Outbreak Investigation | Open Access | Volume 9 (Suppl 13): Article 02 | Published: 28 Apr 2026
Views: 683
Menu, Tables and Figures
| Variable | Frequency N=180 | Percentage (%) |
|---|---|---|
| Sex | ||
| Female | 95 | 53 |
| Male | 85 | 47 |
| Age (years) | Median age = 2 years. IQR; 1-3 years | |
| 0-4 | 147 | 81.7 |
| 5-9 | 16 | 8.9 |
| 10-14 | 4 | 2.2 |
| 15+ | 13 | 7.2 |
| Outcome | ||
| Alive | 180 | 100 |
| Dead | 0 | 0 |
Table 1: Distribution of measles cases in Moroto district by sex, age and outcome
Ajumo Mary Goretti1,&, Bernard Lubwama2, Tusiime Wilson1, Katusiime Clare1, Akello Linda Mercy1, Lutgard Musiime1, Arac Oscar1, Suzanne Namusoke Kiwanuka1
1Department of Health Policy, Planning and Management, School of Public Health, Makerere University, Kampala, Uganda, 2Division of Integrated Epidemiology and Surveillance, Ministry of Health, Kampala, Uganda
&Corresponding author: Mary Goretti Ajumo, Department of Health Policy, Planning and Management, School of Public Health, Makerere University, Kampala, Uganda, Email: marygajumo@gmail.com, ORCID: https://orcid.org/0009-0005-5243-8420
Received: 15 Oct 2025, Accepted: 23 Apr 2026, Published: 28 Apr 2026
Domain: Infectious Disease Epidemiology
Keywords: Measles, Outbreak, Uganda, Vaccination, Cross-border movement
©Ajumo Mary Goretti et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Ajumo Mary Goretti et al. Descriptive analysis of measles cases during an outbreak in Northeastern Uganda, July 2024. Journal of Interventional Epidemiology and Public Health. 2026; 9(Suppl 13):02. https://doi.org/10.37432/jieph-d-25-00237
Introduction: In Uganda, measles outbreaks persist due to challenges in public health infrastructure, low vaccination coverage, and socio-economic factors. Moroto District reported a measles outbreak in April 2024 affecting all eight sub-counties. We investigated from April to July 2024 to describe the outbreak and identify predisposing factors in the three most affected sub-counties.
Methods: We reviewed medical records from April to July 2024 in three health facilities in the most affected sub-counties and conducted six key informant interviews with district health officials. A suspected measles case was defined as any person with fever and maculopapular rash plus cough, coryza, or conjunctivitis; a confirmed case in this outbreak was a suspected case with laboratory-confirmed measles IgM or a clinically confirmed case. After confirmation of five cases, subsequent suspected cases were considered measles-positive through epidemiological linkage. Data were analysed in Microsoft Excel to obtain descriptive statistics. Attack rates were computed using the projected sub-county populations from the Uganda Bureau of Statistics, and inductive thematic analysis was used to analyse the qualitative data.
Results: A total of 180 measles cases were reported across the three sub-counties, with no deaths. The majority were females (53%, 95/180), with a median age of 2 years (Interquartile range: 1-3years), and 81.7% (147/180) of cases were children under 4 years. Lotisan Sub-County recorded the highest attack rate (33 cases per 1,000), followed by Rupa (16 cases per 1,000) and Nadunget Town Council (6 cases per 1,000). Peak admissions occurred in July (36 cases). Key informant interviews identified low vaccination coverage, poor housing, and cross-border movement from Turkana County, Kenya, which had an ongoing measles outbreak, as the possible predisposing factors.
Conclusion: The Moroto measles outbreak predominantly affected children under five years, highlighting their vulnerability. The July spike corresponded with the influx of pastoralists from Turkana, Kenya, a measles high-risk area. Strengthening vaccination coverage, border surveillance, and community risk communication is vital for controlling and preventing future outbreaks in pastoralist communities.
Measles is an acute viral respiratory illness that remains a significant public health challenge globally, despite the availability of an effective vaccine [1, 2]. Characterised by high fever, cough, conjunctivitis, and a distinctive rash, measles is highly contagious and spreads from infected persons through respiratory droplets and direct contact with an infected person. It can lead to severe complications and death in susceptible populations, especially unvaccinated young children [3].
