Research | Open Access | Volume 9 (1): Article 13 | Published: 20 Jan 2026
Views: 3,507
Menu, Tables and Figures
Table 1. Participants Characteristics and Prevalence of Hypertension in Tanga region, 2023 (N=1818)
| Characteristic | Total (%) | Hypertensive n (%) | 95% Confidence Interval |
|---|---|---|---|
| Age (years) | |||
| Below 25 | 237 (13.0) | 53 (22.4) | 17.5–28.1 |
| 25–34 | 372 (20.5) | 101 (27.2) | 22.9–32.0 |
| 35–44 | 442 (24.3) | 142 (32.1) | 27.9–36.6 |
| 45–54 | 378 (20.8) | 176 (46.6) | 41.6–51.6 |
| 55–64 | 225 (12.4) | 108 (48.0) | 41.5–54.5 |
| 65 and above | 164 (09.0) | 106 (64.6) | 57.0–71.6 |
| Gender | |||
| Male | 1231 (67.7) | 475 (38.6) | 35.9–41.3 |
| Female | 587 (32.3) | 211 (36.0) | 32.2–39.9 |
| Education | |||
| Primary | 1145 (63.0) | 434 (37.9) | 31.5–40.7 |
| Secondary | 401 (22.1) | 139 (34.7) | 30.2–39.5 |
| University/College | 107 (06.0) | 41 (38.3) | 29.6–47.8 |
| No formal | 165 (09.1) | 72 (43.6) | 36.3–51.3 |
| Marital status | |||
| Married | 1239 (68.2) | 487 (39.3) | 36.6–42.1 |
| Single | 374 (20.6) | 100 (26.7) | 22.5–31.5 |
| Widow/Widower | 95 (5.2) | 54 (56.8) | 46.7–66.4 |
| Divorced | 110 (6.1) | 45 (40.9) | 32.1–50.3 |
| Occupation | |||
| Government employed | 111 (6.1) | 43 (38.7) | 30.1–48.1 |
| Private employed | 163 (9.0) | 55 (33.7) | 26.9–41.3 |
| Self employed | 1369 (75.3) | 519 (37.9) | 35.4–40.5 |
| Unpaid employed | 175 (9.6) | 69 (39.4) | 32.5–46.9 |
| Residence | |||
| Muheza | 364 (20.0) | 133 (36.5) | 31.7–41.6 |
| Mkinga | 357 (19.6) | 120 (33.6) | 28.9–38.7 |
| Tanga City | 1097 (60.3) | 433 (37.7) | 36.6–42.4 |
| BMI | |||
| Underweight | 137 (7.5) | 34 (24.8) | 18.3–32.7 |
| Normal | 542 (29.8) | 148 (27.3) | 23.7–31.2 |
| Overweight | 421 (23.1) | 181 (43.1) | 38.4–47.9 |
| Obese | 719 (39.6) | 323 (44.9) | 41.3–48.6 |
| Smoking | |||
| Yes | 316 (17.4) | 106 (33.5) | 30.9–37.3 |
| No | 1502 (82.6) | 580 (38.6) | 36.1–41.6 |
| Alcohol | |||
| Yes | 279 (15.4) | 102 (36.6) | 31.1–42.4 |
| No | 1539 (84.7) | 584 (37.9) | 35.6–40.4 |
| Exercise | |||
| Yes | 844 (46.4) | 298 (35.3) | 32.2–38.6 |
| No | 974 (53.6) | 388 (39.8) | 36.8–42.9 |
| Eating Fruits | |||
| Yes | 1728 (95.1) | 657 (38.0) | 35.8–40.4 |
| No | 90 (5.0) | 29 (32.2) | 23.4–42.5 |
| Eating Vegetables | |||
| Yes | 1729 (95.1) | 650 (37.6) | 35.3–39.9 |
| No | 89 (4.9) | 36 (40.4) | 30.8–50.9 |
| Family History of HTN | |||
| Yes | 632 (34.8) | 266 (42.1) | 38.3–46.0 |
| No | 1186 (65.2) | 420 (35.4) | 32.7–38.2 |
Table 1. Participants Characteristics and Prevalence of Hypertension in Tanga region, 2023 (N=1818)
Table 2. Modified Poisson regression analysis of hypertension among the survey participants in the Tanga region in 2023 (N=1818)
| Characteristic | Total n (%) | Prevalence of HTN n (%) | Crude prevalence ratio (95% CI) | Adjusted prevalence ratio (95% CI) |
|---|---|---|---|---|
| Age groups | 1.02 (1.01–1.02) | 1.02 (1.02–1.03) © | ||
| Below 25 | 237 (13.0) | 53 (22.4) | Ref | Ref |
| 25–34 | 372 (20.5) | 101 (27.2) | 1.21 (0.91–1.62) | 1.17 (0.85–1.62) |
| 35–44 | 442 (24.3) | 142 (32.1) | 1.43 (1.09–1.89) | 1.38 (0.99–1.94) |
| 45–54 | 378 (20.8) | 176 (46.6) | 2.08 (1.60–2.70) | 2.07 (1.48–2.89) |
| 55–64 | 225 (12.4) | 108 (48.0) | 2.14 (1.63–2.82) | 2.18 (1.54–3.07) |
| 65 and above | 164 (09.0) | 106 (64.6) | 2.89 (2.22–3.76) | 3.00 (2.13–4.23) |
| Gender | ||||
| Male | 1231 (67.7) | 475 (38.6) | 1.02 (0.98–1.05) | 1.20 (1.05–1.37) |
| Female | 587 (32.3) | 211 (36.0) | Ref | Ref |
| Education | ||||
| No formal | 165 (09.1) | 72 (43.6) | Ref | Ref |
| Primary | 1145 (63.0) | 434 (37.9) | 0.87 (0.72–1.05) | 1.01 (0.83–1.22) |
| Secondary | 401 (22.1) | 139 (34.7) | 0.79 (0.64–0.99) | 1.06 (0.84–1.34) |
| University/College | 107 (06.0) | 41 (38.3) | 0.88 (0.65–1.18) | 1.06 (0.78–1.44) |
| Marital status | ||||
| Married | 1239 (68.2) | 487 (39.3) | 0.98 (0.92–1.06) | 0.94 (0.75–1.18) |
