Research | Open Access | Volume 9 (2): Article 81 | Published: 21 May 2026

Views: 1,315
Menu, Tables and Figures
| Variable | Number (N=268) | Frequency % | (95% CI) | P value |
|---|---|---|---|---|
| Median age in years [IQR] | 45 [28-68] | |||
| Sex | ||||
| Male | 170 | 63 | 57-69 | < 0.0001 |
| Female | 87 | 32 | 27-38 | |
| Not classified | 11 | 4 | 2.1-7.2 | |
| Age-group | ||||
| 0-28 days | 15 | 6 | 3-9 | < 0.0001 |
| 1-11 months | 5 | 2 | 0.6-4.3 | |
| 1-4 yrs | 8 | 3 | 1.3-5.8 | |
| 5-14 yrs | 19 | 7 | 4.3-11 | |
| 15-24 yrs | 17 | 6 | 3.7-10 | |
| 25-49 yrs | 81 | 30 | 25-36 | |
| 50-64 yrs | 39 | 15 | 11-19 | |
| 65-79 yrs | 36 | 13 | 9.6-18 | |
| ≥ 80 yrs | 31 | 12 | 8.0-16 | |
| Not classified | 17 | 6 | 3.7-9.9 | |
| Usual place of residence | ||||
| Within Masaka City and District | 149 | 56 | 49-62 | 0.07 |
| Outside Masaka City and District | 119 | 44 | 38-51 | |
| Source of death alert | ||||
| Community members | 82 | 31 | 25-36 | < 0.0001 |
| Police | 48 | 18 | 13-23 | |
| VHT system | 17 | 6.3 | 3.7-9.9 | |
| Funeral Home | 2 | 0.8 | 0.1-2.7 | |
| Facility | 119 | 44 | 38-50 | |
| Place of death | ||||
| Community | 137 | 51 | 45-57 | 0.74 |
| Facility | 131 | 49 | 43-55 | |
| Sample collection status | ||||
| Collected | 240 | 90 | 85-93 | < 0.0001 |
| Not collected | 28 | 10 | 7-15 | |
| Sample collection results (n=240) | ||||
| Negative | 240 | 100 | ||
| Death has documented cause of death | ||||
| Yes | 101 | 38 | 32-44 | < 0.0001 |
| No | 167 | 62 | 56-68 | |
| Nature of death | ||||
| Natural death | 73 | 27 | 22-33 | < 0.0001 |
| Unnatural death | 28 | 10 | 7.1-15 | |
| Not recorded | 167 | 62 | 56-68 | |
Table 1: Characteristics of deaths reported during an SVD outbreak in Masaka, Uganda, November to December 2022 (N=268)
| Variable | Community deaths | Health facility deaths | Community vs Health facility deaths P value | ||||
|---|---|---|---|---|---|---|---|
| n=137 | % | (95% CI) | n=131 | % | (95% CI) | ||
| Median age in years [range] | 45 [2-107] | 47 [0-95] | |||||
| Sex | |||||||
| Male | 94 | 69 | 60-76 | 76 | 58 | 49-66 | 0.06 |
| Female | 39 | 28 | 21-37 | 48 | 37 | 28-45 | 0.0008 |
| Not classified | 4 | 3 | 0.8-7.3 | 7 | 5 | 2.2-10 | 0.40 |
| Age-group | |||||||
| 0-28 days | 5 | 3.7 | 1.2-8.3 | 10 | 7.6 | 3.7-13 | 0.17 |
| 1-11 months | 3 | 2.2 | 0.5-6.3 | 2 | 1.5 | 0.2-5.4 | 0.67 |
| 1-4 yrs | 3 | 2.2 | 0.5-6.3 | 5 | 3.8 | 1.3-8.7 | 0.44 |
| 5-14 yrs | 11 | 8.0 | 4.1-14 | 8 | 6.1 | 2.7-12 | 0.54 |
| 15-24 yrs | 8 | 5.8 | 2.6-11 | 9 | 6.9 | 3.2-13 | 0.72 |
| 25-49 yrs | 43 | 31.4 | 24-39 | 38 | 29.0 | 21-38 | 0.67 |
| 50-64 yrs | 17 | 12.4 | 7.4-19 | 22 | 16.8 | 10-24 | 0.31 |
| 65-79 yrs | 17 | 12.4 | 7.4-19 | 19 | 14.5 | 8.9-22 | 0.61 |
| ≥ 80 yrs | 21 | 15.3 | 9.8-22 | 10 | 7.6 | 3.7-14 | 0.05 |
| Not classified | 9 | 6.6 | 3.1-12 | 8 | 6.1 | 2.7-12 | 0.88 |
| Usual place of residence | |||||||
| Within Masaka City and District | 95 | 69 | 61-77 | 54 | 41 | 33-50 | 0.01 |
| Outside Masaka City and District | 42 | 31 | 23-39 | 77 | 59 | 50-67 | < 0.0001 |
| Source of death alert | |||||||
| Community members | 75 | 55 | 46-63 | 7 | 5 | 2.2-11 | < 0.0001 |
| Police | 44 | 32 | 24-41 | 4 | 3 | 0.8-7.6 | < 0.0001 |
| VHT system | 13 | 9 | 5.2-16 | 4 | 3 | 0.8-7.6 | 0.04 |
| Funeral Home | 2 | 1 | 0.2-5.2 | 0 | 0 | 0-2.8 | 0.25 |
| Facility | 3 | 2 | 0.5-6.3 | 116 | 89 | 82-93 | < 0.0001 |
| Sample collection status | |||||||
| Collected | 116 | 85 | 78-90 | 124 | 95 | 89-98 | 0.007 |
| Not collected | 21 | 15 | 9.8-22 | 7 | 5 | 2.2-11 | 0.007 |
| Sample collection results | |||||||
| Negative | 116 | 100 | 124 | 100 | |||
| Nature of death | |||||||
| Natural death | 30 | 22 | 15-30 | 43 | 33 | 24-42 | 0.04 |
| Unnatural death | 23 | 17 | 11-24 | 5 | 3.8 | 1.3-8.9 | 0.002 |
| Not recorded | 84 | 61 | 53-70 | 83 | 63 | 55-72 | 0.74 |
Table 2: Reported Deaths by Community and health facility November – December 2022 (N=268)
| Age-group | Sex | Place of usual residence | Nature of death | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Males (n=170) | Females (n=87) | P value | Within Masaka (n=149) | Outside Masaka (n=119) | P value | Natural causes (n=73) | Unnatural causes (n=28) | P value | |||||||
| n (%) | 95% CI | n (%) | 95% CI | n (%) | 95% CI | n (%) | 95% CI | n (%) | 95% CI | n (%) | 95% CI | ||||
| 0-28 days | 4 (2) | 0.64-5.9 | 1 (1.2) | 0.03-6.2 | 0.59 | 8 (5.4) | 2.4-10 | 7 (5.9) | 2.4-12 | 0.86 | 9 (12) | 5.8-22 | 0 (0) | 0-12 | 0.06 |
| 1-11 months | 3 (2) | 0.37-5.1 | 1 (1.2) | 0.03-6.2 | 0.59 | 2 (1.3) | 0.2-4.8 | 3 (2.5) | 0.5-7.2 | 0.47 | 2 (2.7) | 0.3-9.6 | 0 (0) | 0-12 | 0.38 |
| 1-4 yrs | 7 (4) | 1.7-8.3 | 1 (1.2) | 0.03-6.2 | 0.14 | 6 (4.0) | 1.5-8.6 | 2 (1.7) | 0.2-5.9 | 0.27 | 3 (4.1) | 0.9-12 | 1 (3.6) | 0.1-18 | 0.91 |
| 5-14 yrs | 8 (5) | 2.1-9.1 | 11 (13) | 6.5-21 | 0.01 | 8 (5.4) | 2.4-10 | 11 (9.2) | 4.7-16 | 0.23 | 3 (4.1) | 0.9-12 | 1 (3.6) | 0.1-18 | 0.91 |
| 15-24 yrs | 7 (4) | 1.7-8.3 | 10 (11) | 5.7-20 | 0.02 | 8 (5.4) | 2.4-10 | 9 (7.6) | 3.5-14 | 0.46 | 4 (5.5) | 1.5-13 | 4 (14) | 4.0-33 | 0.16 |
| 25-49 yrs | 60 (35) | 28-43 | 21 (24) | 16-35 | 0.04 | 40 (27) | 20-35 | 41 (34) | 26-44 | 0.21 | 12 (16) | 8.8-27 | 16 (57) | 37-76 | <0.0001 |
| 50-64 yrs | 31 (18) | 13-25 | 8 (9.2) | 4.1-17 | 0.03 | 24 (16) | 11-23 | 15 (13) | 7.2-20 | 0.49 | 14 (19) | 11-30 | 3 (11) | 2.3-28 | 0.34 |
| 65-79 yrs | 25 (15) | 9.8-21 | 11 (13) | 6.5-21 | 0.62 | 25 (17) | 11-24 | 11 (9.2) | 4.7-16 | 0.06 | 15 (21) | 12-32 | 1 (3.6) | 0.1-18 | 0.03 |
