Research | Open Access | Volume 9 (2): Article 58 | Published: 10 Apr 2026

Views: 1,342
Menu, Tables and Figures
| Variables | Total N (%) |
|---|---|
| Sex (N = 1058) | |
| Female | 712 (67.3) |
| Male | 346 (32.7) |
| Age (N = 1058) years | |
| 15–20 | 68 (6.4) |
| 21–24 | 233 (22.0) |
| 25–34 | 513 (48.5) |
| 35–49 | 191 (18.1) |
| 50+ | 53 (5.0) |
| Population type (N = 1004) | |
| General Population | 624 (62.2) |
| Key Population | 326 (32.5) |
| Priority Population | 54 (5.3) |
| Facility (N=1058) | |
| HBCTRH | 226 (21.4) |
| Makongeni DICE | 489 (46.2) |
| Marindi SCH | 116 (11.0) |
| Miniambo HC | 163 (15.4) |
| Nyalkiny Disp | 64 (6.0) |
| Reason for PrEP initiation (N = 773) | |
| Key population risk | 185 (23.9) |
| Other/unspecified | 67 (8.7) |
| Partner-related risk | 293 (37.9) |
| Sexual risk behaviours | 228 (29.5) |
Table 1: Socio-demographic and programmatic characteristics of PrEP clients in selected health facilities in Homabay County, Kenya, January 2021-June 2023
| Indicator | HBCTRH | Makongeni DICE | Marindi | Miniambo | Nyalkinyi | Average |
|---|---|---|---|---|---|---|
| Sex | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Age | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Population type | 90.6% | 94.1% | 98.4% | 100.0% | 99.1% | 96.4% |
| Assessed | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Eligible | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| PrEP initiation date | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Reason for PrEP initiation | 92.4% | 76.5% | 75.6% | 35.2% | 68.8% | 69.7% |
| HTS done | 91.5% | 94.5% | 98.4% | 100.0% | 100.0% | 96.9% |
| STI screened | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Adherence | 13.5% | 58.3% | 22.8% | 15.8% | 18.8% | 25.8% |
| Received adherence counselling | 99.5% | 98.8% | 96.7% | 100.0% | 87.5% | 96.5% |
| PrEP status | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Reason for discontinuation | 14.8% | 0.0% | 0.0% | 0.6% | 0.0% | 3.0% |
| Average | 84.8% | 86.3% | 84.0% | 80.9% | 82.6% | 83.7% |
Note: Cell-level shading indicates data completeness below the 95% benchmark recommended for routine health information systems. Shading is applied for descriptive flagging and does not alter the benchmark definition.
Table 2: EMR data completeness by facility in Homabay town Sub-county, January-March 2023
| Facilities | January – March 2021 | January – March 2022 | January – March 2023 | |||
|---|---|---|---|---|---|---|
| Rate | Timeliness | Rate | Timeliness | Rate | Timeliness | |
| HBCTRH | 66.70% | 0% | 100% | 33.30% | 100% | 100% |
| Marindi SCH | 100% | 100% | 100% | 100% | 100% | 66.70% |
| Makongeni DICE | 100% | 100% | 100% | 100% | 33.30% | 33.30% |
| Miniambo HC | 100% | 100% | 100% | 100% | 100% | 100% |
| Nyalkinyi Dispensory | 100% | 100% | 100% | 100% | 100% | 100% |
Table 3: Quarterly reporting rates and timeliness by facility in Homabay town Sub-county, Kenya, January-March (2021-2023)
Brian Onyango Sigu1,&, Fred Omino2, Abdiaziz Mohamed1, Carrey Abuya1, Maurice Owiny1, Fred Odhiambo1, Dickens Onyango3
1Field Epidemiology and Laboratory Training Program, Ministry of Health, Kenya,2Homabay County Department of Health, Kenya, 3Kisumu County Department of Health, Kenya,
&Corresponding author:Brian Onyango Sigu, Field Epidemiology and Laboratory Training Program, Ministry of Health, Nairobi, Kenya, Email: bryoscii@gmail.com ORCID: https://orcid.org/0009-0001-7612-4750
Received: 07 Jul 2025, Accepted: 03 Apr 2026, Published: 10 Apr 2026
Domain: Infectious Disease Epidemiology
Keywords: HIV pre-exposure prophylaxis (PrEP), Data quality, Routine health information systems (RHIS), PrEP retention, Electronic medical records (EMR), HIV prevention, Kenya (Homabay County)
©Brian Onyango Sigu et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Brian Onyango Sigu et al., Suboptimal data quality and poor HIV pre-exposure prophylaxis retention in Western Kenya. Journal of Interventional Epidemiology and Public Health. 2026; 9(1):58. https://doi.org/10.37432/jieph-d-25-00156
Introduction: HIV remains a major challenge in Kenya, particularly in Homabay County, with the highest (19.6%) prevalence nationally. While HIV pre-exposure prophylaxis (PrEP) is highly effective in preventing HIV infection, its programmatic impact depends on the availability of high-quality routine data and sustained user retention. This evaluation assessed routine PrEP data quality and reporting systems and examined uptake and retention patterns among PrEP users aged ≥15 years.
