Research | Open Access | Volume 8 (2): Article 40 | Published: 05 Jun 2025
Godbless Henry Mfuru1,2,&, Asha Mohamed Gembe3, Khadija Yahya Malima4
1Muhimbili University of Health and Allied Sciences, School of Public Health and Social Sciences, Department of Epidemiology and Biostatistics, Dar es Salaam, Tanzania, 2Tanzania Field Epidemiology and Laboratory Training Program (TFELP), Dar es Salaam, Tanzania, 3Ministry of Health, Non Communicable Diseases section, Dodoma, Tanzania, 4Muhimbili University of Health and Allied Sciences, School of Nursing, Department of Nursing Management, Dar es Salaam, Tanzania
&Corresponding author: Godbless Henry Mfuru, Muhimbili University of Health and Allied Sciences, School of Public Health and Social Sciences, Department of Epidemiology and Biostatistics, Dar es Salaam, Tanzania, Email: mfurugodbless725@gmail.com, ORCID: https://orcid.org/0009-0004-7569-7014
Received: 09 Dec 2024, Accepted: 02 Jun 2025, Published: 05 Jun 2025
Domain: Cancer Epidemiology, Surveillance System Evaluation
Keywords: Cervical cancer, surveillance system, Dodoma
©Godbless Henry Mfuru et al Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Godbless Henry Mfuru et al Evaluation of Dodoma cervical cancer population-based surveillance system in Dodoma, Tanzania, January to December 2022. Journal of Interventional Epidemiology and Public Health. 2025;8:40. https://doi.org/10.37432/jieph-d-24-02029
Introduction: Cervical cancer has been noted as one of the major life-threatening non-communicable diseases globally. It is the fourth most frequent cancer among women, with an estimated 604 000 new cases in 2020. In Tanzania, it’s the leading cause of cancer-related deaths, with an incidence of 625 cases per 1,000,000 women per year. Cervical cancer surveillance is an essential component in cancer control and prevention. However, the performance of this system in Tanzania is not known. We conducted an evaluation to assess the usefulness and performance of the cervical cancer surveillance system in Dodoma to identify areas for improvement.
Methods: We evaluated Dodoma’s population-based cervical cancer surveillance system from January 2022 to December 2022. Using the United States Centre for Disease Control and Prevention guidelines for evaluating public health surveillance systems, eight attributes were assessed. For each attribute, indicators were developed and described using quantitative or qualitative methods. Scores for each indicator were categorised as <60%, 60–79%, and >80% as weak, moderate, and good performance, respectively. Document review and interviews were conducted to collect relevant data on system performance. Data were analyzed by Epi Info 7.
Results: Between January and December 2022, the system recorded 123 cases of cervical cancer. Of these, 76 (62%) were reported by the Makey Pathology Laboratory. Squamous cell carcinoma accounted for 109 cases (89%), and 25 cases (20%) involved patients under 45 years of age. The system performed well on timeliness, acceptability, flexibility, and sensitivity, while it showed moderate performance on data quality and weaker performance in stability. The overall mean score across all eight attributes was 2.4, indicating moderate to good performance.
Conclusion: Overall system performance was satisfactory, with moderate to good performance. Data have been useful in guiding resource allocation and forming strategic guidelines for the prevention of cervical cancer. To strengthen the system further, efforts should focus on improving financial sustainability as well as data quality.
Cancer is one of the major life-threatening non-communicable diseases globally. In 2020, an estimated 10 million people died from cancer, equivalent to one-sixth of all global deaths[1]. Major cancers, including cervical, breast, prostate, and gastrointestinal malignancies, are expected to increase to 22 million new cases each year by 2030 if no interventions are implemented [1]. In this context, effective cancer registration is crucial for tracking disease patterns, guiding resource allocation, and informing evidence-based interventions to control the rising burden.
Cancer registration involves collecting, collating, analyzing, and reporting cancer data. There are three types of cancer registries. The population-based cancer registries (PBCRs) systematically collect information from multiple sources on all reportable cancers within a defined geographic area, forming a core component of a cancer control strategy. Hospital-based cancer registries on the other hand maintain data on all patients diagnosed and/or treated for cancer at a specific facility. Lastly, pathology-based cancer registries record cancer cases diagnosed in pathology laboratories [2].
