Research | Open Access | Volume 9 (2): Article 71 | Published: 29 Apr 2026

Views: 1,155
Menu, Tables and Figures
| Table 1: Social demographic and clinical characteristics of COVID-19 infections among health workers in Namibia, 2020-2023 | ||
|---|---|---|
| Variables | Frequency (N=4975) | Percentage (%) |
| Sex | ||
| Female | 3595 | 72.3 |
| Male | 1380 | 27.7 |
| Age (Years) | ||
| 15-24 | 386 | 7.7 |
| 25-34 | 2157 | 43.4 |
| 35-44 | 1222 | 24.6 |
| 45-55 | 792 | 15.9 |
| 55+ | 418 | 8.4 |
| Occupation | ||
| Others+ | 2055 | 41.3 |
| Nurse | 1906 | 38.3 |
| Medical doctor | 645 | 13.0 |
| Pharmacy personnel | 194 | 3.9 |
| Environmental Health practitioner | 63 | 1.3 |
| Emergency care practitioner (Paramedics) | 61 | 1.2 |
| Laboratory personnel | 51 | 1.0 |
Table 1: Social demographic and clinical characteristics of COVID-19 infections among health workers in Namibia, 2020-2023
| Table 2: Comorbidities among COVID-19 health workers in Namibia 2020-2023 | ||
|---|---|---|
| Comorbidities (N= 4975) | Present (%) | Absent (%) |
| Other Cardiovascular diseases | 311 (6.3) | 4664 (93.7) |
| Diabetes | 90 (1.8) | 4885 (98.2) |
| Chronic lung disease | 64 (1.7) | 4911 (98.7) |
| HIV | 60 (1.2) | 4915 (98.8) |
| Asthma | 56 (1.1) | 4919 (98.9) |
| Hypertension | 55 (1.1) | 4920 (98.9) |
| Renal disease | 6 (0.1) | 4969 (99.9) |
| Chronic neurological disease | 7 (0.1) | 4968 (99.9) |
| Malignancy | 5 (0.1) | 4970 (99.9) |
| TB | 4 (0.1) | 4971 (99.9) |
| Obesity | 23 (0.5) | 4952 (99.5) |
| Liver Disease | 8 (0.2) | 4967 (99.8) |
Table 2: Comorbidities among COVID-19 health workers in Namibia 2020-2023
| Table 3: Vaccination status of COVID-19 infections and deaths among health workers in Namibia, 2020-2023 | ||
|---|---|---|
| Vaccine status | Frequency (N=4975) | Percentage (%) |
| Vaccinated | 1024 | 20.5 |
| Unvaccinated | 1540 | 31.0 |
| N/A | 2411 | 48.5 |
| Deaths by vaccination status | Frequency (N= 20) | Percentage (%) |
| Vaccinated | 1 | 5.0 |
| Unvaccinated | 7 | 35.0 |
| N/A | 12 | 60.0 |
| N/A: Health workers who were not vaccinated because the vaccination program was not yet rolled out in the country | ||
Table 3: Vaccination status of COVID-19 infections and deaths among health workers in Namibia, 2020-2023
| Table 4: Different types of COVID-19 vaccines received by health workers in Namibia, 2020-2023 | ||||||||
|---|---|---|---|---|---|---|---|---|
| Name of vaccine | One Dose | Two Doses | Three Doses | Four Doses | Not Indicate | Total | Required Dose | Completed course % |
| Sinopharm | 68 | 390 | 33 | 0 | 63 | 554 | 2+Booster | 82.7 |
| AstraZeneca | 52 | 152 | 29 | 0 | 30 | 263 | 2+Booster | 77.6 |
| Johnson&Johnson | 116 | 4 | 1 | 0 | 1 | 122 | 1+Booster | 98.3 |
| Pfizer | 6 | 26 | 11 | 1 | 0 | 44 | 2+Booster | 72.7 |
| Abdala | 0 | 0 | 2 | 1 | 0 | 3 | 3+Booster | 100 |
| Moderna | 0 | 2 | 0 | 0 | 0 | 2 | 2+Booster | 100 |
| Sputnik | 0 | 1 | 0 | 0 | 1 | 2 | 2+Booster | 50 |
| Not Indicated | 6 | 13 | 8 | – | 7 | 34 | – | – |
| Total | 248 | 588 | 84 | 2 | 102 | 1024 | – | – |
Table 4: Different types of COVID-19 vaccines received by health workers in Namibia, 2020-2023