Method: A facility-based retrospective evaluation was conducted in five purposively selected high-volume PrEP service delivery sites in Homabay town Sub-county from January 2021 to June 2023. Data were abstracted from Electronic Medical Records (EMR) and the Kenya Health Information System (KHIS) using a standardized Excel-based abstraction template. Data quality and reporting processes were concurrently assessed using the Routine Data Quality Audit (RDQA) tool. Descriptive statistics summarized baseline characteristics, data quality indicators, and PrEP retention patterns. An exploratory multivariable logistic regression examined correlates of PrEP initiation age, adjusting covariates. PrEP retention was assessed descriptively due to limited completeness of follow-up variables.
Result: A total of 1,058 PrEP client records were reviewed. The median age at PrEP initiation was 28 years (IQR: 24-34), and females were 67%. In exploratory analysis, female clients had a higher odds of initiating PrEP at age ≤20 years (aOR = 3.53; 95% CI: 1.74–8.16), while clients initiating PrEP due to partner-related risk had lower odds (aOR = 0.20; 95% CI: 0.03–0.73), with consistent sensitivity analyses. Overall average data completeness was 87.3%, with completeness for adherence (12%) and reasons for discontinuation (3%). Verification factors were 52.4% in 2021 and 77.4% in 2022, far below the recommended 95%-105% range. The average system assessment score was 2.50 on a 1–3 scale, with the lowest observed in the data management process (2.0). Documented PrEP continuation declined over follow-up visits and should be interpreted as minimum estimates due to incomplete follow-up data.
Conclusion: While PrEP initiation data were sufficiently complete to assess uptake, incomplete follow-up documentation constrained retention analysis, underscoring the need to strengthen the routine PrEP data system for effective monitoring, evaluation, and informed programmatic decision-making.
The Human Immunodeficiency Virus (HIV)/ Acquired Immunodeficiency Syndrome (AIDS) remains a global burden, with over 39 million people globally living with HIV in 2022. That year, on average 1.3 million people were newly infected, approximately 630,000 died from HIV-related illnesses, and 29.8 million were receiving antiretroviral therapy [1]. Sub-Saharan Africa (SSA), with an estimated 12% of the global population, bore the burden of 65% of all HIV-related deaths and 58% of new HIV infections in 2021, making it one of the epicenters of the HIV epidemic [2]. While Kenya has made significant gains in curbing the HIV epidemic, HIV remains one of the leading causes of mortality in the country in general [3]. According to the National AIDS and STI Control Program (NASCOP), the prevalence of HIV in Homabay (19.6%) is four times that of the national HIV prevalence of 4.9% [3].
HIV PrEP is a prevention intervention that involves the use of antiretroviral medication by HIV-negative people at high risk of infection. When taken consistently as directed, PrEP demonstrates high effectiveness in preventing HIV transmission and has been shown to decrease HIV infections by more than 90% when used alongside other interventions for HIV prevention and treatment [2, 4].
Optimal data quality is fundamental in decision-making, as it informs policy and measures the program’s effectiveness, advocacy, and resource allocation [5]. HIV data in systems such as the Kenya Health Information System (KHIS) are only as good as their quality [6]. Hence, the capacity of HIV healthcare workers and other entities to report complete, accurate, and timely data is paramount in monitoring trends in HIV care and prevention services. The need for quality data became particularly pressing after the introduction of the United Nations’ 2030 Agenda for Sustainable Development and its associated Sustainable Development Goals (SDGs), which meant that tracking progress towards health and other development goals became more important than ever [7].
