Perspective![]() | Volume 8, Article 19, 10 Apr 2025
| Volume 8, Article 19, 10 Apr 2025
Vulstan James Shedura1,2,&, Shira Mangube2, Sabina Julius Ipembe2
1Department of Clinical Research, Training, and Consultancy, Southern Zone Referral Hospital, Mtwara, Tanzania, 2Health department, Regional Public Health Emergency Operational Centre, Mtwara, Tanzania.
&Corresponding author: Vulstan James Shedura, Department of Clinical Research, Training, and Consultancy, Southern Zone Referral Hospital, P.O. Box 272, Mtwara, Tanzania. Tel:+255659808713. Email: vulstanshedura@gmail.com, ORCID: https://orcid.org/0000-0002-1939-2492.
Received: 13 Jan 2025, Accepted: 09 Apr 2025, Published: 10 Apr 2025
Domain: Outbreak Investigation, Field Epidemiology, Infectious Disease Epidemiology
Keywords: Cholera, Masasi District Council Mtwara, Miesi, Outbreak
©Vulstan James Shedura et al Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Vulstan James Shedura et al Responding to cholera outbreak in the Mtwara Region, Tanzania: Lessons learned, effective strategies, and scalable recommendations for broader impact. Journal of Interventional Epidemiology and Public Health. 2025;8:19. https://doi.org/10.37432/jieph-d-25-00021
Cholera, caused by Vibrio cholerae, remains a significant public health threat, particularly in sub-Saharan Africa, where outbreaks are recurrent due to inadequate water, sanitation, and hygiene (WASH) infrastructure. In Tanzania, cholera has persisted since its first detection in 1974, with major outbreaks occurring periodically. In 2024, a cholera outbreak emerged in Mtwara Region, specifically in Masasi District Council, necessitating a coordinated emergency response. This perspective provides insights into the outbreak response, highlights key lessons learned, and offers scalable recommendations for broader impact in cholera-prone regions.
Following an alert on June 4, 2024, the Mtwara Regional Public Health Emergency Operations Center (RPHEOC) and the Masasi District Health Management Team (HMT) deployed a Rapid Response Team (RRT) to investigate and contain the outbreak. Field investigations confirmed Vibrio cholerae contamination in water sources and among symptomatic individuals. The outbreak resulted in 47 reported cases and 2 deaths, with a case fatality rate (CFR) of 4.3%. Immediate interventions included enhanced surveillance, case management, and community engagement. WASH measures, such as chlorine water treatment, household hygiene inspections, and distribution of Aqua tabs, were implemented to mitigate further transmission.
Key lessons from the response included the importance of early detection, multisectoral collaboration, and strong community engagement in outbreak containment. The integration of geographic information system (GIS) mapping facilitated targeted interventions, while proactive risk communication enhanced public awareness and compliance with preventive measures.
To improve future outbreak management, we recommend strengthening surveillance systems, expanding WASH infrastructure, and institutionalizing rapid response mechanisms. These strategies, if scaled, could significantly reduce cholera morbidity and mortality in Tanzania and other endemic regions. The Mtwara experience underlines the need for sustainable, community-centered approaches to cholera prevention and control.
Cholera is an acute diarrheal disease caused by the bacterium Vibrio cholerae, primarily transmitted through ingestion of contaminated water or food [1]. Its incubation period ranges from two hours to five days, with only 25% of those infected developing symptoms, and approximately 20% of symptomatic cases progressing to severe disease, which can result in a case fatality rate (CFR) of up to 50% without adequate treatment[1,2]. Cholera outbreaks are often linked to poor water quality, inadequate sanitation, and insufficient hygiene practices. World Health Organization (WHO) recommends maintaining a minimum of 0.2 mg/liter free residual chlorine in safe drinking water, increasing to 5 mg/liter during outbreaks to limit the disease’s spread[3].
Globally, cholera remains a significant public health threat and an indicator of social inequity and underdevelopment. Approximately 1.3 billion people are at risk, with 2.86 million cases and 95,000 deaths annually in endemic countries, primarily in Asia, Africa, Latin America, and the Middle East [4]. Sub-Saharan Africa alone contributes over half of the cases reported to WHO, though these figures may be underestimated due to variations in reporting systems and definitions among member states[5].
