Research | Open Access | Volume 8 (3): Article 46 | Published: 01 Jul 2025
Obed Bangdome Ofori1, Joseph Asamoah Frimpong2,&, Isaac Baffoe-Nyarko1, Azumah Abdul-Tawab1, Horlali Yao Gudjinu1, Eunice Baiden Laryea2, Marion Okoh-Owusu3, Ernest Kenu2,4, Dennis Odai Laryea1, Franklin Asiedu-Bekoe5
1Disease Surveillance Department, Ghana Health Service, Accra, Ghana, 2Ghana Field Epidemiology and Laboratory Training Program, University of Ghana, Accra, Ghana, 3Western North Regional Health Directorate, Ghana Health Service, Bodi, Ghana, 4Department of Epidemiology and Disease Control, School of Public Health, University of Ghana, Accra, Ghana, 5Public Health Division, Ghana Health Service, Accra, Ghana
&Corresponding author: Joseph Asamoah Frimpong, Ghana Field Epidemiology and Laboratory Training Program, University of Ghana, Accra, Ghana, Email: asamoah.frimpong@gmail.com ORCID: https://orcid.org/0000-0002-4758-0589
Received: 08 Jan 2024, Accepted: 01 Jul 2025, Published: 01 Jul 2025
Domain: Polio Elimination, Vaccine Preventable Diseases, Field Epidemiology
Keywords: Acute Flaccid Paralysis, Poliomyelitis, Ghana
©Obed Bangdome Ofori et al Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Obed Bangdome Ofori et al Factors influencing the achievement of core acute flaccid paralysis indicators in the Western North Region, Ghana, 2022. Journal of Interventional Epidemiology and Public Health. 2025;8:46. https://doi.org/10.37432/jieph.2025.8.3.170
Background: In response to polio outbreaks, Ghana enhanced its Acute Flaccid Paralysis (AFP) surveillance system, revising the target for the Non-polio AFP (NP-AFP) rate for children under 15 years from at least 2 to 3 cases per 100,000 population. However, some districts in the Western North Region (WNR) continue to fall short of achieving both the NP-AFP rate and stool adequacy targets. This study examined factors influencing the achievement of core AFP indicators in the WNR.
Methods: An analytical cross-sectional study was conducted from 4th to 31st October 2022 using a multistage sampling technique. Data were collected on demographic characteristics, achievement of NP-AFP rate and stool adequacy targets from January 2019 to June 2022, AFP surveillance knowledge and practices, and availability of resources. A multivariable logistic regression analysis was performed using Stata to identify factors associated with achievement of the core indicators.
Results: A total of 62 health workers with median age of 34 years (IQR: 29 – 39.75) completed the survey. Only 43.6% (27/62) had worked in facilities that met both core AFP indicators during their period of service. Adequate knowledge of AFP surveillance was demonstrated by just 21.0% (13/62), and 37.1% (23/62) had both good surveillance practices and adequate resources. Notably, access to adequate resources was significantly associated with higher odds of achieving both indicators (aOR = 4.5, 95% CI: 1.1–19.8, p = 0.045), while working in a health centre was associated with significantly lower odds (aOR = 0.05 95% CI: 0.0–0.44, p = 0.007)
Conclusions: Achievement of core AFP surveillance indicators in the WNR remains suboptimal. Inadequate knowledge, poor surveillance practices, insufficient resources and lower-level health facilities were major contributors. To strengthen early detection and improve performance, the WNR Health Directorate should prioritise health centres, training and ensure consistent provision of logistics such as vehicles, fuel, stool containers, and specimen carriers.
The World Health Organization (WHO) adopted Acute Flaccid Paralysis (AFP) surveillance as part of strategies for the Global Polio Eradication Initiative (GPEI) to end poliomyelitis globally [1]. This has contributed to a 99.9% reduction in the global incidence of Wild Poliovirus (WPV) [2]. The persistent detection of polio cases in Afghanistan and Pakistan puts polio-free countries at risk of WPV importation [3]. In February and May 2022, Malawi and Mozambique respectfully imported WPV of Pakistan origin [4]. These were the first WPV cases in the African region since 2020 [5].
Ghana adopted GPEI in 1996, which included the implementation of AFP surveillance as a cornerstone of polio eradication efforts. AFP surveillance involves the systematic monitoring of all cases of sudden flaccid paralysis, particularly in children under the age of 15 [6]. Two core indicators, namely Non-polio AFP (NP-AFP) rate and stool adequacy, are used to monitor AFP surveillance performance in Ghana. The target for NP-AFP rate is minimum of 2 cases per 100,000 children under 15 years in the absence of polio outbreaks, rising to at least 3 per 100,000 children under 15 years during outbreaks. The stool adequacy target is set at 80%, ensuring sufficient stool samples for laboratory analysis. These indicators help assess surveillance effectiveness and guide polio eradication efforts [7].
In response to the Circulating Vaccine-Derived Poliovirus type 2 (cVDPV2) outbreak, Ghana activated enhanced AFP surveillance along with other interventions, which led to the revision of the Non-polio AFP (NP-AFP) rate target. The target was increased from a minimum of 2 cases to at least 3 cases per 100,000 population of children under 15 years. Between 2019 and 2021, some districts within the Western North Region (WNR) failed to meet the revised NP-AFP rate, as well as the stool adequacy target. Notably, performance for the NP-AFP rate declined by the first half of 2022. In 2019 and 2020, 66.7% (6/9) of districts achieved the target for NP-AFP rate, but this proportion decreased from 88.9% (8/9) in 2021 to 55.6% (5/9) in the first half of 2022. Similarly, AFP stool adequacy remained suboptimal, with only 77.8% (7/9) of districts meeting the 80% target during the 2019-2021 period, and this stagnation continued into the first half of 2022. These trends highlight significant gaps in surveillance performance, which may hinder the effectiveness of polio eradication efforts in the region. The most recent comprehensive evaluation of national AFP surveillance in Ghana was conducted in 2014 [6]. Rising inadequate stools have been associated with polio-compatible cases and inadequate disease surveillance data have resulted in missing outbreaks, delayed contact tracing and public health actions [8] [9]. As a region bordering La Cote D’Ivoire to the west, the risk of international spread of diseases, including polio, is high. To enhance AFP surveillance and improve early detection and response to outbreaks in the WNR, this study was conducted to identify factors influencing the achievement of core AFP indicators in the region.