The PrEP framework was officially launched in Kenya in 2017, and implementation began after participating in clinical trials and demonstration studies [8]. Since the rollout, Kenya has cumulatively initiated 157,538 individuals on PrEP as of December 2021, with 58,204 individuals reported to be on PrEP as of the same period, as per KHIS program data for 2021 [8]. At the time of this evaluation, there was no documented PrEP-specific routine data quality audit conducted within Homabay County. On the other hand, previous research on PrEP uptake focusing on adolescents and young women in Kenya (AYWG) revealed low PrEP uptake and continuation [9]. The primary objective of this evaluation was to assess the quality of routine PrEP data and reporting systems and describe PrEP uptake patterns and retention over time among PrEP users aged 15 years and older in selected public health facilities in Homabay County.
Study design and settings
This was a facility-based retrospective evaluation conducted in five public health facilities in Homabay town Sub-county, Homabay County, western Kenya. Homabay County has the highest HIV prevalence in Kenya (19.6%) and is a priority setting for HIV prevention interventions, including scale-up of oral PrEP services among general and high-risk populations [3]. Homabay town Sub-county comprises a mix of peri-urban and rural communities with a high burden of HIV and substantial demand for prevention services, where PrEP is delivered through routine outpatient HIV prevention programs integrated within public health facilities and community-based service delivery points, with data captured in EMR and reported through the KHIS.
The five sites included rural and urban settings and were purposively sampled based on the facility level and workload: one community-based or PrEP – Drop-in centres (DICE), one dispensary, one health center, one Sub-county hospital, and one County referral hospital. These facilities represent different tiers of the Kenyan health system and variations in service delivery models, patient volume, and data management capacity, making them suitable for assessing routine PrEP data quality and reporting performance across levels of care.
Study population
The study population were all eligible PrEP clients registered in the facility’s PrEP register (EMR) from January 2021 through to June 2023.
Data collection
Data were collected from facility EMR and KHIS using a standardized Excel abstraction tool and an adopted routine data quality audit (RDQA) tool [10]. Both PrEP enrolment and follow-up data are routinely captured electronically in the EMR at the point of client engagement. Baseline enrolment data were obtained from the PrEP EMR initiation register, and the data collected was as at the time of oral PrEP initiation, and it included socio‐demographic characteristics (age, sex and facility), client population type (discordant couple, fisher folk, the general population, key populations and others), eligibility status, reasons for PrEP initiation (client type, sex with a partner of known HIV‐positive status, transactional sex, condom-less sex, or inconsistent condom use, intravenous drug use, multiple sexual partners and sex with partners with unknown HIV status), and HIV testing and services (HTS) status. Follow-up data were abstracted from EMR follow-up registers and included PrEP continuation status, adherence status, and reasons for discontinuation at 1, 3, 6, 9, and 12 months after initiation. The reasons for discontinuation included HIV test positive, low risk of HIV, renal dysfunction, client request, non-adherence, viral suppression of an HIV positive partner, too many other HIV tests and other documented reasons.
While both baseline and follow-up information are digitized, follow-up documentation depends on subsequent client return visits and completion of longitudinal records by providers. PrEP continuation was defined as documentation of a renewed PrEP prescription at each scheduled follow‐up visit. Clients without documented visits or renewals were classified as discontinued at that time point. Individuals who restarted PrEP after a documented gap were not considered continuing users for missed follow-up periods.
Data analysis
We used descriptive statistics to summarize client baseline socio-demographic and programmatic characteristics, and to describe PrEP uptake and retention patterns. For analytical purposes, age at PrEP initiation was further categorized to examine early initiation, defined as ≤20 years, reflecting adolescence and early youth in line with World Health organization (WHO) definitions to distinguish adolescent from adult PrEP initiation in line with programmatic HIV prevention priorities [11]. It was analysed as a binary outcome using multivariable logistic regression. Independent variables (sex, population type, facility, and reason for PrEP initiation) were selected based on their programmatic relevance and to maintain a parsimonious model in light of event frequency and variable completeness.
Sensitivity analysis using firth penalised logistic regression was conducted to assess the robustness of estimates in the presence of sparse data. Inconsistent population type classification was observed in the EMR, with some facilities using a non-standard “priority population” category; therefore, key and priority populations were analytically combined into a single higher-risk population group.
Data quality elements included completeness (percentage of required PrEP data elements that were filled), accuracy (concordance between source documents and reported KHIS data measured as a verification factor), reporting rates (proportion of expected PrEP reports submitted by each facility), and timeliness (the proportion of reports submitted within nationally stipulated deadlines).