| Single | 374 (20.6) | 100 (26.7) | 0.89 (0.83–0.97) | 1.02 (0.75–1.42) |
| Widow/Widower | 95 (5.2) | 54 (56.8) | 1.11 (1.01–1.21) | 1.20 (0.90–1.60) |
| Divorced | 110 (6.1) | 45 (40.9) | Ref | Ref |
| Occupation | ||||
| Government employed | 111 (06.1) | 43 (38.7) | Ref | Ref |
| Private employed | 163 (09.0) | 55 (33.7) | 0.96 (0.88–1.05) | 1.14 (0.82–1.58) |
| Self employed | 1369 (75.3) | 519 (37.9) | 0.99 (0.92–1.06) | 1.19 (0.92–1.55) |
| Unpaid employed | 175 (09.6) | 69 (39.4) | 1.00 (0.92–1.09) | 1.28 (0.94–1.76) |
| Residence | ||||
| Mkinga | 357 (19.6) | 120 (33.6) | Ref | Ref |
| Muheza | 364 (20.0) | 133 (36.5) | 1.02 (0.97–1.07) | 1.24 (1.01–1.52) |
| Tanga CC | 1097 (60.3) | 433 (37.7) | 1.04 (1.00–1.08) | 1.47 (1.24–1.75) |
| BMI | ||||
| Underweight (<20) | 137 (07.5) | 13 (23.64) | Ref | Ref |
| Normal (20–24.9) | 542 (29.8) | 231 (27.60) | 1.10 (0.80–1.52) | 1.05 (0.77–1.45) |
| Overweight (25–29.9) | 421 (23.1) | 242 (43.06) | 1.74 (1.27–2.37) | 1.62 (1.18–2.21) |
| Obese (30 and above) | 719 (39.6) | 200 (54.95) | 1.81 (1.34–2.45) | 1.79 (1.32–2.43) |
| Family history of hypertension | ||||
| Yes | 632 (34.8) | 266 (42.09) | 1.04 (1.01–1.08) | 1.13 (1.01–1.27) |
| No | 1186 (65.2) | 420 (35.41) | Ref | Ref |
Key: © The prevalence ratios for age as a continuous data.
Table 2. Modified Poisson regression analysis of hypertension among the survey participants in the Tanga region in 2023 (N=1818)
1Department of Epidemiology and Biostatistics, Muhimbili University of Health and Allied Sciences, School of Public Health and Social Sciences, Dar es Salaam, P.O.Box 65001, Dar es Salaam, Tanzania, 2Tanzania Field Epidemiology and Laboratory Training Programme (TFELTP), Ministry of Health, P.O. Box 743, Dodoma, Tanzania
&Corresponding author: Sephord Saul Ntibabara, Department of Epidemiology and Biostatistics, Muhimbili University of Health and Allied Sciences, P.O.Box 65001, Dar es Salaam, Email: sesantiro@gmail.com, ORCID: https://orcid.org/0009-0001-4487-512X
Received: 15 May 2025, Accepted: 10 Jan 2026, Published: 20 Jan 2026
Domain: Non-communicable Disease Epidemiology
Keywords: Hypertension, prevalence, community, survey, Tanga
©Sephord Saul Ntibabara et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Sephord Saul Ntibabara et al., Hypertension prevalence and associated factors among adults in Tanga region, 2023: A community-based cross-sectional survey. Journal of Interventional Epidemiology and Public Health. 2025; 9(1):13. https://doi.org/10.37432/jieph-d-25-00121
Introduction: Hypertension remains a leading cause of cardiovascular disease globally. Tanzania reported 25% prevalence in 2020, but recent surveys indicate 30%-35%. This study determined hypertension prevalence and associated factors in the Tanga region to inform NCD interventions.
Methods: A community-based cross-sectional survey used WHO STEPS methodology across Tanga City, Muheza, and Mkinga districts (N=1818). Data on demographics, lifestyle, family history, and antihypertensive use were collected via standardized questionnaire. Prevalence was calculated descriptively; modified Poisson regression estimated adjusted prevalence ratios (APR) with robust standard errors. Significance was P<0.05 (95% CI).
Results: Hypertension prevalence was 37.7% (95%CI: 35.5-40.0%). Among hypertensives, 65.6% (450/686) were not aware of their hypertension status. In multivariable modified Poisson regression, older age increased hypertension risk: 45-54 years (APR= 2.07, 95%CI: 1.48-2.89), 55-64 years (APR =2.18, 95%CI: 1.54-3.07), and ≥65 years (APR= 3.00, 95%CI: 2.13-4.23) versus <25 years. Male sex (APR= 1.20, 95%CI: 1.05-1.37), urban residence (Muheza: APR= 1.24, 95%CI: 1.01-1.52; Tanga CC: APR= 1.47, 95%CI: 1.24-1.75), overweight (APR =1.62, 95%CI: 1.18-2.21), obesity (APR =1.79, 95%CI: 1.32-2.43), and family history (APR =1.13, 95%CI: 1.01-1.27) were significant risk factors. Physical exercise was protective (APR =0.89, 95%CI: 0.79-0.99).