Study setting
The study was conducted in WNR, one of the 16 regions of Ghana. It is bordered by La Cote d’Ivoire to the west, the Central Region to the southeast, and the Ashanti, Ahafo, and Bono regions to the north. The population of WNR is 880,921, based on the 2021 Population and Housing Census. The region consists of nine districts, namely Sefwi Wiawso, Aowin, Bia East, Bia West, Sefwi Akontombra, Juaboso, Bodi, Suaman, and Bibiani-Anhwiaso-Bekwai, all of which are classified as rural. There are 335 health facilities in the region, including 16 hospitals, 26 health centers, 31 clinics, 238 functional Community-based Health Planning and Services zones, and 24 maternity homes. All these facilities participate in AFP surveillance activities. AFP stool samples are collected at the health facility level, transported to the district capital, and then sent to the national polio public health and reference laboratory in Accra for analysis. Vaccination coverage for Oral Polio Vaccine 3 (OPV-3), based on administrative data, was reported at 90.5% in 2019, 75.8% in 2020, and 91.6% in 2021 [10].
Study Design
An analytic cross-sectional study was conducted to collect data from key health personnel involved in AFP surveillance. Data collection took place from 4th to 31st October 2022, approximately two months after the WNR held its annual half-year performance review meeting.
Study Population
The study targeted key health personnel involved in Acute Flaccid Paralysis (AFP) surveillance across public and private health facilities in five selected districts of the WNR. Participants included Disease Control Officers (including Public Health Officers, Technical Officers, and Field Technicians), Medical Doctors, and Physician Assistants. Eligible participants were health personnel stationed at the selected health facilities in the sampled districts, who were engaged in AFP surveillance activities and had been at post at any time between 1st January 2019 and 30th June 2022. Health personnel who were off duty or unavailable on the day of the facility visit were excluded from the study.
Study Variables
The dependent variable in this study was the achievement of both core AFP surveillance indicators, namely non-polio AFP (NP-AFP) rate and stool adequacy. This variable was measured on a binary scale, defined as “achieved” if the respondent was at post during a period in which their health facility consistently met both indicator targets (NP-AFP rate and stool adequacy) throughout the time they were at post between 1st January 2019 and 30th June 2022. It was classified as “not achieved” if the targets were not met during the respondent’s period of service within that timeframe. The independent variables were factors that may influence the attainment of these indicators, including the health personnel’s level of knowledge on AFP surveillance, their practices in implementing surveillance activities, and the availability of resources for AFP surveillance. Knowledge level was assessed using 12 questionnaire items, with responses scored on a binary scale (0 = no, 1 = yes). A composite score greater than 6 was classified as adequate knowledge, while a score of 6 or less indicated inadequate knowledge. Practices towards AFP surveillance were measured using 8 items, also scored on a binary scale, with a total score above 4 indicating good practices and a score of 4 or less indicating poor practices. Resource allocation was measured using 7 items, similarly assessed on a binary scale, with a score above 4 classified as adequate resource allocation and a score below 4 indicating inadequate allocation. Although all items were adapted from the Ghana Polio Surveillance Guidelines [7], the scoring thresholds were determined by the study team based on expert judgment and distribution of responses, not directly from the guideline.
Sample Size Determination
The sample size was determined using Cochran’s formula (1977), adjusted for a finite population of 179 key health personnel involved in AFP surveillance in the Western North Region. A hypothetical estimate of 50% was assumed for the proportion achieving both core AFP surveillance indicators. With a 5% level of significance (α = 0.05), a 95% confidence level, a margin of error of 5%, and an anticipated non-response rate of 5%, the final estimated sample size was 62.
Sampling Procedure
The Western North Region was divided into nine clusters based on district administrative boundaries. Each district was assigned a unique number from 1 to 9. Five districts, namely Bia East, Suaman, Aowin, Bibiani Anhwiaso Bekwai, and Bodi were randomly selected using the Rand function in Excel. Within each selected district, all public and private health facilities that had reported at least one AFP case between 1 January 2019 and 30 June 2022 were included. The study period was chosen because the cVDPV 2 outbreak was detected in 2019 and data up to June 2022 was the most recent complete dataset. In the second stage, a proportionate sampling was used to allocate the number of participants from each district relative to its AFP surveillance workforce size. In Aowin 16 of 17 eligible health personnel were selected; in Bia East 5 of 6; in Bibiani Anhwiaso Bekwai 25 of 27; in Bodi 9 of 10; and in Suaman 7 of 10, making a total of 62 participants out of 70 eligible health workers. In the third stage, a list of eligible health personnel from each selected facility were compiled and each individual was assigned a unique number. Simple random sampling using Excel’s random number generator was then applied to select participants from these lists according to the district and facility quotas. Selected participants were visited at their facilities for data collection. All invited individuals participated except for three who were unavailable and were replaced by randomly selected alternatives from the same district and facility to maintain sample size and representativeness.