| ≥ 80 yrs | 16 (9) | 5.5-15 | 15 (17) | 9.9-17 | 0.04 | 22 (15) | 9.5-21 | 9 (7.6) | 3.5-14 | 0.06 | 6 (8.2) | 3.1-17 | 0 (0) | 0-12 | 0.12 |
| Not classified | 9 (5) | 2.5-9.8 | 8 (9.2) | 4.0-17 | 0.15 | 6 (4) | 1.5-8.6 | 11 (9.2) | 4.7-16 | 0.08 | 5 (6.9) | 2.3-15 | 2 (7) | 0.9-24 | 0.99 |
Table 3: Distribution of Deaths across Age-groups by Sex, Usual Residence, and Nature of Death in Masaka City and District , November to December 2022, (N=268)
| Cause of death | Total | Females | Males | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | 95% CI | n | % | 95% CI | n | % | 95% CI | |
| Accidents and Injuries | 27 | 27 | 19-36 | 5 | 19 | 6.3-38 | 22 | 33 | 22-45 |
| Cardiovascular conditions | 16 | 16 | 9.3-24 | 4 | 15 | 4.2-34 | 12 | 18 | 9.6-29 |
| Respiratory conditions | 12 | 12 | 6.3-20 | 2 | 7.4 | 0.9-24 | 10 | 15 | 7.4-26 |
| Perinatal conditions | 9 | 9 | 4.2-16 | 0 | 0 | 0.0-13 | 9 | 3 | 0.4-10 |
| HIV related conditions | 7 | 7 | 2.8-14 | 4 | 15 | 4.2-34 | 3 | 4.5 | 0.9-13 |
| Cancer | 6 | 6 | 2.2-12 | 3 | 11 | 2.4-29 | 3 | 4.5 | 0.9-13 |
| Disease not specified | 5 | 5 | 1.6-11 | 3 | 11 | 2.4-29 | 2 | 3 | 0.4-10 |
| Other causes | 4 | 4 | 1.2-10 | 0 | 0 | 0.0-13 | 4 | 5.4 | 1.2-10 |
| Anaemia | 3 | 3 | 0.6-8.4 | 2 | 7.4 | 0.9-24 | 1 | 1.5 | 0.0-8.0 |
| Kidney related conditions | 3 | 3 | 0.6-8.4 | 1 | 3.7 | 0.1-19 | 2 | 3 | 0.4-10 |
| Septicaemia | 3 | 3 | 0.6-8.4 | 2 | 7.4 | 0.9-24 | 1 | 1.5 | 0.0-8.0 |
| Diabetes | 2 | 2 | 0.2-7.0 | 0 | 0 | 0.0-13 | 2 | 3 | 0.4-10 |
| Malaria | 2 | 2 | 0.2-7.0 | 1 | 3.7 | 0.1-19 | 1 | 1.5 | 0.0-8.0 |
| Old age | 2 | 2 | 0.2-7.0 | 0 | 0 | 0.0-13 | 2 | 3 | 0.4-10 |
Table 4: Distribution of causes of death during an Ebola outbreak in Masaka, Uganda, November to December 2022 (n=101)
Maureen Katusiime1,&, Alice Namale1, Samuel Kalungi2, Allan Muruta3, David Musoke4, Evelyn Akello1, Anatoli Mawanda2, Edgar Kansiime1, Bernard Lubwama3, Faith Nakiyimba5, Peter James Elyanu6, Rachel King7, Patrick Kagurusi8, Rhoda Wanyenze1,4, Henry Kyobe Bosa3,9
1Disease Surveillance and Response Unit, Makerere University School of Public Health, Monitoring and Evaluation Technical Support (METS) Program, Kampala, Uganda, 2Department of Pathology, Mulago National Referral Hospital, Kampala, Uganda, 3Department of Integrated Epidemiology, Surveillance, and Public Health Emergencies, Ministry of Health, Kampala, Uganda, 4School of Public Health, Makerere University College of Health Sciences, Kampala, Uganda, 5District Health Office, Masaka District Local Government, Masaka, Uganda, 6Global Health Security, Baylor College of Medicine Children’s Foundation, Uganda, 7Department of Epidemiology and Biostatistics, University of California, San Francisco, 8Amref Health Africa, Uganda, 9Uganda People’s Defence Forces, Bombo, Uganda
&Corresponding author: Maureen Katusiime, Makerere University School of Public Health, Kampala, Uganda, Email: mkatusiime@musph.ac.ug, ORCID: https://orcid.org/0000-0003-0643-9957
Received: 01 Apr 2026, Accepted: 20 May 2026, Published: 21 May 2026
Domain: Infectious Disease Epidemiology
Keywords: Mortality surveillance, outbreak investigation, infectious diseases, Sudan virus disease outbreak, cause of death
©Maureen Katusiime et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Maureen Katusiime et al., Mortality surveillance implementation to identify transmission chains during the Sudan virus disease outbreak in Masaka, Uganda, 2022. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):81.https://doi.org/10.37432/jieph-d-26-00105
Introduction: Six weeks into the Sudan Virus Disease (SVD) outbreak response in Uganda, Masaka City registered a case on November 1st, 2022. We describe the design of mortality surveillance implemented to ensure no transmission chains were missed and epidemiologically characterise deaths reported.
Methods: Similar to other SVD epicentre districts (Mubende, Kassanda, and Kampala) in Uganda, health workers, Village Health Teams, security, and other local structures were trained in death reporting. Records at 33 health facilities in Masaka City and District were reviewed, and an alert desk was activated. Upon receiving a death alert, laboratory and surveillance officers were dispatched to investigate deaths and collect samples (arterial blood or buccal swab) from cadavers for Sudan Virus testing. A death-linelist was populated by sociodemographics, date of death, source of alert, and test result. We conducted a descriptive analysis of deaths.
Results: Between November 10th and December 30th 2022, 268 deaths were reported, 90% had samples collected, and none (0%) tested positive for SVD. Median age at death was 45 years (IQR: 28-68), and the age group 25-49 years (30%) recorded most deaths. Males (170, 63%) were more affected than females (87, 32%) (p<0.001). Community (137, 51%) and facility deaths (131, 49%) (p=0.74) were comparable. Thirty eight percent (101 of 268) had cause of death documented. Leading causes of death were accidents and injuries (27%), cardiovascular (16%), respiratory (12%) and perinatal conditions (9%). Natural causes of death (21% [15 of 73] were more prevalent among individuals aged 65-79 years vs unnatural causes (3.6% [1 of 28]; p<0.03). Unnatural causes were more prevalent among the age group 25-49 years (57% [16 of 28] compared to natural causes 16% [12 of 73]; p<0.0001).