In Tanzania, cholera has been a persistent challenge since its first detection in 1974. The country has experienced recurring outbreaks with significant morbidity and mortality. Major outbreaks include the 2006 with 14,297 cases and 254 deaths (Case-Fatality Rate (CFR) of 1.8%) and those between 2015 and 2018 with cumulative 33,421 cases with 542 deaths (CFR of 1.6%) [6,7]. Recently, from September 2023, cholera outbreaks were reported in 13 regions, with cumulative cases reaching 1,521 and 34 deaths (CFR of 2.3%). The regions of Mwanza, Shinyanga, Simiyu, and Kagera remain the most affected, intensified by El Niño-induced heavy rains and overwhelmed sanitation infrastructure[7,8].
Simiyu region, for instance, reported 1,691 cases in 2024, constituting 28.7% of the national burden[9]. Interventions by WHO, including water quality monitoring, sanitation training, and community engagement, have significantly reduced daily new cases from double digits to fewer than seven[2,3,9]. Community-led initiatives, such as those by trained leaders, have also played a critical role in promoting safe water use and hygiene practices [9].
Cholera’s persistence highlights the need for strong health promotion strategies, improved sanitation, and targeted interventions in hotspots. Efforts such as geographic information system (GIS) mapping have been used to identify cholera clusters and guide resource allocation, particularly in resource-limited settings like Tanzania [10]. Effective containment strategies, including isolation and treatment camps, remain critical in managing outbreaks and minimizing transmission [7].
Despite extensive research and ongoing response efforts, there remains a significant gap in documented lessons learned from regional outbreaks, particularly in Mtwara Region located in Southern Tanzania where recent cholera outbreaks have posed unique challenges. Limited published evidence exists on the effectiveness of locally implemented response strategies, the role of community engagement, and the scalability of successful interventions. This perspective aims to bridge this gap by analyzing the cholera response in Mtwara, identifying key lessons, and providing evidence-based, scalable recommendations for broader outbreak management and policy enhancement.
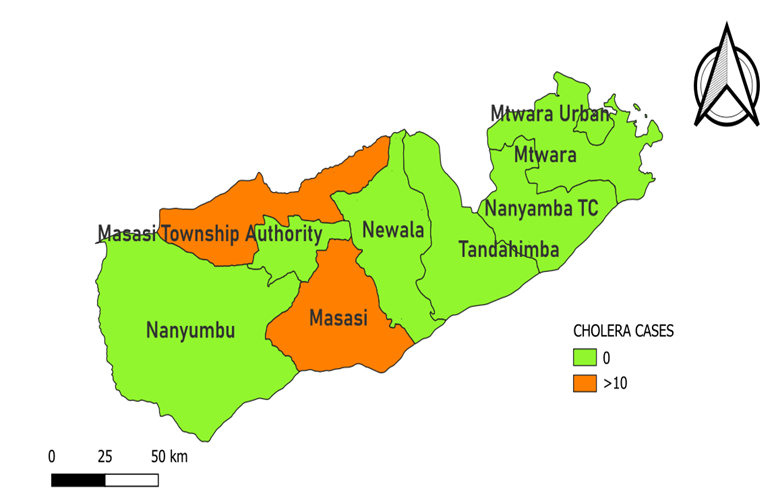
Mtwara Region, located in southern Tanzania, experienced a cholera outbreak confined to Masasi District Council. The outbreak was first reported in Lupaso Ward, specifically in Mbangala Village, within Miesi Hamlet (Figure 1). Masasi District Council is one of seven councils that make up Mtwara Region. According to the 2022 Tanzania National Census, Masasi District had a population of 314,778 [11]. Masasi District is bordered by Nachingwea and Ruangwa Districts to the north, Lindi and Newala Districts to the east, the Ruvuma River to the south, and Nanyumbu District to the west. The outbreak site was characterized by poor sanitation and reliance on untreated river water for drinking and domestic use, contributing to the rapid spread of Vibrio cholerae (Figure 2).