Data Collection Procedure
Data were collected using a researcher-administered questionnaire adapted from the monitoring and evaluation criteria outlined in the Ghana Polio Surveillance Guidelines [7]. Before the actual implementation of the study, the adapted questionnaire was pre-tested in the Ablekuma West district of the Greater Accra Region to ensure its clarity and relevance. Following the pre-test, the data collected was thoroughly reviewed by the research team for logical coherence to confirm its accuracy and consistency.
Data Analysis
The data were cleaned, coded, and analysed using Stata (Stata Statistical Software: Release 14; College Station, TX; Stata Corp LP). Descriptive statistics were used to summarise the distribution of demographic characteristics of the respondents. Categorical variables were summarized using frequencies and their associated percentages. The dependent variable was the achievement of both core AFP surveillance indicators, which was categorized as a dichotomous variable (No, Yes). Bivariate analyses were conducted to determine the association between the dependent variable and independent variables. The Pearson Chi-squared test or Fisher’s Exact test, and multivariable logistic regression were employed to examine the relationships between the achievement of both core AFP surveillance indicators and independent variables. The statistical significance of the association between the achievement of these surveillance indicators and variables such as knowledge of AFP surveillance, practices towards AFP surveillance implementation, and resource allocations for AFP surveillance was set at a p-value of < 0.05.
Ethical Considerations
This study was conducted as part of the routine monitoring and supervision responsibilities of the GHS and the Ghana Field Epidemiology and Laboratory Training Program (GFELTP), in accordance with the Ghana Public Health Act 851 [11]. Participants’ privacy and confidentiality were upheld throughout the research. Identifiable data was securely handled, with restricted access to ensure the authors did not view personally identifiable information during data collection and analysis. Permission was obtained from relevant authorities, including facility and district heads. Informed consent was sought from all participants, ensuring they understood the study’s objectives and procedures.
Socio-demographic factors of health personnel engaged in AFP surveillance.
A total of 62 health personnel involved in AFP surveillance were recruited across selected districts in the WNR. The majority were male (69.4%, 43/62), and the most represented age group was 30–39 years (41.9%, 26/62). Nearly half of the respondents were Physician Assistants (45.2%, 28/62), and half had been in the profession for 0–4 years (50.0%, 31/62). Most held a degree (38.7%, 24/62). Participants were mainly drawn from hospitals (37.1%, 23/62) and health centres (32.3%, 20/62), with the vast majority (83.9%, 52/62) working in government-owned facilities (Table 1).
Achievement of Core AFP surveillance indicators
Among the five selected districts, the achievement of the two core AFP surveillance indicators (NP-AFP rate and stool adequacy) varied across the years. According to the District Annual Performance Reports, in 2019, Bia East, Bibiani Anhwiaso Bekwai, and Suaman met both targets. In 2020, only Bodi achieved both indicators, while in 2021, Aowin, Bibiani Anhwiaso Bekwai, and Suaman met the two targets. By June 2022, only Bodi and Suaman had achieved both indicators. Overall, based on the defined criteria, 43.6% (27/62) of respondents worked in facilities that achieved both core AFP surveillance indicators during their period of service. Bia East (2019), Suaman (2019, 2021, 2022), Aowin (2021), Bibiani Anhwiaso Bekwai (2019, 2021), and Bodi (2020, 2022)
Knowledge of AFP surveillance
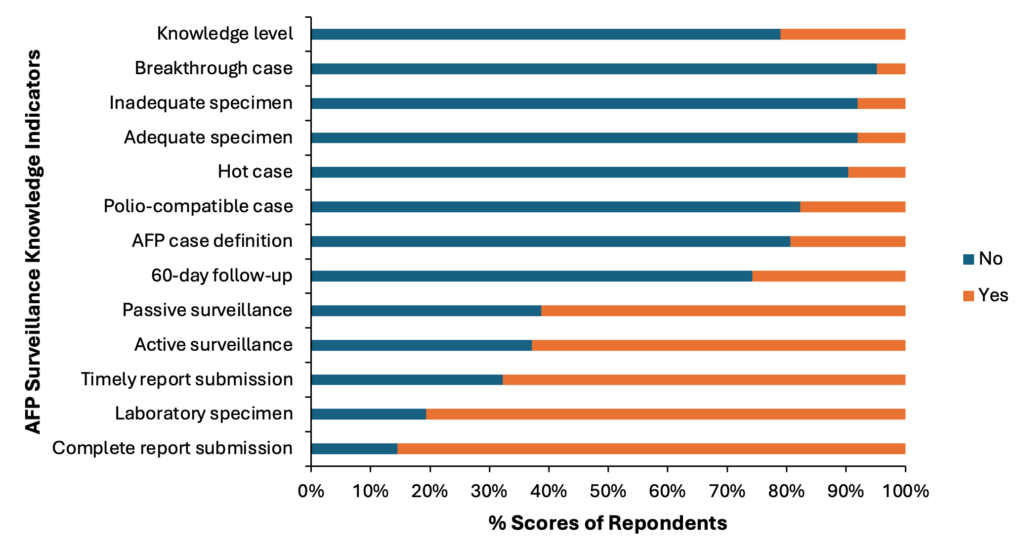
Most respondents demonstrated good knowledge of basic AFP surveillance procedures. Specifically, 85.5% (53/62) understood the requirement for complete report submission, and 80.6% (50/62) knew the correct type of specimen required for AFP laboratory investigation. Awareness of timely report submission procedures was also relatively high at 67.7% (42/62). Regarding surveillance strategies, 62.9% (39/62) and 61.3% (38/62) correctly identified active and passive surveillance methods, respectively. Knowledge declined for more specialized and technical aspects of the surveillance system. Only 25.8% (16/62) of participants were aware of the 60-day follow-up requirement, and just 19.4% (12/62) could accurately define an AFP case. The understanding of case classifications was limited, with 17.7% (11/62) familiar with the term polio-compatible case, and 9.7% (6/62) understood what constitutes a hot case. Similarly, only 8.1% (5/62) could correctly identify criteria for both adequate and inadequate stool specimens. The concept of a breakthrough case was the least understood, with just 4.8% (3/62) demonstrating correct knowledge. Overall, only 21.0% (13/62) of the participants demonstrated adequate knowledge of AFP surveillance (Figure 1).
