Research | Open Access | Volume 9 (2): Article 62 | Published: 15 Apr 2026

Views: 2,674
Menu, Tables and Figures
| Table 1: Age- and Sex-Specific Diarrheal Morbidity in Children Under Five, Hohoe Municipality, 2017-2021 | |||||
|---|---|---|---|---|---|
| Sex, age | Period (years) | ||||
| 2017 | 2018 | 2019 | 2020 | 2021 | |
| Males <28 days | 32 | 1 | 4 | 3 | 1 |
| Females <28 days | 5 | 1 | 1 | 1 | 3 |
| Males 1-11 months | 464 | 483 | 475 | 285 | 253 |
| Females 1-11 months | 310 | 398 | 484 | 270 | 262 |
| Males 12-59 months | 876 | 1463 | 1190 | 778 | 721 |
| Females 12-59 months | 834 | 1240 | 1089 | 678 | 687 |
Table 1: Age- and Sex-Specific Diarrheal Morbidity in Children Under Five, Hohoe Municipality, 2017-2021
Sadat Ibrahim1,2,3,&, Yussif Yakubu1,2, Eric Kporsu3, Agorde Richmond Ferguson1, Yahuza Sabit Tanko1, Kwaku Apiagyei1,2
1Department of Epidemiology and Biostatistics, Fred N. Binka School of Public Health, University of Health and Allied Sciences, Ho, Volta Region, Ghana, 2Ghana Field Epidemiology Laboratory Training Program, 3KNUST-International Vaccine Institute Collaborative Center, Asante Akim Agogo, Ashanti Region, Ghana
&Corresponding author: Sadat Ibrahim, Department of Epidemiology and Biostatistics, Fred N. Binka School of Public Health, University of Health and Allied Sciences, Ho, Volta Region, Ghana, Email: sadathajjuhas@gmail.com ORCID: https://orcid.org/0009-0007-9374-4074
Received: 31 Oct 2025, Accepted: 11 Apr 2026, Published: 15 Apr 2026
Domain: Infectious Disease Epidemiology
Keywords: Epidemiology, Diarrheal disease, Under-five children, Ghana
©Sadat Ibrahim et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Sadat Ibrahim et al., Epidemiology of diarrheal disease in children under five years, Hohoe Municipality, Ghana, 2017 – 2021. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):62. https://doi.org/10.37432/jieph-d-25-00264
Introduction: Diarrheal disease remains a major contributor to childhood morbidity and mortality in resource-constrained settings, particularly sub-Saharan Africa. Despite significant progress in prevention and management, diarrheal illness persists as a major public health problem in Ghana. We assessed a five-year pattern of diarrheal morbidity in children aged 0-59 months by examining epidemiological trends, including demographic distribution and seasonal variation in Hohoe Municipality, to guide localized interventions.
Methods: A retrospective descriptive study was conducted using routinely collected outpatient surveillance data from Hohoe Municipality. The dataset recorded 13,292 diarrheal cases from January 1, 2017, to December 31, 2021 and was sourced from the District Health Information Management System II of the Ghana Health Service. The extracted data were analyzed by age, sex, and year. Descriptive statistics using percentages were computed, and temporal trends were visualized using Microsoft Excel 2018 to assess annual and seasonal fluctuations.
Results: A total of 13,292 diarrheal cases from 2017 to 2021 were included in the analysis. The prevalence fluctuated between 2,015 (9.97%) and 3,586 (18.57%), peaking in 2018 and showing a resurgence in 2021. Children aged 12-59 months accounted for the largest proportion of cases, 9,556 (71.89%), followed by those aged 1-11 months (27.72%), while neonates contributed less than 2% of reported cases. Male children consistently recorded slightly higher prevalence than females. Clear seasonal peaks were observed between March and July, aligning with the early wet season.
Conclusion: Diarrheal morbidity among children under five in Hohoe Municipality remained high with year-to-year fluctuations and a resurgence in 2021. Children aged 12-59 months and males recorded the highest case proportion. Clear peaks during the early wet season highlight the role of environmental factors. Strengthening surveillance systems to include pathogen-specific data will further enhance local public health response and policy planning.
Diarrheal disease is an infectious disease caused by viruses, bacteria or parasites. Globally, it is rated a major public health challenge, particularly in low and middle-income countries, where it contributes significantly to morbidity, mortality, and economic burden among households with young children. Diarrhoea is clinically defined as the passage of three or more loose or watery stools within 24 hours or a noticeable decrease in stool consistency compared with a patient’s normal pattern. It is further categorised as acute if it lasts less than 14 days and chronic or persistent if it lasts 14 days or longer. Acute watery diarrhoea, such as cholera, is a distinct clinical form often associated with rapid dehydration and severe outcomes [1–3]. Children under five remain highly vulnerable because of their fragile immune system and frequent exposure to contaminated environments.
Globally, diarrheal disease is the second leading cause of morbidity and mortality in children under five years, accounting for approximately 525,000 deaths annually, or 8% of all child deaths [4,5]. In 2019, diarrhoea was responsible for about 9% of under-five deaths worldwide, translating to more than 1,300 deaths each day, despite the availability of effective, low-cost treatments such as oral rehydration solution [6,7]. Each year, more than 910 million diarrheal episodes occur among children globally, with the greatest burden emanating from South Asia and sub-Saharan Africa [8,9]. In Ghana, diarrhoea consistently ranks among the top ten causes of morbidity and mortality, with an estimated 1,700 under-five deaths in 2015 attributed to the disease [10]. It is implicated in about 9% of under-five deaths in Ghana, with an estimated 113,786 annual cases, including 2,318 severe presentations and 354 deaths, yielding a case fatality rate of 0.31% [9].
While mortality rates from diarrhoea are highest in young children, older children aged 6-14 years and adults also experience substantial morbidity, with nearly 2.8 billion diarrheal episodes annually in these groups [4]. Pathogens such as rotavirus and Escherichia coli are recognized as the most common etiological agents of moderate-to-severe diarrhoea in low-income countries, with rotavirus alone responsible for approximately 40% of hospital admissions related to diarrhoea among children under five [1,11]. The primary determinants of diarrheal disease include inadequate access to safe drinking water, poor sanitation, malnutrition, and substandard housing conditions [11,12].
