Lesson from the field | Open Access | Volume 9 (1): Article 35 | Published: 25 Feb 2026

Views: 2,254
Menu, Tables and Figures
Joshua Kwabena Aniaku1,&, George Akowuah2, Geoffrey Delali Komla Gone3, Moses Barima Djimatey4
1Chereponi District Health Directorate, Ghana Health Service, North East Region, Ghana, 2Ghana Field Epidemiology and Laboratory Training Programme, University of Ghana, Accra, Ghana, 3Sagnarigu Municipal Health Directorate, Ghana Health Service, Northern Region, Ghana, 4North East Regional Health Directorate, Ghana Health Service, North East, Ghana
&Corresponding author: Joshua Kwabena Aniaku, Chereponi District Health Directorate, Ghana Health Service, North Region, Ghana, Email: joshuaaniaku@yahoo.com ORCID: https://orcid.org/0000-0001-6257-5297
Received: 21 Apr 2025, Accepted: 23 Feb 2026, Published: 25 Feb 2026
Domain: One Health
Keywords: One Health, Rabies, Post-exposure prophylaxis
©Joshua Kwabena Aniaku et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Joshua Kwabena Aniaku et al. Averting human rabies transmission using One Health approach in a rural community in northeast Ghana. Journal of Interventional Epidemiology and Public Health. 2026; 9(1):35. https://doi.org/10.37432/jieph-d-25-00097
This case report explores the implementation of a One Health approach to avert human rabies transmission in a rural community in the North East Region of Ghana, specifically within the Chereponi District. Rabies, a severe zoonotic disease predominantly transmitted by domestic dogs, poses a significant public health risk, particularly in underserved areas. The report highlights a specific incident involving a dog bite on a four-year-old boy, detailing the swift response by health authorities and the effective use of Integrated Bite Case Management (IBCM). Despite the challenges of weak surveillance and community awareness, the collaborative efforts between the District Health Directorate, Veterinary Services, and local health facilities facilitated prompt post-exposure prophylaxis for the child. This case emphasises the critical role of a One Health framework in enhancing rabies detection and prevention, advocating for increased dog vaccination and community education as vital preventative measures against rabies in rural settings. The findings underscore the importance of multi-sectoral collaboration in addressing zoonotic diseases and improving public health outcomes.
This report details a successful intervention in Ghana’s Chereponi District that averted a potential human rabies death. We present the case of a four-year-old boy in a remote community who sustained a category-three bite from a stray dog. Through an activated Integrated Bite Case Management (IBCM) protocol, the human health sector conducted an immediate risk assessment, requested post-exposure prophylaxis (PEP) via a regional One Health platform, and facilitated its delivery by drone to the clinic within hours. Concurrently, the veterinary sector investigated the dog, which the community had euthanised, and laboratory testing confirmed rabies. The child received his first vaccine dose within 24 hours of the report, completed the full PEP schedule, and remained healthy upon follow-up. This case demonstrates a practical model of prevention.
Rabies remains a fatal zoonotic disease targeted for elimination in Ghana, yet the country faces significant challenges, including weak surveillance systems and difficulty accessing reliable data [1]. Although preventable through timely PEP, rabies continues to pose a serious public health threat, with domestic dogs responsible for 99% of human transmissions [2,3]. The World Health Organisation (WHO) estimates the disease causes approximately 59,000 human deaths annually worldwide[3].
The One Health approach, emphasising cross-sectoral collaboration, is recognised as essential for controlling zoonotic diseases like rabies [4,5]. However, implementing it effectively at the local level is often hampered by challenges such as fragmented coordination, weak infrastructure, and a lack of information sharing [6,7]. In response, the North East Region of Ghana in the year 2022 intensified dog bite surveillance and adopted a collaborative One Health framework, with IBCM as a key component. This has led to an increase in the number of recorded dog bite cases. For instance, the Chereponi district recorded 6, 7, and 27 dog bites in 2022, 2023, and 2024, respectively, a marked increase following strengthened efforts.
Unlike most rabies case reports that describe fatal outcomes [8], this report highlights a replicable example of successful prevention. Our objective is to demonstrate how proactive surveillance, guaranteed PEP supply, and structured intersectoral coordination under a One Health framework can directly prevent rabies mortality in rural, resource-limited settings.
The Chereponi District is in the eastern part of the North East Region of the Republic of Ghana. It covers a land area of about 1,080 sq km and shares boundaries with four neighbouring districts. To the east is the Oti District of the Republic of Togo; to the west is the Gushegu District; to the north is the Yunyoo-Nasuan District; and to the south is the Saboba District. There are five subdistricts and 206 communities. The 2021 population of the district stood at 87,176 [9]. Many communities become difficult to reach, while others are completely cut off during rainy seasons due to floods. The area is multi-ethnic with Anofo (Chokosi) constituting the majority.
