Perspective | Open Access | Volume 8 (2): Article 44 | Published: 25 Jun 2025
Samuel Onyinyechukwu Azubuike1,&
1Department of Public Health, Faculty of Health Sciences, National Open University of Nigeria
&Corresponding author: Samuel Onyinyechukwu Azubuike, Department of Public Health, Faculty of Health Sciences, National Open University of Nigeria, Email: samonaz2000@yahoo.com, sazubuike@noun.edu.ng
Received: 09 Dec 2024, Accepted: 25 Jun 2025, Published: 25 Jun 2025
Domain: Communicable and Non-Communicable Disease Epidemiology, Public Health
Keywords: COVID-19, Sub-Saharan Africa, Non-communicable diseases, Communicable diseases, Prevention
©Samuel Onyinyechukwu Azubuike et al Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Samuel Onyinyechukwu Azubuike et al COVID-19 pandemic experience in sub-Saharan Africa: the need to narrow the dichotomy between communicable and non-communicable diseases prevention. Journal of Interventional Epidemiology and Public Health. 2025;8:44. https://doi.org/10.37432/jieph-d-24-02028
Existing evidence suggests that pre-existing non-communicable diseases (NCDs) contributed significantly to the morbidity and mortality associated with COVID-19 infection in Africa. This underscores how the growing burden of communicable diseases in Africa could be complicated by the increasing burden of NCDs in the region. On the other hand, there are suggestions that the direct and indirect effects of communicable diseases such as COVID-19 infection could also complicate the existing burden of NCDs on the continent through their potential biological or socioeconomic disruptions. The available data on the COVID-19 pandemic experience in Africa suggests the need to re-evaluate the traditional dichotomy between communicable and non-communicable diseases’ preventive strategies in the region with the aim of adopting a more integrated approach where necessary. Policy frameworks aimed at preventing communicable diseases or managing large-scale outbreaks must account for their potential interplay with NCDs. Such an approach would facilitate coordinated efforts, foster partnerships, and enable the efficient mobilization of existing human and material resources toward the mutual prevention and management of both communicable and non-communicable diseases
Introduction
Available data shows that more than 500 million cases of confirmed COVID-19 infections and above 6 million deaths were recorded globally by the beginning of June 2022. Of these figures, 1.7% of the cases and a disproportionate 2.4% of deaths occurred in Africa, while 41.9% cases and only 3.4% deaths occurred in Europe [1]. Although the pandemic has declined, it is necessary to understand the drivers of morbidity and mortality in the region for the purpose of the ongoing and future control programmes. The understanding of the drivers of morbidity and mortality associated with COVID-19 in the continent has evolved overtime. While the role of some factors implicated seems not to be very clear, that of others seem to be well established. For example, the role of extreme poverty and the overcrowded nature of African households on the occurrence and severity of the disease in the region remains a paradox, although emerging evidence suggests that they increase the risk of dying [2-4]
There is now sufficient data to suggest that pre-existing NCDs contributed to the severity of the infection in sub-Saharan Africa (SSA). For example, data from South Africa showed that 61% and 52% of the hospitalised COVID-19 patients had hypertension and diabetes respectively[5]. In the Democratic Republic of Congo, patients with NCDs comprised about 85% of all deaths[5] while in south west, Nigeria, cancer patients were 12 times more likely to die of COVID-19 infection (than non-cancer patients)[6]. In addition, the presence of diabetes, hypertension and renal diseases were noted as the commonest predictors of death in the Nigerian study[6]. Notably, the prevalence of pre-existing conditions such as cardiovascular diseases, cancer, and diabetes tends to increase with age. This suggests that these conditions may have complicated the increased risk of the COVID-19 among the older population. Incidentally, the elderly population of Africa is on the increase despite the population being predominantly young with the elderly (above 60 years) predicted to increase from 35 million in 2005 to 67 million by 2025 and 163 million by 2050 ( an estimated 218% increase between 2019-2050 has been projected [7-9]. The COVID-19 pandemic has, therefore, re-emphasised the potential dangers NCDs pose to the health and well-being of the continent presently and in the future. It could superimpose on the outbreak of communicable diseases as seen during the COVID-19 pandemic to wreak havoc on the population’s health and socioeconomic well-being. It is against this backdrop that this paper aims to highlight the impact of the burden of NCDs on the burden of COVID-19 infection in Africa (especially the sub-Saharan region) and vice versa, and the need to narrow the dichotomy between communicable and noncommunicable disease prevention, where necessary, in the region.
The paper was based on an analysis of COVID-19 and noncommunicable disease data extracted from the World Health Organisation website and other relevant publications available online. These data and information were critically reviewed, integrated, and appropriate conclusions were drawn, taking into consideration their epidemiological implications and potential relationships.
Non-communicable disease prevalence in Africa and its potential impact on the burden of COVID-19 in the region.