Globally, an estimated 780 million people lack potable water and 2.5 billion lack improved sanitation [13]. The majority of diarrheal cases and deaths, nearly 88% are attributed to unsafe water, poor sanitation, and insufficient hygiene, with the highest burden occurring before a child’s second birthday [12,14,15]. Children under three years in low-income settings experience an average of three diarrheal episodes per year [13].
Despite its high burden, diarrheal disease is both preventable and treatable through interventions such as safe drinking water and sanitation improvements, exclusive breastfeeding, appropriate complementary feeding, rotavirus vaccine availability, oral rehydration therapy, and food safety measures [12,16]. These strategies are central to achieving Sustainable Development Goal 3, which endeavours to end preventable deaths of newborns and children under five by 2030 [16]. In spite of the availability of these cost-effective interventions, the burden of diarrheal disease remains significant in many settings, including Ghana, where national surveillance consistently ranks diarrhoea among the leading causes of outpatient morbidity.
Effective surveillance is essential for understanding disease burden; however, in many low-income countries, existing systems are largely passive and often limited to short-term reporting. Such limitations hamper the ability to capture long-term variations in disease occurrence and distribution. While routine surveillance systems generate a wealth of health data, these datasets are not always analyzed or disseminated to support local decision-making. In the Hohoe Municipality, diarrheal disease continues to be a key driver of childhood illness; yet, there is limited published evidence examining multi-year epidemiological trends specific to the administrative area, despite persistent water, sanitation, and hygiene (WASH) challenges.
Thus, we analyzed a five-year trend of diarrheal morbidity and explored demographic patterns by age and sex. We also identified seasonal variations observed in routine surveillance data to enhance understanding of the existing burden and support evidence-based municipal-level public health planning.
Study setting
This study was conducted in Hohoe Municipality, one of the 18 administrative districts in Ghana’s Volta Region, with Hohoe as its capital. The municipality covers a land area of about 1,172 km² and is bordered by Jasikan District to the north, Biakoye District to the northwest, Kpando Municipality and Afadzato South District to the south and southwest, and the Republic of Togo to the east [17]. According to the 2021 Population and Housing Census, Hohoe has a population of approximately 114,000, with a slightly higher proportion of females (52%) than males (48%), and over half of the residents live in urban areas [17]. Children under five are estimated to number about 12,000 – 13,000, forming the key at-risk population for diarrheal disease [17].
The municipality is predominantly semi-urban, with population density concentrated in Hohoe town, while the surrounding rural communities are more sparsely populated. Access to improved drinking water sources is relatively high, driven by piped water supplied from the River Dayi in urban areas and boreholes, small-town water systems, and protected wells in rural settlements, while sanitation access remains mixed, with a substantial proportion of households relying on public or shared facilities. Hohoe lies within the forest-savanna transitional zone and experiences a tropical climate with two rainy seasons (May-July and August-October) and a dry Harmattan season from November to February.
The health system consists of four sub-districts (Hohoe, Agumatsa, Alavanyo, and Gbi), eight health centers, and six community-based health planning and services (CHPS) compounds all of which routinely report data to the national health information system (DHIMS-II), the source of our study data. The Volta Regional Hospital, situated in Hohoe serves as the primary referral centre, delivering essential and specialised healthcare services to the municipality and surrounding districts.
Study design
This study was a retrospective descriptive study of routine outpatient surveillance records on diarrheal disease among children aged 1-59 months. The records reviewed covered a five-year period from January 1, 2017 to December 31, 2021. The period 2017-2021 was selected because it represented the most recent continuous five-year dataset that had undergone routine validation by the municipal health authorities at the time this study was conceptualised. Data were sourced from the District Health Information Management System II (DHIMS-2), a routine electronic database of the Ghana Health Service between March 6 and March 30, 2023.
Standard case definition of diarrheal disease
A case of acute diarrhoea was defined as the passage of three or more abnormally loose or watery stools within 24 hours, with or without additional symptoms such as fever (axillary temperature ≥38°C), abdominal cramps, nausea, or vomiting [18].
Study variables and data extraction
The study utilised data from the routine passive surveillance system conducted year-round across all sub-districts and health facilities within the Hohoe Municipality. This system routinely collects information on childhood diarrheal disease among children under five years, diagnosed based on standard clinical symptoms at the point of care. The main variables of interest were sex, age and confirmed diarrheal disease case count. Following administrative approval, we worked with the Municipal Health Information Officer to identify relevant diarrheal disease indicators for children under five. Using the disease surveillance module, we retrieved monthly case counts for the period disaggregated by sex and age group (<28 days, 1-11 months, and 12-59 months).
We exported the data in Microsoft Excel format and undertook verification of reporting completeness, assessment for missing or duplicate entries, and consistency checks between aggregated and disaggregated counts. We also obtained population estimates from the Hohoe Municipal and Volta Regional Health Directorates for the corresponding years to support the interpretation of the data obtained. The retrieved data were disaggregated routine surveillance summaries extracted from DHIMS-2 and were already anonymized at the point of reporting, with no case-level or personal identifiers available to the research team. As such, no additional anonymization was required, and in the use of the data, we ensured full compliance with confidentiality and data protection standards.
Statistical analysis
The disaggregated diarrheal case counts were exported from the DHIMS-2 platform and organized according to sex and predefined age groups (<28 days, 1-11 months, and 12-59 months), consistent with the standard DHIMS-2 age categorization. Descriptive statistics were used to summarize the distribution of cases across age, sex, month, and year. For each age group and sex, we calculated the proportion of cases by dividing the number of cases reported in that category by the total under-five diarrheal cases for the corresponding year and multiplied by 100. Further, we examined temporal patterns by plotting monthly and annual case counts to visualise long-term and seasonal variations from 2017 to 2021. Seasonal trends were assessed by examining cyclical fluctuations in monthly counts across the five years. We generated all summaries and visualisations in tables and graphs with Microsoft Excel 2018.
