Research | Open Access | Volume 9 (2): Article 57 | Published: 10 Apr 2026

Views: 1,437
Menu, Tables and Figures
| Year | Population at risk | Suspected tested | Confirmed cases | No of deaths | Incidence per 100,000 | Case fatality rate | Positivity rate (%) |
|---|---|---|---|---|---|---|---|
| 2019 | 1,273,677 | 42 | 13 | 7 | 1.0 | 53.8 | 31.0 |
| 2020 | 1,302,718 | 111 | 28 | 14 | 2.1 | 50.0 | 25.2 |
| 2021 | 1,318,351 | 24 | 1 | 0 | 0.1 | 0.0 | 4.2 |
| 2022 | 1,328,551 | 46 | 5 | 0 | 0.4 | 0.0 | 10.9 |
| 2023 | 1,356,451 | 16 | 5 | 2 | 0.4 | 40.0 | 31.3 |
| Cumulative * | – | 239 | 52 | 23 | 3.9* | 44.2 | 21.8 |
Cumulative* incidence per 100,000 population. We used the mid-year population of 1,318,351 as an average to calculate the cumulative incidence for the five-year period.
Table 1: Incidence and mortalities of confirmed meningitis cases reported, Upper East Region, 2019-2023

Dominic Yeboah1, Rita Asante Kusi2,3,&, George Akowuah2, Joseph Asamoah Frimpong2, Mavis Osafo2, Samuel Sackey2, Ernest Kenu2, Freeman Samson Samani1
1Ghana Health Service, Upper East Regional Health Directorate, Bolgatanga, Ghana, 2Ghana Field Epidemiology and Laboratory Training Program, School of Public Health, University of Ghana, Legon, Accra, Ghana, 3Food and Drugs Authority, Accra, Ghana
&Corresponding author: Rita Asante Kusi, Ghana Health Service, Upper East Regional Health Directorate, Bolgatanga, Ghana, Email: angeasante@yahoo.com rita.asante@fda.gov.gh ORCID: https://orcid.org/0000-0003-1907-3667
Received: 01 Oct 2025, Accepted: 09 Mar 2026, Published: 10 Apr 2026
Domain: Infectious Disease Epidemiology
Keywords: Meningitis, surveillance, Ghana, meningitis belt
©Rita Asante Kusi et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Rita Asante Kusi et al., Descriptive analysis of meningitis surveillance data, Upper East Region, Ghana, 2019–2023. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):57. https://doi.org/10.37432/jieph-d-25-00215
Introduction: The global incidence of meningitis is estimated at 20 per 100,000 population. Ghana, located within the “African meningitis belt”, has experienced recurrent outbreaks with case fatalities ranging from 36% to 50%. In 2008, the Upper East Region recorded an incidence of 15 per 100,000 population. Data analysis is a core component of enhanced meningitis surveillance for early case detection and response. However, routine analyses were not consistently conducted. We therefore analysed surveillance data from 2019 to 2023 in the region to describe the distribution of cases and deaths to inform decisions.
Methods: We conducted a descriptive analysis of meningitis surveillance data in the Upper East Region from 2019-2023. An adapted checklist was used to extract variables from line lists and case-based forms. Data were triangulated and validated. Microsoft Excel 365, Epi Info 7.2.6.0, and Quantum Geographic Information System (QGIS) software were used for analysis. Frequencies, proportions, and rates were computed and presented in tables, charts, and maps.
Results: A total of 239 suspected cases were reported, of which 21.8% (52/239) were confirmed. The case fatality rate among confirmed cases was 44.2% (23/52). The most affected age group was 10-19 years, 26.9% (14/52), with a median age of 34 years (range: 0-89). Males accounted for 63.5% (33/52) of confirmed cases and 56.5% (13/23) of deaths. The highest proportion of cases occurred in 2020; 53.8% (28/52), with peaks in February and March. Cases were reported in 86.7% (13/15) of districts. Non-residents accounted for 5.8% (3/52) of cases and 13.0% (3/23) of deaths. The cumulative incidence was approximately 4 per 100,000 population.
Conclusion: Meningitis incidence fluctuated over the study period, with higher occurrence among males and adolescents. Cases peaked during the dry season and were widely distributed geographically. Persistently high fatality rates highlight the need to strengthen surveillance, early detection, and cross-regional coordination.
Meningitis is an inflammation of the membranes surrounding the brain and spinal cord, commonly caused by infectious agents. It remains an epidemic-prone disease affecting approximately 1.2 million people globally, with an estimated incidence of 20 per 100,000 population [1]. The disease is a major public health concern in the African “meningitis belt”, which stretches from Senegal to Ethiopia and experiences frequent outbreaks with high fatality rates [2]. Between 2015 and 2017, a total of 18,262 suspected cases were reported in sub-Saharan Africa with an average case fatality rate of 8.0% [3].