The burden of NCDs is on the rise in Africa, especially in SSA. A recent study showed an increase of 67% between 1990 (90·6 million DALYs (95% UI 81·0–101·9) and 2017 (151·3 million DALYs (133·4–171·8)[10]. It is worrisome that while the burden of NCDs showed a rapid increase, that of communicable, maternal, neonatal and nutritional diseases declined, with age-standardised NCDs (measured in DALY) closely trailing that of communicable diseases in SSA [10]. Similarly, WHO has observed that the age-standardised mortality rate of cancer in Africa is among the highest in the world ( > 650 per 100,000 compared to 438 per 100,000 in the WHO Region of the Americas)[11]. Besides, the risk of dying from the NCDs in Africa for both men and women aged between 30-70 years ( 20.6%) is higher than the global average (18%)[12]. The NCD burden in Africa is accounted for to a large extent by cardiovascular disease (17·9 million deaths annually)[13, 14] cancers (9·0 million), diabetes[(1·6 million)[14-1)] respiratory diseases(3·9 million )[13, 14] chronic kidney diseases[17], and mental health disorder[18], with the first three accounting for most cases.
Evidence from the COVID-19 pandemic showed that in spite of the low COVID-19 mortality rate in Africa compared to North America and Europe, the continent had the highest mortality rate among critically ill patients [19]. Although this could, in part, be attributed to other factors such as high prevalence of HIV/AIDS (especially in South Africa), the emergence of a more virulent strain, shortage and underutilisation of critical care resources (mechanical ventilator, oxygen supplies), lack of specialised staff to provide critical care treatment; the prevalence of NCDs among critically ill patents was undoubtedly a significant determinant of morbidity and mortality [19-22].
Moreover, the fact that the burden of some of these NCDs such as CVDs, diabetes and hypertension tend to be higher in younger age groups in SSA compared to the rest of the world (due to their early onset and possibly population structure)[23-25] suggests that communicable diseases like COVID-19 whose impact was aggravated by NCDs could take a higher toll on younger age group in SSA compared to the observations in high income countries. For instance, preliminary data suggested that while the higher proportion of COVID-19 cases among African men (63%) occurred among those aged 31-49 years, a greater proportion of cases among men in Europe was observed among those > 55 years of age[26, 27]. A similar observation was made in a Congolese study (mean age of 48 years compared to 54 years in the USA)[22]. The synergistic effect of NCDs and communicable diseases like COVID-19 could therefore have a negative implication for the socioeconomic well-being of families and countries in Africa, considering the age groups affected.
Notably, there is evidence that just as poverty and low socioeconomic status increase vulnerability to NCDs in low- and middle-income countries, NCDs also elevate the risk of becoming poor[28]. Incidentally, poverty remains the strongest driver of communicable disease prevalence across the globe, especially in SSA. Evidence of higher COVID-19-related mortality among low-income (compared with high income) communities in urban centres has been reported in South Africa and other parts of the world[29, 30]. It is, therefore, obvious that tackling NCDs and the socioeconomic variables associated with its prevalence in the region could invariably reduce the burden associated with outbreaks and prevalence of communicable diseases in the region. Hence, the prevalence of NCDs in the region should be taken into consideration when discussing the potential threat communicable disease outbreaks or pandemics such as COVID-19 pose to the health of the region. The pandemic should, therefore, provide an opportunity for increased awareness and the need for action (with respect to NCDS) given the direct and indirect threat it poses to the health and well-being of the continent.
Communicable diseases as a potential predisposing factor to NCDs and their severity in sub-Saharan Africa: Insights from the COVID-19 Pandemic
The COVID-19 pandemic has highlighted potential pathways through which communicable diseases could exacerbate existing NCD burden in the region or trigger new ones. For example, it has been suggested that COVID-19 has the potential to disrupt normal biological mechanisms in the body with potential adverse effects on NCDs [ 31]. The potential pathological relationship between COVID-19 infection and NCDs has been hypothesised to be mediated through the angiotensin converting enzyme 2 (ACE2) pathway, which provides an access door for SARS-COV-2 to enter human cells[32,33]. This enzyme is expressed in the heart, lungs, pancreatic cells, kidneys, liver and other organs[33, 34]. Through this pathway, the virus has been shown to be associated with multiple direct and indirect cardiovascular complications such as myocardial ischaemia, acute myocardial injury, myocarditis, cardiac arrhythmias, and venous thromboembolism[35]. For example, elevated troponin levels (associated with heart attack) or cardiac arrest were observed in 12% of COVID-19 patients without a history of CVD in China[35]. Moreover, insulin resistance, impaired insulin secretion, acute hyperglycaemia, pancreatic cell damage (which produces insulin needed for sugar metabolism), and beta cell autoimmunity (autoimmune diabetes) have also been associated with the infection[36,37]. There were also suggestions that it could lead to long-term lung damage, including pulmonary fibrosis. Although these were acute events, the potential long-term effects and implications for NCD incidence among patients, especially those who experienced long COVID in the region, deserve further investigation.