Ethical considerations
Administrative approval to access diarrheal disease data in children under five was obtained from the Hohoe Municipal Health Directorate of the Ghana Health Service through the Ghana Field Epidemiology and Laboratory Training Program, University of Health and Allied Sciences. The study was solely a secondary data analysis of anonymized, facility-level surveillance data and did not include any direct contact with human subjects. Therefore, informed consent was not required. Data-sharing agreements were observed, and all institutional guidelines for data access, confidentiality, and use were strictly followed.
Age and sex-specific diarrheal morbidity in children under five
A total of 13,292 childhood diarrheal cases, comprising 7,029 males and 6,263 females, were recorded from 2017 to 2021. Annual case totals were 2,521 in 2017, 3,586 in 2018, 3,243 in 2019, 2,015 in 2020, and 1,927 in 2021. Across the five-year period, children aged 12-59 months accounted for the largest proportion of cases (9,556), followed by those aged 1-11 months (3,684), while neonates aged <28 days contributed the fewest cases (52). Among children aged 12-59 months, male cases increased from 876 in 2017 to a peak of 1,463 in 2018, then declined to 1,190 in 2019, 778 in 2020, and 721 in 2021. Female cases in the same age group followed a similar pattern, rising from 834 in 2017 to 1,240 in 2018 and 1,089 in 2019, before decreasing to 678 in 2020 and 687 in 2021. In the 1-11-month age group, male cases were 464, 483, 475, 285, and 253 from 2017 to 2021, respectively, while female cases were 310, 398, 484, 270, and 262 across the same years. The <28-day age group recorded the lowest counts throughout the study period. Male neonates reported 32, 1, 4, 3, and 1 cases from 2017 to 2021, respectively, while female neonates recorded 5, 1, 1, 1, and 3 cases (Table 1).
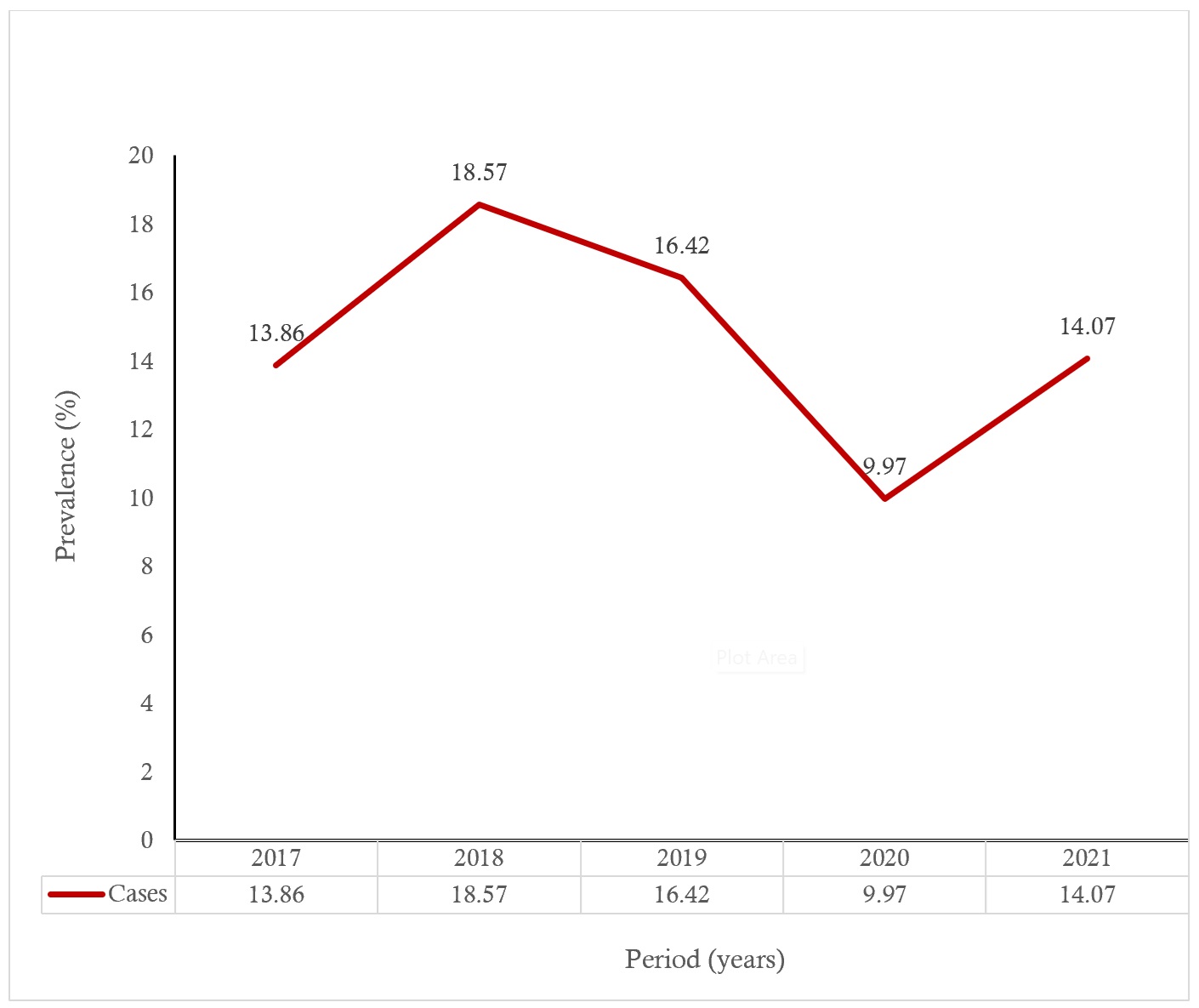
Trend of diarrheal disease prevalence in children under five
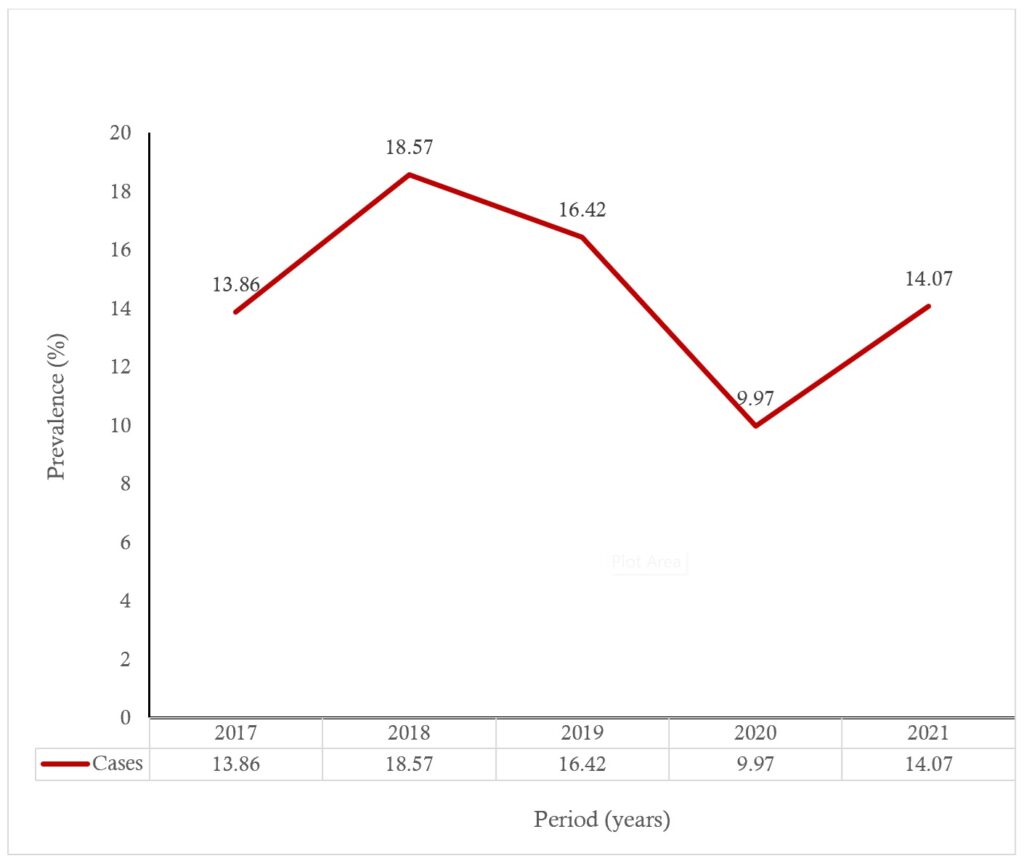
The trend in diarrheal disease among children under five in Hohoe Municipality from 2017 to 2021 showed fluctuating prevalence over the years (Figure 1). In 2017, the prevalence was 2521 (13.36%), which increased markedly to 3,586 (18.57%) in 2018, representing the highest rate during the study period. This rise was followed by a sharp decline to 9.97% in 2020, indicating a substantial