All WHO member states have approved the Global Monitoring Framework on Non-communicable Diseases (NCDs), which includes a commitment to report on cancer incidence and type as an indicator for the 2025 mortality target [2]. This framework emphasizes the monitoring of NCDs and their determinants, as well as evaluating progress over time at national, regional, and global levels. In line with this activity, the population-based cervical cancer surveillance system in Tanzania will be evaluated.
Worldwide, cervical cancer is the fourth most frequent cancer among women, with an estimated 604,000 new cases in 2020. Of the 342,000 deaths from cervical cancer in 2020, about 90% occurred in low- and middle-income countries [3,4]. In Tanzania, WHO data from 2020 showed that cervical cancer was a leading cause of cancer-related death among women, with an age-standardized incidence rate of 62.5 cases per 100,000 women per year [3]. Current estimates indicate that each year, 10,241 women are diagnosed with cervical cancer and 6,525 die from the disease. In Tanzania, cervical cancer represents the most prevalent malignancy among women overall, as well as among those aged 15 to 44 years [5]. Approximately 16.4 million women aged 15 years and older are at risk of developing cervical cancer in Tanzania [5].
In low- and middle-income countries (LMIC), cervical cancer is often identified in its advanced stages. Limited access to treatment modalities, such as surgery, radiotherapy, and chemotherapy, results in higher mortality rates. Unfortunately, while early detection and effective management make cervical cancer one of the most treatable forms of cancer, challenges remain in these LMIC settings [6].
More than 95% of cervical cancers are attributable to human papillomavirus (HPV) infection, the most common viral infection of the reproductive tract [7,8,9]. Although most sexually active individuals will be infected with HPV at some point—with around 90% of infected women eventually clearing the infection—women living with HIV are six times more likely to develop cervical cancer compared to those without HIV. An estimated 5% of all cervical cancer cases are attributable to HIV [3,6]. Despite most HPV infections and pre-cancerous lesions resolving spontaneously, there is a risk for chronic infection leading to progression to invasive cervical cancer [5,10,11,12]. Additional risk factors include early onset of sexual activity, multiple sexual partners, multiparity, long-term oral contraceptive use, HIV positivity, and cigarette smoking [13–15].
The global strategy toward eliminating cervical cancer as a public health problem, adopted by the World Health Assembly in 2020, recommends a comprehensive approach to prevention and control. The strategy includes primary prevention through HPV vaccination, secondary prevention through screening for women from the general population (from 30 years of age) and for women living with HIV (from 25 years of age), and tertiary prevention involving treatment of invasive cancer [16]. Tanzania has aligned with these international goals through ongoing interventions, including the HPV vaccination program and cervical cancer screening at primary health facilities [17,18]. Furthermore, in collaboration with stakeholders, the country is working to strengthen its cancer registration system [19].
Accurate population data are essential to improve cervical cancer control, screening, and treatment programs in Tanzania. Routine data collection is paramount for identifying needs, planning interventions, allocating resources, and evaluating the overall effectiveness of cancer prevention and treatment initiatives.
Since its inception, the Dodoma population-based cervical cancer registry has not been evaluated. This assessment aims to evaluate the usefulness and attributes of the cervical cancer surveillance system in Dodoma from January to December 2022 and to provide recommendations for its improvement based on the findings.
Study design
The study utilizes a descriptive cross-sectional design to evaluate the existing cervical cancer surveillance system in Dodoma.
Study area and period of data collection
The evaluation was conducted in the Dodoma region from 27 February to 3rd March 2023. Located in Central Tanzania, it is one of 31 administrative regions. According to the 2022 national census, the region had a population of 3,085,625, with 1,572,865 of them female [20]. The Dodoma population-based cervical cancer surveillance system was founded in 2018, as a population-based cancer registry. The registry supports early detection, case reporting, and data collection on cervical cancer incidence within its catchment area. This evaluation was conducted using the United States Centers for Disease Control and Prevention Updated Guidelines for Evaluating Public Health Surveillance System [21].