Practices of AFP surveillance
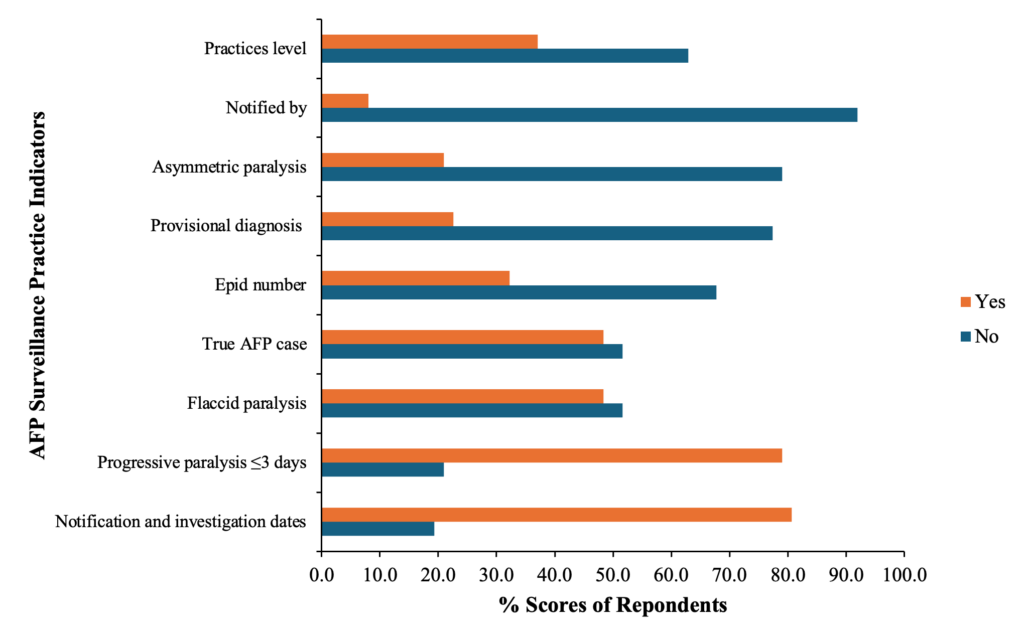
The findings revealed varying levels of application of AFP surveillance knowledge among respondents, particularly in completing the AFP Case Investigation Form (CIF). Among the 62 respondents, 80.6% (50/62) correctly understood the notification and investigation dates on the CIF, while 79.0% (49/62) accurately explained the criteria for progressive paralysis occurring within three days. Only 48.4% (30/62) were able to correctly define flaccid paralysis, and the same proportion (48.4%, 30/62) could accurately classify a true AFP case. Regarding the assignment of epidemiological numbers, 32.3% (20/62) correctly provided the appropriate coding format for their respective districts. Accurate reporting of provisional diagnoses was observed in 22.6% (14/62), while just 21.0% (13/62) correctly distinguished asymmetric paralysis. Notably, only 8.1% (5/62) correctly identified the appropriate notifier for the “Notified by” field on the CIF. Overall, based on the assessment criteria, only 37.1% (23/62) of the participants demonstrated adequate practice in AFP surveillance (Figure 2).
Resource availability for AFP surveillance
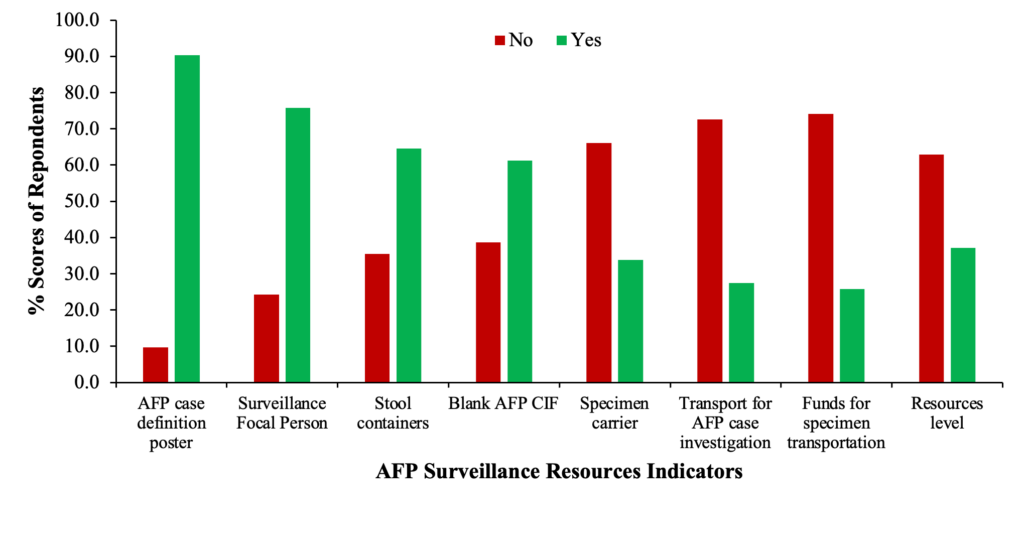
The availability of essential resources to support AFP surveillance varied across the surveyed areas. Among the 62 respondents, 90.3% (56/62) reported the availability of the AFP case definition poster, while 75.8% (47/62) indicated they had a Surveillance Focal Person (SFP) at their facilities. Stool containers were accessible to 64.5% (40/62), and 61.3% (38/62) confirmed the availability of blank AFP CIFs. However, only 33.9% (21/62) reported access to a specimen carrier, and just 27.4% (17/62) had transport available for AFP case investigations. Furthermore, only 25.8% (16/62) of respondents indicated that funds were available for specimen transportation. Overall, only 37.1% (23/62) of respondents had access to an adequate level of resources necessary for effective AFP surveillance (Figure 3).