reduction in reported cases. However, in 2021, the prevalence increased again to 1,927 (14.07%), suggesting a resurgence of diarrheal diseases after the decline observed in the preceding year.
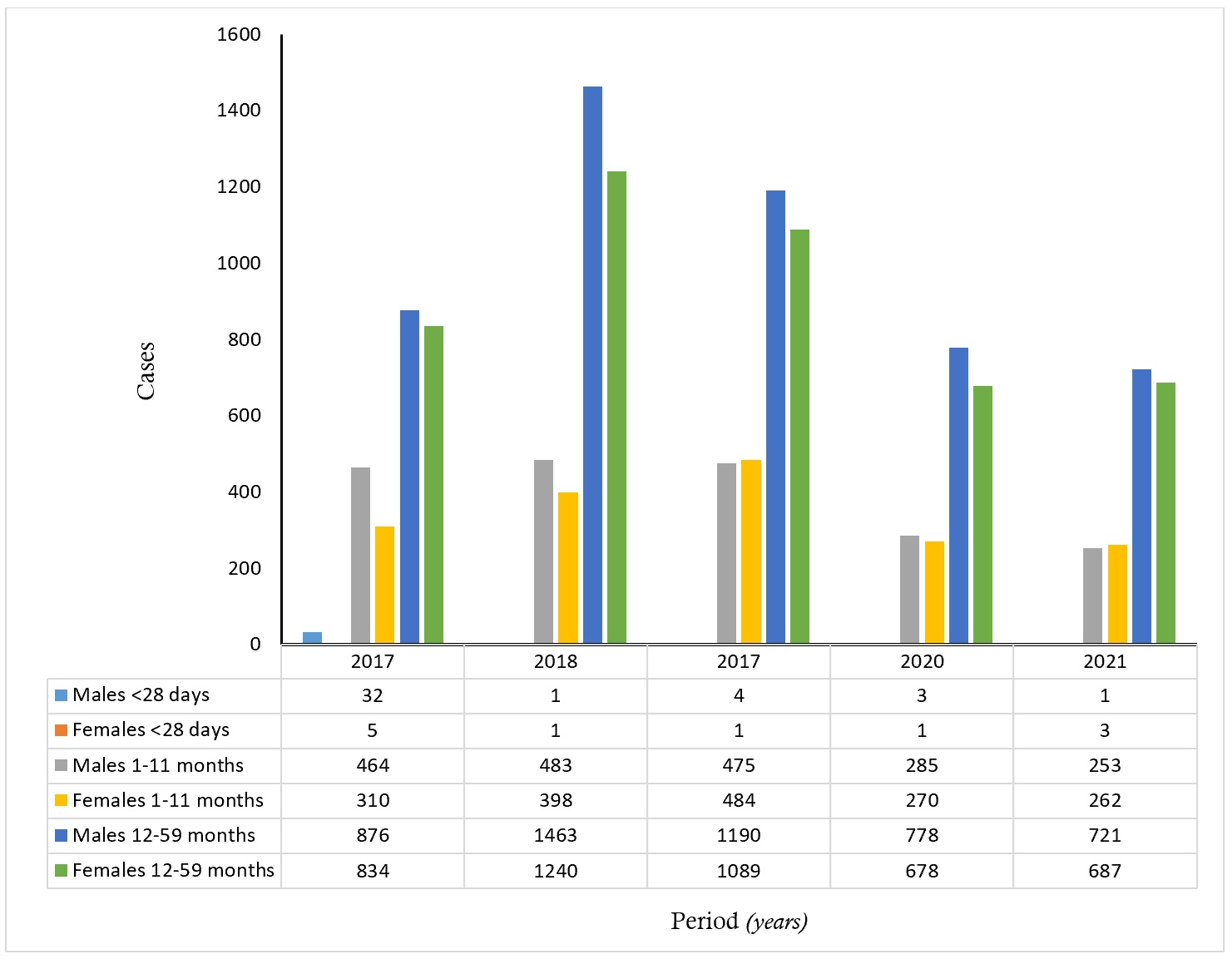
Age and sex distribution of diarrheal disease cases in children under five
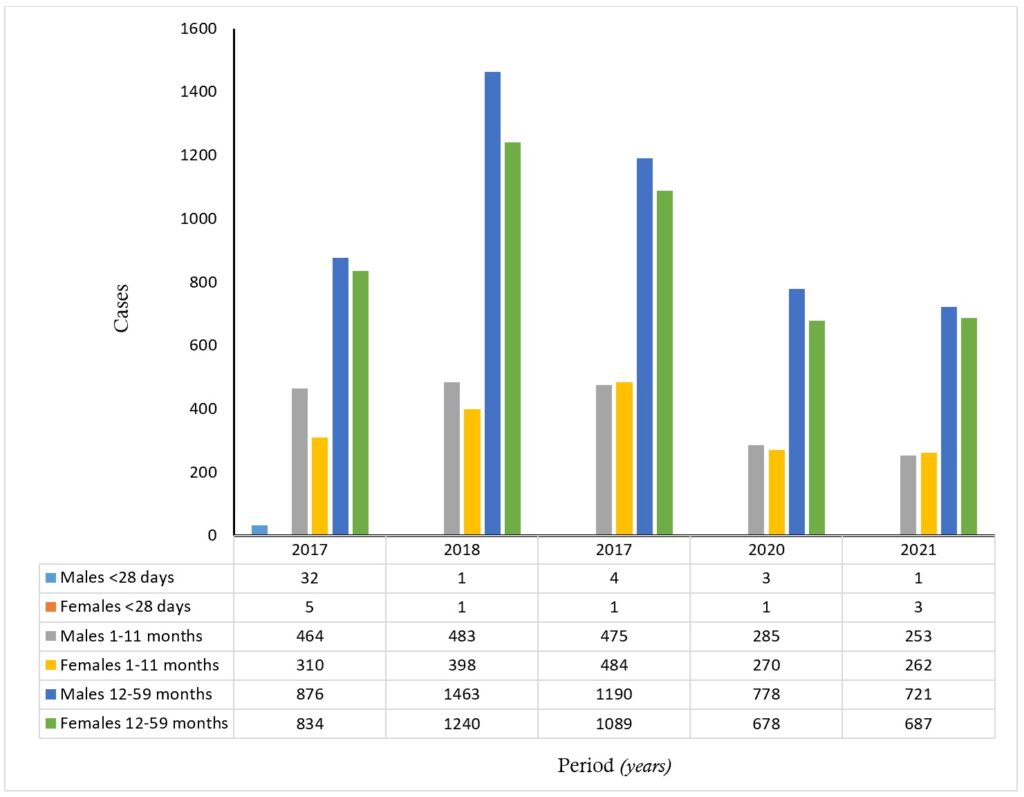
In Figure 2 below, from 2017 to 2021, the highest number of cases consistently occurred among children aged 12-59 months, followed by those aged 1-11 months, while infants below 28 days recorded the lowest number of cases throughout the study period. Among the 12-59-month-olds, male children generally exhibited higher case counts than females across all years, with the peak observed in 2018 (1,463 cases for males and 1,240 for females). A similar pattern was seen among children aged 1-11 months, where male cases were slightly higher than female cases in most years. For infants below 28 days, the number of cases remained very low, with minimal fluctuations between years for both sexes. Overall, diarrheal disease was most prevalent among older under-five children (12-59 months), with male children consistently experiencing more cases than females.