| Table 5: Unadjusted and adjusted Generalized Estimating Equation analysis of factors associated with COVID-19 vaccine uptake among health workers in Namibia, 2020-2023 | ||||||
|---|---|---|---|---|---|---|
| Variables | Vaccination status | Crude odds Ratio (95% CI) | p-value | Adjusted Odds Ratio (95% CI) | p-value | |
| Yes N=1024(%) | No N=1540(%) | |||||
| Gender | ||||||
| Female | 709(69.2) | 1132(73.5) | 0.81 (0.68-0.96) | 0.015 | 0.89 (0.74 -1.07) | 0.214 |
| Male | 315(30.8) | 408(26.5) | Reference | |||
| Age (years) | ||||||
| 15-24 | 47(4.5) | 150(9.7) | 0.44 (0.30 -0.66) | < 0.001 | 0.56 (0.37 -0.85) | 0.006* |
| 25-34 | 439(42.9) | 680(44.2) | 0.91 (0.69 -1.20) | 0.503 | 0.95 (0.71-1.27) | 0.736 |
| 35-44 | 272(26.6) | 373(24.2) | 1.03 (0.76 -1.39) | 0.846 | 1.08 (0.79-1.48) | 0.621 |
| 45-55 | 179(17.5) | 214(13.9) | 1.18 (0.84 -1.67) | 0.336 | 1.08 (0.79 -1.67) | 0.431 |
| 55+ | 87(8.4) | 123(8.0) | Reference | |||
| Occupation | ||||||
| Nurses | 344(33.6) | 597(38.8) | 0.95 (0.61 -1.48) | 0.816 | 0.92 (0.58-1.45) | 0.714 |
| Medical doctor | 184(18.0) | 163(10.6) | 1.86 (1.14 -3.03) | 0.013 | 1.71(1.02-2.87) | 0.041 |
| Others | 429(41.9) | 673(43.7) | 1.05 (0.72 -1.55) | 0.790 | 1.02 (0.69-1.51) | 0.929 |
| Environmental Health practitioners | 12(1.2) | 20(1.3) | 0.99 (0.44 -2.19) | 0.975 | 0.96 (0.43-2.16) | 0.923 |
| Emergency care practitioners (Paramedics) | 14(1.4) | 15(1.0) | 1.54 (0.69 -3.41) | 0.289 | 1.42 (0.63-3.18) | 0.394 |
| Laboratory personnel | 10(0.9) | 21(1.3) | 0.78 (0.35 -1.74) | 0.546 | 0.81 (0.36- 1.82) | 0.607 |
| Pharmacy personnel | 31(3.0) | 51(3.3) | Reference | |||
| Number of Comorbidities | ||||||
| Zero Comorbidities | 880(85.9) | 1418(91.1) | Reference | |||
| One Comorbidity | 66(6.4) | 54(3.5) | 1.97 (1.35 -2.87) | < 0.001 | 1.72 (1.16-2.55) | 0.007* |
| Two – Three Comorbidities | 76(7.4) | 63(4.1) | 1.94 (1.36 -2.77) | < 0.001 | 1.69 (1.17-2.45) | 0.005* |
| > three Comorbidities | 2(0.2) | 5(0.3) | 0.64(0.12 -3.31) | 0.593 | 0.58 (0.11-3.06) | 0.521 |
Table 5: Unadjusted and adjusted Generalized Estimating Equation analysis of factors associated with COVID-19 vaccine uptake among health workers in Namibia, 2020-2023
| Table 6: Regional health facility distribution of COVID-19 case fatality rate among health workers in Namibia, 2020-2023 | |||
|---|---|---|---|
| Region | Cases | Deaths | CFR (%) |
| Erongo | 480 | 2 | 0.42 |
| Hardap | 211 | 0 | 0 |
| Karas | 258 | 1 | 0.39 |
| Kavango East | 268 | 1 | 0.37 |
| Kavango West | 53 | 0 | 0 |
| Khomas | 1686 | 8 | 0.47 |
| Kunene | 153 | 0 | 0 |
| Ohangwena | 228 | 0 | 0 |
| Omaheke | 81 | 0 | 0 |
| Omusati | 288 | 2 | 0.69 |
| Oshana | 578 | 3 | 0.52 |
| Oshikoto | 299 | 2 | 0.67 |
| Otjozondjupa | 309 | 1 | 0.32 |
| Zambezi | 83 | 0 | 0 |
| Total | 4975 | 20 | 0.40 |
Table 6: Regional health facility distribution of COVID-19 case fatality rate among health workers in Namibia, 2020-2023
Maria Mukoya1,2,3,&, Ndeshihafela Sakaria1,2, Loide Ndimulunde2, Roswitha Ndjengwa2, Secilia Nghidishange2, Dianah Ewaga3