Upon receiving an alert on June 4, 2024, the Mtwara Regional Public Health Emergency Operation Center (RPHEOC), in collaboration with the Health Management Team (HMT) of Masasi District, deployed a Rapid Response Team (RRT). The RRT, consisting of health and water specialists, prepared for field investigations by gathering essential supplies, including rapid diagnostic kits, laboratory materials, and personal protective equipment (PPE). The investigation followed a case-control study design to identify risk factors and transmission patterns.
On June 5, 2024, the RRT conducted an initial site visit, engaging with village leadership and community members to assess the situation. Epidemiological investigations identified contributing factors such as poor sanitation and contaminated water sources. Stool samples were collected from the suspected cases to confirm the cause of the AWD, the samples were transported in Cary-Blair transport media to the St. Benedict’s Ndanda Referral Hospital Laboratory and plated on thiosulfate-citrate-bile salts agar (TCBS). Two hundred (300) milliliters (ml) of water were collected from the Miesi river using sterile bottle and transported to St. Benedict’s Ndanda Referral Hospital Laboratory at <8°C to assess water quality. The water sample was filtered, and the filters placed in petri dishes containing MacConkey agar and Nutrient agar and incubated at 35°C for a period of 24 hours. Colonies were identified based on morphological characteristics and coliforms identified were counted. The resultant colonies were evaluated using biochemical reactions and serotyped using commercial antisera. Colonies were also tested for antimicrobial susceptibility using disk diffusion method. Laboratory results confirmed the presence of Vibrio cholerae in water samples, and one stool sample collected from patients in Miesi Hamlet, and a rapid cholera test confirmed infection in a deceased individual. The bacterium was found to be