Conclusion: Hypertension prevalence exceeds national estimates, with poor screening and treatment adherence. Urban residence, male sex, advanced age, and obesity increase risk; exercise protects. Ministry of Health and its stakeholders must prioritise community screening, especially in urban areas, reinforce antihypertensive adherence through education, and promote physical activity to curb the NCD burden.
Annually, non-communicable diseases (NCDs) contribute to about 41 million deaths worldwide. This burden is equivalent to 74% of all fatalities [1,2]. Among all deaths, 77% are in low and middle-income countries [2–4]. It is estimated that 80% of all premature deaths are from chronic NCDs such as cardiovascular diseases, malignancies, chronic respiratory diseases, and diabetes [3–6]. Recent studies have shown that the age group of starting from 40 years and above is the most affected in developing countries [7]. About 33% of all deaths in Tanzania each year are due to NCDs, of which cardiovascular diseases account for 12%, followed by cancer 7%, chronic respiratory diseases 7%, and diabetes 2% [7, 8]. The NCDs have major impacts on communities ranging from the nations, households, and individual economies by affecting younger age groups and causing longer disease durations, untimely deaths, and lost productivity [2,3]. The 2016-2020 national non-communicable strategic plan for Tanzania revealed that CVDs contribute to 12% deaths [9]. In Tanzania, the prevalence of hypertension is increasing and was about 25% by 2020 [10]. Moreover, hypertension patterns, like other NCDs, are rapidly changing. Studies done in Tanzania show an even distribution of hypertension among all groups of individuals with different economic status [11, 12]. Moreover, the young aged 34 to 44 years were revealed to be hypertensive for about 30% of the population [11]. We conducted this survey in the Tanga region due to a unique demographic and lifestyle patterns such as urbanisation, dietary habits and healthcare access, which warrant region-specific data to guide interventions. Since hypertension is highly associated with a wide range of CVDs, stringent and reliable surveys on its risk factors should be conducted to obtain relevant information for CVD prevention and management planning. We therefore conducted a survey to determine the community-based prevalence and risk factors associated with hypertension among adults in the Tanga region.
Study design and setting
The study design was a community-based cross-sectional survey to assess the hypertension prevalence and possible factors that could be associated with it in the Tanga region, Tanzania. A survey was carried out in January 2023, in the three selected district councils out of the 11 districts, which were Muheza District, Mkinga District, and Tanga City Councils. Tanga is among 31 regions of Tanzania, bordered to the north by Kenya and the Kilimanjaro region; to the south by the Pain and Morogoro regions; to the west by Manyara; and to the east by the Indian Ocean. The region covers an area of 26,667 km2 [13].
Sample size and sampling procedures
The sample size was calculated by using the single-proportion population formula. The sample size was calculated at 95% CI (z =1.96) on the basis of a 5% margin of error, an estimated prior national prevalence of hypertension of 41% [14]. The sample size was calculated using the formula below:
$$ S = \frac{Z^2 \times P(1 – P)}{e^2} $$
$$ S = \frac{1.96^2 \times 0.41(1 – 0.41)}{0.05^2} = 1633 $$
Where: S=Sample size, P=Prevalence and e=Standard error
Then the final sample size was 1633 individuals. Using probability proportional to size, the minimum number of participants to be recruited from the districts was determined to be: Tanga City -1000, Mkinga – 350 and Muheza – 350. Calculation of number of participants to be recruited from each council was based on the national population census report (2022) proportion [13].
A multistage cluster sampling technique was employed, where for the first stage, a random sample of three district councils was selected by simple random sampling out of eleven district councils found in the Tanga region. In the second stage, ten wards were selected in every district council. In the third stage, three villages or streets were selected in each ward. In the fourth stage, participants were recruited by considering the proportion to size of the village or street based on population density using simple random sampling. The list of all house-holds in a street (sampling frame) was obtained where eligible members of the house-hold (not more than three) were recruited.
Inclusion and exclusion criteria
Participants who were adults aged 18 years and older, residents of the study district councils for not less than three months, were eligible to be enrolled. We excluded participants who were unable to offer informed consent. Women who reported being pregnant, patients who are critical and or mentally ill individuals were excluded from our survey.
Variables and their measurements
Blood pressure was measured using a calibrated digital sphygmomanometer after 5 minutes of rest in the sitting position, with three readings taken and the average of the two closest used. Hypertension was defined as systolic blood pressure ≥140 mmHg or diastolic pressure ≥90 mmHg per Tanzania Standard Treatment Guidelines. Hypertensive participants received counselling and referral to nearby health facilities. Body weight (kg) was measured on a calibrated scale placed on a flat surface after removing heavy clothing; height (m) was measured standing upright using a stadiometer. BMI was calculated as weight/height² and categorised as underweight (<20 kg/m²), normal (20-24.9 kg/m²), overweight (25-29.9 kg/m²), or obese (≥30 kg/m²) [16]. Smoking was defined as current use (daily or occasional) of tobacco products. Alcohol use included daily or occasional consumption (abstainers reported none). Fruit intake was daily (≥1 fruit), occasional, or never; vegetable intake was daily (≥2 servings), occasional, or never.