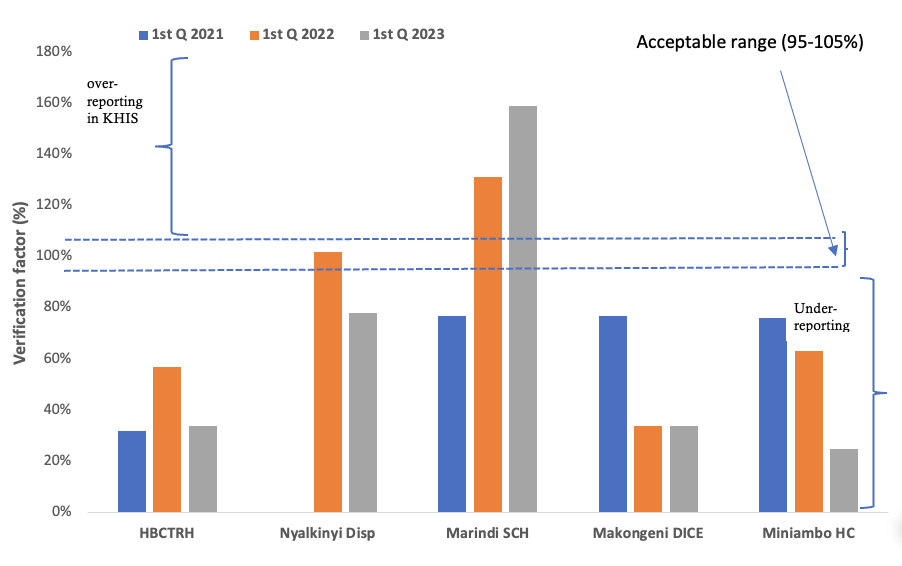
For verification factor assessment, data were re-counted from facility source documents and compared with values reported in the facility’s monthly PrEP summary tool (MOH 731) and in the KHIS for the January–March reporting period of each year from 2021 to 2023. In line with World Health Organization (WHO) guidelines on health management information system (HMIS) data verification, the verification factor was defined as the percentage ratio of values from the facility-based PrEP summary tool (MOH 731) to those reported in KHIS. Verification factor values between 95% and 105% were considered acceptable, while values below 95% or above 105% indicated under-reporting and over-reporting in KHIS, respectively. Data timeliness and reporting rates were downloaded from the KHIS.
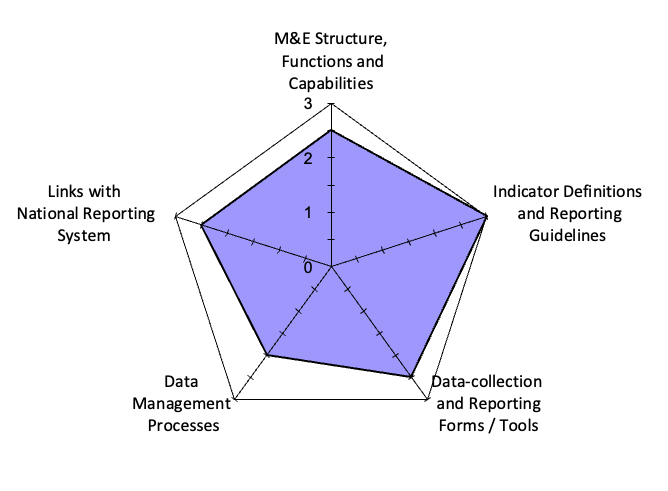
The system assessment was based on indicator definitions and reporting guidelines, data collection and reporting forms and tools, data management processes, and links with the national reporting system. Questionnaire data was collected and simultaneously entered into the RDQA tool. The tool has an in-built data analysis formula that automatically analyzes and displays the data using a web chart drawn on a scale of 1-3, where 1 is the weak point, while 3 is the strong point.
Ethical considerations
Ethical review was waived by the Ministry of Health since this was a retrospective data review. Authorization to conduct the evaluation was obtained through the Kenya Field Epidemiology and Laboratory Training Program (K-FELTP) and the Homabay County Department of Health. Confidentiality and privacy of the data were ensured through the use of unique identifiers and secure storage of collected data.