sensitive to chloramphenicol, doxycycline, and ciprofloxacin. Clinical case definitions were used to classify cases, and an increase in diarrhea and vomiting cases in the community validated the outbreak. The confirmation triggered immediate public health interventions. Based on the investigation, a suspected cholera case was defined as any person presenting with acute watery diarrhea (AWD), abdominal pain, nausea, or vomiting. A confirmed cholera case was any person from whose stool sample Vibrio cholerae was isolated, while a probable cholera case was any suspected case epidemiologically linked to a confirmed case. The confirmation of the outbreak led to the immediate implementation of public health interventions, including enhanced surveillance, community engagement, and water, sanitation, and hygiene (WASH) measures.
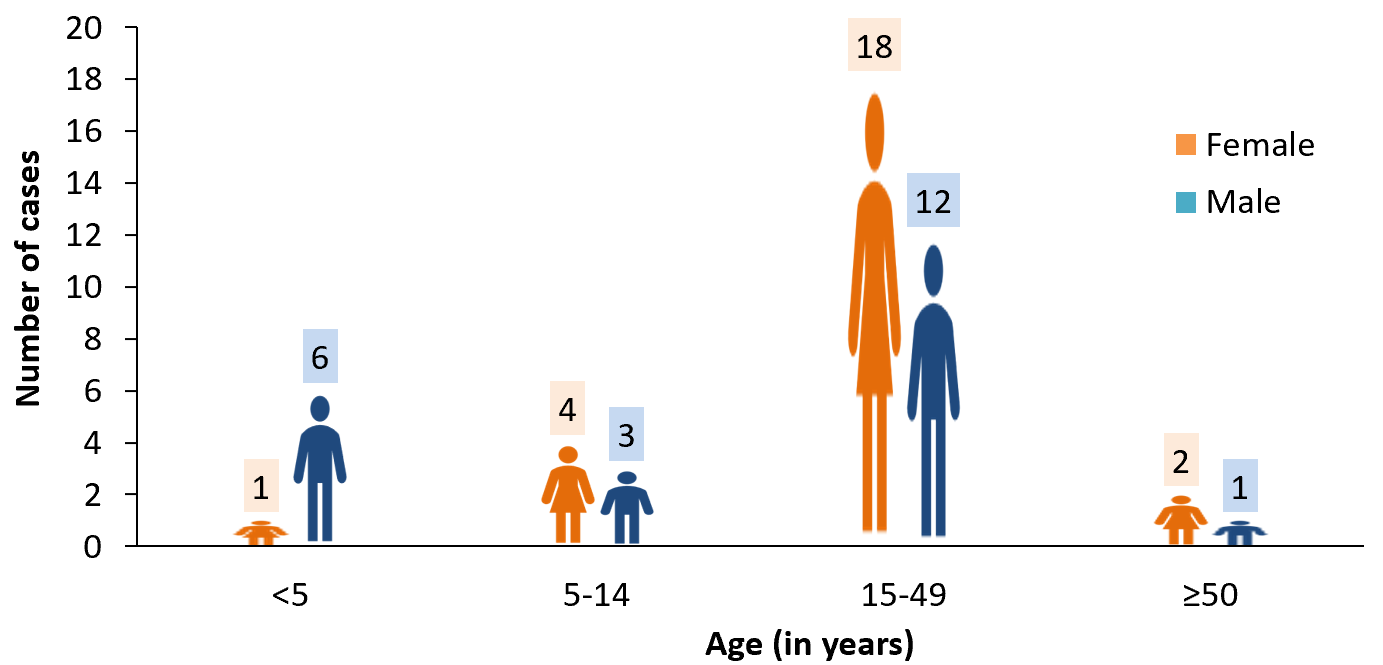
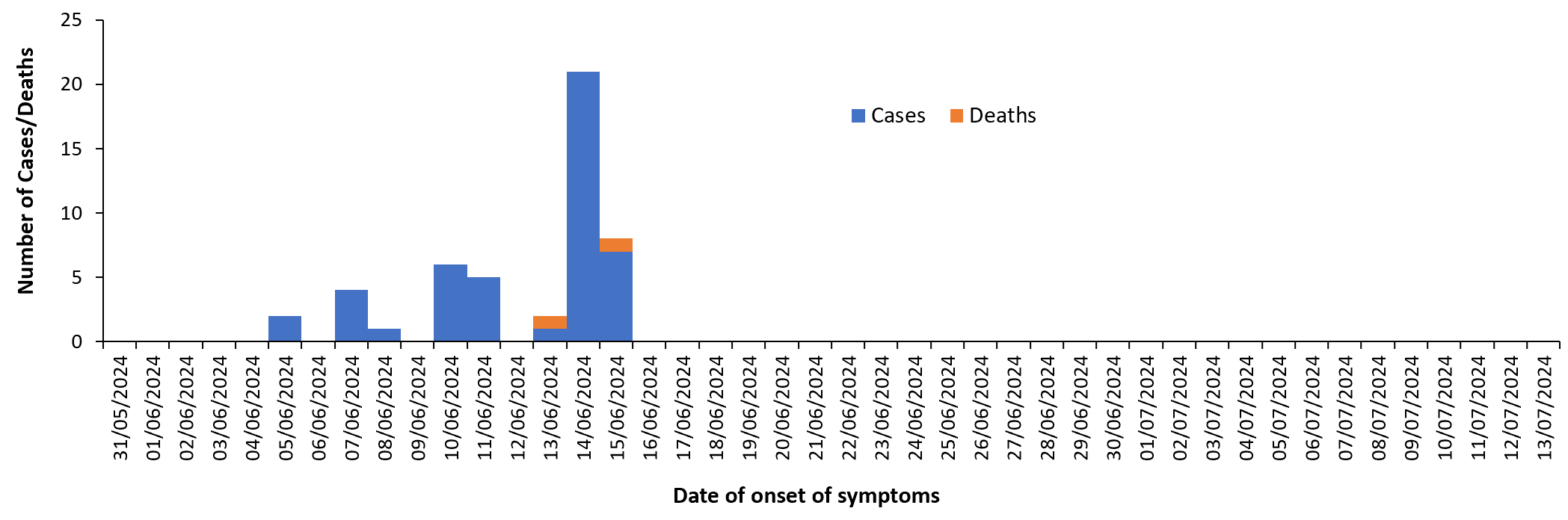
Between June 5 and July 13, 2024, 47 cholera cases and 2 deaths were recorded, resulting in a CFR of 4.3%. Females accounted for 53.2% of cases (25/47), while individuals aged 15 to 49 years were most affected (63.8%, 30/47) (Figure 3). The outbreak remained localized to Miesi Hamlet in Mbangala Village, with no spread to neighboring areas, indicating successful containment efforts. A coordinated response was led by RPHEOC and Masasi District HMT. The response included surveillance, community engagement, case management, logistics support and WASH interventions which involved distributing 15,800 Aqua tabs to 193 households, inspecting hygiene conditions in 307 households, and providing 20,000 liters of clean water to Miesi Hamlet in collaboration with Rural Water Supply and Sanitation Agency (RUWASA). Stakeholders involved included the local government authorities, healthcare providers, and community leaders. The epidemic curve showed an initial peak soon after the outbreak’s onset, followed by a decline due to public health interventions (Figure 4).