1Ministry of Health and Social Services, Windhoek, Namibia, 2Namibia Field Epidemiology and Laboratory Training Programme, Windhoek, Namibia, 3Faculty of Health Sciences and Veterinary Medicine, University of Namibia
&Corresponding Author: Maria Mukoya, Ministry of Health and Social Services, Windhoek, Namibia, Email: mariamukoya@gmail.com ORCID: https://orcid.org/0009-0005-6186-0498
Received: 12 May 2025, Accepted: 28 Apr 2026, Published: 28 Apr 2026
Domain: Infectious Disease Epidemiology
Keywords: COVID-19, Health, Namibia, Vaccination, 2020-2023
©Maria Mukoya et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Maria Mukoya et al., COVID-19 infections and vaccine uptake among health workers in Namibia, 2020–2023. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):71. https://doi.org/10.37432/jieph-d-25-00118
Introduction: COVID-19 infected over 775 million people globally, with Namibia accounting for 172,560 infections and 4,109 deaths from 2020 to 2024. About 4,975 infections and 20 deaths were recorded among health workers from 2020 to 2023 in Namibia. With the launch of COVID-19 vaccine globally, Namibia rolled out the vaccination campaign in March 2021. This study, therefore, described the epidemiology of COVID-19 infections, the level of COVID-19 vaccine uptake and factors associated with vaccine uptake among health workers in Namibia from 2020 to 2023.
Methods: An analytic longitudinal study was conducted. A secondary data analysis using the Namibian national COVID-19-line list was performed. All 4975 documented health workers out of 178965 COVID-19 positive entries in the national COVID-19-line list were captured in this study. A case was defined as any health worker in the Namibia health system with laboratory-confirmed SARS-CoV-2 infection from January 2020 to December 2023. The uptake of the COVID-19 vaccine was defined as any confirmed SARS COV-2 cases who received at least one dose of the COVID-19 vaccine. We assessed associations between independent variables and binary outcomes using Generalised Estimating Equations (GEE) with a logit link and binomial distribution to account for both clustering within regions and correlation arising from repeated measurements among the same individuals using SPSS version 25. Odds ratios (ORs) were determined, and statistical significance was determined at a 95% confidence interval (CI) with a p-value of <0.05.
Results: Out of 4975 cases analysed, 3,595 (72.3%) were female. The age group 25-34 years had the highest number of infections with 2,157 (43.4%). Of the 2,564 health workers eligible for vaccination,1024 (40%) received the COVID-19 vaccine, and out of 20 deaths, 19 (95%) were from the unvaccinated groups. Medical doctors, compared to pharmacy personnel, had a positive association with vaccine uptake (OR = 1.71, 95%CI: 1.02–2.87, p = 0.041). Additionally, comorbidity was a strong predictor of vaccine uptake among health workers.
Conclusion. This study found that less than half of eligible health workers with laboratory-confirmed SARS-CoV-2 infections in Namibia were vaccinated against COVID-19 between 2020 and 2023. Comorbidity was a strong predictor of vaccine uptake among health workers.
