health education, policy formulation, and capacity building for future outbreak preparedness and response. Therefore, this study assessed the KAP of CHWs regarding mpox in Mbarara City, Uganda, February 2025, to inform targeted interventions and strengthen community-based surveillance for mpox.
Study design and setting
This cross-sectional study was conducted from February 1–15, 2025, among CHWs from the 23 Wards of Mbarara City, located approximately 270 kilometres (about 168 miles) southwest of Kampala. Mbarara City has a catchment population of approximately 238,500 people. The city is bordered by Isingiro District to the south, Kiruhura District to the north, Rwampara District to the east, and Mbarara District to the west.
The public health disease surveillance system in Mbarara City is coordinated by a city surveillance focal person, who oversees surveillance activities citywide. The city is divided into two main divisions: North and South, with the South Division having two designated surveillance officers and the North Division having one. CHWs play an integral role in the disease surveillance structure and are routinely involved in community-level detection and reporting, particularly during public health events.
Study population and eligibility criteria
This study was conducted among CHWs in Mbarara city, southwestern Uganda. Eligible participants were CHWs aged ≥18 years, with at least one year of experience, and who provided voluntary consent. CHWs who were unavailable during the data collection period were excluded.
Sample size and sampling procedure
The sample size was determined using a single population proportion formula with the assumption of 50% proportion (since no previous such study was done in Uganda), 95% confidence level, and 5% margin of error. A 15% nonresponse rate was added, making the final sample size 206. The list of CHWs was obtained from the city health office, which was then used as a sampling frame. A simple random sampling technique was used to select the study participants, and the selection process was carried out using Microsoft Excel to ensure that each CHW member had an equal chance of being included in the study.
Data collection tools and procedures
Data were collected using a self-administered, researcher-developed structured questionnaire, comprised of four sections: sociodemographic characteristics, knowledge, attitudes, and practices related to mpox. Questionnaires were delivered by three trained public health officers.
The instrument began with sociodemographic items, including age, gender, education level, and years of service and proceeded to an 11-item knowledge section covering mpox aetiology, transmission, clinical presentation, and management. While the section contained 11 main questions, several allowed multiple correct response options, for example, symptoms, transmission routes, and preventive measures. Scoring was therefore based on individual correct response options rather than the number of questions. Each correct response option was awarded one point, and incorrect or “I don’t know” responses were scored zero. The maximum attainable knowledge score was 26 points.
Attitude items were single-response statements scored 1 for positive responses and 0 for negative responses, yielding a maximum attitude score of five points. Statements on perceived severity, confidence in response, and effectiveness of control measures were some of the questions.
Practices were assessed using seven questions related to prevention, case identification, referral, and reporting. Some questions included multiple appropriate practices. Each correct or appropriate practice was awarded one point. The cumulative maximum practice score was 17 points.
For each domain, individual scores were summed and converted into percentages. A threshold of ≥60% was used to classify respondents as having good knowledge, positive attitudes, or good practices, while scores <60% were classified as poor or negative. This cut-off follows Bloom’s criteria and has been widely applied in KAP studies to reflect a meaningful level of functional competence [10–13]. The questionnaire was developed based on a review of the literature and prior KAP studies on infectious diseases. Content validity was ensured by having the questionnaire reviewed by two public health experts for relevance and clarity. Although formal reliability testing was not conducted, the tool was pre-tested among 10 CHWs to assess clarity and comprehension.
Prior to participation, all CHWs provided verbal informed consent. This approach was chosen to minimise physical contact and potential transmission during the active mpox outbreak. The consent process, conducted by the trained public health officers, included an explanation of the study purpose, voluntary participation, confidentiality protections, and the right to withdraw at any time without consequence. Verbal consent was documented by the data collectors in Kobo Collect, which recorded the date and participant’s unique identifier, confirming that consent was obtained.
Data management and analysis
Data were collected using Kobo Collect and exported to Epi Info version 7.2.6.0 for analysis. Categorical variables were summarised using frequencies and percentages. Binary logistic regression was used to assess the association between independent (good KAP) and dependent variables. All variables in the bivariate analysis with a P-value of ≤0.2 were entered into a multivariate logistic regression model to determine the independent factors associated with KAP. A p-value of <0.05 was considered statistically significant.