Socio-demographic and programmatic characteristics at PrEP initiation
A total of 1,058 EMR records across five facilities were abstracted. The overall median age at PrEP initiation was 28 years (IQR: 24-34), and females accounted for 67% (712/1058) of the clients.
Across the five facilities, the distribution of PrEP clients by population type varied substantially (Table 1). The general population clients predominated in all public PrEP-based facilities, accounting for nearly all initiations at Homabay County teaching and referral hospital (HBCTRH) (99.5%), Marindi Sub-county hospital (100%), and Nyalkiny dispensary (98.4%), and the majority at Miniambo health centre (80.4%). In contrast, Makongeni DICE served a predominantly higher-risk population, which comprised 75.2% of initiations at that site.
Early PrEP initiation occurred in 6% (68/1058) of clients and was more common among females. In multivariable logistic regression, adjusting for population type, facility, and reason for PrEP initiation, females had significantly higher odds of early PrEP initiation compared with males (aOR = 3.53; 95% CI: 1.74–8.16). Clients initiating PrEP due to partner-related risk had significantly lower odds of early initiation compared with those initiating PrEP for other or unspecified reasons (aOR = 0.20; 95% CI: 0.03–0.73).
Although early PrEP initiation appeared more common among clients documented as priority population in descriptive analyses, the combined higher-risk population category was not independently associated with early PrEP initiation in adjusted analyses. Sensitivity analysis using Firth penalised logistic regression yielded directionally consistent estimates, supporting the robustness of these findings.
Data quality and routine PrEP reporting performance
The average data completeness across the five facilities was 83.7%. Baseline enrolment variables recorded at PrEP initiation, including age, sex, assessment status, and PrEP initiation date, were consistently and fully documented across facilities. In contrast, documentation of population type (96%) and HTS status (96%) showed minor incompleteness, while reason for PrEP initiation was substantially incomplete (70%); however, the available records were sufficient to support the planned analyses. Client’s follow-up details, such as reasons for discontinuation and adherence status, were the least documented at 3% and 25%, respectively (Table 2).
Verification factor analysis comparing facility-based PrEP summary tool (MOH 731) with aggregate reports in KHIS revealed variability in data concordance across facilities. None of the five facilities consistently achieved verification factors within the acceptable 95%–105% range over the evaluation period. Only Nyalkinyi dispensary had concordance (102%) within the acceptable range in 2022. In contrast, Marindi Sub-county hospital, Makongeni DICE, and Miniambo health centre consistently had a discordant verification factor. Overall, while verification factors improved between 2021 and 2022, data concordance remained suboptimal across most facilities (Figure 1).
Reporting rates and timeliness were high across most facilities from 2021 to 2023. All facilities achieved 100% reporting by 2022, although Makongeni DICE and Marindi Sub-county hospital showed reduced timeliness in 2023, while other facilities maintained consistently complete and timely reporting (Table 3).
The average performance on the data system assessment across the five facilities was suboptimal, 2.50 on a 1–3 scale. Indicators related to data management processes, including routine data review and verification prior to submission, recorded the lowest scores (2.0), while indicator definitions and reporting guidelines scored highest (3.0) across the five facilities (Figure 2).