Conclusion: No secondary transmission of SVD occurred; instead, individuals died of other causes. It is feasible to conduct mortality surveillance during an SVD outbreak to rule out silent transmission. We recommended strengthening mortality surveillance at the local and national levels to improve epidemic surveillance and response.
Infectious diseases with the potential to trigger severe outbreaks and cause mortality remain a critical threat to global health, especially in low-income countries [1-3]. Emerging pathogens causing these diseases include: coronaviruses, novel influenza strains, arboviruses, hemorrhagic fevers, antimicrobial-resistant bacteria, climate-linked fungal and parasitic infections [2-6]. Factors precipitating disease transmission include: ecological factors, climate change, global mobility, antimicrobial resistance, systemic weaknesses and expanding human-animal interfaces [3-8]. Most emerging infections (60% to 80%) stem from animal sources [6]. Substantial advancements, including genomic surveillance, molecular diagnostics such as PCR and metagenomic sequencing, vaccine utilisation, development of novel pharmaceuticals like monoclonal antibodies, broad-spectrum antivirals and the optimization of vector and zoonotic control have strengthened global response capacity for detection, diagnosis, infection control and therapy [3, 7, 9]. However, substantial gaps in surveillance, diagnostics, and access to medical countermeasures persist which makes infectious diseases continue to cause morbidity and mortality [3, 7].
Ebola Disease (EBOD) is an emerging and re-emerging zoonotic disease [8,10]. It is a hemorrhagic, severe and often fatal illness caused by Orthoebolavirus genus of the filoviridae family that affects humans and other primates [10,11]. Ebolaviruses enter the human population through close contact with the blood, secretions, organs or other bodily fluids of infected animals [10-12]. Human-to-human transmission occurs through direct contact with blood, organs, secretions or body fluids of infected or dead people and/or contaminated surfaces and materials [11,12].
EBOD has triggered severe outbreaks and has pandemic potential [11,12]. Most large outbreaks in Africa have been caused by Bundibugyo Virus (BDBV), Sudan Virus (SUDV), and Ebola viruses [11,13-15]. The largest and most complex outbreak since EBOD discovery in the Democratic Republic of Congo (DRC) and Sudan in 1976 was the 2014–2016 outbreak in West Africa (Guinea, Sierra Leone, and Liberia), which resulted in over 28,600 cases and 11,325 deaths [11,13, 14]. In the last four decades (1976 to 2019), 34 outbreaks have occurred, resulting in over 34,350 cases and 14,820 deaths in 11 Sub-Saharan African countries, including the DRC, South Sudan, Uganda, Mali, Nigeria, Sierra Leone, Guinea, Liberia, South Africa, Gabon, and Côte d’Ivoire [11-15]. Case fatality rates vary from 25% to 90%, with an average of 50% [11,12, 14, 16]. Without treatment, up to 90% of cases with Ebola virus disease (EVD) die while the Sudan virus disease (SVD) has CFR of about 50% (range 41%-100%) of cases [11, 13, 14]. There are no licensed vaccines or therapeutics for the prevention and treatment of SVD [11] but candidate therapeutics and vaccines have been availed [8, 17].
Uganda reported the first and largest EBOD outbreak in 2000, due to the SUDV in Gulu District, where 425 cases and 224 deaths (CFR=53%) were recorded [16, 18]. Since then, several SVD outbreaks have been reported in Masindi (2000), Mbarara (2000), Luwero (2011 and 2012), and Kibale (2012) [14, 16,18]. On 20th September 2022, Uganda declared an SVD outbreak in Mubende District. This outbreak marked the 7th EVD outbreak in the country, representing the 5th outbreak due to SUDV, and the 8th globally [14, 16, 19, 20]. Six weeks into the outbreak response, the disease had spread to six districts from Mubende to Kassanda, Kyegegwa, Kagadi, Bunyangabu, Wakiso, and Kampala.
On November 1st, 2022, the Masaka City reported its first confirmed case and death from SUDV, marking the eighth district affected in the country. This was a female in their early 20s who had travelled from Kampala District to Masaka to be taken care of by her parents. [21]. While in Masaka, she was first hospitalised at a private clinic in Kimaanya, a village, where health workers handled her with the necessary precautions before referral to a higher-level facility. Two days prior, she presented to Masaka Regional Referral Hospital (RRH) with signs and symptoms of Ebola. She was immediately isolated, and a blood sample was collected and shipped to Uganda Virus Research Institute (UVRI)-Entebbe, which tested positive for SUDV by Polymerase Chain Reaction (PCR). She was immediately evacuated to the Entebbe Ebola treatment Unit, where she succumbed to the deadly virus [21].
The staff at the private clinic were immediately isolated, and the clinic closed temporarily [22]. Contact tracing and follow-up were initiated, and community encouraged to be vigilant in identifying and reporting anyone with symptoms related to SUDV [22]. Since the case had interacted with many contacts, many of whom were untraceable, we anticipated uncharacterised SUDV transmission chains. The Ministry of Health (MoH), Uganda, immediately dispatched a team to boost an end-to-end case identification process and strengthen mortality surveillance implementation in Masaka City and Masaka District [20].
Conducting mortality surveillance during emergencies is essential to measure the impact of the outbreak on affected populations, estimate the magnitude of needs, monitor the effectiveness of response efforts and advocate for resources [23, 24]. Mortality surveillance is the systematic and continuous collection, compilation, analysis and dissemination of the incidence and causes of deaths in defined populations [24]. The gold standard tools for monitoring mortality are civil registration and vital statistics (CRVS) systems, complemented by regular census [23]. Having functional CRVS systems can provide governments with information about deaths and their causes [25]. However, such tools are missing or deficient in most emergencies [23, 24].
Most low and middle-income countries have CRVS systems that are incomplete or are not able to provide reliable data about deaths and their causes [24, 26, 27]. The CRVS system in Uganda remains weak, with a death registration rate of 17% [28]. Furthermore, a rapid assessment of mortality surveillance in Uganda revealed data quality and completeness gaps, including suboptimal data being transmitted from the community and health facilities to the national database [28]. Therefore, this article describes the design of mortality surveillance implemented during the SVD outbreak response in Masaka and presents an epidemiological analysis of deaths reported.
Study design and setting
This was a cross-sectional study of mortality surveillance data collected prospectively during the 2022 SVD outbreak in Uganda. The study was conducted in Masaka City and Masaka District, located in Central Uganda, approximately 132 kilometres from Kampala. Masaka City had an estimated population of 121,200, and Masaka District had 227,600 people [29] with a population growth rate of 1%. Masaka City has 11 health facilities, and Masaka District has 21 health facilities.
Description of the mortality surveillance intervention
The design of mortality surveillance was an extension of what was already happening in other response districts: Mubende, Kassanda and Kampala. Mortality surveillance was systematically rolled out at national, district, health facility and community levels.
At the national level: Following a presidential directive to investigate all deaths during the SVD outbreak, national-level teams were deployed to affected districts, including Masaka, to establish networks for death reporting and conduct field investigations at the health facility and community level [20]. To facilitate investigations, a case was defined as the death of a person of any age that occurred from November 6th, 2022, to December 30th, 2022, who was a resident of or visitor to Masaka City and Masaka District.