Ethical considerations
This study was carried out as a response to a public health emergency and was classified as non-research. Administrative clearance was given by the Ministry of Health, Uganda, through the Office of the Director General of Health Services to conduct the study. Furthermore, the Centre for Global Health at the US Centers for Disease Control and Prevention (CDC) determined that the activity did not constitute human subjects research and was primarily intended for public health practice and disease control. Verbal informed consent was obtained from all participants, who were informed that participation was voluntary and that declining would not lead to any negative consequences. Verbal consent was chosen to minimize physical contact and potential transmission during the active mpox outbreak, in alignment with infection prevention and control guidance. To ensure confidentiality, unique identifiers were assigned, interviews were conducted privately, and data were stored securely under password protection by the study team. This activity was reviewed by the CDC and conducted in accordance with relevant federal laws and CDC policies (e.g., 45 C.F.R. part 46; 21 C.F.R. part 56; 42 U.S.C. §241(d); 5 U.S.C. §552a; 44 U.S.C. §3501 et seq.).
All 206 (100%) CHW members who received questionnaires completed and returned them. However, four participants were excluded from the analysis because they had not heard of mpox, leaving 202 participants for the assessment of knowledge, attitudes, and practices.
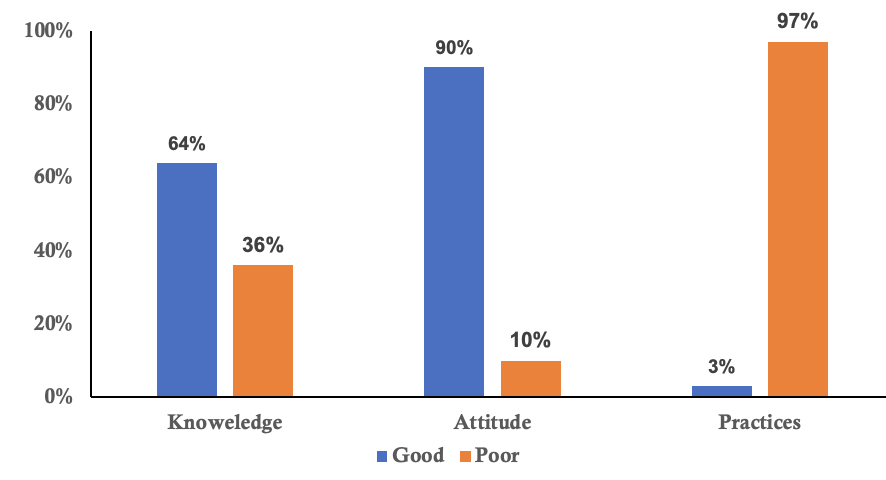
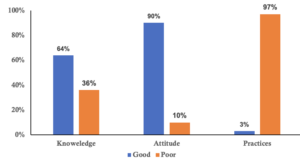
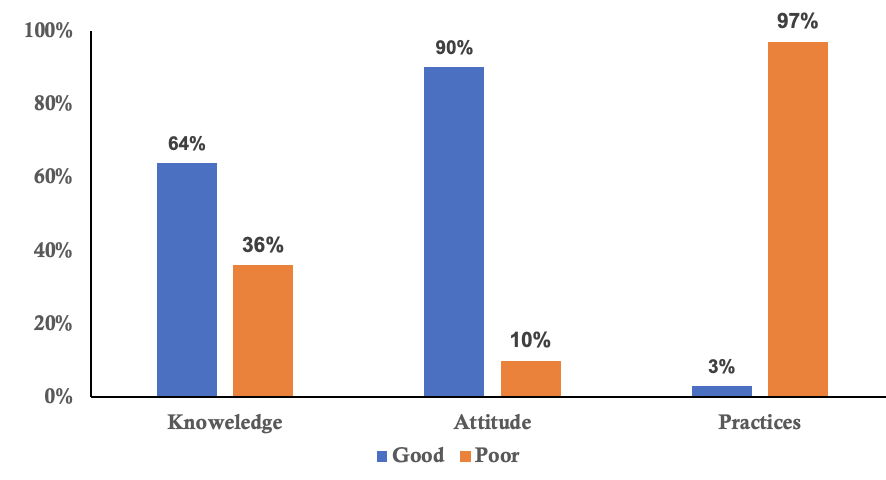
The mean age of respondents was 45 years (SD ± 10.5), with ages ranging from 20 to 70 years. The majority were female 159 (77%), with males accounting for 47 (23%). Most CHWs 127(62%) had over ten years of experience, and while 121(59%) had completed secondary education, only 41(20%) had attained tertiary education. Overall 202 (98%) participants had heard of mpox, and 61(30%) had received specific training on mpox (Table 1). Among 202 community health workers, 66% had good knowledge, 90% had a positive attitude, and only 3% demonstrated good practices (Figure 1).