PrEP initiation and retention patterns
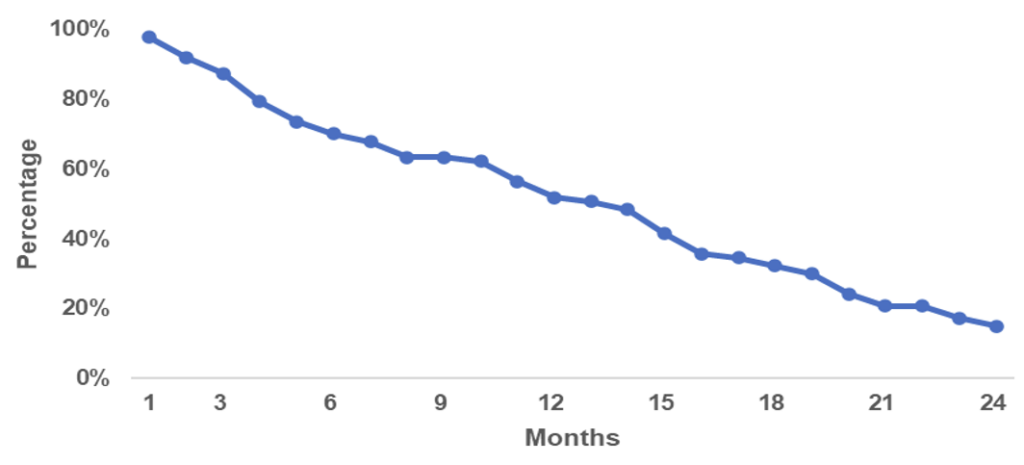
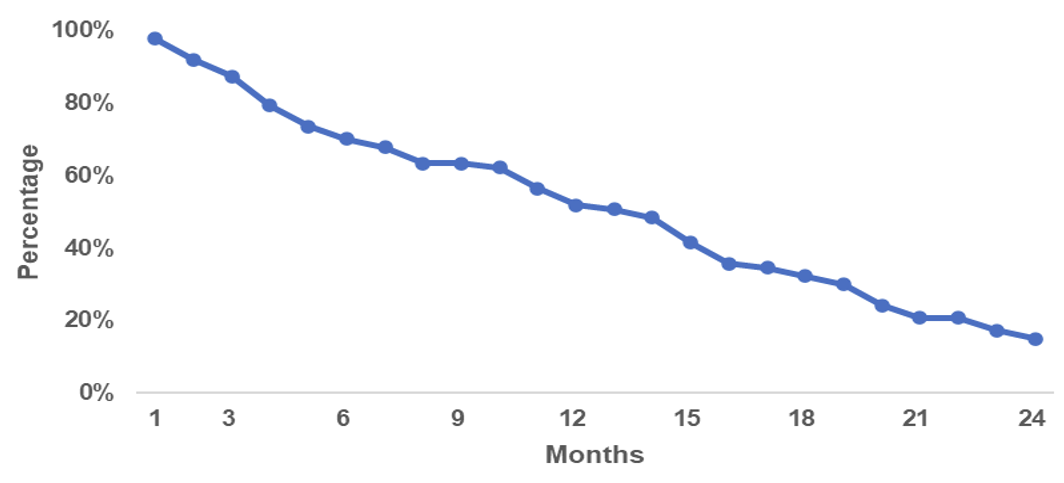
Quarterly PrEP initiation trends varied across facilities. Makongeni DICE demonstrated greater temporal variability, with sporadic increases in initiation, while public facilities showed comparatively more stable initiation patterns over time. Longitudinal analysis of documented PrEP follow-up data showed a gradual decline in PrEP continuation across the subsequent follow-up visits (Figure 3).
Analysis of abstracted EMR data records across the five facilities reveals key insights into PrEP usage patterns, with a median age of 28 years at PrEP initiation indicative of high PrEP use among the young population, with females comprising the majority and significantly more likely to initiate PrEP at the age of 20 and below compared to males. The predominance of younger age groups among PrEP users may reflect higher levels of sexual activity and HIV vulnerability among adolescents and young adults, who experience elevated HIV incidence in sub-Saharan Africa [12]. For females, one possible explanation is the higher biological and socio-structural vulnerability to HIV infection compared to males, particularly among adolescent girls and young women (AGYW) aged 15–24 years, who experience disproportionate HIV incidence in SSA due to factors such as age-disparate relationships, limited power to negotiate condom use, and higher exposure to transactional sex [12].
Similarly, the general population was the primary user category across most facilities, except at the DICE, where the key population, that is, the HIV high-risk category, predominates. Key population preference for DICE over public facility-based PrEP clinics could be explained by the awareness and friendliness towards all possible population backgrounds at the DICEs, which are likely to be lacking in public facility-based PrEP clinics. In agreement with these findings, evidence from rural Kenya and Uganda shows that drivers for PrEP use are highly gendered, which may partly explain the demand for differentiated and community-based delivery models. In that study, young men viewed PrEP as a means of reducing HIV risk while engaging in multiple sexual partnerships, while young women viewed PrEP as a strategy to manage HIV risk in a transactional sex context and in situations with limited agency to negotiate condom use and partner testing [13]. Another study in the SSA settings showed that Community-based DICEs were the most (66%) preferred PrEP outlet for AGYW, compared with public clinics (25%) and private clinics (9%) [14], and that most men preferred community-based delivery models.
Study findings show that Key populations contributed to about half of the new HIV infections in 2021 in SSA [10, 15]. Therefore, understanding the risk factors and implementing strategies to deal with these risk factors effectively are critical elements for HIV epidemic control in SSA.