Globally, measles remains one of the top five causes of vaccine-preventable morbidity and mortality, with an estimated 107,500 deaths and 10.3 million cases in 2023, representing a 20% increase from 2022. The vaccine coverage for the first dose of measles was 83% both in 2022 and 2023 [4-6].
In sub-Saharan Africa, an estimated incidence rate of 343 cases per 1,000,000 population was reported in the World Health Organisation (WHO) Africa region in 2023 [4]. Measles is endemic in Africa and Asia regions, with approximately 136,000 deaths reported in 2022, and over 95% of measles deaths occurring in nations with inadequate health infrastructure and low per capita income [1].
Uganda has experienced several measles outbreaks over the years despite having a 90% national vaccine coverage for the first dose of measles and 50% for the second dose [4].[1] The outbreaks have been associated with challenges in public health infrastructure, low vaccination coverage, socio-economic factors, stock-outs of measles vaccines at the district and health facility levels, and irregular outreach activities [7]. In 2019, Uganda reported a total of 139 suspected measles cases from 38 districts [8] and in 2023, the country had a measles incidence rate of 9.5/1,000,000 population [9].
On June 18, 2024, Uganda’s Ministry of Health declared a measles outbreak in Moroto district in Karamoja region after 6 out of 12 blood samples tested positive for measles-specific IgM at the Uganda Virus Research Institute (UVRI). The Karamoja sub-region, including Moroto district, has experienced recurrent measles outbreaks in the past. From 2011 to 2018, the region had a measles incidence rate of 2.3 cases per 1,000 people [10], which surged between 2016 and 2020 to 16-31 cases per 1,000 people [11]. The outbreak in Moroto highlights the persistent public health challenges in controlling measles. We conducted a measles outbreak investigation to assess the burden and identify the predisposing factors of the measles outbreak in Moroto district.
Study design and setting
This was an outbreak investigation conducted from April to July 2024 in Moroto District. Moroto district is a border district to Kenya, located in the Karamoja region, North-Eastern Uganda. The district population is predominantly inhabited by pastoralists whose lifestyle is characterised by livestock rearing, seasonal migration in search of pasture and water, and a strong cultural attachment to cattle.
The outbreak affected all the 8 Sub Counties of Moroto district, which included: Lotisan, Rupa, Nadunget town council, Northern division, Loputuk, Southern Division, Katikekile and Tapac, with 3 of the Sub Counties (Rupa, Katikekile and Tapac) bordering Turkana, Kenya. However, our investigation was tailored to the three most burdened sub-counties of Nadunget town council, Rupa and Lotisan, with data collected from the health facilities of Nadunget HCIV, Rupa HCII and St. Pius Kidepo HCIII located in the respective sub-counties.
Case definition
We defined a suspected measles case as any person with fever and maculopapular rash with at least one of the following: cough, runny nose (Coryza) or conjunctivitis (red eyes). A confirmed case was defined as a suspected case with a laboratory-confirmed positive measles IgM [12] or a clinically confirmed case in Moroto district from April 2024 to July 2024. During measles outbreaks, once 5 cases are laboratory confirmed, the rest of the cases are presumed positive for measles through epidemiological linkage.
Data source
Data source included outpatient and inpatient registers of the selected health facilities. We also conducted key informant interviews with the district health officials who were knowledgeable about the measles outbreak.
Sample size and sampling procedure
We reviewed all the medical records from April to July 2024 of patients meeting the measles case definition and six key informants, including the district health officer, the district surveillance focal person, the measles incident commander, a nurse, the World Health Organisation field coordinator and the manager of the Public Health Emergency Operation Centre. These key informants were purposely selected based on their roles and responsibilities in the outbreak response.
Data collection method and procedure
We reviewed the out-patient and in-patient medical records to identify laboratory and clinically confirmed measles cases from health facility records, and a line list was created. The variables collected included the case demographics, the health facility where the case was recorded, the sub-county of residence and the signs and symptoms of each case. A semi-structured key informant interview (KII) guide was used to collect qualitative data from district health officials, and notes were taken. The tool was developed based on existing literature on measles transmission in pastoralist and cross-border settings, and it explored participants’ perspectives on vaccination coverage, population mobility among pastoralist communities, geographic and security barriers to access to immunisation services, cross-border movement and transmission risk, and household living conditions.