The district has one government hospital located in the district capital, two health centres, and thirteen community-based health planning and services (CHPS) compounds. A CHPS compound in the Ghana Health Service structure is the main health facility that exists, especially in rural communities, to provide primary health care services. The major occupation of the people in the district is farming and petty trading. Dogs are kept as pets and for security and hunting purposes. The district has a One Health team which comprises the Disease Control and Surveillance Unit (DCSU), Veterinary Service Department (VSD) and Environmental Health Unit. These units work collaboratively to carry out surveillance activities and outbreak investigations in the district.
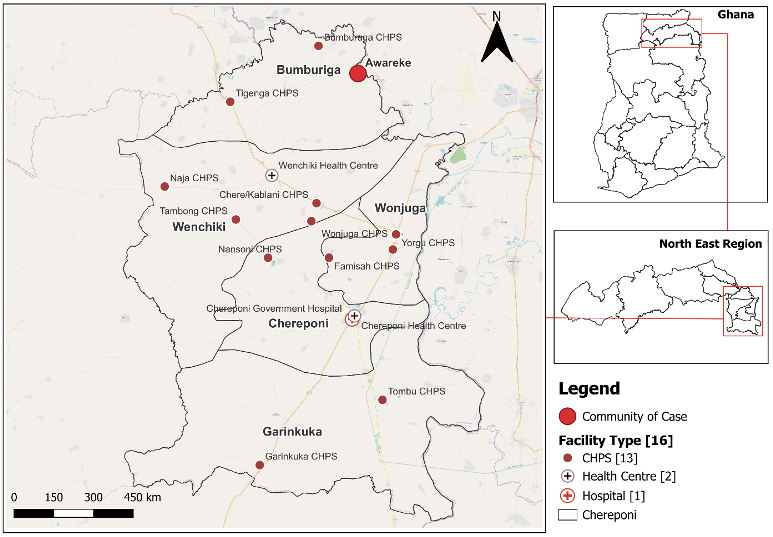
The dog bite occurred in the Awareke community, which is in the Bumburuga sub-district of the Chereponi District. The community has a population of 487 and has no health facility. The closest health facility is the Bumburuga CHPS, which is over 5 kilometers in distance (Figure 1).
Ethical considerations
Ethical Approval: This case report is derived from routine public health surveillance and outbreak response activities conducted by the Chereponi District Health Directorate and its One Health partners. The activities described, including case investigation, sample collection for rabies diagnosis, and the administration of post-exposure prophylaxis, are standard procedures mandated by Ghana’s technical guidelines for Integrated Disease Surveillance and Response (IDSR) and do not constitute a research study on human subjects. Therefore, formal institutional ethical review board approval was not required for this descriptive account of a public health intervention.
Informed Consent: Verbal informed consent was obtained from the child’s parents for all medical procedures, including wound management and the administration of the rabies vaccine series. Given that this report involves a minor, written informed consent for the publication of the de-identified case details was also obtained from the parents. They were informed of the purpose of the publication, to share a successful public health practice for educational purposes, and assured of the complete anonymity of the child.
Data Confidentiality and Anonymity: All patient data were collected and handled in strict confidence by the District Disease Control and Surveillance Unit. In this manuscript, all personal identifiers have been removed. The case is described using non-identifiable demographic information (age, sex). The community name is provided as it is relevant to understanding the remote operational context, but no family or household details are disclosed.
On 26th October, 2024, the Disease Control and Surveillance Unit (DCSU) of the Chereponi District Health Directorate received a phone call from the Bumburuga CHPS about a dog attack. The incident occurred in Awareke, a rural community in the Bumburuga Sub-district. The case involved a four-year-old boy who sustained bites from a dog on his lower back. The dog involved was a stray dog with an unknown vaccination history against rabies. The incident occurred when two brothers, aged four and ten, were sent on an errand in the afternoon. The dog attacked the brothers unprovoked and overpowered the younger brother because he could not outrun the dog. The children reported the incident to their parents, who then brought the bitten child to the Bumburuga CHPS compound.
On assessment at the health facility, the boy had sustained a category three bite, which showed wounds and bleeding from the bite site. Details of the child were captured, and the wound was washed with water and soap. The attending clinician then reported the case to the DCSU on the next course of action in managing the case. Detailed information about the circumstances of the bite was obtained from the clinician by the unit. The unit then supported the facility to fill in an IBCM form and informed the Veterinary Officers about the event.
Within 30 minutes of receiving the report, the DCSU decided there was a need for the child to be given the rabies post-exposure prophylaxis (PEP) due to the circumstances of the bite. This decision was based on the initial report from the facility, which indicated that the dog was a stray and that the bite was category three. An anti-rabies vaccine was requested by the unit through the Regional One Health WhatsApp platform at the regional level. The request was approved by the Deputy Director of Public Health of the North East Region, and four vaccine vials were dispatched by Zipline Vobsi through their drone delivery service to the District Health Directorate on the evening of the same day. The vaccines were then transported to the Bumburuga CHPS facility the next day for the child to receive his first dose on 27th October 2024. The disease surveillance officer kept monitoring the progress of the vaccination of the child based on the WHO-approved vaccination schedule (whole vial intramuscular doses on days 0, 3, 7 and 14) [10].