Data collection and analysis
Data collection was done through the Kobo Collector Toolbox application loaded on Android tablets. A standardised STEPwise questionnaire for NCDs surveillance from WHO was adopted, which included demographic information, information on associated risk factors for hypertension, blood pressure and body mass index measurements [16]. During analysis, data were cleaned by using Microsoft Excel version 2013. Frequencies and proportions for categorical variables, the interquartile range (IQR), and the median for continuous variables were descriptively analyzed. Chi square tests for binary and categorical variables were done to ascertain significance differences in proportions based on hypertension status. Bivariable and multivariable modified Poisson regression was used to ascertain the relationship between independent factors and hypertension. When performing the bivariable analysis p-value of < 0.20 was used to ascertain variables to be included in the multivariable analysis. Variables which had no collinearity were included in the multivariable model. Throughout the study, a significance level was ascertained when p value was less than 0.05 at the 95% confidence Interval.
Ethical considerations
The Ministry of Health’s Ethics Review Committee, under its institutional review board (Muhimbili University of Health and Allied Sciences) waived the requirement for formal ethics approval. This study poses minimal risk to participants, does not involve sensitive personal data, it was part of the national campaign to monitor the trend of Cadio-vascular diseases (CVDs). Only de-identified data were collected from participants. It was conducted following the revised Declaration of Helsinki concerning biomedical research involving human participants. Participants were fully informed about the study’s aims and benefits, and oral consent was obtained from both participants who voluntarily agreed to participate. Additionally, participants found to have high blood pressure were referred to nearby health facilities for further care. All authors have agreed to the publication of this manuscript. The final report was shared with the local authorities for action based on the study findings and their corresponding recommendations.
Participants’ social demographic characteristics