Relationship between the achievement of AFP core indicators and socio-demographic characteristics, knowledge, practice, and resource levels
Bivariate analysis using Pearson’s chi-squared test revealed no statistically significant associations between the achievement of AFP core indicators and sex (p= 0.879), age (p= 0.059), profession (p= 0.203), duration in the profession (p= 0.123), or educational level (p= 0.227). However, facility-related factors were significantly associated with performance. Specifically, working in a government-owned facility was linked to a higher likelihood of achieving AFP indicators compared to private facilities (p= 0.002). Additionally, personnel working in Health Centres were significantly less likely to achieve the AFP targets compared to those in Hospitals (p< 0.01) (Table 1). In the bivariate logistic regression model, facility ownership did not show a statistically significant association with the outcome. However, compared to personnel working at District Health Administrations (DHA), those stationed at Health Centres had significantly lower odds of achieving both AFP core indicators (cOR= 0.03, 95% CI: 0.01–0.24, p< 0.01). This association remained statistically significant in the multivariable model, though with slightly higher adjusted odds (aOR= 0.05, 95% CI: 0.00–0.44, p= 0.007). Respondents with adequate knowledge of AFP surveillance were significantly more likely to work in a health facility that met both AFP indicator targets in both bivariate analyses (p= 0.006 and p= 0.011). However, this relationship lost statistical significance after adjustment (aOR= 4.7, 95% CI: 0.7–33.9, p= 0.122). Similarly, good practice of AFP surveillance was associated with a higher likelihood of achieving the indicators in the bivariate models (p= 0.008 and p= 0.010), but this association was not statistically significant in the adjusted analysis (aOR= 0.5, 95% CI: 0.1–2.8, p= 0.411). In contrast, access to adequate resources for AFP surveillance showed a strong and consistent relationship with indicator achievement, remaining statistically significant in both bivariate analyses (p= 0.008 and p= 0.010), and multivariable analysis (aOR= 4.5, 95% CI: 1.1–19.8, p= 0.045) (Table 2).
This study aimed to assess the achievement of the two core AFP surveillance indicators in the WNR and determine factors influencing their attainment. Overall, 43.6% of respondents in this study reported working in facilities that met both core AFP surveillance indicators during their period of service. This achievement is notably lower than the 66.0% reported across counties in Kenya between 2016 and 2018 [12] and significantly lower than the 100% recorded by all local government areas in Sokoto State, Nigeria [13]. The comparatively lower performance observed in our study in the WNR may be attributed to differences in data sources. While this study relied on primary data collected directly from health workers at the facility and district levels, the Kenyan and Nigerian studies utilized secondary data aggregated at broader administrative levels, namely county and local government area, respectively.
Only 21.0% of participants in this study demonstrated adequate knowledge of AFP surveillance, which is considerably lower than the 52% reported among nurses in Mwenezi District, Masvingo Province, Zimbabwe [14]. This disparity may be attributed to differences in study populations, as the Zimbabwean study focused exclusively on nurses, while our study included a broader range of healthcare professionals such as medical doctors, physician assistants, public health officers, and disease control officers with varying levels of involvement in AFP surveillance. Notably, only 19.4% of participants accurately mentioned the AFP case definition, which is markedly lower than the 95.6% reported in Sokoto State, Nigeria [15], and 91.4% in Najaf City, Iraq [16]. The lower proportion observed in our study may be influenced by methodological differences, our respondents were required to verbally recall and define the AFP case, whereas the Iraq study asked participants to agree or disagree with a case definition that was read to them, and the Nigeria study was conducted shortly after an AFP surveillance intervention. Accurate knowledge of disease case definitions is essential for effective surveillance system implementation. A study assessing the Integrated Disease Surveillance and Response (IDSR) system in the Eastern Region, Ghana, found that health workers’ limited knowledge of priority diseases contributed to poor data collection and underutilization of surveillance information for outbreak prevention and control [17].
In our study, 80.6% of respondents correctly identified stool as the appropriate specimen for AFP laboratory investigation. This finding is slightly higher than the 76.0% reported in Mwenezi District, Masvingo Province, Zimbabwe, where a similar study assessed the knowledge of health workers on AFP surveillance procedures [14]. However, it is slightly lower than the 90.0% reported among health workers in Sanyati District, Zimbabwe, who accurately identified stool as the specimen of choice for AFP diagnosis [18]. The variation in findings may be attributed to the geographical scope of the studies; the Sanyati study was limited to a single district, potentially allowing for more targeted capacity-building interventions, whereas our study spanned multiple districts, which could have introduced heterogeneity in training coverage and staff capacity.
Regarding surveillance strategies, over 60.0% of participants correctly identified both active and passive surveillance methods, a figure higher than the 30.5% recorded among clinicians in Sokoto State, Nigeria [15]. The difference in findings may be attributed to the composition of the study populations. While the Sokoto study exclusively involved clinicians, the current study included a wider range of health professionals across multiple cadres, potentially offering a broader perspective on surveillance knowledge. In addition, 25.8% of the participants demonstrated awareness of the 60-day follow-up requirement for AFP cases, a finding that surpasses the 6.0% reported among nurses in Mwenezi District, Masvingo, Zimbabwe [14].