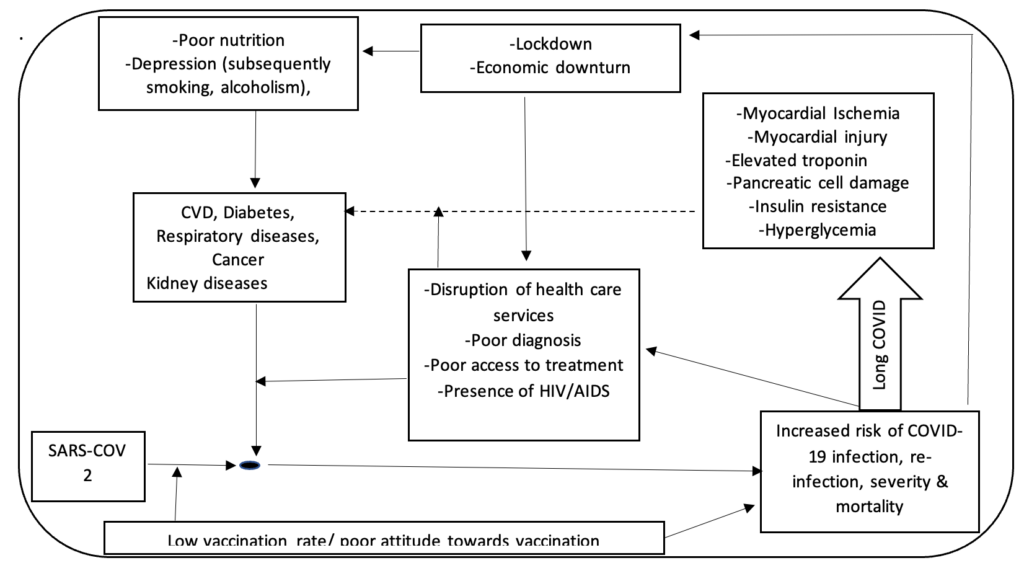
Furthermore, other potential indirect effects of large-scale communicable disease outbreaks similar to the COVID-19 pandemic will potentially complicate or increase vulnerability to NCDs. For example, health system disruption resulting from limited resources, time and manpower impeded the ability of NCD patients to access adequate treatment for their ailments during the current pandemic.[38]. A survey of 41 SSA countries by WHO in 2020 showed that more than 55% of the countries reported disruptions in the management of key NCDs such as hypertension and diabetic complications. In some places only emergency inpatient care for chronic diseases was available[5]. . Moreover, the economic downturn associated with communicable disease pandemics as seen in that of COVID-19 could have a substantial indirect negative effect on the burden of NCDs through its adverse impact on access to treatment, essential drugs, foods and capacity for individuals and families to cope with daily financial responsibilities. For example, a preliminary study by the World Bank on the socioeconomic impact of the COVID-19 pandemic among individuals and households in four SSA countries showed that 77% of the population live in households that have lost income due to the pandemic, while 20-25% of household in each country were unable to purchase essential medicines and staple foods[39]. A more recent report observed a 34% increase (since 2020) in the number of households who were unable to meet their basic food needs in West Africa alone[40]. This has peculiar implications for NCD patients, given that most of them require daily access to drugs to control their conditions and maintain a healthy living. Similarly, most NCD patients require specific dietary recommendations and foods which would be difficult to access in the event of financial hardship. Besides, the fact that the cost of health care in many African countries are borne by patients themselves has negative implications on the burden of diagnosed and undiagnosed NCDs[41]. This is because many of such patients or potential patients may find it difficult to secure medical appointments due to financial hardship. The inability of individuals to meet daily financial obligations, in addition to other adverse impacts of lockdowns (such as physical inactivity and frustrations), where applicable, has implications for mental health problems such as depression. Depression could increase vulnerability to alcoholism, obesity and smoking, which could further increase the risk of NCDs in the region. This, therefore, calls for a broader perspective, a more comprehensive approach and partnership towards disease prevention in the region. A hypothesised illustration of this relation based on the experience of the COVID-19 pandemic (Figure 1).
The COVID-19 pandemic experience in SSA calls for an appreciation of the fact that the direct and indirect effects of the increasing burden of NCDs in the region will complicate the existing burden of communicable diseases. Health policies towards the prevention and management of communicable diseases and large outbreaks should take that into consideration. On the other hand, the potential for large-scale communicable disease outbreaks such as COVID-19 to complicate the burden of key NCDs suggests the need to narrow the dichotomy between the prevention of both conditions. There is a need to encourage partnership (for example, in vaccination drives, research, improved access to health care, poverty reduction programmes, and risk factor awareness programmes) among teams implementing communicable and non-communicable disease programmes that hold mutual or complementary benefits. This will enhance both the effectiveness and efficiency of such programmes, given the limited resources to tackle the increasing burden of NCD amidst a significant burden of communicable diseases. The understanding of the potential relationship between communicable and non-communicable diseases can be harnessed towards the strengthening of community awareness and action against factors that predispose or increase vulnerability to communicable and non-communicable diseases. Finally, there is a need to review existing communicable and non-communicable disease programmes/policies in the region with the aim of integrating them where necessary. For example, consideration should be made towards integrating NCD prevention into primary health care programming.
Views: 3,241
Menu, Tables and Figures