At the district level: A death-tracking desk was established in the Situation Room located at the District Health Office. The situation room was established to coordinate and support the SVD response efforts. Communities and health facilities reported death alerts to the situation room through the alert management using a toll-free number that had been widely disseminated. Upon receiving a death alert, a surveillance officer and a laboratorian or mortician were dispatched to investigate the deaths and collect samples (arterial blood or buccal swab) from cadavers for SUDV testing.
At the health facility level: Health workers were trained on death identification and reporting through the ‘alert management’ desk. They reviewed medical records daily to systematically identify deaths. Upon death identification, the cadaver was moved to the facility’s mortuary or holding room, where the trained mortuary attendant and surveillance officer administered a viral haemorrhagic fever case investigation form (VHF CIF) by interviewing the health workers and close relatives of the deceased and ensured sample collection. The VHF form included questions about demographics (age, sex, residence, and occupation of the deceased), clinical signs and symptoms, including the date and time of onset, hospitalization information, risk factors and exposures for SVD transmission, and laboratory characteristics of the deceased. The health facility detained any suspicious death until the results were issued before burial.
At the community level, networks of community resource persons were established to report deaths, including Village Health Teams (VHTs), Parish Coordinators, funeral homes’ staff, security and police officers, Local Council chairpersons, and media stations. The resource persons were oriented on death identification and reporting and provided a toll-free line to report any death occurrence within the community. Leveraged other programs within the community to sensitise the public about SVD and the need for real-time reporting. A coordinator in each Parish was assigned to collect death information from every village within their catchment and report it to the district while trained VHTs moved door to door to identify deaths and report to parish coordinators. Upon finding a death, the parish coordinator or any resource person would alert the district situation room through the toll-free number. The district would in turn dispatch officers to investigate the death and collect a sample for SUVD testing. Relatives of the deceased were encouraged not to bury any suspicious deaths before receipt of results.
Laboratory investigation
Clinical samples, including arterial blood and/or buccal swabs from cadavers, were transported using the existing MOH hub system to the Central Public Health Laboratories (CPHL) Kampala or Uganda Virus Research Institute for PCR testing. Blood specimens were tested using Reverse Transcription (RT)-quantitative PCR or Enzyme-Linked Immunosorbent Assay (ELISA) (Centers for Disease Control and Prevention [CDC], Atlanta, GA, USA) at the UVRI -Haemorrhagic Fever laboratory. The UVRI used the MagMax Kit (Applied Biosystems, Lithuania) to extract Ribonucleic Acid (RNA), followed by RT-PCR on Applied Biosystems QuantStudio 5 or 7500 Real-Time PCR System instruments (Applied Biosystems, Lithuania) using the CDC custom primers and probes. Laboratory detection of the six species that cause EBOD , Marburg disease, Crimean–Congo haemorrhagic fever, and Rift Valley fever viruses was conducted [16].
Data management and analysis
Teams populated a death-linelist in Excel using the data captured from the VHF CIF forms from the field (health facilities and community). Death line-lists had variables such as age, sex, residential address of deceased by village, parish, subcounty, district, place and date of death, source of death alert and SUDV test result. We analyzed data using Excel and EpiInfo 7.2. We describe deaths rates by age-group and sex, and place of usual residence, nature of death and cause of death. We calculated crude death rates per 100,000 population using the Uganda Population and Housing Census data from 2014 to 2019 [29]. We computed frequencies and percentages and compared proportions using χ2. A p value of < 0·05 was considered statistically significant.
Ethical considerations
This investigation was conducted in response to a public health emergency, and as such, it was determined to be non-research. As such, the MOH authorised this study and waived the requirement for IRB approval and written consent from participants. The MOH and District provided administrative clearance and approval to investigate because its primary intent was to inform outbreak response and disease control. Verbal informed consent in the local language was obtained from all respondents who were aged >18years and close relatives of the deceased. They were informed that their participation was voluntary, and their refusal would not result in any negative consequences. Risks to investigators were minimised by ensuring that they underwent training on SVD infection prevention and control (IPC). To enable sample collection from cadavers, they were equipped with the necessary Personal Protective Equipment (PPE) to prevent infection. The analysis was conducted using anonymised administrative data collected during the outbreak response. Data collected did not contain any individual personal identifiers and was stored in password-protected computers. This was only accessed and analysed by designated staff. It was not accessible to anyone outside the investigation team.
Characteristics of reported deaths
A total of 268 deaths were reported (from the community and health facilities) between November 10th and December 30th, 2022. Median age at death was 45 years [IQR: 28-68] and most were among persons aged 25-49 years (30% [81 of 268]). Males (170, 63%) were more affected than females (87, 32%) (p<0.001) (Table 1). Community (137, 51%) and facility deaths (131, 49%), p=0.07) were comparable. Of the 268 reported deaths, 240 (90%) had samples collected for SVD testing, and all tested negative. Data on nature of death were available for 101 (38%) deaths, and 73 (27%), p < 0.001, were natural causes (Table 1).
Differences between facility and community deaths
Age, sex, nature of death and usual place of residence differed between community and facility deaths. Facility deaths had a higher median age (47 years [range: 0-95] compared to community deaths (45 years [range: 2-107]. More females died in the health facility (37% [48 of 131] compared to community 28% [39 of 137]; p=0.001 while more males died in the community (69% [94 of 137] compared to facility (58% [76 of 131]; p=0.06). Natural causes of death were more prevalent in both health facility and community deaths compared to unnatural causes, with a higher proportion of natural causes being registered among facility deaths, 33% [43 of 131] compared to community deaths, 22% [30 of 137]; p=0.04. Most facility deaths were individuals whose usual place of residence was outside Masaka, 59% [77 of 131] (Table 2).
More deaths occurred among males than females across most age-groups except for the age groups: 5-14years (13% [11of 87 females] vs 5% [8 of 170 males]; p=0.01), 15-24-years (11% [10 of 87 females] vs 4% [7 of 170 males]; p=0.02) and those ≥ 80 years (17% [15 of 87] vs 9% [16 of 170]; p=0.04) where more deaths occurred among females (Table 2). A higher proportion of deaths across most age groups had their usual place of residence outside Masaka City and District. However, age-groups 50-64 years (16% [24 of 149] vs 13% [15 of 119]; p=0.49), 65-79 years (17% [25 of 149] vs 9.2% [11 of 119]; p=0.06) and those aged ≥ 80 years (15% [22 of 149] vs 7.6% [9 of 119]; p=0.06) had usual place of residence within Masaka City and District (Table 2).
More deaths were due to natural compared to unnatural causes across most age-groups, being most prevalent among the age group 65-79 years (21% [15 of 73 natural] vs 3.6% [1 of 28 unnatural causes]; p<0.03). However, unnatural causes were most prevalent among those aged 25-49 years (57% [16 of 28 unnatural] compared to natural causes 16% [12 of 73 natural causes]; p<0.0001) (Table 2).
Causes of death
Of the 268 deaths, 167 (62%) had missing data on the cause of death. Among the 101 deaths with data on cause of death, accidents and injuries (27%), cardiovascular diseases (16%), respiratory diseases (12%), perinatal conditions (9%) and HIV related conditions (7%) were the leading causes of death in Masaka from November 10th to December 30th, 2024 (Table 4).