A total of 1818 adults in Tanga the aged starting from 18 years and older, were enrolled. The final sample size had 118 increased number from the calculated sample size of 1700 participants. We recruited proportionally across councils: Tanga City (1097/1818, 60.3%), Mkinga (357/1818, 19.6%), and Muheza (564/1818, 20.0%), while maintaining probability proportional to size using 2022 census data. The median age (IQR) was 41 (30-52) years of whom 1231 (67.7%) were males. Among age groups, majority (442 /1818, 24.3%) were of age between 35 to 44 years. Among all participants, more than half of them, 1145 (63.0%) had at least a primary school education, with very few, 165 (9.1%), who did not have any formal education. The majority, 1239 (68.2%), were married. On employment, 1369 (75.3%) were self-employed, with only 111 (6.1%) working for the government (Table 1).
Prevalence of hypertension by their characteristics
The survey revealed a prevalence of hypertension of 37.7% (686/1818),95%CI: 35.5 to 40.0). The study shows that there was an increase in hypertension among participants as their age was increasing where by prevalence was high (106/164, 64.6%, 95% CI: 57.0 to 71.6) among individuals were of 65years and above. Males had relatively high prevalences than women (475/1231, 38.6% 95% CI; 35.9-41.3). Individuals who were either widowed or widower had highest prevalence (54/95, 56.8% 95% CI: 46.7 to 66.4) among other marital status categories. Individuals who had no habit of doing physical exercises at least 30 minutes a day had a relative higher prevalence (388/974, 39.8% 95%CI: 36.8 to42.9) of hypertension unlike those who do exercises. The prevalence of individuals who had family history of hypertension was higher (266/632, 42.1% 95%CI: 38.3 to 46.0) compared to individuals who had no family history of hypertension (Table 1).
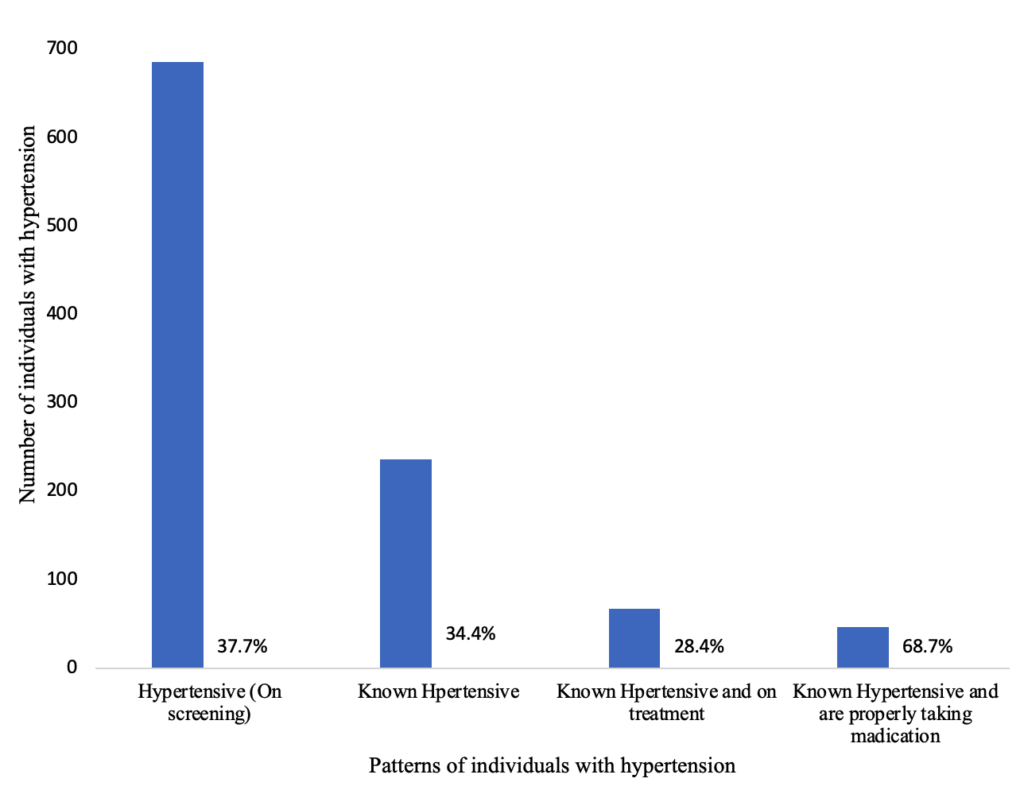
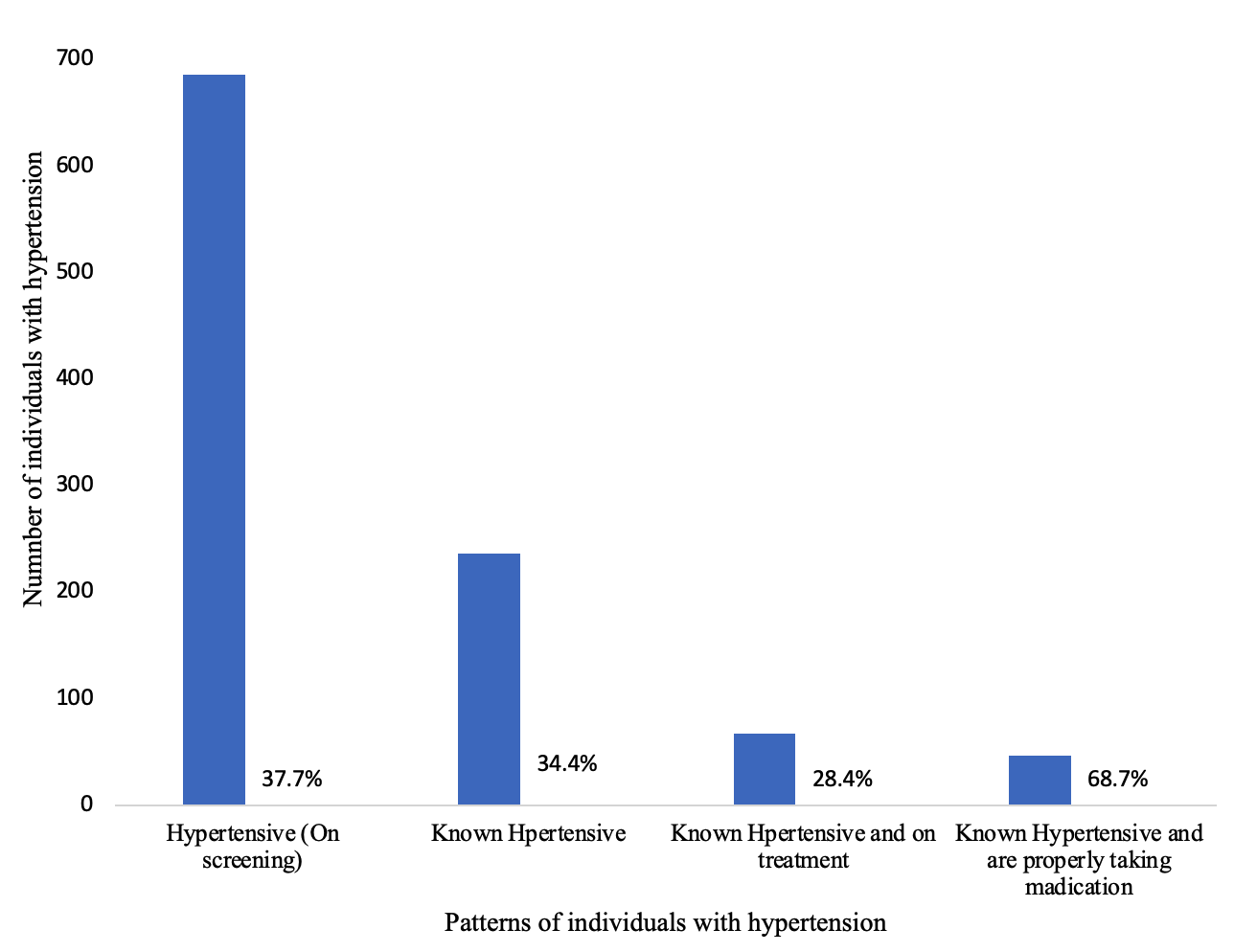
Patterns of hypertension and anti-hypertensive medication use among participants.
We found that out of 686/1818 (37.7%) participants who were diagnosed with hypertension, only 236/686 (34.4%) were previously diagnosed and were aware that they had hypertension. This shows that 450/686 (65.6%) of the hypertensive individuals did not know if they had hypertension. Moreover, among the known individuals who are hypertensive, only 67/236 (28.4%) were on medication. On assessing if those who are on medication are adhering to the instructions, we found that 46/67 (68.7%) reported having been using anti-hypertensive medication for the past two weeks (Figure 1).