System attributes evaluated
The performance of the system was evaluated using these eight surveillance attributes: (i) data quality and completeness for key variables, (ii) timeliness, (iii) representativeness, (iv) flexibility, (v) simplicity, (vi) acceptability, (vii) stability and (viii) usefulness. For each attribute, specific indicators were developed and described using either quantitative or qualitative methods.
Data collection
Interviews were conducted at the National and health facility levels. At the national level, the coordinator of Cancer from the NCD unit and RCH programme under the Ministry of Health was interviewed. At the facility level, clinicians, nurses and medical records personnel dealing with cervical cancer were interviewed. Two different questionnaires were developed: one used at the National level and the other at the health facility level. These interviews were conducted using semi-structured questionnaires.
Data review (cancer registry) was conducted from January 2022 to December 2022 in Dodoma Population Based Cancer Registry (PBCR) to check for consistency of data reported to the Ministry of Health, as well as computing timeliness, completeness and quality of data.
Documents review included WHO cervical cancer annual reports, National annual reports on cervical cancer, facility-based cancer registry, Tanzania National Strategic Plan for the Control and Prevention of Cervical Cancer and Tanzania Treatment Guideline (STG).
Throughout the whole course of the evaluation process, the US Centres for Disease Control and Prevention (CDC) updated guidelines for evaluating the public health surveillance system [22] were utilized.
Data Analysis
Data collected was analyzed using MS Excel and Epi info version 7.2. A scale from 1 to 3 was used to provide a score for each quantitative indicator as follows: < 60% scored 1 (weak performance); 60–79% scored 2 (moderate performance); ≥80% scored 3 (good performance. The scale was adopted from other studies used to evaluate surveillance systems elsewhere in Africa [18].
Usefulness: The usefulness of the surveillance system was assessed by reviewing its impact on public health actions and policy decisions.
Representativeness: The representativeness of the surveillance system was assessed by examining the demographic and clinical characteristics of the cases reported from January to December 2022. The data were analyzed to determine the proportion of cases by age, tumor type (squamous cell carcinoma vs. adenocarcinoma), and the location of reporting sites.
Timeliness: Timeliness was evaluated in two main areas:
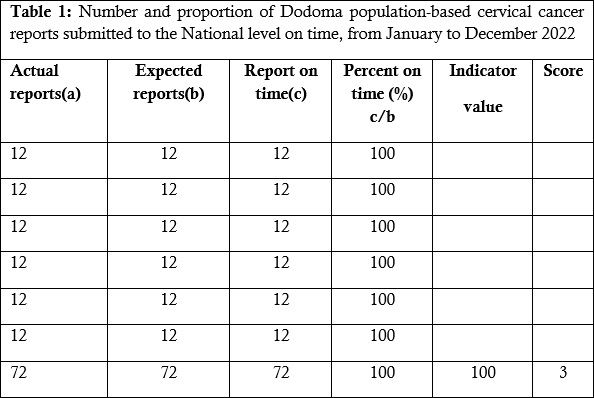
Submission of Reports: The timeliness of report submission was determined by comparing the number of actual reports submitted to the expected reports from each facility between January and December 2022. Each facility is required to send one report by the 4th of each month. The percentage of reports submitted on time was calculated for each facility.
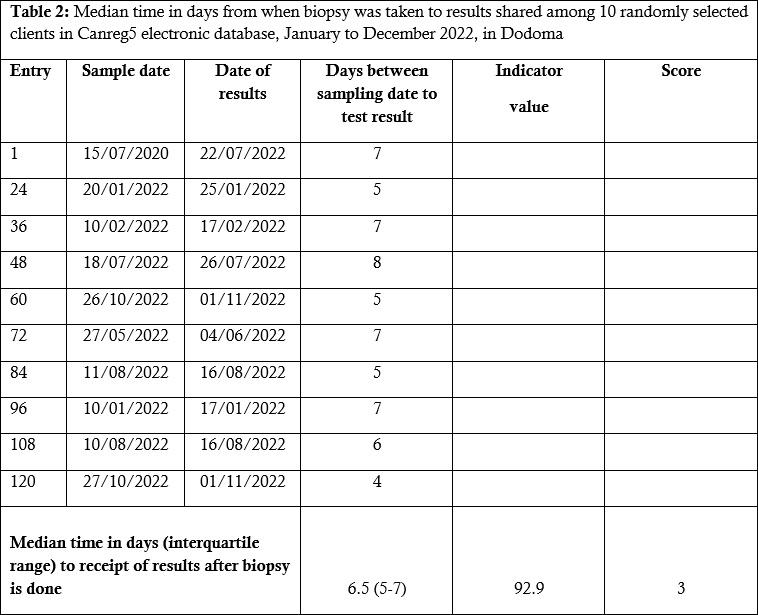
Time from Biopsy to Results: A random sample of 10 entries from the Canreg5 database was selected to calculate the median time from the date of biopsy to the date of results. The time difference in days between the biopsy date and the result date was computed to assess the speed of reporting.