Data management and analysis
Data were analysed descriptively in Excel, and attack rates were computed using sub-county populations from the Uganda Bureau of Statistics (UBOS) 2014 census. Spatial mapping was done in Quantum Geographic Information System version 15 (QGIS). The qualitative data were analysed using manual inductive thematic analysis to allow context-specific drivers of transmission to emerge directly from the data. Similar codes from the notes were generated, grouped into categories, and then themes related to the possible predisposing factors in Moroto were developed. The preliminary themes were discussed among team members and the supervisors to validate the interpretations.
Ethical considerations
Ethical approval was obtained from Makerere University School of Public Health Research and Ethics Committee (IRB No: SPH-2024-591). To maintain the confidentiality of patient data, patients’ names were excluded from the collected data and permission to use the medical records was sought from Moroto District Health Office, and Karamoja region Public Health Emergency Operation centre (PHEOC). Verbal informed consent was sought from the district health officials to participate in the interviews.
We reviewed a total of 180 records of measles cases with no deaths recorded, and 95(53%) of the measles cases were females. The median age of measles cases was 2 years (Interquartile range [IQR]: 1-3 years), indicating that the majority of the cases occurred among young children under 4 years, and the age group 15+ years had the least number of cases (Table 1).
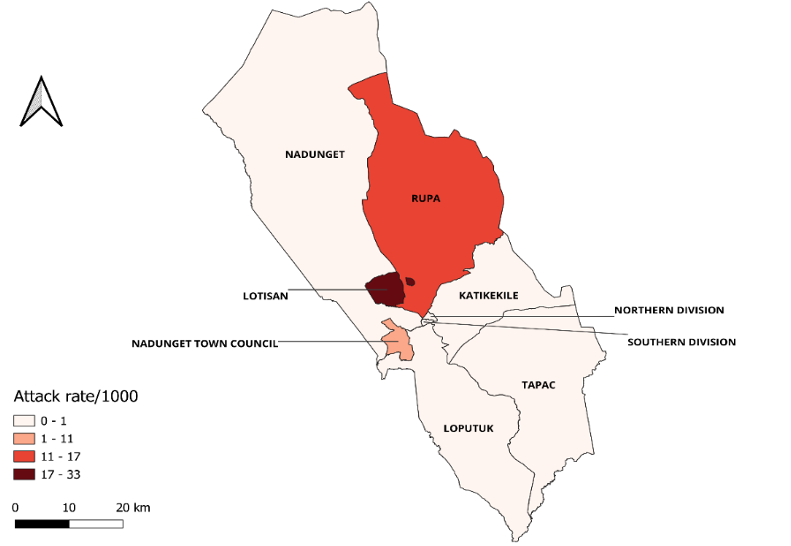
From the records reviewed in the three health facilities serving the high-burdened sub-counties, St. Pius Kidepo HC III in Lotisan Sub- County had 120 cases, Rupa HC II in Rupa Sub- County had 33 cases, and Nadunget HC IV in Nadunget town council had 27 cases. The overall attack rate in the three sub-counties was 18 cases per 1,000 population. Lotisan Sub-County was the most affected with an attack rate (AR) of 33/1000 population as compared to Rupa (16 cases per 1,000 population) and Nadunget (6 cases per 1,000 population) Sub-counties (Figure 1). St. Pius Health centre III in Lotisan Sub- County was one of the health facilities designated for isolation and a treatment centre for measles in Moroto. The health facility admitted a total of 51 cases, with the highest admissions registered in July (36 cases), and only one case in May.
The results from the key informant interviews yielded five themes of the likely predisposing risk factors of measles that is;
Theme 1: Low vaccination coverage
Nearly all the district officials interviewed described that the measles outbreak was linked to low vaccination coverage in Moroto district. Animal health services are more prioritised than health services like immunisation among the pastoralist community of Moroto, hence affecting the uptake of immunisation services in the district.