COVID-19 infected over 775 million people globally [1], with Namibia accounting for 172,560 infections and 4,109 deaths from 2020 to 2024 [2]. The World Health Organisation [WHO] estimates that between 80,000 and 180,000 health workers died of COVID-19 between January 2020 and May 2021 [3]. Furthermore, about 4,975 infections and 20 deaths were recorded among health workers from 2020 to 2023 in Namibia [3]. Namibia rolled out the COVID-19 vaccination campaign in March 2021 in two of the 14 regions and further rolled out to the rest of the country in April 2021[4]. The rollout targeted the frontline health workers and high-risk individuals to protect them from fatal complications of infection. The uptake of the COVID-19 vaccine has been varied across the regions and the continent.
A systematic review and meta-analysis of COVID-19 vaccine acceptance among healthcare workers in Africa revealed that less than half of healthcare workers accepted the COVID-19 vaccine. This was attributed to concerns about side effects, doubts regarding its safety, short duration of clinical trials, limited information and community trust [5]. Furthermore, findings recorded in Namibia showed a low uptake of COVID-19 vaccines observed in the general public, with only 207, 950[6.9%] Namibians vaccinated, representing a total of 159 881(10.6%) for first dose and only 48,069 (3.2%) second dose from the 1,501,041 (60%) projected targeted population by the MoHSS after four months of the vaccination campaign rollout [4]. The factors that contributed to the low uptake in Namibia included misinformation in the communities. Factors that contributed to the low vaccine uptake among health workers included concerns over the safety and efficacy of the vaccines and vaccine hesitancy [4]. The level of vaccine uptake and factors driving vaccine uptake are unknown among the frontline health workers, given their strategic importance in the effort to contain the pandemic and provide the routine health care services to the populace. This study therefore described the epidemiology of COVID-19 infections, the level of COVID-19 vaccine uptake and factors associated with vaccine uptake among health workers in Namibia from 2020 to 2023.
Study design and setting
A longitudinal study was conducted among health workers in Namibia using secondary data from the Namibian national COVID-19-line list. Namibia has a population of about three million people, with 51.3% being female [8]. Namibia is served by 36 hospitals, 56 health centers, 322 clinics,1150 outreach points and over 200 private health facilities. Windhoek Central Hospital in the Khomas region is the national referral hospital. In addition, Namibia has four intermediate hospitals, namely, Katutura, Rundu, Oshakati and Onandjokwe hospitals. A total of 97 Intensive Care Unit beds were provided in Namibia before the COVID-19 pandemic [9]. 76% of Namibians live within 10km of health facilities. The Khomas and Erongo regions have the highest number of health facilities [10]. With the Namibian population of about three million, 60% of the population density is concentrated in the northern regions, specifically, Ohangwena, Omusati, Oshana and Oshikoto [11].
Study population
This study captured all 4,975 documented health workers with laboratory confirmation of SARS-CoV-2 who had a Polymerase Chain Reaction (PCR) test through nasopharyngeal or oropharyngeal swabs in n the national COVID-19-line list out of a total of 178,965 COVID-19 positive entries. All health workers in Namibia who were captured in the national COVID-19-line list between 2020 and 2023, with confirmed SARS-CoV-2 infection verified by either PCR, were included. Health workers in Namibia who were not captured in the national COVID-19-line list between 2020 and 2023, or without confirmed SARS-CoV-2 infection verified by PCR, were excluded.
Operational definitions
A case was defined as any health worker in the Namibia health system with laboratory-confirmed SARS-CoV-2 infection from January 2020 to December 2023. The uptake of the COVID-19 vaccine was defined as any confirmed SARS COV-2 cases who received at least one dose of the COVID-19 vaccine [6]. A health worker was defined as a professional primarily engaged in improving health by providing preventative, curative, promotional or rehabilitative healthcare services; a paid or unpaid person [7].
Data management
Positive cases were recorded in COVID-19 case investigation forms and transferred into a national COVID-19-line list in Microsoft Excel, which served as the source of information. The variables which were captured in the line list included date of reporting, sex, age, occupation, region, district, health worker status, comorbidities, signs and symptoms, vaccination status, name of vaccine, number of vaccine doses received, travel history, hospital admission status, health facility type, test type, specimen type, laboratory results, patient status outcome and epidemiological week. Single imputation was performed for missing data.