The majority of the CHWs demonstrated a good understanding of key aspects related to mpox. One hundred and thirty-two (65%) knew how mpox is transmitted, and 70% were aware that specific treatments for mpox exist. Additionally, 81% of CHWs were knowledgeable about how to detect mpox cases in their communities, and 85% understood the procedures for reporting suspected cases. The majority of CHWs (96%) were aware of the health facilities to which they should refer suspected mpox cases, and 87% had access to the contact information for these health facilities (Table 2). Overall, 133 (66%) community health workers had good knowledge about the mpox.
The majority of the CHWs (n=158; 78%) considered the threat of mpox to be serious for the community’s health and well-being. Additionally, 176 (87%) of CHWs were confident in their ability to identify and manage a suspected mpox case. 180(89%) of CHWs believed in the effectiveness of mpox prevention measures, such as vaccination and handwashing. However, 123 (61%) of the CHWs felt that the community was not well-prepared to prevent the spread of mpox, while 138 (68%) of CHWs felt supported by local health authorities in their role in preventing mpox (Table 3). Overall, 181(90%) community health workers had a positive attitude towards mpox (Figure 1).
Regarding practices for community education and referral activities related to mpox, most of the respondents indicated involvement in community education or awareness activities about mpox 143 (71%). However, fewer respondents actively referred suspected mpox cases to higher health facilities 55 (27%) or reported suspected cases to health authorities regularly 55 (25%). A portion of participants (29%) reported conducting home visits to educate households on mpox prevention (Table 4). Overall, only 7(3%) community health workers demonstrated good practices regarding mpox and the majority 195(97%) exhibited poor practices (Figure 1).
Individuals who received specific training related to mpox were 5 times more likely to have good knowledge compared to those who did not receive training (aOR=5.0, 95%CI:2.2-11) (Table 5). Similarly, individuals who had good knowledge were 9 times more likely to have a positive attitude compared to those who had poor knowledge (aOR=9.0, 95%CI:2.6-30) (Table 6)
This study assessed the KAP of CHWs in Mbarara City, Uganda, regarding mpox. Overall, 64% of CHWs demonstrated good knowledge, 90% had a positive attitude, yet only 3% exhibited good practices. While mpox-specific training was significantly associated with better outcomes among CHWs [14,15], overall knowledge levels likely reflect multiple contributing factors beyond formal training, including exposure to mpox itself, informal learning from community sensitization efforts and prior experience in epidemic response [16,17]. These findings suggest that both structured training and experiential learning play critical roles in shaping CHWs’ knowledge during emerging infectious disease outbreaks.
The high level of mpox knowledge observed in this study is consistent with findings from other settings where frontline health workers were assessed during an infectious disease outbreak. For example, similar levels of mpox knowledge were reported among health workers in (58.7%), China (56.5%), and Algerian health workers (64.9%) [16–18]. Similarly, moderate to high disease awareness was noted among healthcare workers during the COVID-19 pandemic in Saudi Arabia and Uganda, likely reflecting the impact of intensified public health messaging and emergency response training [8,19]. These observations suggest that repeated exposure to epidemic information and prior experience managing emerging infections can elevate awareness among frontline health workers, including CHWs.
The majority of CHWs (90%) demonstrated a positive attitude toward mpox prevention and control, a proportion comparable to that observed among Indonesian general practitioners (84.3%) and Nigerian health workers (87.8%) [20,21], suggesting that CHWs are generally motivated and receptive to public health guidance. The strong association observed between good knowledge and positive attitude in this study underscores that knowledge acquisition may foster confidence and proactive engagement [21]. Our findings also mirror other studies during COVID-19 among health workers, which reported similarly high positive attitudes [22,23].
In terms of practices, the study findings revealed good practice in only 3%. This finding is comparable to a study among health workers in Uganda, which reported that 88% exhibited poor practices [24]. Other studies, such as one conducted in Vietnam, reported slightly better outcomes, with 51.8% of participants demonstrating good practices [15]. The study from Kenya during COVID-19 among health workers also reported poor practices [25]. The pronounced gap between knowledge and practice likely reflects several contextual challenges. Operational barriers, such as insufficient supplies, lack of personal protective equipment (PPE), and unclear reporting pathways, may limit CHWs’ ability to act on their knowledge [25,26]. Systemic factors, including inadequate supportive supervision and insufficient feedback mechanisms, have also been identified as challenges for effective practice among frontline health workers in Uganda [27].