“…We have a challenge of vaccination coverage, especially for MR2 in all the 8 affected sub-counties. A sub-county like Tapac had a vaccination coverage of 42%, which is very low.” (Public health officer 1).
“…. The problem here is low vaccination coverage because the community here takes animal health as a priority. When an outreach for immunisation for children is organised, very few turn up, but when animal health services are offered in the community, the majority turn up. This needs a one health approach to increase our vaccination coverage.” (District health official 1).
Theme 2: Dominant migrant pastoralists in the community
The results show that communities in Moroto are mainly migrant pastoralists who keep moving from one place to another in search of water and pasture, and this affects the uptake of immunisation services since accessing these communities in one place becomes a challenge.
“…..The communities here are basically nomadic pastoralists; they move from one place to another, looking for water and pasture for their animals. They will not wait for any health outreach like immunisation.” (District Health Official 2).
Theme 3: Limited access to immunisation services
The pastoralists reside in distant kraals, insecure areas and with seasonal rivers cutting off access to immunisation services, thus the low vaccination coverage in most of the sub-counties.
“.…Most areas are hard to reach, some areas are behind here in Mount Moroto, there is insecurity, and many seasonal rivers that are hard to cross” (District Health Official 3).
Theme 4: Increased cross-border movement from Turkana, Kenya
Some of the affected sub-counties, such as Rupa border West Turkana in Kenya, an area that was noted as high-risk areas for measles with a prolonged outbreak. The influx of migrant pastoralists from Turkana in Kenya into the sub-counties of Rupa and Lotisan in Uganda in search of water and pasture for their animals increased the risk of measles transmission.
“…We have high numbers of pastoralists moving from Turkana, Kenya. They come in search of water and pasture. There is a dam that never dries in Lotisan Sub-County. This dam attracts pastoralists from Turkana, Kotido and other districts in the region.” (District Health Official 1).
“…Moroto borders Kenya, and Turkana County in West Kenya has had a prolonged measles outbreak, and I know some of the migrant pastoralists are not vaccinated, leading to the spread of the disease.” (Public health officer 2).
Theme 5: Poor housing conditions
It was also noted that the communities had poor housing conditions, that is, poor ventilation and overcrowding in households, which makes it easy for measles to be spread from one person to another.
“…In the manyattas are households with very many people residing in one small hut that is not ventilated.” (Public health officer 1).
We found that the majority of the measles cases occurred among children aged 0–4 years, and this could be due to low vaccination coverage in the affected sub-counties and the high vulnerability of children below 5 years. The findings are consistent with studies done in Uganda and Ethiopia that showed that children under 4 years had the highest number of measles cases [13, 14].
We observed a relatively high overall attack rate (18/1000 persons) of measles in the three sub-counties, with Lotisan recording the highest rate. This suggests that a significant portion of the population was exposed to and contracted measles, pointing to low immunity levels within the community. Additionally, Lotisan Sub-County hosts a year-round dam that attracts migrant pastoralists from Turkana in Kenya and neighbouring districts. Given that Turkana experienced a prolonged measles outbreak, the influx of pastoralists seeking water and pasture may have contributed to the increased transmission of measles in Lotisan. The attack rate in this outbreak investigation is notably higher than the 12/ 1,000 population reported in a similar study conducted among a pastoralist community in Ethiopia [14]. However, our findings are contrary to the low attack rate (3.2/1000 population) in Nakaseke District, Uganda [15]. This might be explained by the fact that this outbreak was influenced by an ongoing measles outbreak in neighbouring Kenya, compounded by low vaccine coverage.
The spike in measles admissions at St. Pius HCIII in Lotisan sub-county in July may be linked to the seasonal movement of pastoralists in search of water and pasture, as July is typically the start of the dry season. This increased mobility of pastoralists from high-risk areas likely facilitated the spread of measles in Lotisan Sub-County, thus high admissions of measles cases. This observation aligns with findings from a similar study conducted in Zamfara State, Nigeria, which reported a rise in measles cases during the dry season, specifically between October and May [16].