Surveillance activities involved active case searches in 111 households and continuous tracking of alerts. Epidemiological data were collected on patient demographics, symptoms, and risk factors. The AWD line lists´ data from the admitting health facilities were updated, consolidated, and cleaned using Microsoft (MS) excel® version 2019; and analyzed using the Microsoft (MS) excel® version 2019 and STATA version 15 package (StataCorp. 2017.. Stata Statistical Software: Release 15. College Station, TX: Stata-Corp L.L.C.). The data were summarized in terms of person, place and time characteristics using means for continuous variables and proportions for categorical variables. The proportion (%) of cases and CFR were calculated. Data analysis focused on trends and case distribution. Daily situation reports were compiled and submitted to the National Public Health Emergency Operations Center and the Ministry of Health.
A dedicated treatment camp was established in Miesi Hamlet, where healthcare workers were trained on cholera management protocols. Utimbe Dispensary supported case management by providing medical supplies and treatment. Psychosocial support was offered to affected individuals. Laboratory capacities were strengthened to ensure timely diagnosis and response. Continuous monitoring involved tracking new cases, assessing intervention outcomes, and ensuring adherence to public health measures. Regular field visits were conducted to evaluate sanitation improvements and water quality. The outbreak was officially declared over on July 14, 2024, following a decline in cases and successful containment measures.
Community engagement efforts reached 633 individuals across 218 households. Health education campaigns emphasized safe water use, handwashing, and proper sanitation (Figure 5 and Figure 6). Local leaders played a critical role in mobilizing communities and reinforcing public health messages (Figure 7). These efforts helped mitigate misinformation and increased compliance with preventive measures.
An AAR meeting was conducted three months post-outbreak, highlighting best practices and challenges. Effective community engagement, rapid response, and WASH interventions were identified as key success factors. Challenges included inadequate funding, limited access to clean water, poor communication networks, and patient reluctance to use the treatment camp. Recommendations included strengthening funding mechanisms, improving water infrastructure, and enhancing surveillance systems. Long-term strategies include strengthening community health education, improving WASH infrastructure, and enhancing disease surveillance. Capacity-building initiatives for healthcare workers and local leaders will ensure sustained outbreak preparedness. Collaboration with stakeholders such as RUWASA will focus on long-term water safety interventions. These measures aim to prevent future cholera outbreaks and enhance regional public health resilience.
This was a public health emergency that required immediate investigation and response, as such, could not go through the formal ethical review process due to time constraints. However, permission to investigate the suspected outbreak was granted by the Ministry of Health, the Mtwara Regional Administration and the Masasi council management. The objectives of the investigations were also explained to the participants and their verbal consent was obtained for the publication of their information including the images.