Data Quality: Data quality was assessed by reviewing the completeness and accuracy of key data fields. Ten entries were randomly selected from the Canreg5 database to assess the completeness of critical variables such as patient ID, address, age, date of birth, type of tumour, morphology, stage, and type of treatment. Completeness was calculated as the percentage of required fields (32 key variables) filled in the registry forms. The data were also reviewed to ensure they met international standards for comparability, including TNM and ICD coding systems. Data Accuracy Assessment was evaluated by cross-checking records with source documents (that is, medical files and laboratory reports) to ensure consistency and correctness of recorded data.
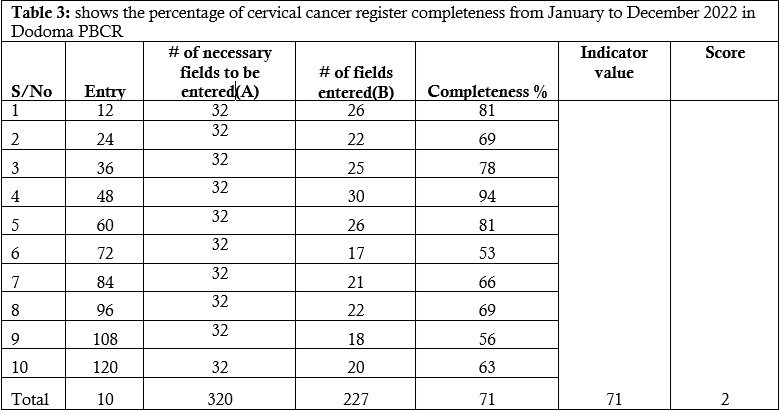
Completeness: Completeness was evaluated by verifying the number of required data fields entered into the Canreg5 electronic database. Ten entries (cases) were randomly selected, and the number of fields entered was compared against the total number of necessary fields (320 fields in total). The overall completeness was calculated by dividing the number of fields filled by the number required, expressed as a percentage.
Validity: Validity was assessed by determining the proportion of cases that were morphologically confirmed, as all cases (n=123) captured by the system were reviewed for confirmation. The assessment also involved verifying that data were collected using international standards for cancer registration (TNM stages and ICD coding).
Comparability: Comparability was assessed by ensuring that the data collected adhered to international standards, such as the TNM staging and ICD coding systems for oncology. The information collected, including tumour topography, morphology, behaviour, and grade, was reviewed to ensure that it met the requirements for international comparability.
Stability: Stability was assessed by examining the financial and operational support of the surveillance system. The assessment included reviewing the total amount of funding received from various sources, such as the Government of Tanzania, individual voluntary contributions, and external partners (Vital Strategies and AFCRN). Additionally, the frequency of shortages of data collection forms and tools was examined to determine the system’s operational stability.
Simplicity: Simplicity was evaluated by assessing the ease of data collection, entry, and processing. The assessment included a review of the structure and content of the data collection forms, the average time required to fill out the forms (less than 20 minutes), and the time needed for data entry into the Canreg5 electronic database (less than 10 minutes). The need for training and the number of staff required to operate the system were also considered.
Flexibility: Flexibility was assessed by examining the system’s ability to adapt to changes over time, including updates and revisions to data collection tools, modifications to the Canreg5 database, and integration with other health information systems such as DHIS2. The integration of other types of cancer (e.g., breast, prostate, and oesophageal cancers) into the surveillance system was also considered.