Despite active participation in awareness campaigns, CHWs infrequently referred or reported suspected mpox cases to health authorities. This pattern mirrors observations from other African settings, where CHWs while essential for community sensitization and preventive outreach, proved most effective only when supported by comprehensive training and adequate resources [26].
A key limitation of this study was its reliance on quantitative survey data alone; the absence of a qualitative component prevented in-depth exploration of CHWs’ experiences, motivations, and the contextual factors influencing their mpox-related KAP. Incorporating qualitative methods, such as in-depth interviews or focus groups, in future research could elucidate the specific barriers and facilitators that shape CHW engagement in outbreak response. Additionally, the reliance on self-reported data may have introduced social desirability bias, where participants tend to overreport desirable behaviours, such as participation in community education, and underreport undesirable ones, like failure to refer suspected cases. These biases could have led to an overestimation of knowledge and attitude levels, while underestimating the extent of poor practices among the CHWs. Information bias is also possible, as the study did not capture the sources of CHWs’ knowledge, for example, community sensitization and social media, which may affect the validity of the ‘good knowledge’ classification.
Several practice items were binary (yes/no) and did not capture frequency, consistency, or quality of behaviour, potentially limiting precision. The questionnaire was pre-tested among only 10 CHWs, and formal reliability testing was not conducted, which may affect measurement accuracy. Finally, our findings are specific to an urban setting (Mbarara City) and may not be generalizable to CHWs in rural Uganda, where access to resources, information, and training may differ substantially.
Although CHWs in Mbarara City demonstrated adequate mpox knowledge and positive attitudes, largely due to targeted training their actual referral and reporting practices were insufficient. While mpox-specific training was associated with improved knowledge, overall knowledge levels likely reflect multiple factors, including outbreak exposure, informal learning, and prior epidemic response experience. These findings highlight a critical gap between knowledge and practice, suggesting that awareness alone is insufficient for effective outbreak response.
From a public health perspective, strengthening CHWs’ capacity requires targeted hands-on training, supportive supervision, timely feedback, and provision of the necessary resources to facilitate case detection, referral, and reporting. Future research should investigate the operational and systemic factors, as well as potential behavioural barriers, that could influence CHWs’ translation of knowledge into practice. Addressing these gaps is critical to improving community-level mpox detection, referral, and outbreak control
What is already known about the topic
What this study adds
The authors declare no competing interests. Lilian Bulage is an Associate Editor at the Journal of Interventional Epidemiology and Public Health (JIEPH) and a co-author of this manuscript. In line with the journal’s conflict of interest policy, he was fully recused from the peer review process and had no involvement in editorial handling or decision-making for this submission. An independent editor oversaw the review and decision-making process.
This study was supported by Korea Foundation for International Healthcare (KOFIH) under the project titled, “Strengthening Health Systems to Prevent, Detect and Respond to Infectious Diseases in Uganda”. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
We extend our appreciation to Mbarara City Health Office team, City Health Educator for their overall coordination and leadership during the study in the city. We also thank Community health workers for the active participation. Lastly, we recognize the Uganda Public Health Fellowship Program that provided technical oversight, and the Ministry of Health offered supervisory support.
PK, conceptualized the study idea, collected data, analyzed it and wrote the manuscript.HK, CM, EM, OJK, LON, EOO, AM, conceptualized the study idea, collected data and reviewed the manuscript. RM, IL, BK, LB, DA and ARA supported in editing, and reviewing of the manuscript. All authors read and approved the final manuscript.