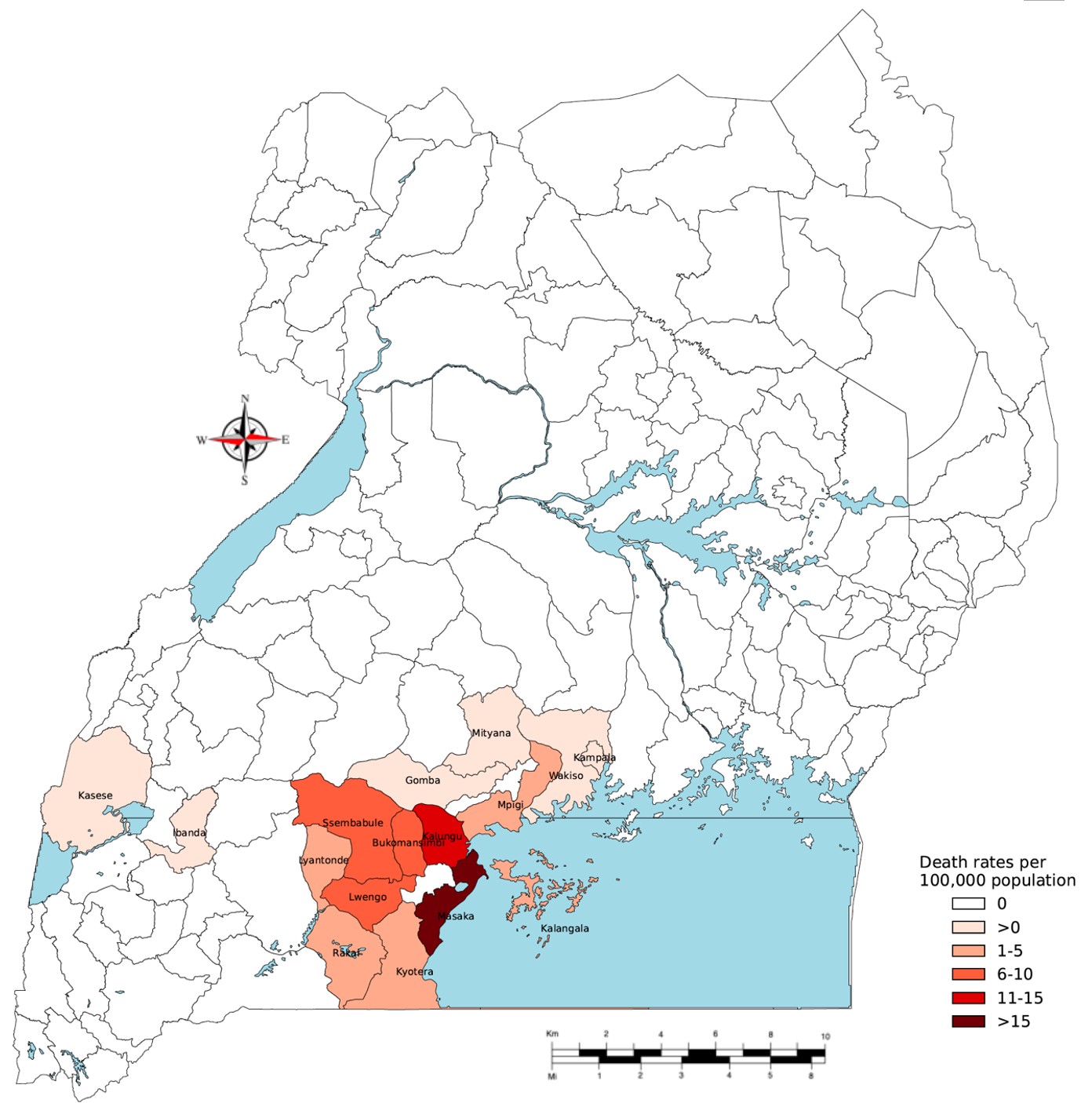
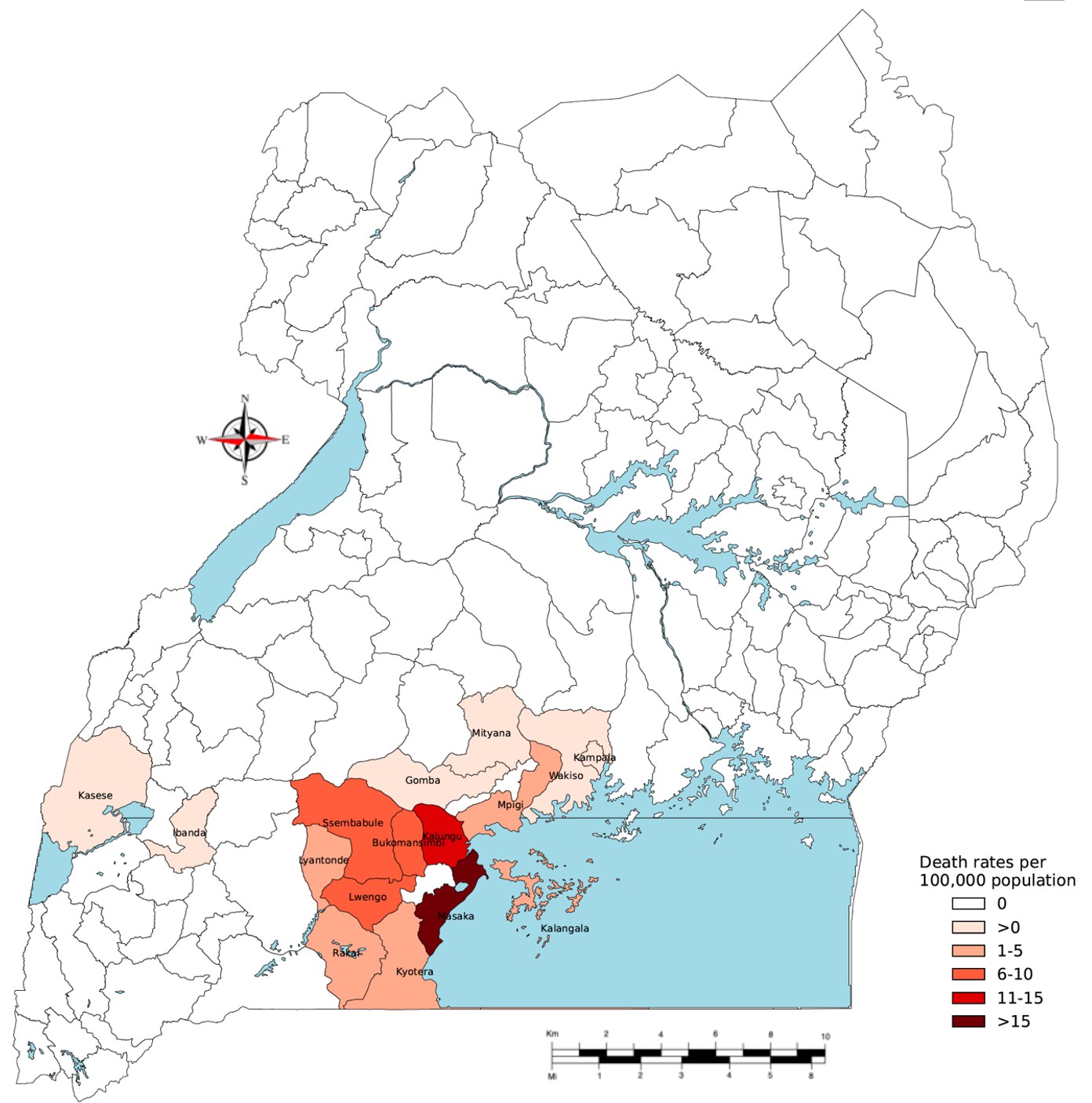
Deaths by usual place of residence
Masaka City and District registered the highest crude death rate (43 deaths per 100,000 population), followed by Kalungu (12.2 deaths per 100,000 population) and Lwengo (9.5 deaths per 100,000 population, Figure 1).
Our study describes the design of implementing systematic mortality surveillance to ensure no transmission chains were missed during the SVD outbreak and presents an epidemiological analysis of investigated deaths reported from Masaka City and District between November 10th and December 30th, 2022. We found that deaths differed between community and health facility by age, sex, nature of death and place of usual residence. All samples collected tested negative for SUDV, indicating that we did not detect secondary transmission of SVD within Masaka, but rather these people died from other causes. Therefore, strengthening mortality surveillance avails timely data for epidemic surveillance and response [30] and informs strategic public health actions to improve the health system. Our study highlights that it is feasible to implement systematic mortality surveillance during an SVD outbreak.