The cholera outbreak in Mtwara Region presented unique challenges and opportunities for strengthening response mechanisms. The investigation revealed critical factors influencing cholera transmission, including inadequate water sanitation, poor hygiene practices, and delayed community engagement. Effective outbreak response requires a multidisciplinary approach integrating epidemiological surveillance, rapid diagnostics, and public health interventions to curb disease spread and mitigate its impact [1, 4]. One of the major lessons learned from the Mtwara outbreak was the effectiveness of community-led interventions in curbing disease transmission. Trained village leaders and health volunteers played a crucial role in promoting safe water practices, disseminating hygiene education, and coordinating local sanitation efforts. Similar approaches have been successful in other regions, where community participation significantly reduced the burden of waterborne diseases[5,6]. The success of such initiatives underlines the importance of continuous health education and social mobilization to enhance local preparedness and resilience against cholera[7]. Water, Sanitation, and Hygiene (WASH) interventions proved instrumental in controlling the outbreak. The provision of safe drinking water through emergency chlorination efforts, along with infrastructure improvements such as the construction of latrines and handwashing stations, demonstrated immediate benefits in reducing new cases. WHO guidelines emphasize that maintaining a free residual chlorine level of at least 0.2 mg/L in drinking water is essential for cholera prevention, with increased concentrations necessary during outbreaks[3]. This aligns with our findings, as increased chlorination efforts in affected areas contributed to a decline in new cases, reinforcing the importance of WASH investments as a long-term solution [8, 9]
Timely case detection and laboratory confirmation were essential in outbreak management. The deployment of rapid diagnostic tests and laboratory-based culture methods facilitated early identification of Vibrio cholerae, allowing for prompt treatment and contact tracing. Studies have demonstrated that timely laboratory confirmation is critical for implementing targeted interventions and optimizing resource allocation in outbreak settings[10]. Additionally, antimicrobial susceptibility testing provided valuable insights into the effectiveness of treatment options, ensuring appropriate case management and minimizing the risk of antibiotic resistance [11]. The high CFR of 4.3% observed in this outbreak highlights the need for strengthened clinical case management and rapid referral systems. While oral rehydration therapy (ORT) remains the cornerstone of cholera treatment, severe cases require timely administration of intravenous fluids and appropriate antimicrobial therapy. Research has shown that delayed access to treatment facilities is a major contributor to high CFRs in cholera outbreaks[12, 13]. Enhancing healthcare accessibility, ensuring adequate supplies of rehydration solutions, and training frontline health workers in cholera case management are crucial steps in reducing mortality rates [14].
Moreover, the integration of Geographic Information System (GIS) technology in outbreak response enabled precise identification of hotspots and facilitated efficient resource allocation. GIS mapping has been increasingly utilized in public health to monitor disease trends and guide targeted interventions, particularly in resource-limited settings [15]. The implementation of this technology in Mtwara Region provided a valuable framework for outbreak management, supporting data-driven decision-making and improving response efficiency.
Despite the success of these interventions, challenges remain in sustaining cholera control efforts beyond outbreak periods. Strengthening routine surveillance, improving WASH infrastructure, and integrating cholera vaccination into national immunization programs are essential for long-term prevention [1, 16]. The lessons learned from this outbreak provide valuable foundation for future preparedness and response strategies, emphasizing the need for a holistic, evidence-based approach to cholera control in Tanzania and beyond.
The prompt activation of the Rapid Response Team by the Mtwara RPHEOC and the Masasi District Health Management Team was crucial in limiting the outbreak to a single village, demonstrating the effectiveness of early detection and swift intervention. Laboratory confirmation of Vibrio cholerae in stool and water samples emphasized the need for improved water quality monitoring and routine surveillance to prevent future outbreaks. Community sensitization and distribution of water treatment tablets proved essential in reducing transmission, reinforcing the role of grassroots involvement in outbreak control. However, gaps in sanitation infrastructure and reliance on untreated water sources revealed persistent vulnerabilities, showing the need for sustained investment in water supply and sanitation systems. The CFR of 4.3% exceeded the WHO-recommended target of less than 1%, stressing the need for strengthened case management, timely rehydration therapy, and improved referral systems. The cholera outbreak management in the Mtwara region revealed the importance of rapid coordination, community engagement, and strengthening health and WASH systems in any cholera outbreak in the future.