| Variable | Frequency (%) |
|---|---|
| Age (years) | |
| ≤ 35 | 31 (15) |
| > 35 | 175 (85) |
| Gender | |
| Male | 47 (23) |
| Female | 159 (77) |
| Work experience of CHWs (years) | |
| < 5 | 43 (21) |
| 5–10 | 36 (17) |
| > 10 | 127 (62) |
| Level of education completed | |
| Primary | 44 (21) |
| Secondary | 121 (59) |
| Tertiary | 41 (20) |
| Have you heard about mpox | |
| Yes | 202 (98) |
| No | 4 (2) |
| Have you received any specific training related to mpox | |
| Yes | 61 (30) |
| No | 141 (70) |
| Items* | N (%) |
|---|---|
| 1. How is mpox transmitted? | 132 (65) |
| 2. Are there specific treatments for mpox? | 141 (70) |
| 3. Do you know how to detect mpox cases in your community? | 163 (81) |
| 4. Do you know the procedure for reporting a suspected mpox case? | 172 (85) |
| 5. Are you aware of the specific health facilities to which you should refer suspected mpox cases in your community? | 194 (96) |
| 6. Do you have access to the contact information of health facilities for mpox referrals in your community? | 175 (87) |
| *Responses to the items indicate only the “yes” category | |
| Items | N (%) |
|---|---|
| 1. How serious do you think the threat of mpox is for the community’s health and well-being? | 158 (78) |
| 2. How confident are you in your ability to identify and manage a suspected mpox case? | 176 (87) |
| 3. Do you think the community is well-prepared to prevent the spread of mpox? | 123 (61) |
| 4. How would you rate your personal belief in the effectiveness of mpox prevention measures (e.g., vaccination, hand washing)? | 180 (89) |
| 5. Do you feel supported by local health authorities in your role as a CHWs in preventing mpox? | 138 (68) |
| Item | N (%) |
|---|---|
| Have you been involved in community education or awareness activities about mpox? | 143 (71) |
| Do you actively refer suspected mpox cases to higher health facilities? | 55 (27) |
| How regularly do you report suspected mpox cases to health authorities? | 51 (25) |
| Do you conduct home visits to educate households on mpox prevention? | 59 (29) |
| Variable | Knowledge | COR (95% CI) | AOR (95% CI) | |
|---|---|---|---|---|
| Good (%) | Poor (%) | |||
| Age (years) | ||||
| ≤35 | 22 (17) | 8 (11) | Ref | |
| >35 | 107 (83) | 65 (89) | 1.7 (0.7–3.9) | 0.7 (0.2–1.9) |
| Gender | ||||
| Male | 28 (22) | 18 (25) | Ref | |
| Female | 101 (78) | 55 (75) | 1.9 (0.8–4.5) | 0.6 (0.3–1.6) |
| Work experience of CHWs (years) | ||||
| <5 | 53 (71) | 38 (72) | Ref | |
| 5–10 | 22 (29) | 15 (28) | 0.9 (0.4–2.1) | 1.1 (0.5–2.8) |
| >10 | 54 (50) | 20 (34) | 1.1 (0.4–2.6) | 1.0 (0.4–2.3) |
| Level of education completed | ||||
| Secondary | 78 (79) | 43 (69) | Ref | |
| Primary | 21 (21) | 19 (31) | 1.6 (0.8–3.3) | 0.8 (0.4–1.7) |
| Tertiary | 30 (28) | 11 (20) | 0.7 (0.3–1.5) | 1.5 (0.6–3.5) |
| Have you received any specific training related to mpox reporting and referral | ||||
| No | 77 (39) | 64 (93) | Ref | |
| Yes | 52 (61) | 9 (7) | 4.8 (2.1–10) | 5 (2.2–11) |
| Ref: reference; COR: crude odds ratios; AOR: adjusted odds ratios; CI: confidence interval | ||||
| Variable | Attitude | cOR (95% CI) | aOR (95% CI) | |
|---|---|---|---|---|
| Positive | Negative | |||
| Age (years) | ||||
| ≤35 | 1 (5) | 29 (16) | Ref | |
| >35 | 20 (95) | 152 (84) | 3.8 (0.5–30) | 0.3 (0.03–2.9) |
| Gender | ||||
| Male | 39 (22) | 7 (33) | Ref | |
| Female | 142 (78) | 14 (67) | 0.5 (0.2–1.5) | 0.4 (0.1–1.4) |
| Work experience of CHWs (years) | ||||
| <5 | 80 (71) | 11 (73) | Ref | |
| 5–10 | 33 (29) | 4 (27) | 0.5 (0.1–3.2) | 1.1 (0.3–4.3) |
| >10 | 68 (46) | 6 (35) | 0.3 (0.1–1.5) | 0.9 (0.2–3.8) |
| Level of education completed | ||||
| Secondary | 109 (77) | 12 (60) | Ref | |
| Primary | 32 (23) | 8 (40) | 0.8 (0.3–2.9) | 0.6 (0.2–1.9) |
| Tertiary | 40 (27) | 1 (13) | 0.6 (0.2–1.8) | 4.3 (0.5–37) |
| Have you received any specific training related to mpox reporting and referral | ||||
| No | 124 (69) | 17 (81) | Ref | |
| Yes | 57 (31) | 4 (19) | 1.9 (0.6–6.1) | 0.9 (0.9–5.0) |
| Mpox knowledge | ||||
| Poor | 56 (31) | 17 (81) | Ref | |
| Good | 125 (69) | 4 (19) | 9.9 (3.1–29) | 9 (2.6–30) |
| Ref: reference; cOR: crude odds ratios; aOR: adjusted odds ratios; CI: confidence interval | ||||