We demonstrate the capacity of local authorities at various levels to respond to the sudden increased demand for real-time data because they were able to identify, report deaths, and conduct deeper epidemiological investigations, which informed response actions. This design may be adopted in both routine and outbreak response protocols for local, national and global levels. Given that in 2020–2021, 37 (19%) of World Health Organization (WHO) member states produced partial or incomplete mortality data with limited utility, while 84 (43%) states had no mortality data [24, 27]. Furthermore, Uganda has had mechanisms to generate mortality data, such as the rapid mortality surveillance project, which aimed to understand the true impact of COVID-19 on excess mortality, but sustaining its gains after the pandemic was dependent on donor funding [24, 31]. In addition, the Maternal and Perinatal Death Surveillance and Response implementation is limited to maternal and perinatal deaths and has not been implemented rigorously during outbreaks [32], yet the Demographic and Health Surveys are conducted periodically to get estimates of child and maternal mortality [24]. Following the 2022 SVD response, the Ministry of Health adapted mortality surveillance as part of the outbreak response protocols in Uganda. Since then, the country has had a resurgence of EBOD, particularly the SVD outbreak in 2025 [33] and the Bundibugyo virus disease (BVD) outbreak confirmed on 15th May 2026, currently in response mode [34]. This underscores the critical need for heightened mortality surveillance in outbreaks and continuous strengthened pandemic preparedness and response efforts.
Consistent with other studies, we found more deaths among males compared to females [31, 35, 36 – 38]. Women tend to live longer than men in most countries [36, 37]. Possibly because of differences in biological factors (hormonal and chromosomal genetic differences), epidemiological context (how people live, disease dominance and exposures to mortality risk, and health resources in place), and social and behavioural circumstances [36-39]. For example, female hormones may provide protection against some inflammatory and immunological-related conditions like cardiovascular disease, yet males are more vulnerable to these conditions; women are able to maintain homeostasis and have greater resistance to oxidative damage, unlike men [37, 40]. Second, women have 2 X chromosomes, which may help to compensate for a mutation, unlike men, so any sexually antagonistic male genes would shorten male life [37]. Third, women are more likely to adopt healthier habits and lifestyles, such as healthier diets, less smoking and alcohol consumption, safer driving, fewer violent deaths and accidents, and regular medical checkups compared to men [39]. To support this further, our results showed that more female deaths occurred in health facilities than in communities when compared to males, similar to findings from Ethiopia [41]. Hence, the need for targeted interventions to reduce sex-specific mortality.
While women have lower mortality than men in most countries [42], we found higher deaths among females aged 5-14, 15-24 years and those ≥ 80 years compared to males. Similar findings were reported among females aged 0 to 25 years in Trinidad during an investigation on the survival of males and females under extreme conditions of famine, epidemics, and slavery [42]. However, the WHO Global Health Estimates release in 2019 revealed no difference in death distribution between females and males aged 5-14 years, but higher death rates among males aged 15-29 years compared to females in the African Region [35]. A possible explanation for this finding could be that women and girls face severe disadvantages such as limited access to healthcare, inadequate nutrition and gender-based discrimination practices such as early marriage or pregnancy [38]. As evidenced by 24% of teenagers in Uganda who become pregnant by 19 years, 34% of these girls are married by 18 years, and 28% of maternal deaths occur among young girls aged 15-25 years [43]. Also, 33% of girls below the age of 15 years in Uganda are forced to have their first sex [43]. Furthermore, countries with high gender inequality indices are associated with high maternal deaths, compared with those with lower gender inequality, whilst countries that spend less on health are associated with higher maternal deaths [44]. This underscores the relevance of making strategic investments towards mortality reduction among adolescent girls and young women, including elderly women in Uganda.
We found that community and facility deaths were comparable, similar to a Singapore study [45]. On the contrary, 60% of deaths in low-income countries occur at home, with the highest (90% ) registered in sub-Saharan countries like Ethiopia, Chad, South Sudan [41, 46] and over 70% in Tanzania and Papua New Guinea [47, 48]. In Uganda, health facilities reported more deaths compared to the community during the COVID-19 Pandemic [31]. Having heightened surveillance implemented at both community and facility levels during this SVD outbreak might have contributed to this finding [20]. This may also indicate that when interventions are intensified at various levels, gaps between facility and community death reporting reduce [20]. Additionally, having strong leadership and strategies to coordinate data collection, analysis and dissemination enables countries to meet the mortality data demand [24, 30]. To support this further, our data showed that the major source of death alerts was community members, followed by police and VHTS arising from the rigorous community mobilisation sessions and stakeholder engagements, ensuring the safety of responders by working with local authorities and security organs during the response [20]. In South Africa, the use of community and stakeholder engagement was a key lesson learnt in setting up an urban-based Health and Demographic Surveillance System [49]. Our study supports strengthening local death reporting. Global and local case reporting has been highlighted as a critical research and policy priority [9]. We did not explore reasons why individuals die in the community, but people prefer to die at home because of fear of nosocomial infections, visiting restrictions, and health capacity limitations [50, 51] , especially during outbreaks. Other factors include: social-cultural, attitudes and beliefs [52 -54]. To support this further, one in ten hospitalised patients acquires nosocomial infections mainly due to patient characteristics (age, gender), medical practices and environmental factors [55].
Contrary to our expectation, all samples collected tested negative for SVD, a possible indication that we did not detect secondary transmission of SVD in Masaka, but rather people died from other causes. A possible explanation for this is the intensified IPC measures and community engagement strategies put in place during the response. Furthermore, the index case of Masaka was quickly identified and referred to the Ebola treatment Unit, where standard precautions were implemented, which reduced the risk of infection exposure to the population [20].
Consistent with statistics in the African Region, including Uganda [31, 35], we found that most health facility and community deaths were due to natural causes, especially among individuals aged 65-79 years. Similarly, between 2020 and 2021, the top causes of death for people aged 65 years and older in the United States were natural causes such as heart disease, cancers, COVID-19 and cerebrovascular diseases [56]. One possibility is the limited use of the International Classification of Diseases (ICD -11) to classify the causes of death at health facilities. Cause of death is a critical part of the CRVS and should ideally come from medical certification [46]. In 2023, only one-fifth of the estimated 61 million deaths globally had meaningful ICD-coded data reported to WHO [57]. Moreover, mortality estimation in many African countries is hindered by inadequate capacity to capture the accurate cause of death due to a lack of medical certification of deaths [43, 46] arising from a lack of training for deaths occurring at health facilities and having no clinical oversight for deaths occurring at the community level [43, 46]. Additionally, mortality rates are mostly estimated using incomplete data because many low and middle-income countries have poorly developed CRVS systems to collect data on numbers and causes of death [24, 26], [58]. Hence, strengthening the capacity of health workers to certify causes of death using ICD-11 and investing in health information systems that produce high-quality data are key [30].
Unnatural causes of death, particularly accidents and injuries, were the leading causes of death in our study. On the contrary, injuries in the African region are the 9th leading cause of death, contributing 3.8 % to all deaths while ranking 6th in Uganda [35]. This discrepancy may be attributed to specific characteristics of our study population, where most deaths occurred among individuals aged 25-49, mainly being unnatural deaths. This age group is mobile, in their prime working years and often engages in risk-taking behaviours, which increases their likelihood of experiencing accidents, injuries and occupational hazards. Individuals aged 25-49 years accounted for 31.3% of road fatalities in 2023 in the European Union [59]. Similarly, a rapid assessment of road crashes in Uganda revealed that the age group 18-44 years suffered most road accidents due to careless and/or careless driving, over speeding and road factors [60]. This highlights that Uganda loses a significant proportion of its economically active population [43]. Hence, the need to strengthen efforts such as public awareness and behavioural change communication on accident and injury prevention.