The Data quality and system assessment findings reveal a varied data quality landscape across the five facilities, showcasing strong completeness in baseline client documentation but significant gaps and inconsistencies in follow-up details, recording population types, and eligibility reasons. Discrepancies between primary data sources and system-reported data indicate challenges in data accuracy and reliability. Findings from the system assessment revealed suboptimal performance in data management process, including weak routine data review and verification practices before report submission, which may have contributed to these discrepancies. The data reporting system findings suggest that while there is room for improvement in data system assessment across the five facilities, particularly in the data management process, there is a strong foundation for understanding indicator definitions and reporting guidelines. Although this evaluation focused on five facilities within Homabay County, the findings are relevant to a broader audience because Kenya’s PrEP program relies on standardized national reporting systems, which are used uniformly across all counties. Similar routine HIV and PrEP reporting structures are employed across many SSA settings, suggesting that the data quality gaps identified reflect system-level challenges rather than isolated facility weaknesses [15].
The findings also suggested a consistent decline in PrEP uptake between 2021 and 2022 across the five facilities, with stability thereafter, aside from sporadic spikes at Makongeni DICE. Higher relative data completeness in baseline documentation could be partly explained by the fact that these data are mandatory and have to be entered into the EMR at enrolment, whereas follow-up visits are more prone to missed or delayed documentation. This agrees with evidence that automated processes improve the completeness and accuracy of indicator data overall [16], which may partly explain the higher completeness observed for baseline documentation during initial client encounters, as shown by this evaluation. On the other hand, the occasional spikes in PrEP uptake observed at Makongeni DICE may plausibly be linked to periodic outreach and community-based activities conducted by the facility. Evidence from similar settings supports this interpretation. The SEARCH study in rural Kenya and Uganda demonstrated that population-level HIV testing combined with community-based PrEP education, initiation, and flexible follow-up modalities resulted in substantial PrEP uptake and sustained engagement over time [17, 18].
Longitudinal data analysis highlights a gradual decrease in PrEP continuation over subsequent follow-ups, which may indicate both potential difficulties in sustaining long-term engagement with PrEP services. However, given the substantial incompleteness in follow-up documentation, these estimates should be interpreted as minimum levels of continuation rather than precise retention rates. This limitation reflects gaps in routine data capture and should be considered when interpreting retention outcome. The findings on declining PrEP uptake and retention rate align with the study findings of a systematic review that showed that 41 % of participants would discontinue PrEP within six months (95% CI: 18.8–63.5%), with the highest rates in observational studies especially in SSA and in contrast, clients with adherence interventions are likely to pool a lower discontinuation rate than those without (24.7% vs. 36.7%, P=0.015) [19]. The gradual decrease in PrEP continuation also confirms the findings of a study done in Kisumu on the uptake and continuation of PrEP, which showed a significant continuation decline with increasing follow-up duration [9]. Similarly, previous findings that included reporting rates showed high self-discontinuation of PrEP and suboptimal reporting rates by facilities on PrEP services in Kenya [8]. On the other hand, the observed poor retention may partly reflect discontinuation among individuals whose perceived HIV risk changed over time. This is informed by the predominance of situational risk factors recorded at initiation, such as transactional sex, condom-less sex, multiple sexual partnerships, and sex with partners of unknown HIV status, which are often episodic rather than sustained. However, although reasons for PrEP initiation were moderately well documented, the extent to which these risks persisted over time could not be directly assessed, as risk duration and reasons for PrEP discontinuation were poorly documented, with only 3% completeness for the ‘reasons for PrEP discontinuation’ indicator.
Limitations
This evaluation has several limitations that should be considered when interpreting the findings. First, it was conducted in a small number of purposively selected facilities within a single Sub-county, which limits the generalizability of the results beyond similar service delivery settings. Second, the analysis relied on routine programmatic EMR and KHIS data that were not originally collected for research purposes and were subject to missingness and documentation inconsistencies, particularly for follow-up indicators. As a result, analyses of PrEP retention were limited to descriptive methods, and observed declines in continuation should be interpreted as minimum estimates rather than precise retention rates. In addition, population type classification was based on routine EMR documentation and may have been subject to misclassification. Finally, the observational design of the evaluation precludes causal inference regarding factors associated with PrEP initiation or continuation.