In terms of AFP practice, 37.1% demonstrated adequate ability in completing the AFP CIF, with 80.6% correctly interpreting notification and investigation dates. However, date-related sections remained among the most inconsistently completed areas, in line with similar studies indicating challenges in accurate documentation [18].
Additionally, 79.0% of participants correctly described the criteria for progressive paralysis occurring within three days. This finding contrasts with the situation in Sokoto State, Nigeria, where only 59.0% of reviewed CIFs lacked documentation on the progression of paralysis [13]. This discrepancy may be partly due to methodological differences. While the present study required respondents to verbally describe the clinical progression criteria, the Nigerian study reviewed already completed forms. Despite 79.0% of participants correctly describing the criteria for progressive paralysis occurring within three days, fewer than 50% of them could correctly define flaccid paralysis or accurately classify a true AFP case. Moreover, accurate reporting of provisional diagnoses was observed among only 22.6% of respondents, and just 21.0% were able to correctly distinguish asymmetric paralysis. These limitations in clinical recognition and reporting could result in misdiagnosis of AFP cases, leading to an overestimation of the actual AFP burden. Such misdiagnosed cases could artificially inflate the NP-AFP rate, a key performance metric, and undermines the sensitivity and specificity of the surveillance system. Furthermore, misdiagnosed AFP cases unnecessarily consume public health resources, as each AFP case requires complete investigation, including clinical assessment, specimen collection, and laboratory confirmation.
In terms of resource availability, 37.1% of participants reported having access to adequate resources for AFP surveillance. This contrasts with findings from Zanzibar, where nearly all districts reportedly had access to the full complement of resources necessary for effective surveillance implementation [9]. Access to AFP case definition posters was reported by 90.3% of respondents, which is slightly lower than the 92.9% coverage reported by clinicians in Nigerian [15]. The availability of stool containers and specimen carriers was 64.5% and 33.9%, respectively. According to [19], the occurrence of temperature excursions in AFP stool samples was significantly associated with inadequate icepack availability, particularly due to failure to replenish icepacks after previous sample transport.
Only 27.4% of participants reported access to transport for case investigations. This is consistent with findings from Mwenezi District, Zimbabwe, where most health facilities lacked vehicles for transporting stool specimens and case investigation forms [14]. Additionally, while 75.8% of respondents reported the presence of a Surveillance Focal Person at their facility, only 27.4% reported access to dedicated funds for surveillance activities. These findings align with those from Northern Ghana, where 77.8% of health facilities had designated disease surveillance officers [20]. Several studies have emphasized that the shortage of trained frontline health personnel and limited funding for IDSR activities at the district and facility levels remain major obstacles to the successful implementation of surveillance systems [21] [22] [23].
This study was limited to five districts within the WNR, which may affect the generalizability of the findings to other regions or the national level. Furthermore, the cross-sectional study design precludes causal inferences. Nevertheless, the findings offer important insights into factors that may influence the achievement of the two core AFP surveillance indicators, warranting further investigation and consideration in the development of targeted interventions.
The achievement of the two core AFP surveillance indicators among facilities in the WNR of Ghana was found to be suboptimal. Key contributing factors to the low case identification included inadequate knowledge of AFP surveillance, poor surveillance practices, inadequate resources to support effective implementation, and lower-level health facilities. To enhance early detection and improve surveillance performance, the WNR Health Directorate should prioritize capacity-building through targeted training of health personnel, with particular focus on health centres and ensure the consistent availability of essential logistics such as vehicles, fuel, stool containers, and specimen carriers.
What is already known about the topic
What this study adds
Factors associated with the low AFP case identification are related to;
OBO: Conceptualization, Formal analysis, Methodology, writing original draft, review and editing; JAF: Writing, review and editing; IBN: Writing – review & editing; AAT: Writing – review & editing; HYG: Writing – review & editing; EBL: Writing – review & editing; MOO: Supervision, Writing – review & editing; EK: Supervision, Writing – review & editing; DOL: Supervision, Writing – review & editing; FAB: Supervision, Writing – review & editing.