Our study had some limitations: It was not possible to determine gender for 4%, age for 6% and cause of death for 62% of individuals in our study, arising from missing medical records. This might have caused some bias in the sex and age-specific death rates, as well as cause-specific mortality fractions affecting representativeness and under-reporting for cause of death. Therefore, our findings should be interpreted with caution. However, we used the complete case/list wise deletion analysis (where we omitted all records with missing cause of death data and only analysed those which had cause of death) to handle missing data because it is known to produce unbiased and conservative results [61].
According to WHO, nearly one-third of countries had never reported cause-of-death data as of the end of 2025. In addition, only one-third of the estimated 61 million deaths reported in 2023 globally had cause-of-death data [57]. Secondly, we did not have complete individual-level mortality data before the SVD outbreak to compare with reported deaths in this study. Third, limited generalizability because our study was conducted in an outbreak setting whose dynamics may be different from routine care because data were primarily collected for outbreak containment. Fourth, death certificates were not used during data collection, but rather teams conducted interviews with relatives and caregivers of deceased persons during the outbreak. However, interviews serve as a valid method often applied in epidemiological studies [62, 63].
Teams purposively investigated communities that had sent death alerts to the district call centre and did not pick samples or conduct interviews in communities that did not send in alerts, hence a risk of under-reporting of mortality. Last, our study ruled out SVD as the cause of death and classified death as natural or unnatural. However, it does not provide evidence towards the use of ICD-11 codes for certification of the cause of death that occurred. This may possibly limit the deeper evaluation of the cause of death, as well as the potential unreliability towards the certification process for causes of death reported in our study. Many countries lack the capacity to capture accurate causes of death due to a lack of medical certification of deaths [46, 57]. Therefore, more investments in stronger systems to increase the use of ICD 11 coding for facility deaths, improve data quality and completeness and understand the nature of death for community deaths are needed.
We highlight that it was possible to avail real-time data on mortality during the SUDV outbreak through implementing systematic mortality surveillance. We did not detect secondary transmission of SVD in Masaka but rather people died of other causes. Health facility and community deaths were comparable, and males had more deaths than females. Natural causes of death were most prevalent among individuals aged 65-79 years while unnatural causes where most prevalent among the 25–49 years age-group. Therefore, implementing prospective mortality surveillance as a key intervention should be adapted in outbreak response protocols at local and/or national levels to inform epidemic surveillance and response. National roll out of mortality surveillance in a phased manner including greater investments in stronger health information systems that will produce quality data is needed.
What is already known about the topic
What this study adds
No specific funding was received for this study, but rather different organizations and agencies facilitated field deployments of responders to enhance mortality surveillance implementation in the study area. Funders had no role in the implementation, data collection, analysis and writing of this manuscript.
We acknowledge the Ministry of Health for granting authorization to conduct this investigation in Masaka City and District. We acknowledge the technical and financial support received from the Uganda Ministry of Health, Masaka City and District health staff, AMREF Health Africa, Rockefeller Foundation, Makerere School of Public Health, US CDC, Baylor Foundation Uganda, JHPIEGO Uganda, WHO, and others. We also thank the community, and data management teams for their determination that led to the successful collection of mortality data during the outbreak.
MK, HKB, AN, AM, DM, SK, EK, PE, RW: designed and led implementation of the study and data collection.
MK: performed analysis, interpretation and drafted the manuscript.
MK, AN, SK, AM, DM, EA, AM, EK, BL, FN, PE, RK, PK, RW, and KKB reviewed the manuscript to ensure intellectual content and scientific integrity. All authors reviewed and approved the final version of the manuscript.
| Variable | Number (N=268) | Frequency % | (95% CI) | P value |
|---|---|---|---|---|
| Median age in years [IQR] | 45 [28-68] | |||
| Sex | ||||
| Male | 170 | 63 | 57-69 | < 0.0001 |
| Female | 87 | 32 | 27-38 | |
| Not classified | 11 | 4 | 2.1-7.2 | |
| Age-group | ||||
| 0-28 days | 15 | 6 | 3-9 | < 0.0001 |
| 1-11 months | 5 | 2 | 0.6-4.3 | |
| 1-4 yrs | 8 | 3 | 1.3-5.8 | |
| 5-14 yrs | 19 | 7 | 4.3-11 | |
| 15-24 yrs | 17 | 6 | 3.7-10 | |
| 25-49 yrs | 81 | 30 | 25-36 | |
| 50-64 yrs | 39 | 15 | 11-19 | |
| 65-79 yrs | 36 | 13 | 9.6-18 | |
| ≥ 80 yrs | 31 | 12 | 8.0-16 | |
| Not classified | 17 | 6 | 3.7-9.9 | |
| Usual place of residence | ||||
| Within Masaka City and District | 149 | 56 | 49-62 | 0.07 |
| Outside Masaka City and District | 119 | 44 | 38-51 | |
| Source of death alert | ||||
| Community members | 82 | 31 | 25-36 | < 0.0001 |
| Police | 48 | 18 | 13-23 | |
| VHT system | 17 | 6.3 | 3.7-9.9 | |
| Funeral Home | 2 | 0.8 | 0.1-2.7 | |