Acceptability: Acceptability was assessed by evaluating the satisfaction of participants with the monthly reporting process. This included analyzing responses from participants regarding their satisfaction with the reporting process and the percentage of reports submitted on time. Additionally, the level of training provided to participants and their perceived ease of use of the system were considered.
Sensitivity and Predictive Value Positive (PVP): Sensitivity and PVP were not calculated because the system captures only confirmed cases of cervical cancer, and data on those tested but found negative were not available
Data Collection Techniques, Tools and Data Sources
Data Collection Techniques: We evaluated data collection techniques by reviewing patient medical files, cancer registry forms, and pathology reports used in the system. The assessment included randomly selecting 10 registry entries, each containing 32 key data variables, to measure completeness and accuracy. Interviews were also conducted at national and health facility levels with key personnel involved in cancer data collection.
Data Collection Tools: We used a semi-structured questionnaire along with registry forms as a data collection tool.
Data Sources: The evaluation reviewed data sources by verifying whether the system captured all relevant cervical cancer cases. The main sources for this assessment included:
Surveillance System Description
Case Definition: All women aged 15 years and above in Dodoma presenting with post-menopausal vaginal bleeding, abnormal discharge, dyspareunia, or any symptoms leading a healthcare provider to suspect cervical cancer, confirmed by histological diagnosis, are included in the surveillance system.
Population under Surveillance: All women aged 15 years and above in the Dodoma region are under surveillance[5].
Flow of information: Information flow starts with an individual passively visiting a health facility. Healthcare providers will take a detailed clinical history and physical examination. If the case fits the case definition confirmatory investigation will be ordered (biopsy) and the results are kept in patient files or in the electronic database of the respective health facility. The cervical cancer registrar then collects all confirmed cases information and uploads them into Canreg5 electronic database.
This information is then transmitted electronically to MoH as well as Monitoring and Evaluation section. MOH is responsible for sharing this information with WHO upon request and with respect to country information sharing regulations (Figure 1).
Purpose and Objective of the System
Data extraction
Data is obtained from patient medical files who are confirmed to have cervical cancer by using cancer registry forms, from participating health facilities, including two pathology laboratories.
Data Storage
Confidentiality of patient identifying information and related medical data is strictly maintained at each cancer registry, where only authorized individuals with passwords have access. External individuals will need permission from the Permanent Secretary at MOH to access patient information from the electronic database. At the data source, patient files are kept in locked drawers.
Data analysis and presentation
Data collected through this surveillance system is analyzed at the facility and national levels. The presentation of data is done in the form of notes, tables, graphs, and reports, depending on the needs and the targeted audience.
Resources needed to operate the system
Funding sources: The system is funded by Vital Strategies, the Global Fund, and the Tanzanian government, which also provides a good working environment, staff, and infrastructure.
Personnel: Key personnel include facility-level healthcare providers (clinicians, nurses, oncologists, gynaecologists, and pathologists), a coordinator from the Reproductive and Child Health (RCH) programme, the NCD unit coordinator, and a Monitoring and Evaluation officer from the Department of Policy and Planning (DPP).
Materials and Resources: Necessary resources include financial support, infrastructure (offices, pathology labs), stationery, computer equipment, utilities (electric power, internet), and cancer registry forms.
Data sharing
De-identified participants data will be made available to others upon reasonable request. Access will be granted after the approval of a proposal, and a signed data access agreement.
Ethical Considerations
Permission to conduct this evaluation was obtained from the Ministry of Health through the non-communicable disease section. No patient identification data were collected.
The questionnaires were completed by 33/33 (100%) and 2/2 (100.0%) personnel involved in cervical cancer surveillance at the facility and at the National level, respectively.
The usefulness of a surveillance system
The cervical cancer population-based surveillance system in Dodoma was instrumental for the MoH in tracking cervical cancer cases. Data from this system led to the establishment of a National Cancer Coordination Unit under the NCD section. Combined with data from other regions, it informed the National Strategic Plan for the Prevention and Control of Cervical Cancer (2013-2022). Additionally, the MoH’s plan to build a cancer centre in Tanzania was driven by data showing an increasing cancer burden. Additionally, based on gaps identified in the data captured by the system, the Ministry of Health plans to train cancer registrars and healthcare providers on cancer staging.