To prevent future outbreaks and enhance outbreak response, a coordinated, multi-sectoral approach is essential. The Ministry of Health, in collaboration with local government authorities and community-based organizations, should scale up health education campaigns in schools, religious institutions, and public gatherings, emphasizing water treatment, sanitation, and hygiene practices. Enforcement of WASH regulations should be strengthened by the National Environment Management Council (NEMC) and municipal authorities to ensure compliance with hygiene and sanitation standards. Sustainable funding and resource mobilization for cholera preparedness should be prioritized by the Ministry of Finance, international donors such as the WHO and UNICEF, and private sector partners to support outbreak response, procurement of essential supplies, and health system strengthening. Infrastructure development, including safe water supply systems and improved sanitation facilities, should be led by the Ministry of Water, with support from development partners like the African Development Bank (AfDB) and the World Bank to enhance long-term access to clean water.
A robust, community-based surveillance system should be implemented by the Ministry of Health and regional health authorities, leveraging digital health technologies such as real-time reporting tools and GIS mapping for rapid outbreak detection and response. Furthermore, integrating oral cholera vaccination (OCV) into routine immunization programs, as recommended by Gavi, the Vaccine Alliance, should be considered to provide short-term protection while long-term WASH interventions are being established.
Future directions should focus on advancing genomic surveillance of Vibrio cholerae, deploying artificial intelligence (AI) for predictive modeling of outbreaks, and enhancing cross-border collaboration for regional epidemic preparedness. By implementing these strategies, Tanzania can strengthen its outbreak response capacity and build resilience against future cholera epidemics.
The cholera outbreak in the Mtwara Region provided critical lessons for strengthening outbreak response and long-term cholera control strategies. First, the rapid activation of the Rapid Response Team (RRT) by the Mtwara RPHEOC and Masasi District Health Management Team played a key role in limiting the outbreak to a single village. This reveals the significance of early detection, intervention, and coordinated response mechanisms in outbreak containment. Second, community-led interventions proved highly effective in limiting cholera transmission. Trained village leaders and health volunteers facilitated the adoption of safe water practices, hygiene education, and local sanitation efforts, demonstrating the value of grassroots involvement in outbreak management. The success of these interventions shows the need for continuous health education and community engagement as a cornerstone of cholera preparedness. Third, WASH interventions, including emergency water chlorination, latrine construction, and handwashing stations, were instrumental in reducing new cases. These findings support the importance of sustained investment in water supply and sanitation infrastructure as a long-term cholera prevention strategy. However, gaps in sanitation and reliance on untreated water sources remain significant challenges that need to be addressed to prevent future outbreaks.
These lessons highlight the need for a multi-sectoral, evidence-based approach to cholera control in Tanzania. Moving forward, prioritizing early response coordination, strengthening community-based interventions, and enhancing WASH infrastructure will be essential for building resilience against future cholera outbreaks in both Tanzania and other resource-limited settings globally.
The authors sincerely appreciate the Ministry of Health, Department of Preventive Services particularly the Epidemiology Section for their invaluable support during the outbreak response and the preparation of this work. We also extend our gratitude to the Mtwara Regional Administration, the Regional Public Health Emergency Operations Center, and the Masasi District Council Health Management Team for their technical and administrative support throughout the cholera outbreak.
Figure 2: An image showing residents of Miesi hamlet in Mbangala Village collecting untreated water from the river for drinking and domestic use.
Figure 5: An image showing a healthcare official conducting community education on safety measures to combat the cholera outbreak for the residents of Miesi Hamlet, Masasi District Council.
Figure 7: Community leaders discussing strategies for managing the cholera outbreak with healthcare officials in Mbangala Village, Masasi District Council.
Views: 6,335
Menu, Tables and Figures
Figure 2: An image showing residents of Miesi hamlet in Mbangala Village collecting untreated water from the river for drinking and domestic use
Figure 3: Distribution of Cholera cases by age in Masasi District Council, Mtwara Region by 13th July 2024.
Figure 4: Epi-curve showing a trend of Cholera cases reported from 5th June 2024 to 13th July 2024 Masasi District Council, Mtwara Region
Figure 5: An image showing a healthcare official conducting community education on safety measures to combat the cholera outbreak for the residents of Miesi Hamlet, Masasi District Council
Figure 6: A healthcare official conducting disinfection at Utimbe Dispensary in Mbangala Village, Masasi District Council
Figure 7: Community leaders discussing strategies for managing the cholera outbreak with healthcare officials in Mbangala Village, Masasi District Council.