| Socio-demographic characteristics | Frequency (N=62) | Achievement of AFP core indicators | Chi-square/ Fisher’s exact | p-value | ||
|---|---|---|---|---|---|---|
| Yes (n=27) | No (n=35) | Total (n=62) | ||||
| Sex | ||||||
| Female | 19 (30.7) | 8 (29.6) | 11 (31.4) | 19 (30.7) | ||
| Male | 43 (69.4) | 19 (70.3) | 24 (68.6) | 43 (69.3) | 0.0232 | 0.879 |
| Age | ||||||
| 20–29 | 20 (32.3) | 4 (14.8) | 16 (45.7) | 20 (32.3) | ||
| 30–39 | 26 (41.9) | 14 (51.9) | 12 (34.3) | 26 (41.9) | ||
| 40–49 | 12 (19.4) | 6 (22.2) | 6 (17.1) | 12 (19.4) | ||
| 50–59 | 4 (6.5) | 3 (11.1) | 1 (2.9) | 4 (6.4) | 7.4456 | 0.059 |
| Profession | ||||||
| Field Technician (DC) | 12 (19.4) | 5 (18.5) | 7 (20.0) | 12 (19.4) | ||
| Technical Officer (DC) | 8 (12.9) | 4 (14.8) | 4 (11.4) | 8 (12.9) | ||
| Public Health Officer | 9 (14.5) | 7 (25.9) | 2 (5.8) | 9 (14.5) | ||
| Physician’s Assistant | 28 (45.2) | 9 (33.3) | 19 (54.3) | 28 (45.2) | ||
| Medical Doctor | 5 (8.1) | 2 (7.4) | 3 (8.5) | 5 (8.0) | 5.9493 | 0.203 |
| Duration in Profession | ||||||
| 0–4 | 31 (50.0) | 11 (40.8) | 20 (57.2) | 31 (50.0) | ||
| 5–9 | 11 (17.7) | 3 (11.1) | 8 (22.9) | 11 (17.7) | ||
| 10–14 | 11 (17.7) | 7 (25.9) | 4 (11.4) | 11 (17.7) | ||
| ≥15 | 9 (14.5) | 6 (22.2) | 3 (8.5) | 9 (14.6) | 5.7676 | 0.123 |
| Educational level | ||||||
| Certificate | 12 (19.4) | 5 (18.5) | 7 (20.0) | 12 (19.4) | ||
| Diploma | 20 (32.3) | 8 (29.6) | 12 (34.3) | 20 (32.3) | ||
| Degree | 24 (38.7) | 9 (33.3) | 15 (42.8) | 24 (38.7) | ||
| Masters | 6 (9.7) | 5 (18.5) | 1 (2.9) | 6 (9.6) | 4.34 | 0.227 |
| Facility type | ||||||
| DHA | 16 (23.8) | 12 (44.5) | 4 (11.4) | 16 (25.8) | 19.4834 | <0.01 |
| CHPS | 1 (1.6) | 0 (0.0) | 1 (2.9) | 1 (1.6) | ||
| Clinic | 2 (3.2) | 0 (0.0) | 2 (5.8) | 2 (3.2) | ||
| Health Centre | 20 (32.3) | 2 (7.4) | 18 (51.4) | 20 (32.3) | ||
| Hospital | 23 (37.1) | 13 (48.1) | 10 (28.5) | 23 (37.1) | ||
| Facility ownership | ||||||
| Government | 52 (83.9) | 27 (100.0) | 25 (71.5) | 52 (83.9) | ||
| Private | 10 (16.1) | 0 (0.0) | 10 (28.5) | 10 (16.1) | 9.1978 | 0.002 |
Note: DC stands for Disease Control, DHA denotes District Health Administration, CHPS refers to Community-based Health Planning and Services.
| Factors | Achievement of AFP core indicators | cOR (95% CI) | p-value | aOR (95% CI) | p-value | ||
|---|---|---|---|---|---|---|---|
| Yes (n = 27) | No (n = 35) | Total (n = 62) | |||||
| Facility ownership | |||||||
| Government (ref) | 27 (100.0) | 25 (71.5) | 52 (83.9) | 1 | |||
| Private | 0 (0.0) | 10 (28.5) | 10 (16.1) | 1 (0.6–1.9) | 0.782 | ||
| Facility type | |||||||
| DHA (ref) | 12 (44.5) | 4 (11.4) | 16 (25.8) | 1 | 1 | ||
| CHPS | 0 (0.0) | 1 (2.9) | 1 (1.6) | 1 | 1 | ||
| Clinic | 0 (0.0) | 2 (5.8) | 2 (3.2) | 1 | 1 | ||
| Health Centre | 2 (7.4) | 18 (51.4) | 20 (32.3) | 0.03 (0.01–0.24) | <0.01 | 0.05 (0.0–0.44) | 0.007 |
| Hospital | 13 (48.1) | 10 (28.5) | 23 (37.1) | 0.4 (0.1–1.8) | 0.242 | 0.77 (0.2–3.9) | 0.751 |
| Knowledge of AFP surveillance | |||||||
| Inadequate (ref) | 17 (63.0) | 32 (91.4) | 49 (79.0) | 1 | 1 | ||
| Adequate | 10 (37.0) | 3 (8.6) | 13 (21.0) | 6.3 (1.5–25.9) | 0.011 | 4.7 (0.7–33.9) | 0.122 |
| Practice of AFP surveillance | |||||||
| Poor (ref) | 12 (44.5) | 27 (77.1) | 39 (69.1) | 1 | 1 | ||
| Good | 15 (55.5) | 8 (22.9) | 23 (37.1) | 4.2 (1.4–12.6) | 0.010 | 0.5 (0.1–2.8) | 0.411 |
| Resource gap in AFP surveillance | |||||||
| Inadequate (ref) | 12 (44.5) | 27 (77.1) | 39 (69.1) | 1 | 1 | ||
| Adequate | 15 (55.5) | 8 (22.9) | 23 (37.1) | 4.2 (1.4–12.6) | 0.010 | 4.5 (1.1–19.8) | 0.045 |
Note: cOR = Crude Odds Ratio, aOR = Adjusted Odds Ratio, CI = Confidence Interval. DC = Disease Control, DHA = District Health Administration, CHPS = Community-based Health Planning and Services. “ref” = reference category.