Representativeness
The representativeness of the cervical cancer surveillance system in Dodoma from January to December 2022 was assessed using two indicators: geographical coverage and characteristics of reported cases. For geographical coverage, all 123 reported cases originated from only five facilities located in Dodoma Municipal, with no participation from the remaining six districts, indicating limited coverage and potential underreporting from rural areas; this indicator was therefore assigned a score of 1. For characteristics of reported cases, the majority (88.6%) were squamous cell carcinoma and 11.4% were adenocarcinoma, consistent with the expected histologic distribution. Despite missing data on tumour staging (93.5%), the case profiles were generally aligned with national trends, and this indicator was assigned a score of 3. The mean score for representativeness based on these two indicators was thus calculated as 2.
Timeliness
Timeliness was evaluated in two areas: first, regarding the submission of reports and time from biopsy to result. All facilities assessed achieved a 100% report submission rate in 2022. This indicator was assigned a performance score of 3 (Good) (Table 1). The median time from biopsy to results was 6.5 days, with an interquartile range (IQR) of 5 to 7 days. This corresponds to 91.9% of the expected 7-day standard and was also assigned a performance score of 3 (Good) (Table 2).
Data quality
Completeness: The overall completeness of the cervical cancer registry in Dodoma PBCR for January to December 2022 was 71% and was scored 2, which corresponds to moderate performance (Table 3).
Staging: Also, in the Canreg5 database, the stage of cervical cancer was missing for 115 cases, which accounts for 93.5% of the total entries. This was assigned a performance score of 1.
Validity: All cases n=123 (100%) captured by the system were morphologically confirmed, scoring 3, which means good performance.
Comparability: Information collected was found to follow international classification and standards of tumour registration (TNM stages and ICD 0 coding system- International classification of diseases for oncology) and all entries complied with these standards. Information on topography, morphology, behaviour and grade of cancer were collected which are international requirements for comparability. This indicator was assigned a score of 3 which corresponds to good performance.
Simplicity
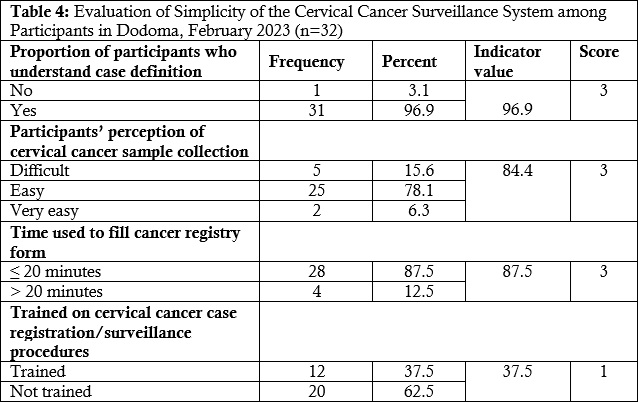
A high proportion of participants (96.9%, 31/32) understood the cervical cancer case definition, and the majority (84.4%, 27/32) found the sample collection process to be easy or very easy. Most participants (87.5%) were able to complete the cancer registry form within 20 minutes, indicating the system’s simplicity in data entry. However, only 37.5% of participants had received training on cervical cancer case registration and surveillance procedures (Table 4).