Data collection and analysis
Data was extracted from the National COVID-19-line list in Microsoft Excel. All entries identified as health workers were selected for analysis. Variables relevant to the study objectives, such as demographic, clinical, and vaccination-related factors, were extracted. The dataset was cleaned and analysed using Statistical Package for the Social Sciences (SPSS) version 25. Descriptive statistics were summarised using frequencies and proportions. The level of COVID-19 vaccine uptake was assessed. Associations between independent variables and binary outcomes were assessed using Generalised Estimating Equations (GEE) with a logit link and binomial distribution to account for both clustering within regions and correlation arising from repeated measurements among the same individuals. Variables of clinical importance and possible confounders were included in the multivariable model. Associations were assessed by calculating odds ratios (ORs, and statistical significance was determined at a 95% confidence interval (CI).
Ethical considerations
The study protocol was approved by the Ministry of Health and Social Services (MoHSS) Research Ethics Committee. An authorisation to conduct the study was issued by the Executive Director of MoHSS and sent to the Epidemiology division at the national level. All records were de-identified to protect the confidentiality of the information collected, and the anonymity of all health workers were respected and protected.
Socio-demographic and clinical characteristics of COVID-19 infections among health workers
Out of 4,975 cases analysed, 3595(72.3%) were female. The mean age of the cases was 37±11 years. The age group 25-34 years was the highest with 2157 (43.4%), followed by the age group of 35-44 years with 1222 (24.6%). Nurses had 1906 (38.3%) infections. Other cardiovascular diseases and diabetes topped the list of comorbidities recorded among the health workers, with 311(6.3%) and 90 (1.8%), respectively (Table 1).
Vaccination uptake and status of COVID-19 infections and deaths among health workers in Namibia
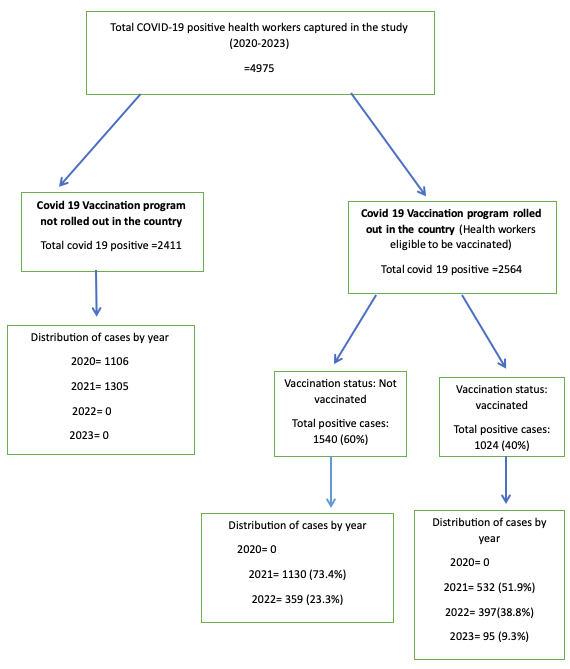
A total of 2,564 health workers were eligible for vaccination. Among these, 1024 (40%) received the COVID-19 vaccine, whereas 1540 (60%) remained unvaccinated. A total of 20 COVID-19-infected health workers died, out of which 12 (60%) were not vaccinated because the vaccination program had not yet been rolled out, seven (35%) were eligible but were not vaccinated, and one (5%) was vaccinated. So out of 20 deaths, 19 (95%) were unvaccinated. Among the vaccines available in Namibia, Johnson & Johnson had the highest uptake and dose completion of 98.3%, followed by Sinopharm (82.7%) (Table 4). Of the 1024 health workers who took the vaccine, the majority 532 (51.9%), got the vaccine in 2021, and a decrease in vaccination was observed over the years, with the least vaccinations being observed in 2023, with 95 (9.3%) (Figure 1).