In Ghana, meningitis case fatality rates have ranged between 36.0% and 50.0% [4]. The Upper East Region recorded a total of 2,312 suspected and confirmed cases between 2016 and 2017, with an incidence of 15 per 100,000 population [5]. The World Health Organization (WHO) framework ‘Defeating Meningitis by 2030’ roadmap outlines global strategies to reduce meningitis burden through prevention, surveillance, and response [6]. Ghana introduced the Meningococcal Type A conjugate vaccine (Men A) into routine immunisation in 2016, aimed at reducing outbreaks and fatalities. Men A vaccination coverage has ranged between 72.8% in 2019 and 74.5% in 2023 [7].
Countries within the meningitis belt operate enhanced meningitis surveillance systems guided by WHO Integrated Disease Surveillance and Response (IDSR) standards. A suspected case is defined as a sudden onset of fever with meningeal signs, while laboratory confirmation requires identification of a causative pathogen in cerebrospinal fluid [8].
Surveillance data should be routinely analysed, interpreted, and disseminated to guide public health action. However, routine analyses were not consistently conducted in the Upper East Region, which can lead to late detection of outbreaks and early initiation of response. We therefore analysed meningitis surveillance data from 2019-2023 to describe the distribution of cases and deaths by person, place, and time to inform decision-making.
Analysis design and setting
We conducted a descriptive analysis of meningitis surveillance data from 2019 to 2023. Data were obtained from regional line lists and IDSR case-based forms. The analysis was conducted between July and October 2024. The Upper East Region is located in the Northern part of Ghana and shares borders with Burkina Faso, Togo North-East Region, and Upper West Region. It has 15 administrative districts, 101 sub-districts, and 682 health facilities.
The projected population was 1,356,451 based on the 2021 population and housing census. The region lies within the meningitis belt and experiences a long dry season (October-April) and a short rainy season (May-September). The dry season is characterised by dusty winds, low humidity, and high temperatures, conditions historically associated with increased meningitis incidence [2]. Historical data from the Ghana Health Service regional annual reports show a higher incidence of meningitis and respiratory tract infections during this season.
Data collection
An adapted IDSR checklist was used to extract variables including age, sex, reporting date, district of residence, laboratory results, and outcomes from line lists and case-based forms.
Case definitions used to generate surveillance data from communities and health facilities are “any person with sudden onset of fever (>38.5 °C rectal or ≥ 38.0 °C axillary) and either neck stiffness, bulging fontanelle, convulsions, altered consciousness or other meningeal signs” is a suspected case. Identification of causal pathogen (Neisseria meningitides, Streptococcus pneumoniae, Haemophilus influenzae b) from the cerebrospinal fluid of a suspected case by culture, Polymerase Chain Reaction or agglutination test” is a confirmed case [8].
Data validation
Meningitis surveillance data is generated and reported using both paper-based and electronic case-based forms on portals such as the District Health Information Management System 2 (DHIMS2) and Surveillance Outbreak Response Management and Analysis System (SORMAS). Data from paper-based forms and electronic platforms were reconciled. Records were screened for completeness and accuracy. Missing variables were retrieved from original case-based forms where available. Cleaned data were compiled into Microsoft Excel 365 for analysis.
Data analysis
The extracted variables were cleaned and analyzed using Microsoft Excel 365, Epi Info 7.2.6.0 and Quantum Geographic Information System (QGIS) software. The analysis was primarily descriptive, and Microsoft Excel helped to further summarise the available data after the use of Epi Info. Age was re-categorised into age groups to determine the median and the range. Proportions of monthly reported cases for each year were calculated to show the trend for the period and presented in a line graph. Person characteristics data from all suspected and confirmed individuals were summarised into frequencies and proportions and presented in a table. Incidence was computed using total confirmed cases among the total population at risk, expressed per 100,000 population. Total deaths among the confirmed cases were used to generate the case fatality rate, while the positivity rate was calculated by dividing the total confirmed cases by the total suspected cases tested. Quantum Geographic Information System (QGIS) software was used to show clustering of cases and hotspots districts for each year in a choropleth map. The annual incidence per 100,000 population, case fatality rate (CFR), and positivity rate were calculated and presented in a table.
Missing data variables were detected in the line lists during the data processing exercise. The specific case-based forms were identified and completed, and the line lists were updated. Vaccination status for most, 88.5% (46/52) of the confirmed cases were not available and could not be validated, hence excluded from the analysis. Also, there were missing data, 15.4% (8/52) on the specific causative organisms and the various species that could not be determined, hence excluded from the analysis.
Ethical considerations
Ethical clearance was obtained from the Ghana Health Service Ethics Review Committee (GHS-ERC: 023/05/24) on 22 August 2024. An introductory letter was obtained from the Ghana Field Epidemiology and Laboratory Training Program (GFELTP) secretariat, and permission was given by the Upper East Regional Health Directorate to access the meningitis database in the region. Data generated was coded, devoid of clients’ names and secured on a computer with a password and was made available only to those who needed to know to ensure confidentiality.