This evaluation shows that while routine EMR data were sufficiently complete to support analyses of PrEP uptake, persistent gaps in follow-up documentation substantially limited accurate assessment of retention. Improving the quality and continuity of routine PrEP data systems is critical to enable meaningful evaluation of PrEP programme performance and inform evidence-based HIV prevention strategies.
What is already known about the topic
What this study adds
We gratefully acknowledge the Field Epidemiology and Laboratory Training Program (FELTP) for the technical and financial support that made this study possible. We also sincerely thank the Homabay County Department of Health for their collaboration and Mr. Obunga, the County AIDS and STI Coordinator (CASCO), for his invaluable support. Special thanks to the LVCT-Homabay team, particularly Mr. Gabriel Tembule and Mr. Ng’eno, for their dedicated assistance throughout the evaluation
BS: Conceptualization, data collection, formal analysis, investigation, methodologies, supervision, visualization, writing original draft, and reviewing and editing.
FO: Data collection, data analysis, and investigation.
AM: Data collection, analysis, investigation, and writing original draft
CA: Data collection, analysis, investigation, writing the original draft, and reviewing and editing
MOO: Conceptualization, writing original draft, reviewing, and editing
FO: Conceptualization, data collection, formal analysis, investigation, methodologies, supervision, writing original draft, and reviewing and editing
DOO: Conceptualization, data collection, formal analysis, investigation, methodologies, supervision, writing original draft, and reviewing and editing
| Variables | Total N (%) |
|---|---|
| Sex (N = 1058) | |
| Female | 712 (67.3) |
| Male | 346 (32.7) |
| Age (N = 1058) years | |
| 15–20 | 68 (6.4) |
| 21–24 | 233 (22.0) |
| 25–34 | 513 (48.5) |
| 35–49 | 191 (18.1) |
| 50+ | 53 (5.0) |
| Population type (N = 1004) | |
| General Population | 624 (62.2) |
| Key Population | 326 (32.5) |
| Priority Population | 54 (5.3) |
| Facility (N=1058) | |
| HBCTRH | 226 (21.4) |
| Makongeni DICE | 489 (46.2) |
| Marindi SCH | 116 (11.0) |
| Miniambo HC | 163 (15.4) |
| Nyalkiny Disp | 64 (6.0) |
| Reason for PrEP initiation (N = 773) | |
| Key population risk | 185 (23.9) |
| Other/unspecified | 67 (8.7) |
| Partner-related risk | 293 (37.9) |
| Sexual risk behaviours | 228 (29.5) |
Table 2: EMR data completeness by facility in Homabay town Sub-county, January–March 2023
| Indicator | HBCTRH | Makongeni DICE | Marindi | Miniambo | Nyalkinyi | Average |
|---|---|---|---|---|---|---|
| Sex | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Age | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Population type | 90.6% | 94.1% | 98.4% | 100.0% | 99.1% | 96.4% |
| Assessed | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Eligible | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| PrEP initiation date | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Reason for PrEP initiation | 92.4% | 76.5% | 75.6% | 35.2% | 68.8% | 69.7% |
| HTS done | 91.5% | 94.5% | 98.4% | 100.0% | 100.0% | 96.9% |
| STI screened | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Adherence | 13.5% | 58.3% | 22.8% | 15.8% | 18.8% | 25.8% |
| Received adherence counselling | 99.5% | 98.8% | 96.7% | 100.0% | 87.5% | 96.5% |
| PrEP status | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Reason for discontinuation | 14.8% | 0.0% | 0.0% | 0.6% | 0.0% | 3.0% |
| Average | 84.8% | 86.3% | 84.0% | 80.9% | 82.6% | 83.7% |
Note: Cell-level shading indicates data completeness below the 95% benchmark recommended for routine health information systems. Shading is applied for descriptive flagging and does not alter the benchmark definition.
| Facilities | January – March 2021 | January – March 2022 | January – March 2023 | |||
|---|---|---|---|---|---|---|
| Rate | Timeliness | Rate | Timeliness | Rate | Timeliness | |
| HBCTRH | 66.70% | 0% | 100% | 33.30% | 100% | 100% |
| Marindi SCH | 100% | 100% | 100% | 100% | 100% | 66.70% |
| Makongeni DICE | 100% | 100% | 100% | 100% | 33.30% | 33.30% |
| Miniambo HC | 100% | 100% | 100% | 100% | 100% | 100% |
| Nyalkinyi Dispensory | 100% | 100% | 100% | 100% | 100% | 100% |