Risk Factors Associated with Hypertension
In the multivariable modified Poisson regression analysis, several factors were independently associated with hypertension prevalence among 1818 participants. Compared to those aged <25 years, individuals aged 45–54 years (APR = 2.07; 95%CI: 1.48–2.89), 55–64 years (APR = 2.18; 95%CI: 1.54–3.07), and ≥65 years (APR = 3.00; 95%CI: 2.13–4.23) were approximately twice to threefold more likely to have hypertension. Each additional year of age increased the prevalence by 2% (APR = 1.02; 95%CI: 1.02–1.03). Males were likely at risk of being hypertensive as compared to females (APR = 1.20; 95%CI: 1.05–1.37). Individuals living in Muheza (APR= 1.24, 95%CI: 1.01–1.52) and Tanga city council (APR=1.47, 95%CI: 1.24–1.75) were likely to have higher prevalence compared to those in Mkinga.. Individuals who are overweight (APR= 1.62, 95%CI: 1.18–2.21) and obese individuals (PR: 1.79, 95%CI: 1.32–2.43) were likely to be hypertensive compared to underweight participants. Individuals who were exercising were likely to be protected from becoming hypertensive compared to those who were not performing exercises (APR=0.89, 95%CI: 0.79–0.99). Individuals with a family history of hypertension had a 13% higher risk compared to those without (APR = 1.13; 95%CI: 1.01–1.27) (Table 2).
There was a high prevalence of hypertension among adults in Tanga, where more than two-thirds of the diagnosed patients were unaware they had hypertension. The majority of patients with known hypertension status were not properly taking anti-hypertensives as directed by the healthcare provider. Risk factors that were likely to be associated with hypertension include: being male gender, having old age, being obese and living in an urban area. Exercise was revealed to likely be a protective factor against hypertension.
Prevalence of hypertension in Tanga Region
The hypertension prevalence that was found in the survey was higher than 26%, which was found in the Tanzania national steps survey of 2012 [1], together with other studies done in different time periods in similar settings of Tanzania [11,12,15,16]. The differences could be life patterns change from the last national survey up to the time of this survey, and differences in cultural and geographical settings with less risk exposures, such as rural environment [16]. The hospital-based prevalence done in Morogoro region (Tanzania) revealed a higher prevalence of hypertension than that reported by this study [17]. This difference could be the fact that other diseases are linked with hypertension, such that patients with other chronic diseases, such as cardiovascular diseases and diabetes, are likely to have hypertension, therefore conducting a study among patients is likely to have high prevalences. Moreover, risk factors of hypertension have significantly increased due to an increase in technological advancements, which lead to changes in lifestyles such as sedentarism. Despite policy improvements in hypertension screening, implementation remains inadequate, as evidenced by the substantial proportion of undiagnosed cases in our study [10]. The observed prevalence was also higher than the one reported in Arusha and Kisarawe in 2018 [2].
Anti-hypertensive use pattern among patients with hypertension
Our studies revealed that only one-third of individuals who were found to be hypertensive were on anti-hypertensive medication. This finding is similar to the WHO report on Africa, which indicates that more than two-thirds of individuals with hypertension are not on antihypertensives [18]. This finding is very similar to most of the studies conducted in Africa [11, 19]. The reason can be the low availability of screening services in our settings and the high cost of drugs, which can influence many individuals not to afford them [9, 19].
Risk factors of hypertension
From our study, men were likely to be hypertensive, unlike women. The finding was similar to other studies which were conducted in Nairobi [3,4]. This can be due to the fact that the majority of men from Tanga are not engaged in strenuous jobs, which exposes them to the risk of sedentarism, unlike women who have to work every day to find a meal for a home, as it is their culture. Different finding was obtained from a study where it was shown that women were at risk of becoming hypertensive, unlike men [11]. This can be due to the nature of participants, where the study involved young adult men, of whom the majority are active, and so they engage in strenuous tasks. The high proportion of women in the study reflects the gender distribution in the Tanga region according to the 2022 national census, which reported more women than men [14]. Additionally, data collection occurred during the daytime when most men were at work, while women were more likely to be at home. Individuals residing in urban areas in this survey (Tanga City) were found to be higher compared to those who are living in rural areas (Mkinga District). The findings in this survey were similar to other Surveys done by Stanifer et al in Northern Tanzania, who reported a prevalence of raised blood pressure of 30.6% for urban and 19.1% for rural settings [11, 12].
In our survey, as the age advances the likelihood of hypertension increases even higher in the age group above 65 years. However, it was found the age group above 45 years was likely to be hypertensive. Studies conducted in Ethiopia and Tanzania they both reported an increased likelihood of hypertension as age was increasing [11,12,14]. The main possibility for this observed phenomenon can be explained by physiological changes which happen as someone ages, resulting in an increase in the stiffness of blood vessels [12].
Our survey revealed an association between BMI and risk of becoming hypertensive, a finding that concurs with eight surveys conducted in urban Varanasi in India [9]. This survey indicates that physical activity (exercise) has a protective effect against the risk of hypertension. Studies have reported the effects of increased BMI as a risk for hypertension. This is because the increase in hypertension is a lead of excess body fat of which affects blood vessels by narrowing the rumen and hence finally leads to hypertension. Participants who engaged in physical activities had reduced risk of getting hypertension unlike those who did not engage in physical activities. This is because WHO recommend that about 150 minutes of physical activities is recommended to keep a man in good health [15]. Physical activities are proven to contribute to the reduction of the risk of hypertension because it facilitates fat metabolism and weight reduction, which are modifiers of hypertension. Moreover, physical exercise enhances renal function and sodium excretion, and hence it improves kidney function and lowers blood volume, which eventually lowers the blood pressure [20]. A study done among African ancestry men shows that with every increase in light physical activity in replacing sedentary behaviours, the risk of hypertension decreases by 12% [21].