Qualitative analysis showed that there was likely a low vaccine coverage in the three sub-counties, especially for MCV2, lowering the herd immunity. Our findings are in agreement with a global measles surveillance study that showed that measles cases in Burkina Faso in Africa increased despite having a high first dose of measles-containing vaccine (MCV1) coverage (88%) while the second dose (MCV2) coverage remained low at 71% [17]. The low vaccination coverage in Moroto could be due to migrant pastoralism, insecurity and hard-to-reach areas that may have made it hard to access immunisation services. Increased cross-border movement from Turkana, Kenya, where a prolonged measles outbreak occurred, poor housing conditions, such as overcrowding and inadequate ventilation, posed a significant risk of transmission within the communities, thus the need for targeted interventions to improve immunization access. These findings align with other studies done in Nigeria and Ethiopia that showed crowded sleeping spaces, built environment, socio-cultural factors, and low vaccination rates as some of the predisposing factors of measles transmission [18, 19].
This outbreak investigation highlights the critical value of addressing both immunisation coverage and socio-cultural factors in managing measles outbreaks in pastoralist communities in Moroto district. Cross-border movement further emphasises the importance of cross-border coordinated efforts in disease surveillance and immunisation, as isolated efforts may not be sufficient to prevent future outbreaks.
A key strength of our outbreak investigation is its identification of measles transmission dynamics within a pastoralist community, particularly emphasising the influence of migrant pastoralism and cross-border movements on disease spread. This offers valuable insights into how mobile populations affect the epidemiology of vaccine-preventable diseases in border areas and among pastoralist communities.
We recommend effective risk communication by the district health office at the district level, as a key for implementation of mass vaccination campaigns, disease awareness and detection. Collaboration between the district health office for human health and the district veterinary office to address health system gaps, integrate vaccination services with nutrition and animal health services to increase access to immunisation services among the pastoralists based on their lifestyle of prioritising animal health over other health services is critical. This will help prevent future outbreaks. At the national level, there is a need for the Ministry of Health to have a robust surveillance system, including ensuring vaccination of migratory pastoralists, through cross-border collaboration with the neighbour country-Kenya, and this in turn may control the spread of measles from high-risk areas.
Limitations of the outbreak investigation
This outbreak investigation relied on secondary data, which may have missed unreported cases and lacked real-time vaccination information. Only health facilities in high-burden sub-counties were included, limiting representativeness. The small number of key informants, particularly district health officials, restricted qualitative insights into community factors influencing measles transmission. These limitations highlight the need for larger, prospective studies to better understand outbreak dynamics in similar contexts.
These findings demonstrate a high burden of measles in Moroto District, with Lotisan Sub County having the highest attack rate despite mass immunization efforts in the district. Low vaccination coverage, cross-border movement from high-risk areas, and poor housing conditions may have contributed to the outbreak. The presence of migratory pastoralists necessitates targeted immunization strategies to protect the at-risk population.
Strengthening targeted immunization for areas with low vaccination coverage and high migratory pastoralists populations, integrating immunization services with nutrition and animal health services, establishing early warning systems following seasonal movement of pastoralists, strengthening cross border coordination, and promoting risk communication and community engagement are critical to prevent future outbreaks and protect mobile, at-risk populations
What is already known about the topic
What this study adds
It highlights the direct impact of cross-border migration from Turkana (Kenya), a high-risk area as one of the drivers of transmission.
Integration of immunization services with animal health addresses the priorities of the mobile pastoralists.
Appreciation goes to African Field Epidemiology Network (AFENET), Uganda, Ministry of Health surveillance department, Makerere University School of Public Health, Moroto District health leadership, and the regional public health emergency staff for their technical support in the data collection and review of the investigation reports.
| Variable | Frequency N=180 | Percentage (%) |
|---|---|---|
| Sex | ||
| Female | 95 | 53 |
| Male | 85 | 47 |
| Age (years) | Median age = 2 years. IQR; 1-3 years | |
| 0-4 | 147 | 81.7 |
| 5-9 | 16 | 8.9 |
| 10-14 | 4 | 2.2 |
| 15+ | 13 | 7.2 |
| Outcome | ||
| Alive | 180 | 100 |
| Dead | 0 | 0 |