Stability
The Stability was assessed using three indicators: source of funding, amount of funding, and availability of data collection tools. Funding came from four sources: the Government of Tanzania (33%), individual voluntary contributions (46%), Vital Strategies (18%), and the African Cancer Registry Network (AFCRN) (3%). While multiple funding streams were present, the limited share from government sources impacted the long-term sustainability of the system. This indicator was assigned a performance score of 1. The total operating cost was $28,000, of which only $9,300 (33%) came from the government. The remaining 67% was sourced from less predictable, short-term contributions, reflecting financial vulnerability. This indicator was assigned a performance score of 1. Regarding operational stability, 75% (24/32) of respondents reported no shortages of cancer data collection tools, while 25% (8/32) experienced shortages two to three times during the year. This inconsistency affected the reliability of data collection and resulted in a performance score of 1. The average performance score for Stability was 1, indicating poor stability of the surveillance system (Table 5)
Flexibility
The system demonstrated flexibility by adapting to numerous updates and revisions without disruption. All data collection tools and the Canreg5 database were updated regularly to ensure the collection of relevant information. The Ministry of Health (MOH) and its partner, Vital Strategies, collaborated to implement these changes. Additionally, the system expanded to include other cancer types, such as breast, prostate, and oesophageal cancer, and efforts are underway to integrate it with the DHIS2 platform. Based on these indicators, the system scored 3 for both the number of changes adopted and system integration, resulting in an overall flexibility score of 3 (good performance).
Acceptability
The surveillance system showed good acceptability among stakeholders. All required monthly reports were submitted on time from January to December 2022, and all facilities consistently adhered to the monthly reporting schedule, indicating strong participation and willingness to engage with the system. Additionally, despite some participants not having received formal training, the majority—23 out of 32 (71.9%)—expressed satisfaction with the reporting process. Based on these indicators, the system scored 3 for timeliness of data reporting, 3 for reporting rate, and 3 for participant satisfaction. The overall score for acceptability was therefore 3, indicating good performance.
Sensitivity and Predictive value positive (PVP)
All the reported cases were morphologically confirmed. However, sensitivity and PVP were not calculated since the system captures only those who have the diseases and the information of those who were tested and had negative results was not found. Based on the 100% morphological confirmation, we assigned a score of 3, implying good sensitivity.
Summary of results
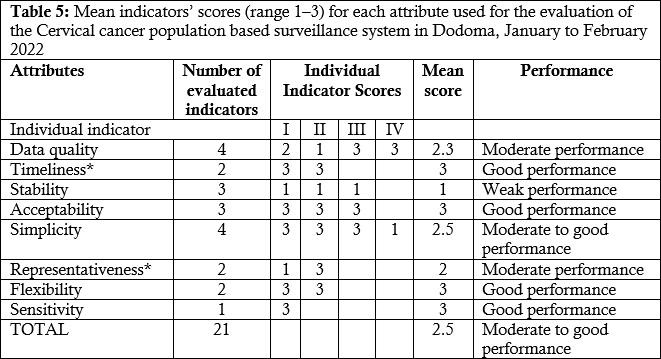
We summarized the mean scores (ranging from 1 to 3) for each attribute assessed to obtain the average performance score of the surveillance system. The cervical cancer surveillance system in Dodoma (January–February 2022) scored an average of 2.4, reflecting moderate to good performance, with good performance in timeliness, simplicity, flexibility, and sensitivity, while data quality and stability scored lower, indicating moderate and weaker performance, respectively (Table 5).
The cervical cancer population-based surveillance system in Dodoma has shown its potential to provide essential data for national cancer control efforts, including contributing to the establishment of the National Cancer Coordination Unit and influencing the creation of the National Strategic Plan for the Prevention and Control of Cervical Cancer. The system’s value is evident in its ability to generate crucial data on cervical cancer incidence, which has supported the Ministry of Health’s plans for expanding cancer care facilities, including the proposed 10 Cancer Excellence Centers. However, the current system is limited in its representativeness, as it only captures data from Dodoma City and excludes six surrounding districts. This limitation could impact the generalizability of the findings to the entire region, a challenge commonly faced by similar population-based cancer registries [23].
Despite this, the system’s overall performance remains noteworthy when compared to other cancer registries in low-resource settings. For instance, a study in Uganda’s cancer registry reported challenges related to data completeness and resource constraints, similar to what is observed in Dodoma [24]. While the Dodoma system captures essential data and operates with a simple one-page form, the lack of critical parameters, such as risk factors, and the inability to distinguish between new and recurrent cases, reflect similar gaps identified in registries elsewhere [23]. This highlights the need for further refinement in data collection tools to improve the registry’s effectiveness in guiding clinical interventions and public health initiatives.