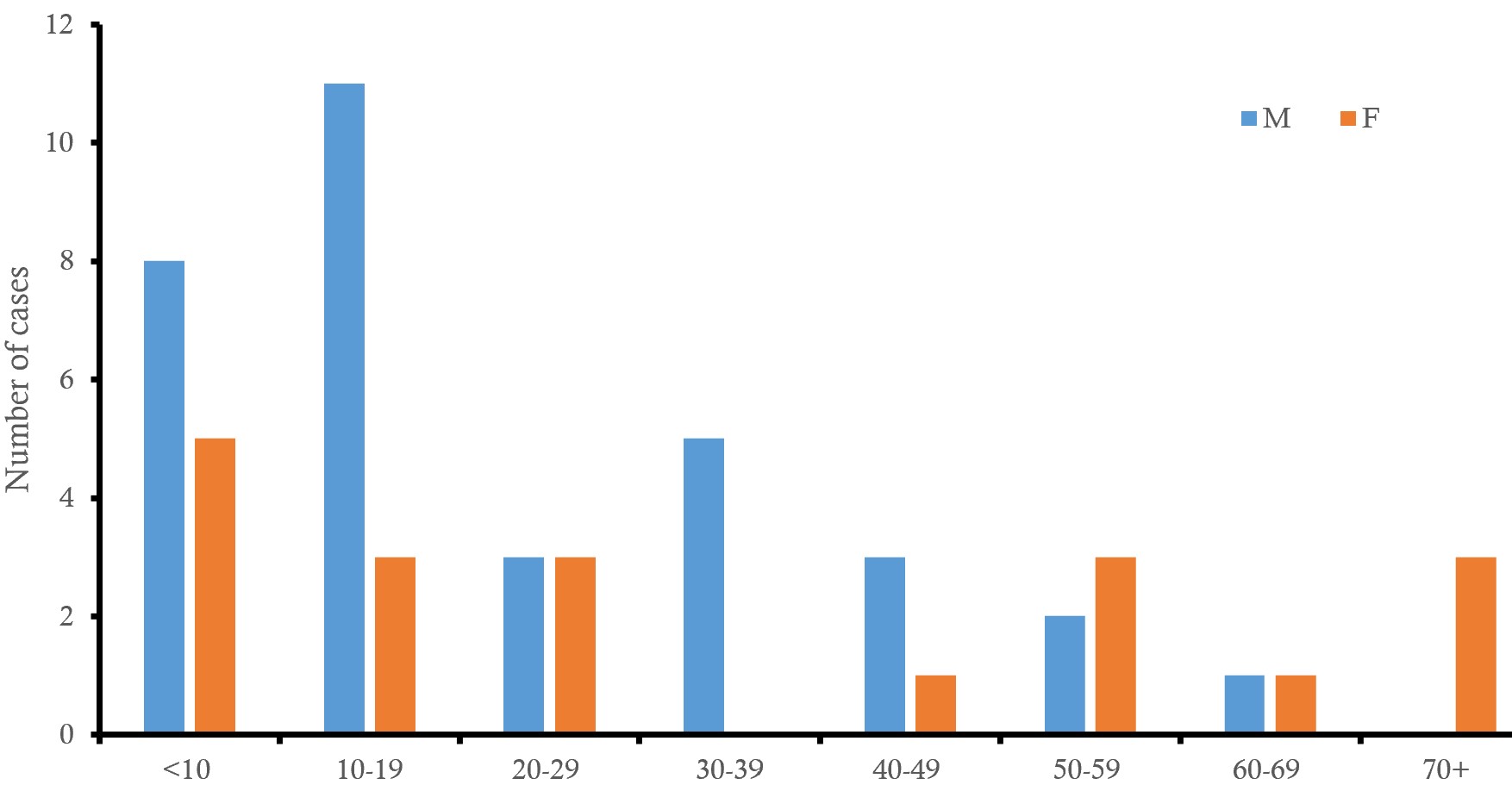
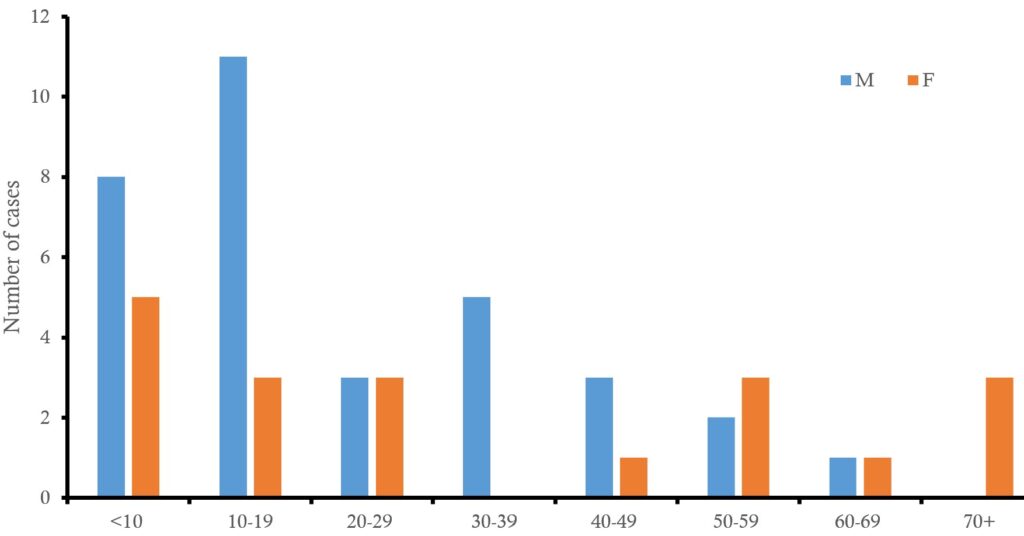
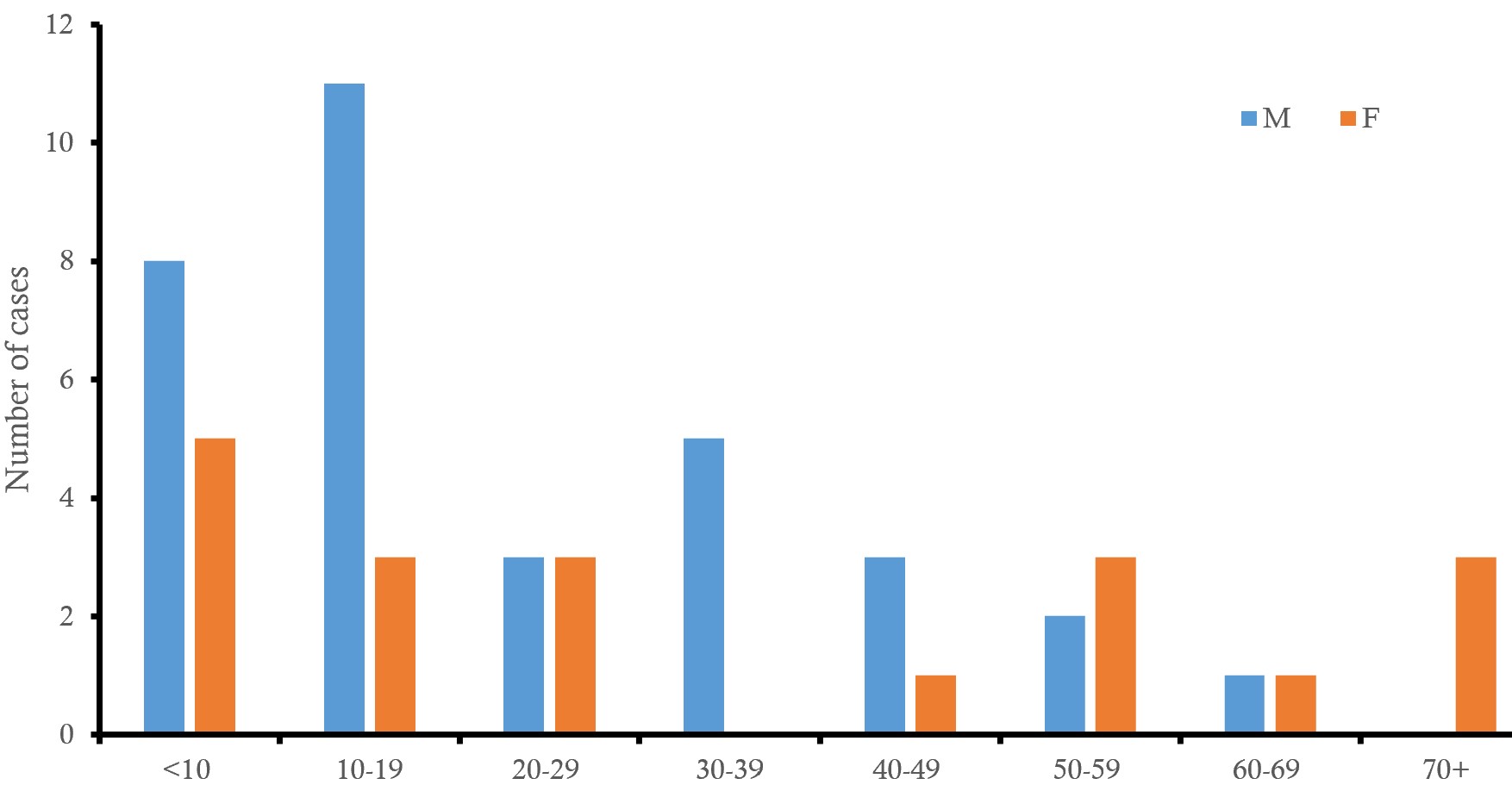
The 10-19-year age group accounted for the highest proportion of confirmed cases, 26.9% (14/52). The median age was 34 (0-89) years. Males constituted 63.5% (33/52) of confirmed cases and 56.5% of deaths (Figure 1).