The next day, the VSD investigated the incident, and reports from the community indicated that the dog looked sick with visible signs of diarrhoea. This influenced the community’s decision to mobilise and euthanise the dog. The clinician requested the head of the canine for laboratory investigations, and the carcass was buried. The clinician transported the sample in a triple packaging system to the DCSU at the district level, and the sample was stored in a sample refrigerator. On 28th October, the veterinary officer transported the sample to the Central Veterinary Laboratory at Pong-Tamale, which is accredited to run rabies investigations. The laboratory carried out a fluorescent antibody test on the sample and sent the test result on the same day to the Regional One Health Platform, which was positive for rabies. The veterinary officer further alerted the DCSU at the district of the outcome of the sample. The unit also informed the facility through a phone call. The child was monitored for between one and three months and has shown no signs or symptoms of rabies and is in good health.
This case report highlights the improvement and consequential effects of rabies surveillance in the Chereponi District. Rabies disease is described as a neglected tropical disease and affects rural communities more than urban communities[11]. The disease mostly affects poor persons living in rural communities, of which Chereponi District is not an exception. The dog bite incident occurred in one of the remote parts of the district. When it comes to dog bites, people in the district have good health-seeking behaviour. They often visit the nearest health facility when they are bitten by a dog. This is often because of the need to dress their wounds and not because of the possible exposure to rabies and the need for vaccination. The danger here is that people are likely to ignore scratches or small wounds which have the potential to result in human rabies. Other studies have also extensively highlighted the lack of knowledge and understanding of rabies as reasons why people do not seek care when bitten by a dog[12, 13].
One preventive measure for rabies is to wash wounds with soap, which was done at the health facility. In other jurisdictions, rabies has almost been eliminated as a consequence of massive animal vaccination campaigns[14]. In the Chereponi district, most people do not vaccinate their dogs, and they cite a lack of money to buy the rabies vaccine as the reason. However, they are ready to pay for vaccines when they experience a dog bite, and the dangers of the bites are explained to them during consultation. On average, vaccinating dogs is less costly than vaccinating a human against rabies because the human rabies vaccine is more expensive. This phenomenon can be attributed to a lack of knowledge on the cost-effectiveness of vaccinating dogs and needs a collaborative effort between the multiple sectors, such as the district assembly, veterinary services department, health service, environmental health and education service to embark on an intensive awareness creation among the population. Even though human vaccines against rabies are free, this is not cost-effective. The government should intensify the vaccination of dogs as well as humans, especially in rural areas like Chereponi.
One Health approach has been documented to be effective in disease detection and control across the globe; however, there exist significant challenges in its implementation. In 2022, the North East Regional Health Directorate pushed for the implementation of an IBCM across the six districts in the region. With the support of the regional level, the district intensified rabies surveillance through a One Health approach. Components of the system aligned with WHO definition of IBCM which included reporting a bite or exposure event, performing a risk assessment, triggering an investigation for any bite, conducting an animal investigation, observing animal for 10-14 days (to confirm a healthy animal) or collecting samples and diagnostic testing (from dead/euthanized animals), and sharing feedback and investigation results across sectors[15].
This has strengthened the entire community-based surveillance approach in the district and has improved disease detection for other diseases. At the local levels, One Health WhatsApp platforms have been created to aid information sharing and ideas for implementing the One Health strategy. This has helped both veterinary officers and human health officers to properly coordinate and implement preventive measures when a dog bite case occurs. However, challenges exist especially within the veterinary department. Veterinary officers use their personal finances to transport samples and carry out other animal surveillance activities. This is unsustainable, hence there should be efforts to retool the department for efficiency of work. The central stocking of human rabies vaccines, analysis of every bite case to determine vaccine need, and drone delivery of vaccines to facilities have led to zero stockouts since the implementation of this strategy.
Limitations
This report has several limitations. First, as a single case study, the findings may not be generalizable to all settings. Second, the intervention’s success depended on specific, potentially unsustainable resources, such as drone delivery and officers’ personal funds for logistics. Finally, while the observed increase in bites primarily reflects improved reporting, the surveillance system is passive and likely undercounts minor exposures. Despite these limitations, this case provides a tangible and instructive model of successful One Health action in a high-risk setting.
Knowledge about the epidemiology, protocols and actions to be carried out by the disease control and surveillance unit helped to mitigate a human rabies incident. Also, strong One Health collaboration between the human health sector and the veterinary department was identified to play a critical role in bite case management.
What is already known about the topic
What this study adds