| Facility | 119 | 44 | 38-50 | |
| Place of death | ||||
| Community | 137 | 51 | 45-57 | 0.74 |
| Facility | 131 | 49 | 43-55 | |
| Sample collection status | ||||
| Collected | 240 | 90 | 85-93 | < 0.0001 |
| Not collected | 28 | 10 | 7-15 | |
| Sample collection results (n=240) | ||||
| Negative | 240 | 100 | ||
| Death has documented cause of death | ||||
| Yes | 101 | 38 | 32-44 | < 0.0001 |
| No | 167 | 62 | 56-68 | |
| Nature of death | ||||
| Natural death | 73 | 27 | 22-33 | < 0.0001 |
| Unnatural death | 28 | 10 | 7.1-15 | |
| Not recorded | 167 | 62 | 56-68 | |
| Variable | Community deaths | Health facility deaths | Community vs Health facility deaths P value | ||||
|---|---|---|---|---|---|---|---|
| n=137 | % | (95% CI) | n=131 | % | (95% CI) | ||
| Median age in years [range] | 45 [2-107] | 47 [0-95] | |||||
| Sex | |||||||
| Male | 94 | 69 | 60-76 | 76 | 58 | 49-66 | 0.06 |
| Female | 39 | 28 | 21-37 | 48 | 37 | 28-45 | 0.0008 |
| Not classified | 4 | 3 | 0.8-7.3 | 7 | 5 | 2.2-10 | 0.40 |
| Age-group | |||||||
| 0-28 days | 5 | 3.7 | 1.2-8.3 | 10 | 7.6 | 3.7-13 | 0.17 |
| 1-11 months | 3 | 2.2 | 0.5-6.3 | 2 | 1.5 | 0.2-5.4 | 0.67 |
| 1-4 yrs | 3 | 2.2 | 0.5-6.3 | 5 | 3.8 | 1.3-8.7 | 0.44 |
| 5-14 yrs | 11 | 8.0 | 4.1-14 | 8 | 6.1 | 2.7-12 | 0.54 |
| 15-24 yrs | 8 | 5.8 | 2.6-11 | 9 | 6.9 | 3.2-13 | 0.72 |
| 25-49 yrs | 43 | 31.4 | 24-39 | 38 | 29.0 | 21-38 | 0.67 |
| 50-64 yrs | 17 | 12.4 | 7.4-19 | 22 | 16.8 | 10-24 | 0.31 |
| 65-79 yrs | 17 | 12.4 | 7.4-19 | 19 | 14.5 | 8.9-22 | 0.61 |
| ≥ 80 yrs | 21 | 15.3 | 9.8-22 | 10 | 7.6 | 3.7-14 | 0.05 |
| Not classified | 9 | 6.6 | 3.1-12 | 8 | 6.1 | 2.7-12 | 0.88 |
| Usual place of residence | |||||||
| Within Masaka City and District | 95 | 69 | 61-77 | 54 | 41 | 33-50 | 0.01 |
| Outside Masaka City and District | 42 | 31 | 23-39 | 77 | 59 | 50-67 | < 0.0001 |
| Source of death alert | |||||||
| Community members | 75 | 55 | 46-63 | 7 | 5 | 2.2-11 | < 0.0001 |
| Police | 44 | 32 | 24-41 | 4 | 3 | 0.8-7.6 | < 0.0001 |
| VHT system | 13 | 9 | 5.2-16 | 4 | 3 | 0.8-7.6 | 0.04 |
| Funeral Home | 2 | 1 | 0.2-5.2 | 0 | 0 | 0-2.8 | 0.25 |
| Facility | 3 | 2 | 0.5-6.3 | 116 | 89 | 82-93 | < 0.0001 |
| Sample collection status | |||||||
| Collected | 116 | 85 | 78-90 | 124 | 95 | 89-98 | 0.007 |
| Not collected | 21 | 15 | 9.8-22 | 7 | 5 | 2.2-11 | 0.007 |
| Sample collection results | |||||||
| Negative | 116 | 100 | 124 | 100 | |||
| Nature of death | |||||||
| Natural death | 30 | 22 | 15-30 | 43 | 33 | 24-42 | 0.04 |
| Unnatural death | 23 | 17 | 11-24 | 5 | 3.8 | 1.3-8.9 | 0.002 |
| Not recorded | 84 | 61 | 53-70 | 83 | 63 | 55-72 | 0.74 |
| Age-group | Sex | Place of usual residence | Nature of death | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Males (n=170) | Females (n=87) | P value | Within Masaka (n=149) | Outside Masaka (n=119) | P value | Natural causes (n=73) | Unnatural causes (n=28) | P value | |||||||
| n (%) | 95% CI | n (%) | 95% CI | n (%) | 95% CI | n (%) | 95% CI | n (%) | 95% CI | n (%) | 95% CI | ||||
| 0-28 days | 4 (2) | 0.64-5.9 | 1 (1.2) | 0.03-6.2 | 0.59 | 8 (5.4) | 2.4-10 | 7 (5.9) | 2.4-12 | 0.86 | 9 (12) | 5.8-22 | 0 (0) | 0-12 | 0.06 |
| 1-11 months | 3 (2) | 0.37-5.1 | 1 (1.2) | 0.03-6.2 | 0.59 | 2 (1.3) | 0.2-4.8 | 3 (2.5) | 0.5-7.2 | 0.47 | 2 (2.7) | 0.3-9.6 | 0 (0) | 0-12 | 0.38 |
| 1-4 yrs | 7 (4) | 1.7-8.3 | 1 (1.2) | 0.03-6.2 | 0.14 | 6 (4.0) | 1.5-8.6 | 2 (1.7) | 0.2-5.9 | 0.27 | 3 (4.1) | 0.9-12 | 1 (3.6) | 0.1-18 | 0.91 |
| 5-14 yrs | 8 (5) | 2.1-9.1 | 11 (13) | 6.5-21 | 0.01 | 8 (5.4) | 2.4-10 | 11 (9.2) | 4.7-16 | 0.23 | 3 (4.1) | 0.9-12 | 1 (3.6) | 0.1-18 | 0.91 |
| 15-24 yrs | 7 (4) | 1.7-8.3 | 10 (11) | 5.7-20 | 0.02 | 8 (5.4) | 2.4-10 | 9 (7.6) | 3.5-14 | 0.46 | 4 (5.5) | 1.5-13 | 4 (14) | 4.0-33 | 0.16 |
| 25-49 yrs | 60 (35) | 28-43 | 21 (24) | 16-35 | 0.04 | 40 (27) | 20-35 | 41 (34) | 26-44 | 0.21 | 12 (16) | 8.8-27 | 16 (57) | 37-76 | <0.0001 |
| 50-64 yrs | 31 (18) | 13-25 | 8 (9.2) | 4.1-17 | 0.03 | 24 (16) | 11-23 | 15 (13) | 7.2-20 | 0.49 | 14 (19) | 11-30 | 3 (11) | 2.3-28 | 0.34 |
| 65-79 yrs | 25 (15) | 9.8-21 | 11 (13) | 6.5-21 | 0.62 | 25 (17) | 11-24 | 11 (9.2) | 4.7-16 | 0.06 | 15 (21) | 12-32 | 1 (3.6) | 0.1-18 | 0.03 |
| ≥ 80 yrs | 16 (9) | 5.5-15 | 15 (17) | 9.9-17 | 0.04 | 22 (15) | 9.5-21 | 9 (7.6) | 3.5-14 | 0.06 | 6 (8.2) | 3.1-17 | 0 (0) | 0-12 | 0.12 |
| Not classified | 9 (5) | 2.5-9.8 | 8 (9.2) | 4.0-17 | 0.15 | 6 (4) | 1.5-8.6 | 11 (9.2) | 4.7-16 | 0.08 | 5 (6.9) | 2.3-15 | 2 (7) | 0.9-24 | 0.99 |
| Cause of death | Total | Females | Males | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | 95% CI | n | % | 95% CI | n | % | 95% CI | |
| Accidents and Injuries | 27 | 27 | 19-36 | 5 | 19 | 6.3-38 | 22 | 33 | 22-45 |
| Cardiovascular conditions | 16 | 16 | 9.3-24 | 4 | 15 | 4.2-34 | 12 | 18 | 9.6-29 |
| Respiratory conditions | 12 | 12 | 6.3-20 | 2 | 7.4 | 0.9-24 | 10 | 15 | 7.4-26 |
| Perinatal conditions | 9 | 9 | 4.2-16 | 0 | 0 | 0.0-13 | 9 | 3 | 0.4-10 |
| HIV related conditions | 7 | 7 | 2.8-14 | 4 | 15 | 4.2-34 | 3 | 4.5 | 0.9-13 |
| Cancer | 6 | 6 | 2.2-12 | 3 | 11 | 2.4-29 | 3 | 4.5 | 0.9-13 |
| Disease not specified | 5 | 5 | 1.6-11 | 3 | 11 | 2.4-29 | 2 | 3 | 0.4-10 |
| Other causes | 4 | 4 | 1.2-10 | 0 | 0 | 0.0-13 | 4 | 5.4 | 1.2-10 |
| Anaemia | 3 | 3 | 0.6-8.4 | 2 | 7.4 | 0.9-24 | 1 | 1.5 | 0.0-8.0 |
| Kidney related conditions | 3 | 3 | 0.6-8.4 | 1 | 3.7 | 0.1-19 | 2 | 3 | 0.4-10 |
| Septicaemia | 3 | 3 | 0.6-8.4 | 2 | 7.4 | 0.9-24 | 1 | 1.5 | 0.0-8.0 |
| Diabetes | 2 | 2 | 0.2-7.0 | 0 | 0 | 0.0-13 | 2 | 3 | 0.4-10 |
| Malaria | 2 | 2 | 0.2-7.0 | 1 | 3.7 | 0.1-19 | 1 | 1.5 | 0.0-8.0 |
| Old age | 2 | 2 | 0.2-7.0 | 0 | 0 | 0.0-13 | 2 | 3 | 0.4-10 |