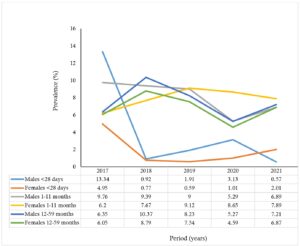
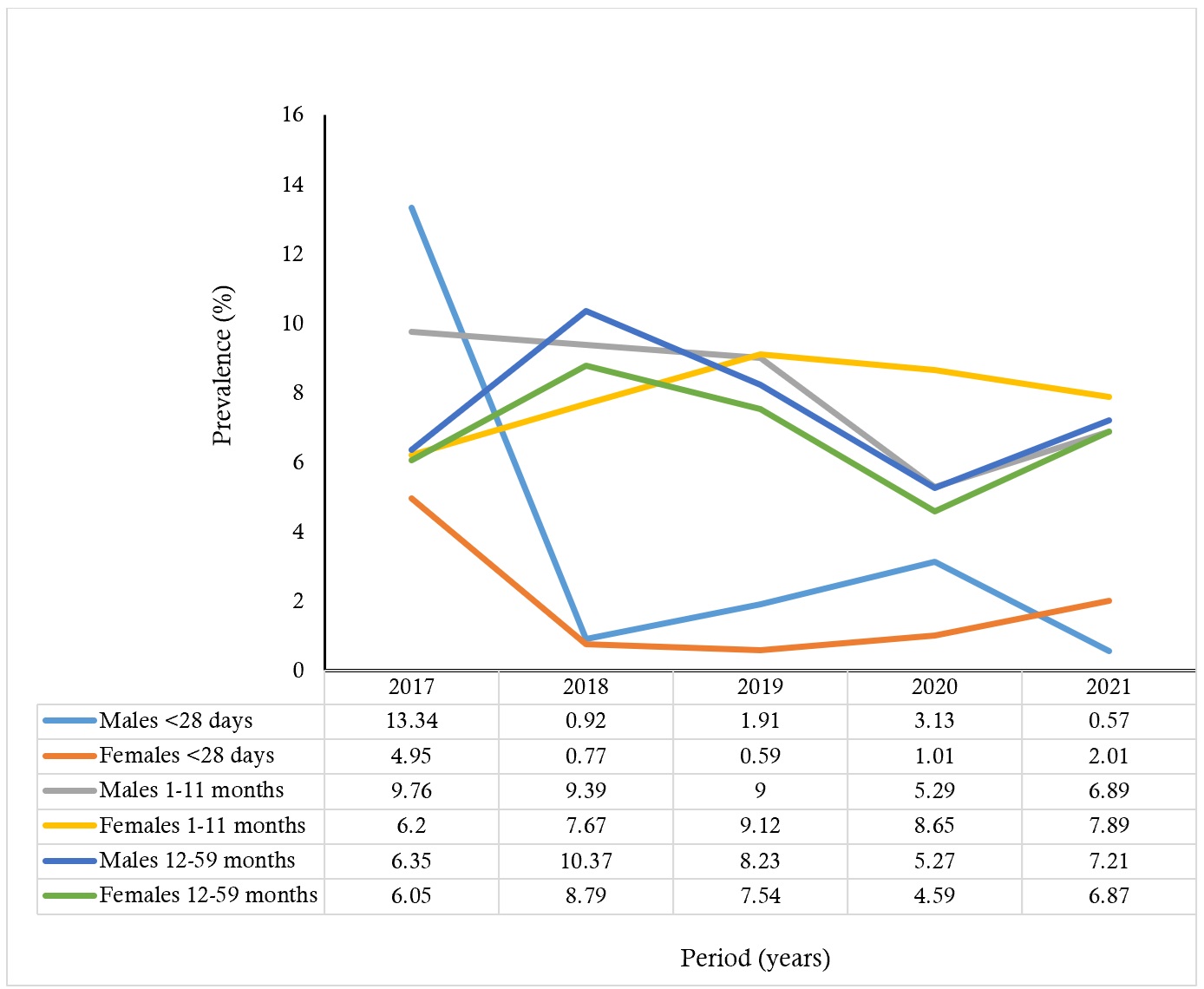
Prevalence of diarrheal disease by age group and sex in children under five
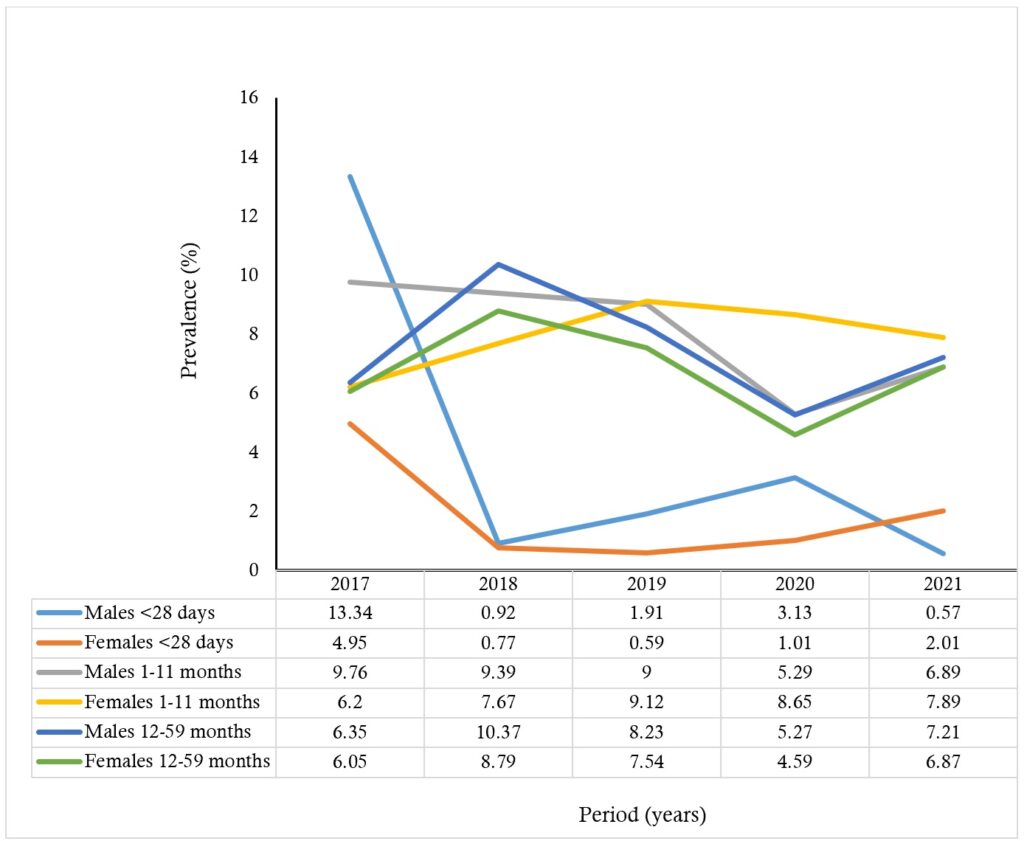
Overall, the prevalence fluctuated across both age and sex groups during the study period. Among males under one year, prevalence declined from 496 (9.76%) in 2017 to 288 (5.29%) in 2020, before rising slightly to 254 (6.89% in 2021. In contrast, females under one year gradually increased from 315 (6.20%) in 2017 to a peak of 485 (9.12%) in 2019, followed by a slight decrease to 265 (7.89%) in 2021. A similar fluctuating pattern was observed for children aged 12-59 months. The prevalence among males increased from 876 (6.35%) in 2017 to 1,463 (10.37%) in 2018, then declined steadily to 778 (5.27%) in 2020, with a subsequent rise to 721 (7.21%) in 2021. Among females in this age group, prevalence rose from 634 (6.05%) in 2017 to 1,240 (8.79%) in 2018, then decreased to 678 (4.59%) in 2020, before rising again to 687 (6.87%) in 2021 (Figure 3).