Factors associated with COVID-19 vaccine uptake among health workers in Namibia, 2020-2023
A total of 2,564 health workers were eligible for vaccination; however, only 1,024 healthcare workers were vaccinated. Variables of clinical importance and possible confounders were included in the multivariable model. Multivariable GEE logistic regression showed that the age group 15–24 years (OR = 0.56, 95% CI: 0.37–0.85, p =0.006), compared to the age group of 55+, was statistically less likely to be vaccinated against COVID-19. Medical doctors (OR = 1.71, 95% CI: 1.02–2.87, p = 0.041), compared to Pharmacy personnel, had a positive association with vaccine uptake, indicating higher odds of being vaccinated because the odds ratio was more than one. Furthermore, comorbidity was a strong predictor for vaccine uptake among health workers, as health workers with one comorbidity (OR=1.72, 95%CI: 1.16-2.55, p-value 0.007) and those with two to three comorbidities (OR=1.69, 95%CI: 1.17-2.45, p-value 0.005) had higher odds of vaccination compared to those with zero comorbidities (Table 5). The highest case- fatality rates were observed in Khomas, Erongo, and the Northern regions, namely, Oshana, Oshikoto and Omusati regions, all with a case-fatality rate greater than 0.40 (Table 6).
In this study, female health workers had more than half of the infections. This could be attributed to women dominating certain healthcare cadres such as nursing and caregiving roles[12]. Our findings are similar to a study done in Iran, which found most infections in female healthcare workers [13]. Similarly, a national surveillance study done in the United States found 79% of the infections were in females [14]. These findings are, however, different from a cross-sectional study done in India, which indicated higher covid infections in males compared to females [15]. Our study findings suggest a gander -sensitive occupational health policy is needed in Namibia. In addition, we need to strengthen infection prevention and control measures. Training and regular screening are to be provided to reduce exposure among female health workers.
The uptake of the COVID-19 vaccine among health workers in Namibia was 40%, which was lower than the 100% global vaccine uptake recommended by WHO [15]. The low uptake of COVID-19 vaccines by health workers might have been contributed to by safety concerns and fear of side effects [4]. Other factors that could have contributed to the low uptake could be the use of traditional medicine. Other reasons could include inconsistent supply of vaccines, namely AstraZeneca, Pfizer, and Johnson & Johnson [4]. Low COVID-19 vaccine uptake poses a risk of high hospitalisation and increased preventable deaths. However, our findings differ from those of studies conducted in other parts of the world. A study done among healthcare workers in Entebbe municipality in Uganda showed a higher uptake of the COVID-19 vaccine (65.6%) than our findings. The study indicated that the high uptake might have been attributed to the fear of healthcare workers contracting the omicron strain, which was observed during that period of the study in the area [16]. Furthermore, findings in a worldwide systematic review contradict our findings since their results showed a high uptake of about 77.3 % of the vaccine by health workers [17]. Policies that encourage continuous education on vaccine benefits should be put in place to enhance vaccine confidence among health workers. Furthermore, the Ministry of Health and Social Services should strengthen risk communication strategies to address misinformation and fears of vaccine safety.
Health workers having one, and those with two to three comorbidities had high odds of receiving COVID-19 vaccination. This is similar to findings from a study done in Bangladesh where the odds of vaccination uptake were higher in people with one and those with more than one comorbidity [18]. However, our findings are inconsistent with results of a study conducted in Zimbabwe where having no comorbidities had high odds of being vaccinated compared to those who had one and more comorbidities [19].
The high vaccine uptake among health workers with one and more than one comorbidity in Namibia could be attributed to the vaccination campaign implemented in Namibia which followed the WHO SAGE Road map, whereby those with comorbidities were prioritised to receive the COVID-19 vaccine although it was voluntary [4]. The high uptake could also be attributed to the complete strategy implemented during the study period by the Ministry of Health and Social Services (MoHSS) and the Ministry of Information, Communication and Technology (MICT) with support from UN agencies to improve vaccine uptake [4]. High COVID-19 vaccination uptakes among health workers with one or more than one comorbidity is essential as this will enhance protection and improve the quality of life of healthcare workers.
Limitations
This study is limited by potential selection bias, as only health workers with laboratory-confirmed SARS-CoV-2 infection from the COVID-19 national line list were included. Findings may not be generalizable to all health workers, and unmeasured factors such as personal beliefs could have influenced vaccine uptake. To address these gaps, future studies should incorporate qualitative approaches to explore attitudes and barriers hence improve on reliability and applicability of findings.
This study found that less than half of eligible health workers with laboratory confirmed SARS-CoV-2 infection in Namibia were vaccinated against COVID-19 between 2021and 2023, which is below WHO’s recommended coverage. Presence of comorbidity was a strong predictor for vaccine uptake among health workers. These findings highlight the need for targeted approaches such as making vaccination programs accessible and convenient in the workplace and correcting vaccine myths among health workers, to improve vaccine acceptance, strengthen pandemic response and reduce preventable deaths.