Our survey reports that living in urban areas is at high risk of becoming hypertensive. This can be due to exposure to sedentary activities for most time of the day [17]. Similar finding has been revealed in a multi-country study conducted in Tanzania and Uganda, where individuals residing in urban areas were likely to be hypertensive [8]. The urbanisation and digital life could be one of the key reasons, unlike in rural areas where the majority are not using a digitalized materials and are engaged with strenuous works unlike in urban areas, where the majority of basic needs are obtained online.
Our study found that individuals with a family history of hypertension had an increased risk (APR 1.13, 95% CI 1.01-1.27). This aligns with findings from China reporting fourfold odds and Sri Lanka showing 1.26 times higher risk, likely [22-23]. This can be due to genetic predisposition among relatives [24].
Strengths and limitations of the study
This study has a number of limitations. First, recruiting participants in public places (markets, bus stands) may under-represent housebound individuals or those with limited mobility, introducing selection bias. Second, the cross-sectional nature of this study limits causal inferences; it captures association but not directionality or causation of risk factors. Third, Variables like diet, smoking, and physical activity may suffer from recall or social desirability bias, affecting their accuracy. Fourth, pregnant women and critically or mentally ill individuals were excluded to ensure the generalizability of findings to those subgroups. Fifth, we did not reach all districts of the region so the results might not be generalizable to all urban and rural areas of Tanga region. Sixth, we also did not assess information on caffeine consumption; literature shows that caffeine consumption is associated with blood pressure.
The strength of this study is that we recruited a large number of study participants, and hence it gives it a large statistical power. Repeated blood pressure measurement favours the validity of blood pressure readings. Consideration of collecting data in both urban and rural settings gives the ability to assess both experiences if they are linked to hypertension.
The survey reports a high hypertension prevalence in Tanga. The associated risk factors for hypertension observed were male, older age (≥70 years) and obesity. Regular screening of hypertension should be emphasized in the societies including rural settings. Health workers health activists should strengthen awareness and education to patients on the importance of proper taking of anti-hypertensives. Exercise was the only preventive measure for hypertension, therefore, practicing physical activities is recommended for the general population as it have been proven to have a protective effect.
What is already known about the topic
What this study adds
This work has been supported by the United States President’s Emergency Plan for Aids Relief (PEPFAR) through Mzumbe University under the Centres for Disease Control and Prevention (CDC). The opinions expressed are those of the authors, as the funders were not directly involved with the work.
All authors made a significant contribution to the work reported. The following; S.S. Ntibabara, P.R. Torokaa, G.H. Mfuru, E.B. Ngoli, T. Bollen, R.M. Mashauri, D.J. Osima, F.M. Juma, F.D. Ng’ida, F.S. Masalu, G.A. Massawe, K. Shamte, N.M. Josaphat, J. Kimambo, M. Monah, M.M. Ramadhani, A.F. Njau, H. Nyigo, J.N. Allan, J. Masatu were involved in the conception, study design, execution, acquisition of data, analysis and interpretation in all these areas including drafting the drafts, and the following ; L. Urio, E. Bukundi, M. Mizinduko, A.K. Hussein were revising and critically reviewing the article and gave final approval of the version to be published.
| Characteristic | Total (%) | Hypertensive n (%) | 95% Confidence Interval |
|---|---|---|---|
| Age (years) | |||
| Below 25 | 237 (13.0) | 53 (22.4) | 17.5–28.1 |
| 25–34 | 372 (20.5) | 101 (27.2) | 22.9–32.0 |
| 35–44 | 442 (24.3) | 142 (32.1) | 27.9–36.6 |
| 45–54 | 378 (20.8) | 176 (46.6) | 41.6–51.6 |
| 55–64 | 225 (12.4) | 108 (48.0) | 41.5–54.5 |
| 65 and above | 164 (09.0) | 106 (64.6) | 57.0–71.6 |
| Gender | |||