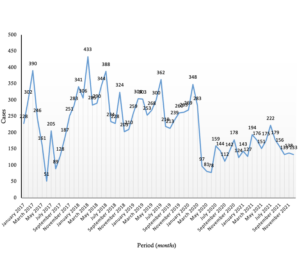
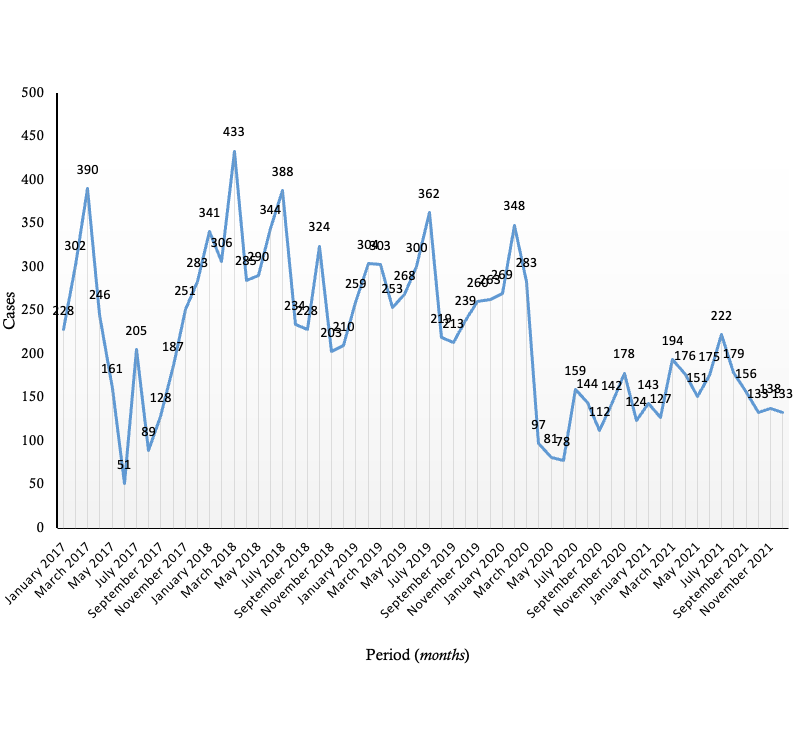
Seasonal trends of diarrheal disease
In the time series graph below, the data show distinct seasonal fluctuations, with peaks and troughs repeating annually (Figure 4). Childhood diarrheal cases in Hohoe Municipality showed a repeating seasonal cycle from 2017 to 2021. In 2017, cases rose from 228 in January to a peak of 390 in May, then declined through the end of the year. Across the five-year period, the highest peaks in cases were consistently observed between March and July, including major surges in May 2019 (433 cases) and July 2021 (362 cases). Consistent declines followed from September to January each year, with some of the lowest values recorded during the dry season, such as the sharp drop to 51 cases in November 2017.
This study analysed a five-year trend (2017-2021) of diarrheal disease among children under five years in Hohoe Municipality using routine surveillance data. The overall findings indicate fluctuating but persistently high diarrheal morbidity across the period, with the highest prevalence observed in 2018 and a significant increase in 2021. Although some decline was noted between 2019 and 2020, the continuing magnitude of reported cases suggested that diarrheal disease remains a significant public health concern in this municipality. The study’s erratic pattern is consistent with results from comparable retrospective analyses conducted in Ghana and other low- and middle-income nations [9,14,18,20]. For instance, studies in the Atwima Nwabiagya and Jasikan districts also reported irregular diarrheal patterns, with incidence peaking during certain years and declining in others, often linked to variations in rainfall, sanitation, and water quality [9,18]. This trajectory aligns with evidence from Ethiopia and Nigeria, where diarrheal incidence in children under five was found to increase during the rainy season due to contamination of water sources and poor sanitation [14,19].
When contextualized within national estimates, the prevalence observed in Hohoe Municipality appears substantial. National surveys in Ghana, including the Ghana Demographic and Health Survey, have reported under-five diarrheal prevalence ranging between approximately 12% and 19% in recent years [21]. The municipal-level prevalence recorded in this study, particularly the peak of 18.57% in 2018, falls within the upper range of national estimates, suggesting that Hohoe reflects the broader national burden while also demonstrating local fluctuations that may be shaped by contextual environmental and infrastructural factors. Interpretation of these findings must be situated within the structural characteristics of the DHIMS-2 platform, which is a passive, facility-based surveillance system. As such, the data are dependent on healthcare utilization patterns and may not fully capture community-level diarrheal episodes that do not present to health facilities. Underreporting, inconsistencies in reporting completeness across facilities, and potential misclassification of clinically diagnosed cases may influence observed trends. These inherent limitations likely shape the magnitude and temporal fluctuations reported and should be considered when interpreting prevalence estimates and seasonal patterns.
The present findings confirm a clear seasonal pattern, with higher cases recorded between March and July, coinciding with the early rainy season. This observation underscores the role of environmental factors such as rainfall and flooding, which facilitate faecal contamination of water and food sources. Similar associations between rainfall and diarrheal outbreaks have been reported in multiple sub-Saharan settings [13,20]. Strengthening water safety management, especially during the rainy season, is therefore important for reducing diarrheal morbidity in endemic communities.