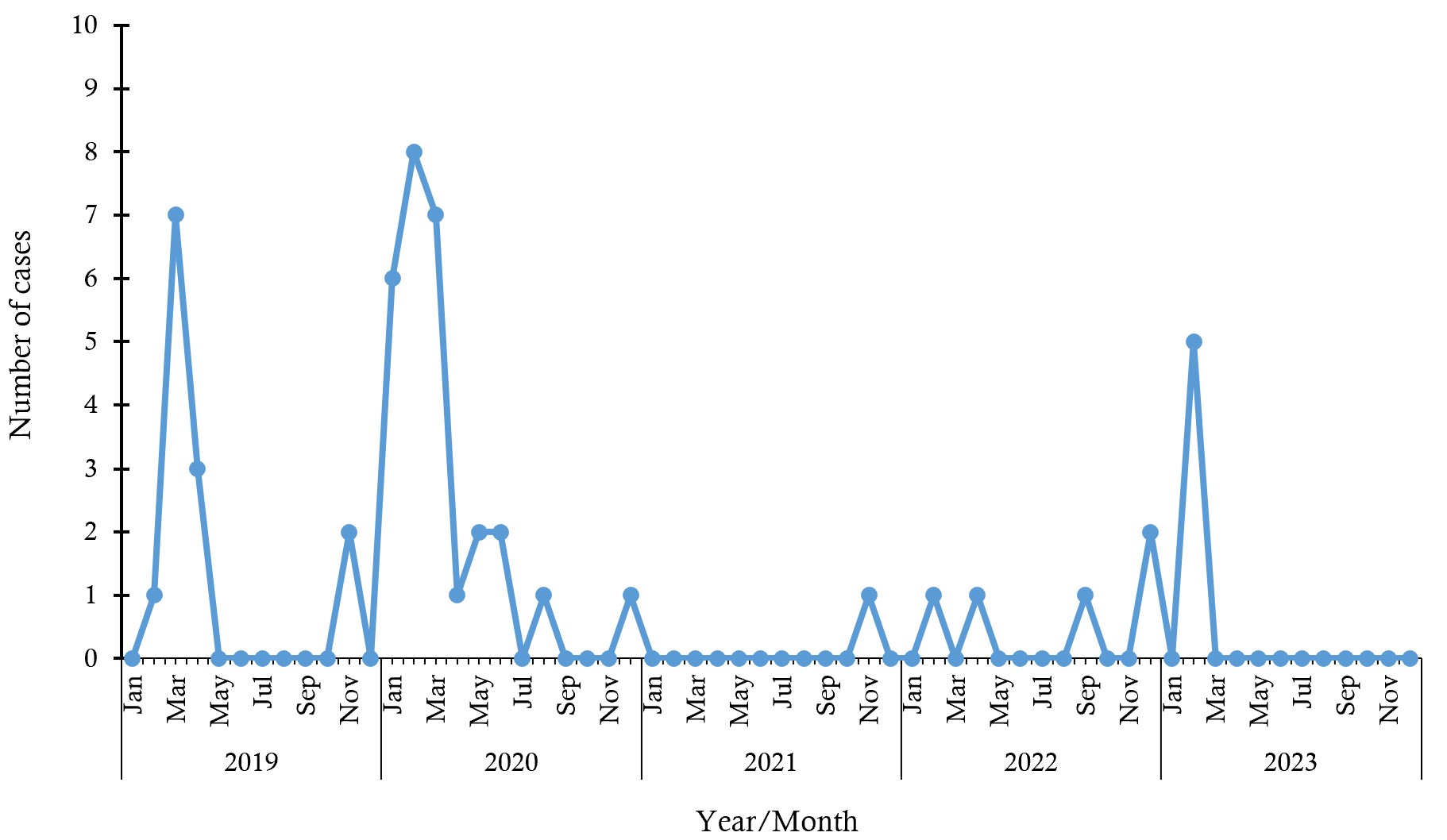
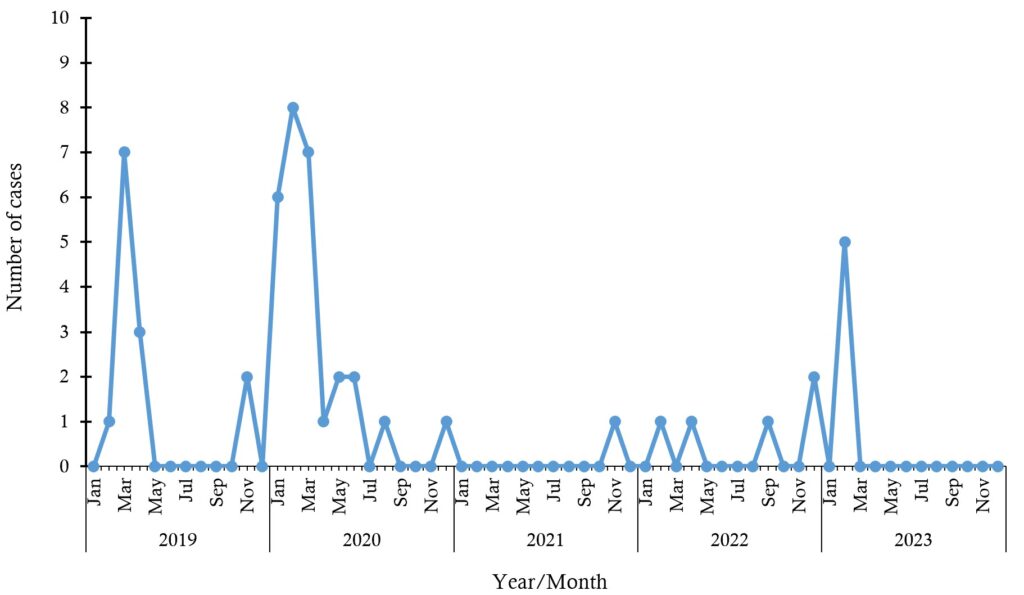
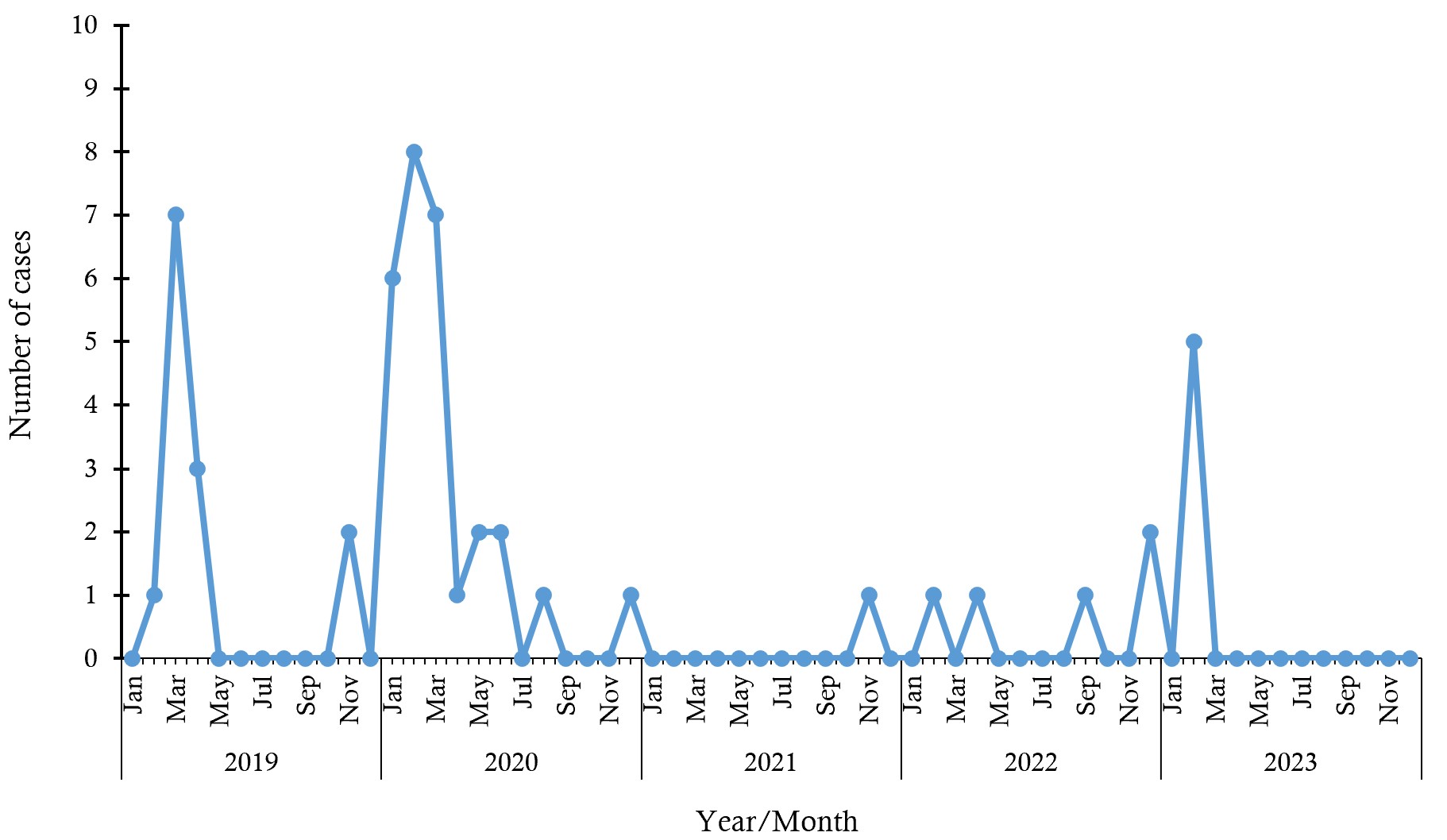
Most cases occurred in 2020, 28/52 (53.8%), and the least, 1/52 (1.9%), was recorded in 2021 (Figure 2). The month during which the highest number of cases was recorded for the five-year period was February 2020 (15.4% [8/52]). Other peaks were also recorded between January and March across the years (Figure 2).