The flexibility of the Dodoma system, which allows for the integration of other cancer types, offers an advantage over standalone registries in other regions. For example, registries in sub-Saharan Africa often require separate systems for different cancer types, leading to duplicated efforts and higher operational costs[25,26]. The integration with DHIS2 in Dodoma could be a significant step towards streamlining data collection processes and improving accessibility, mirroring successful models in countries like Rwanda, where integration into national health information systems has improved data use and decision-making [27,28].
However, data completeness remains a critical issue. In comparison with the more robust registries in high-income countries, where comprehensive training and continuous support mechanisms are in place, the Dodoma system’s challenges with incomplete data and underreporting reflect broader systemic weaknesses in resource-limited settings [29]. These challenges are compounded by insufficient training, lack of supportive supervision, and the need for more standardized data collection protocols. Addressing these gaps through increased training, regular mentorship, and improved resource allocation could elevate the quality of the data collected, aligning the Dodoma system more closely with international standards for cancer registries.
All things considered, the Dodoma cervical cancer population-based surveillance system shows considerable potential in supporting Tanzania’s cancer control efforts. It provides valuable data that has already contributed to the establishment of the National Cancer Coordination Unit and the formulation of the national strategic plan for cervical cancer prevention. However, expanding its coverage to include more districts and improving data quality through enhanced training and supervision will further strengthen its impact. While the system is effective in many respects, its current limitations, such as incomplete data and reliance on a small coverage area, need to be addressed to maximize its utility. By leveraging international best practices and adapting lessons learned from this evaluation and other successful cancer registries, the system can play a pivotal role in advancing cancer surveillance and prevention across the country.
Limitation
Although this evaluation was conducted in only one cancer registry, which may limit the generalizability of the findings, it represents the first of its kind in Tanzania. As such, it provides a valuable baseline assessment to inform system improvements and guide future evaluations in other registries nationwide.
Overall system performance was satisfactory, with moderate to good performance. Data have been useful in guiding resource allocation and forming strategic guidelines for the prevention of cervical cancer. To strengthen the system further, efforts should focus on improving financial sustainability as well as data quality.
RECOMMENDATION
What is already known about the topic
Before this evaluation, it was known that cervical cancer is a significant public health issue in Tanzania.
The need for an effective surveillance system to monitor the incidence of cervical cancer was acknowledged, but there was little information on how well the system functioned.
What this study adds
This study provides the first comprehensive evaluation of the cervical cancer surveillance system in Dodoma, identifying specific gaps in data quality, detection, and reporting.
It offers actionable insights and recommendations for strengthening surveillance efforts, setting a foundation for future improvements and evaluations.
Godbless Henry Mfuru and Khadija Yahya Malima conceptualized the study, developed the methodology, curated the data and performed the formal analysis. Khadija Yahya Malima supervised the study. Asha Mohamed Gembe and Khadija Yahya Malima validated the data. The original manuscript was prepared by Godbless Henry Mfuru and Khadija Yahya Malima, with both authors contributing to the review and editing process. Both Godbless Henry Mfuru and Khadija Yahya Malima had full access to all the data in the study, both participated equally in this study and had final responsibility for the decision to submit for publication.
The successful completion of this study was made possible through the collaborative efforts of members from Muhimbili University of Health and Allied Sciences, the Ministry of Health, the Tanzania Field Epidemiology and Laboratory Training Program (TFELTP), the Centers for Disease Control and Prevention (CDC) through Mzumbe University.

Views: 3,023
Menu, Tables and Figures
Table 1: Number and proportion of Dodoma population-based cervical cancer reports submitted to the National level on time, from January to December 2022
Table 2: Median time in days from when biopsy was taken to results shared among 10 randomly selected clients in Canreg5 electronic database, January to December 2022, in Dodoma
Table 3: shows the percentage of cervical cancer register completeness from January to December 2022 in Dodoma PBCR
Table 4: Evaluation of Simplicity of the Cervical Cancer Surveillance System among Participants in Dodoma, February 2023 (n=32)
Table 5: Mean indicators’ scores (range 1–3) for each attribute used for the evaluation of the Cervical cancer population based surveillance system in Dodoma, January to February 2022