Our age-specific analysis revealed that diarrheal disease was most frequent among children aged 12-59 months, followed by infants aged 1-11 months. This outcome is consistent with national and regional surveys showing increased diarrheal risk among children transitioning from exclusive breastfeeding to complementary feeding [21,15. The higher number of reported cases among older under-fives likely reflects greater environmental exposure, behavioral risk (such as crawling and hand-to-mouth activity), and reduced passive immunity from breastfeeding. These findings reinforce the need for targeted health education on hygiene and food safety for caregivers of young children. Sex-based differences were modest, though male children consistently experienced slightly higher diarrheal prevalence than females. Similar male predominance has been documented in other Ghanaian and African studies [22,12], potentially reflecting behavioral differences or differential care-seeking patterns. Male children may be at slightly higher risk of diarrheal disease due to delayed care-seeking, greater environmental exposure, and less stringent hygiene supervision compared with female children [23]. In many settings, boys are often allowed more outdoor play and exploratory activities at an earlier age, which may increase contact with contaminated surfaces, soil, or water sources, while caregivers may also perceive male illness differently, potentially influencing the timing and pattern of health-seeking behaviour.
In addition to these age-related patterns, rotavirus remains an important cause of diarrheal illness in early childhood and is responsible for many of the severe episodes seen in health facilities [1]. The virus spreads easily among infants and toddlers and often presents with a sudden onset of vomiting, fever, and profuse watery diarrhoea. Although Ghana has integrated the rotavirus vaccine into its routine immunisation schedule, incomplete or delayed vaccination can still leave some children exposed during their most vulnerable period. Countries with high vaccine uptake have recorded sharp declines in rotavirus-related hospital admissions, highlighting the value of maintaining strong coverage [11]. Ensuring timely completion of the vaccine schedule and reinforcing vaccine education during child welfare clinic visits could help reduce the severity and frequency of diarrheal episodes in settings such as Hohoe Municipality.
Future studies should investigate pathogen-specific causes and integrate more granular meteorological indicators such as rainfall intensity, cumulative monthly precipitation, flooding events, ambient temperature, and humidity levels to better quantify environmental influences on diarrheal transmission. Incorporating socioeconomic variables, including household wealth quintile, maternal education, access to improved water and sanitation facilities, population density, and housing conditions, would further strengthen understanding of structural determinants and enable more targeted district-level interventions.
Study limitations
We acknowledge some limitations of the study; therefore, findings should be interpreted in light thereof. First, this study employed a retrospective ecological design using aggregated routine surveillance data structured by monthly diarrheal case counts stratified by sex and predefined age groups (<28 days, 1-11 months, and 12-59 months). This structure did not include any case-level information and, therefore, allowed us to only describe temporal, age-specific, and sex-specific patterns. As a result, we were unable to examine characteristics such as household WASH conditions, feeding practices, or caregiver factors. Thus, we were unable to draw any causal inferences on specific risk factors due to the population-level aggregated nature of the data. It is also worth noting that DHIMS-2 data may be constrained by issues such as underreporting, overreporting, and misclassification due to variability in facility reporting practices, which can affect the completeness and accuracy of diarrheal case counts. Nonetheless, DHIMS-2 remains Ghana’s primary platform for standardized and continuous district-level surveillance.
This review of five years of routine surveillance data shows that diarrheal morbidity among children under five in Hohoe Municipality remained high and varied by year. The highest prevalence was recorded in 2018, followed by a decline through 2020 and an increase again in 2021. Children aged 1-59 months consistently accounted for most cases, and males recorded slightly higher prevalence across age groups. The analysis also identified clear seasonal increases during the early rainy months, suggesting the influence of environmental and seasonal conditions. Although the dataset does not include pathogen-specific or household-level risk information, the findings provide a clearer understanding of temporal and demographic patterns of diarrheal disease in the municipality. These trends offer useful evidence for local planning and for prioritizing resources to address periods and populations at greater risk.
Recommendations
The findings point to clear seasonal peaks and ongoing gaps in sanitation, water safety and surveillance. The Municipal Health Directorate should intensify WASH activities between March and July, focusing on safe drinking water, household water treatment, and handwashing and food hygiene education.
Moreover, regular training and supportive supervision are imperative to improve the accuracy and timeliness of DHIMS-2 reporting, helping reduce inconsistencies in routine surveillance data and improving the municipality’s ability to detect trends timely. The study adduces evidence to expand surveillance to include pathogen-specific laboratory confirmation, particularly for common causes such as rotavirus. Building basic diagnostic capacity at the district or regional level would support more targeted public health action, guide vaccine-related planning, and strengthen outbreak response.
What is already known about the topic
What this study adds
The authors wish to express their sincere appreciation to the mentors of the Ghana Field Epidemiology and Laboratory Training Programme for their valuable guidance and support. We are also grateful to the Hohoe Municipal Health Directorate for their cooperation in granting permission and providing access to the data used in this study.
SI, RAF, KA, and YY conceptualized the study and prepared the initial draft. Data extraction was performed by SI, YY, YST, and RAF, while data curation and formal analyses were carried out by SI, YST, and EK Data interpretation was conducted by YST, EK, and YY The manuscript was edited and critically reviewed by EK, YY, RAF, YST, and KA, with overall supervision provided by KA. All authors reviewed and approved the final version of the manuscript.
| Table 1: Age- and Sex-Specific Diarrheal Morbidity in Children Under Five, Hohoe Municipality, 2017-2021 | |||||
|---|---|---|---|---|---|
| Sex, age | Period (years) | ||||
| 2017 | 2018 | 2019 | 2020 | 2021 | |
| Males <28 days | 32 | 1 | 4 | 3 | 1 |
| Females <28 days | 5 | 1 | 1 | 1 | 3 |
| Males 1-11 months | 464 | 483 | 475 | 285 | 253 |
| Females 1-11 months | 310 | 398 | 484 | 270 | 262 |
| Males 12-59 months | 876 | 1463 | 1190 | 778 | 721 |
| Females 12-59 months | 834 | 1240 | 1089 | 678 | 687 |