Views: 3,237
Menu, Tables and Figures
| Socio-demographic characteristics | Frequency (N=62) | Achievement of AFP core indicators | Chi-square/ Fisher’s exact | p-value | ||
|---|---|---|---|---|---|---|
| Yes (n=27) | No (n=35) | Total (n=62) | ||||
| Sex | ||||||
| Female | 19 (30.7) | 8 (29.6) | 11 (31.4) | 19 (30.7) | ||
| Male | 43 (69.4) | 19 (70.3) | 24 (68.6) | 43 (69.3) | 0.0232 | 0.879 |
| Age | ||||||
| 20–29 | 20 (32.3) | 4 (14.8) | 16 (45.7) | 20 (32.3) | ||
| 30–39 | 26 (41.9) | 14 (51.9) | 12 (34.3) | 26 (41.9) | ||
| 40–49 | 12 (19.4) | 6 (22.2) | 6 (17.1) | 12 (19.4) | ||
| 50–59 | 4 (6.5) | 3 (11.1) | 1 (2.9) | 4 (6.4) | 7.4456 | 0.059 |
| Profession | ||||||
| Field Technician (DC) | 12 (19.4) | 5 (18.5) | 7 (20.0) | 12 (19.4) | ||
| Technical Officer (DC) | 8 (12.9) | 4 (14.8) | 4 (11.4) | 8 (12.9) | ||
| Public Health Officer | 9 (14.5) | 7 (25.9) | 2 (5.8) | 9 (14.5) | ||
| Physician’s Assistant | 28 (45.2) | 9 (33.3) | 19 (54.3) | 28 (45.2) | ||
| Medical Doctor | 5 (8.1) | 2 (7.4) | 3 (8.5) | 5 (8.0) | 5.9493 | 0.203 |
| Duration in Profession | ||||||
| 0–4 | 31 (50.0) | 11 (40.8) | 20 (57.2) | 31 (50.0) | ||
| 5–9 | 11 (17.7) | 3 (11.1) | 8 (22.9) | 11 (17.7) | ||
| 10–14 | 11 (17.7) | 7 (25.9) | 4 (11.4) | 11 (17.7) | ||
| ≥15 | 9 (14.5) | 6 (22.2) | 3 (8.5) | 9 (14.6) | 5.7676 | 0.123 |
| Educational level | ||||||
| Certificate | 12 (19.4) | 5 (18.5) | 7 (20.0) | 12 (19.4) | ||
| Diploma | 20 (32.3) | 8 (29.6) | 12 (34.3) | 20 (32.3) | ||
| Degree | 24 (38.7) | 9 (33.3) | 15 (42.8) | 24 (38.7) | ||
| Masters | 6 (9.7) | 5 (18.5) | 1 (2.9) | 6 (9.6) | 4.34 | 0.227 |
| Facility type | ||||||
| DHA | 16 (23.8) | 12 (44.5) | 4 (11.4) | 16 (25.8) | 19.4834 | <0.01 |
| CHPS | 1 (1.6) | 0 (0.0) | 1 (2.9) | 1 (1.6) | ||
| Clinic | 2 (3.2) | 0 (0.0) | 2 (5.8) | 2 (3.2) | ||
| Health Centre | 20 (32.3) | 2 (7.4) | 18 (51.4) | 20 (32.3) | ||
| Hospital | 23 (37.1) | 13 (48.1) | 10 (28.5) | 23 (37.1) | ||
| Facility ownership | ||||||
| Government | 52 (83.9) | 27 (100.0) | 25 (71.5) | 52 (83.9) | ||
| Private | 10 (16.1) | 0 (0.0) | 10 (28.5) | 10 (16.1) | 9.1978 | 0.002 |
Note: DC stands for Disease Control, DHA denotes District Health Administration, CHPS refers to Community-based Health Planning and Services.
Table 1: Frequency distribution of Socio-Demographic Factors and their Association with Achievement of AFP core indicators, WNR, 2024
| Factors | Achievement of AFP core indicators | cOR (95% CI) | p-value | aOR (95% CI) | p-value | ||
|---|---|---|---|---|---|---|---|
| Yes (n = 27) | No (n = 35) | Total (n = 62) | |||||
| Facility ownership | |||||||
| Government (ref) | 27 (100.0) | 25 (71.5) | 52 (83.9) | 1 | |||
| Private | 0 (0.0) | 10 (28.5) | 10 (16.1) | 1 (0.6–1.9) | 0.782 | ||
| Facility type | |||||||
| DHA (ref) | 12 (44.5) | 4 (11.4) | 16 (25.8) | 1 | 1 | ||
| CHPS | 0 (0.0) | 1 (2.9) | 1 (1.6) | 1 | 1 | ||
| Clinic | 0 (0.0) | 2 (5.8) | 2 (3.2) | 1 | 1 | ||
| Health Centre | 2 (7.4) | 18 (51.4) | 20 (32.3) | 0.03 (0.01–0.24) | <0.01 | 0.05 (0.0–0.44) | 0.007 |
| Hospital | 13 (48.1) | 10 (28.5) | 23 (37.1) | 0.4 (0.1–1.8) | 0.242 | 0.77 (0.2–3.9) | 0.751 |
| Knowledge of AFP surveillance | |||||||
| Inadequate (ref) | 17 (63.0) | 32 (91.4) | 49 (79.0) | 1 | 1 | ||
| Adequate | 10 (37.0) | 3 (8.6) | 13 (21.0) | 6.3 (1.5–25.9) | 0.011 | 4.7 (0.7–33.9) | 0.122 |
| Practice of AFP surveillance | |||||||
| Poor (ref) | 12 (44.5) | 27 (77.1) | 39 (69.1) | 1 | 1 | ||
| Good | 15 (55.5) | 8 (22.9) | 23 (37.1) | 4.2 (1.4–12.6) | 0.010 | 0.5 (0.1–2.8) | 0.411 |
| Resource gap in AFP surveillance | |||||||
| Inadequate (ref) | 12 (44.5) | 27 (77.1) | 39 (69.1) | 1 | 1 | ||
| Adequate | 15 (55.5) | 8 (22.9) | 23 (37.1) | 4.2 (1.4–12.6) | 0.010 | 4.5 (1.1–19.8) | 0.045 |
Note: cOR = Crude Odds Ratio, aOR = Adjusted Odds Ratio, CI = Confidence Interval. DC = Disease Control, DHA = District Health Administration, CHPS = Community-based Health Planning and Services. “ref” = reference category.
Table 2: Relationship between the achievement of AFP core indicators and socio-demographic characteristics, knowledge, practice, and resource levels, WNR, 2024