| Male | 1231 (67.7) | 475 (38.6) | 35.9–41.3 |
| Female | 587 (32.3) | 211 (36.0) | 32.2–39.9 |
| Education | |||
| Primary | 1145 (63.0) | 434 (37.9) | 31.5–40.7 |
| Secondary | 401 (22.1) | 139 (34.7) | 30.2–39.5 |
| University/College | 107 (06.0) | 41 (38.3) | 29.6–47.8 |
| No formal | 165 (09.1) | 72 (43.6) | 36.3–51.3 |
| Marital status | |||
| Married | 1239 (68.2) | 487 (39.3) | 36.6–42.1 |
| Single | 374 (20.6) | 100 (26.7) | 22.5–31.5 |
| Widow/Widower | 95 (5.2) | 54 (56.8) | 46.7–66.4 |
| Divorced | 110 (6.1) | 45 (40.9) | 32.1–50.3 |
| Occupation | |||
| Government employed | 111 (6.1) | 43 (38.7) | 30.1–48.1 |
| Private employed | 163 (9.0) | 55 (33.7) | 26.9–41.3 |
| Self employed | 1369 (75.3) | 519 (37.9) | 35.4–40.5 |
| Unpaid employed | 175 (9.6) | 69 (39.4) | 32.5–46.9 |
| Residence | |||
| Muheza | 364 (20.0) | 133 (36.5) | 31.7–41.6 |
| Mkinga | 357 (19.6) | 120 (33.6) | 28.9–38.7 |
| Tanga City | 1097 (60.3) | 433 (37.7) | 36.6–42.4 |
| BMI | |||
| Underweight | 137 (7.5) | 34 (24.8) | 18.3–32.7 |
| Normal | 542 (29.8) | 148 (27.3) | 23.7–31.2 |
| Overweight | 421 (23.1) | 181 (43.1) | 38.4–47.9 |
| Obese | 719 (39.6) | 323 (44.9) | 41.3–48.6 |
| Smoking | |||
| Yes | 316 (17.4) | 106 (33.5) | 30.9–37.3 |
| No | 1502 (82.6) | 580 (38.6) | 36.1–41.6 |
| Alcohol | |||
| Yes | 279 (15.4) | 102 (36.6) | 31.1–42.4 |
| No | 1539 (84.7) | 584 (37.9) | 35.6–40.4 |
| Exercise | |||
| Yes | 844 (46.4) | 298 (35.3) | 32.2–38.6 |
| No | 974 (53.6) | 388 (39.8) | 36.8–42.9 |
| Eating Fruits | |||
| Yes | 1728 (95.1) | 657 (38.0) | 35.8–40.4 |
| No | 90 (5.0) | 29 (32.2) | 23.4–42.5 |
| Eating Vegetables | |||
| Yes | 1729 (95.1) | 650 (37.6) | 35.3–39.9 |
| No | 89 (4.9) | 36 (40.4) | 30.8–50.9 |
| Family History of HTN | |||
| Yes | 632 (34.8) | 266 (42.1) | 38.3–46.0 |
| No | 1186 (65.2) | 420 (35.4) | 32.7–38.2 |
| Characteristic | Total n (%) | Prevalence of HTN n (%) | Crude prevalence ratio (95% CI) | Adjusted prevalence ratio (95% CI) |
|---|---|---|---|---|
| Age groups | 1.02 (1.01–1.02) | 1.02 (1.02–1.03) © | ||
| Below 25 | 237 (13.0) | 53 (22.4) | Ref | Ref |
| 25–34 | 372 (20.5) | 101 (27.2) | 1.21 (0.91–1.62) | 1.17 (0.85–1.62) |
| 35–44 | 442 (24.3) | 142 (32.1) | 1.43 (1.09–1.89) | 1.38 (0.99–1.94) |
| 45–54 | 378 (20.8) | 176 (46.6) | 2.08 (1.60–2.70) | 2.07 (1.48–2.89) |
| 55–64 | 225 (12.4) | 108 (48.0) | 2.14 (1.63–2.82) | 2.18 (1.54–3.07) |
| 65 and above | 164 (09.0) | 106 (64.6) | 2.89 (2.22–3.76) | 3.00 (2.13–4.23) |
| Gender | ||||
| Male | 1231 (67.7) | 475 (38.6) | 1.02 (0.98–1.05) | 1.20 (1.05–1.37) |
| Female | 587 (32.3) | 211 (36.0) | Ref | Ref |
| Education | ||||
| No formal | 165 (09.1) | 72 (43.6) | Ref | Ref |
| Primary | 1145 (63.0) | 434 (37.9) | 0.87 (0.72–1.05) | 1.01 (0.83–1.22) |
| Secondary | 401 (22.1) | 139 (34.7) | 0.79 (0.64–0.99) | 1.06 (0.84–1.34) |
| University/College | 107 (06.0) | 41 (38.3) | 0.88 (0.65–1.18) | 1.06 (0.78–1.44) |
| Marital status | ||||
| Married | 1239 (68.2) | 487 (39.3) | 0.98 (0.92–1.06) | 0.94 (0.75–1.18) |
| Single | 374 (20.6) | 100 (26.7) | 0.89 (0.83–0.97) | 1.02 (0.75–1.42) |
| Widow/Widower | 95 (5.2) | 54 (56.8) | 1.11 (1.01–1.21) | 1.20 (0.90–1.60) |
| Divorced | 110 (6.1) | 45 (40.9) | Ref | Ref |
| Occupation | ||||
| Government employed | 111 (06.1) | 43 (38.7) | Ref | Ref |
| Private employed | 163 (09.0) | 55 (33.7) | 0.96 (0.88–1.05) | 1.14 (0.82–1.58) |
| Self employed | 1369 (75.3) | 519 (37.9) | 0.99 (0.92–1.06) | 1.19 (0.92–1.55) |
| Unpaid employed | 175 (09.6) | 69 (39.4) | 1.00 (0.92–1.09) | 1.28 (0.94–1.76) |
| Residence | ||||
| Mkinga | 357 (19.6) | 120 (33.6) | Ref | Ref |
| Muheza | 364 (20.0) | 133 (36.5) | 1.02 (0.97–1.07) | 1.24 (1.01–1.52) |
| Tanga CC | 1097 (60.3) | 433 (37.7) | 1.04 (1.00–1.08) | 1.47 (1.24–1.75) |
| BMI | ||||
| Underweight (<20) | 137 (07.5) | 13 (23.64) | Ref | Ref |
| Normal (20–24.9) | 542 (29.8) | 231 (27.60) | 1.10 (0.80–1.52) | 1.05 (0.77–1.45) |
| Overweight (25–29.9) | 421 (23.1) | 242 (43.06) | 1.74 (1.27–2.37) | 1.62 (1.18–2.21) |
| Obese (30 and above) | 719 (39.6) | 200 (54.95) | 1.81 (1.34–2.45) | 1.79 (1.32–2.43) |
| Family history of hypertension | ||||
| Yes | 632 (34.8) | 266 (42.09) | 1.04 (1.01–1.08) | 1.13 (1.01–1.27) |
| No | 1186 (65.2) | 420 (35.41) | Ref | Ref |