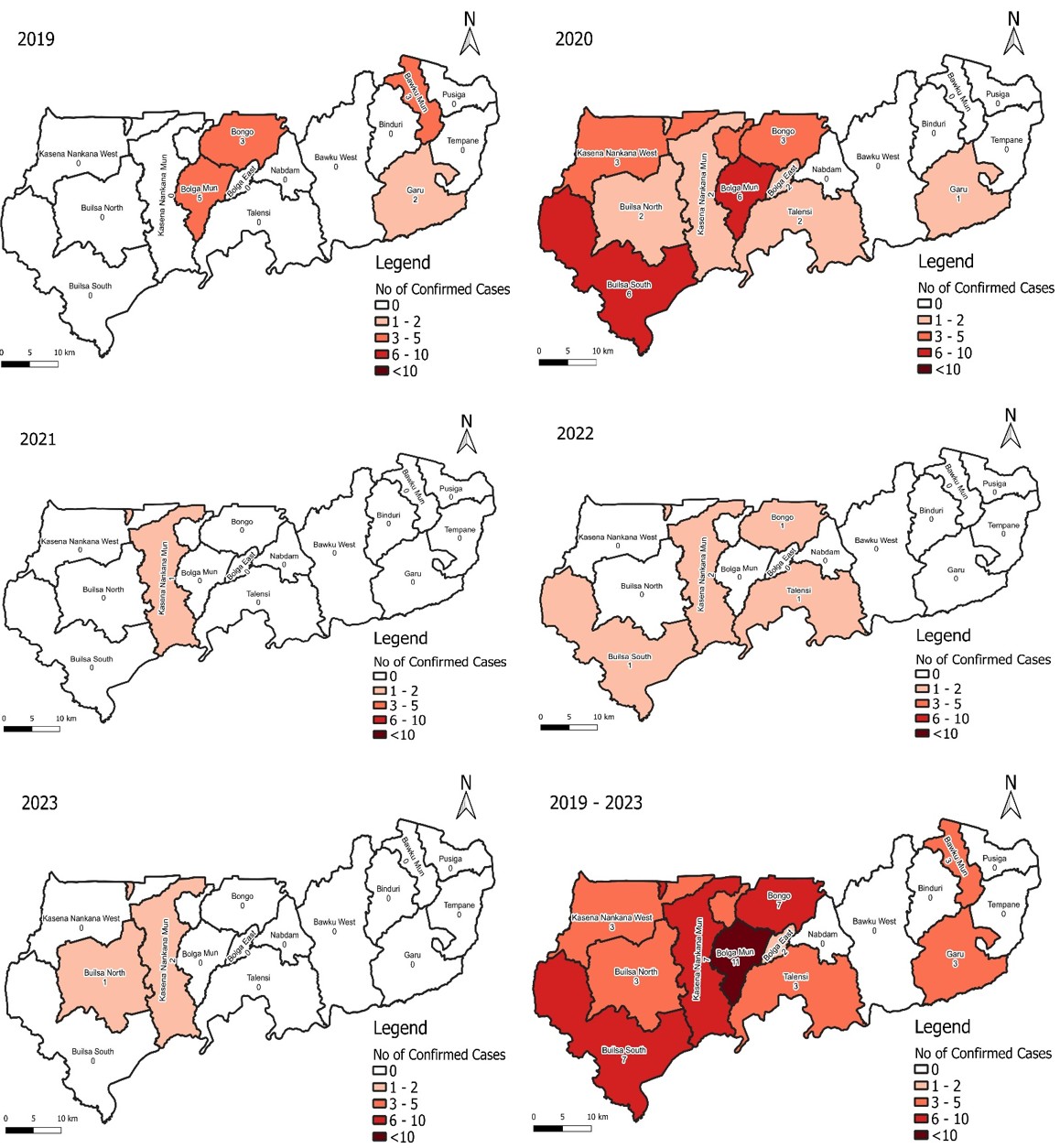
Cases were reported in 86.7% (13/15) of districts. Non-residents accounted for 5.8% (3/52) of cases and 13.0% (3/23) of deaths (Figure 3). A total of 21.8% (52/239) of suspected meningitis cases were confirmed. The cumulative incidence for the five years was approximately 4 per 100,000 population. The case fatality rate was 44.2% (23/52) (Table 1).
This analysis showed seasonal and demographic variations in meningitis occurrence. Males and adolescents were disproportionately affected, consistent with findings from the Upper West Region between 2018 and 2020, where males formed most cases, with the age group between 15 and 29 years mostly affected [6]. These findings affirm the high-risk social behaviours among males in general and adolescents in particular, especially engaging in activities in overcrowded and less ventilated areas.
Higher case counts during the dry season align with known environmental risk factors such as low humidity and dust exposure that increase nasopharyngeal vulnerability. It has been a general practice that during the dry season, people in the region gather to perform social activities in overcrowded spaces with limited ventilation in most instances, which facilitates the transmission of infectious strains [4]. Meningitis data analysis conducted in Amhara, Ethiopia, between 2015 and 2019 found that the trend of meningitis was higher during the dry season and progressively decreased during the rainy season [9].
Meningitis continues to threaten the region as a higher proportion of districts reported cases, coupled with threats of imported cases from neighbouring regions and countries like Burkina Faso. Similarly, a significant proportion of meningitis cases in Jaman North District in Bono Region were imported from a border town in La Côte d’Ivoire [8]. Cross-border movements contribute to case importation, emphasising the need for cross-regional and cross-border surveillance coordination.
The incidence of meningitis has been irregular, as it increased in 2020 and declined in 2023. Surveillance on priority diseases was enhanced and strengthened in 2020 when Ghana recorded its first COVID-19 imported cases. The COVID-19 pandemic created fear and panic among the populace, thereby reporting early to health facilities with a lot of varied cases including meningitis. Globally, it is noted how existing public health programs were interrupted due to physical distancing measures and reallocation of resources amidst the pandemic [10]. Despite these, the onset of the COVID-19 pandemic also intersected with advancements in technologies and surveillance advancements that potentially supported public health surveillance efforts, especially in tracking the distribution of infectious diseases [11]. The series of training for stakeholders in the surveillance system also influenced case detection across all notifiable diseases. Yearly fatality rates remained high, which could be due to non-adherence to public health preventive interventions, late reporting to health facilities and/or late detection of cases by the surveillance system, jeopardising the seaming efforts to prevent outbreaks and protect the public. This is in line with the assertion that the earlier a case is detected and managed, the better the outcome; however, the high case fatality rate casts doubt on the control and preventive measures [12]. The high positivity rates in the years signify the presence and circulation of causative organisms. This necessitates efforts to strengthen surveillance on early case detection, confirmation and prompt management for better outcomes and enhanced community engagement activities in the outbreak-prone communities [9].
A key limitation of this data analysis was missing data on vaccination status and causative organisms. Data inconsistencies between line lists and case-based forms reduced completeness. The analysis could not assess etiologic patterns or vaccine effectiveness. The analysis could therefore not determine whether the observed trends are driven by shifts in etiologic agents or changes in vaccine coverage. As a result, interpretations are limited to overall temporal patterns, and recommendations are framed at a general population-health level. Despite these limitations, inferences have been deduced, and some recommendations have been made to improve data quality in the region.
Meningitis incidence fluctuated from 2019–2023, with persistent high fatality rates and seasonal peaks during the dry season. Males and adolescents were most affected. The regional surveillance staff were oriented on the use of QGIS to geocode and map out case locations to aid in geographical analysis of cases and also to scrutinise case-based forms to ensure data quality as public health actions. The Public Health Directorate of the Ghana Health Service should strengthen surveillance and cross-regional coordination for early case detection and response. Regional Health Promotion Officers should facilitate community education on meningitis prevention and the benefits of early reporting.
What is already known about the topic
What this study adds
DY, RAK and GA conceptualized the analysis and designed the protocol. DY and GA did the data collection, cleaning, analysis, and interpretation. DY, RAK, GA, JAF, MO and SS contributed to data analysis and interpretation. FSS facilitated data acquisition. DY, RAK, GA, JAF, MO, SS and EK contributed to the original draft and revising of the manuscript. All the authors read and approved of this final manuscript.
| Year | Population at risk | Suspected tested | Confirmed cases | No of deaths | Incidence per 100,000 | Case fatality rate | Positivity rate (%) |
|---|---|---|---|---|---|---|---|
| 2019 | 1,273,677 | 42 | 13 | 7 | 1.0 | 53.8 | 31.0 |
| 2020 | 1,302,718 | 111 | 28 | 14 | 2.1 | 50.0 | 25.2 |
| 2021 | 1,318,351 | 24 | 1 | 0 | 0.1 | 0.0 | 4.2 |
| 2022 | 1,328,551 | 46 | 5 | 0 | 0.4 | 0.0 | 10.9 |
| 2023 | 1,356,451 | 16 | 5 | 2 | 0.4 | 40.0 | 31.3 |
| Cumulative * | – | 239 | 52 | 23 | 3.9* | 44.2 | 21.8 |
Cumulative* incidence per 100,000 population. We used the mid-year population of 1,318,351 as an average to calculate the cumulative incidence for the five-year period.