What is already known about the topic
What this study adds
The authors of this work declare no competing interests.
Data availability
The dataset upon which the findings are based belongs to the Ministry of Health and Social Services of Namibia under the Epidemiology sub-division. The dataset is publicly available upon request from the corresponding author and with permission from the Ministry of Health and Social Services.
The authors would like to extend their gratitude to the Ministry of Health and Social Services (MoHSS) Research Ethics Committee for allowing them to access the dataset. To the University of Namibia and the Epidemiology Sub-division at National Level for their unwavering support, Moreover, the authors would like to thank all who have put effort in supporting this work.
| Table 1: Social demographic and clinical characteristics of COVID-19 infections among health workers in Namibia, 2020-2023 | ||
|---|---|---|
| Variables | Frequency (N=4975) | Percentage (%) |
| Sex | ||
| Female | 3595 | 72.3 |
| Male | 1380 | 27.7 |
| Age (Years) | ||
| 15-24 | 386 | 7.7 |
| 25-34 | 2157 | 43.4 |
| 35-44 | 1222 | 24.6 |
| 45-55 | 792 | 15.9 |
| 55+ | 418 | 8.4 |
| Occupation | ||
| Others+ | 2055 | 41.3 |
| Nurse | 1906 | 38.3 |
| Medical doctor | 645 | 13.0 |
| Pharmacy personnel | 194 | 3.9 |
| Environmental Health practitioner | 63 | 1.3 |
| Emergency care practitioner (Paramedics) | 61 | 1.2 |
| Laboratory personnel | 51 | 1.0 |
| Table 2: Comorbidities among COVID-19 health workers in Namibia 2020-2023 | ||
|---|---|---|
| Comorbidities (N= 4975) | Present (%) | Absent (%) |
| Other Cardiovascular diseases | 311 (6.3) | 4664 (93.7) |
| Diabetes | 90 (1.8) | 4885 (98.2) |
| Chronic lung disease | 64 (1.7) | 4911 (98.7) |
| HIV | 60 (1.2) | 4915 (98.8) |
| Asthma | 56 (1.1) | 4919 (98.9) |
| Hypertension | 55 (1.1) | 4920 (98.9) |
| Renal disease | 6 (0.1) | 4969 (99.9) |
| Chronic neurological disease | 7 (0.1) | 4968 (99.9) |
| Malignancy | 5 (0.1) | 4970 (99.9) |
| TB | 4 (0.1) | 4971 (99.9) |
| Obesity | 23 (0.5) | 4952 (99.5) |
| Liver Disease | 8 (0.2) | 4967 (99.8) |
| Table 3: Vaccination status of COVID-19 infections and deaths among health workers in Namibia, 2020-2023 | ||
|---|---|---|
| Vaccine status | Frequency (N=4975) | Percentage (%) |
| Vaccinated | 1024 | 20.5 |
| Unvaccinated | 1540 | 31.0 |
| N/A | 2411 | 48.5 |
| Deaths by vaccination status | Frequency (N= 20) | Percentage (%) |
| Vaccinated | 1 | 5.0 |
| Unvaccinated | 7 | 35.0 |
| N/A | 12 | 60.0 |
| N/A: Health workers who were not vaccinated because the vaccination program was not yet rolled out in the country | ||
| Table 4: Different types of COVID-19 vaccines received by health workers in Namibia, 2020-2023 | ||||||||
|---|---|---|---|---|---|---|---|---|
| Name of vaccine | One Dose | Two Doses | Three Doses | Four Doses | Not Indicate | Total | Required Dose | Completed course % |
| Sinopharm | 68 | 390 | 33 | 0 | 63 | 554 | 2+Booster | 82.7 |
| AstraZeneca | 52 | 152 | 29 | 0 | 30 | 263 | 2+Booster | 77.6 |
| Johnson&Johnson | 116 | 4 | 1 | 0 | 1 | 122 | 1+Booster | 98.3 |
| Pfizer | 6 | 26 | 11 | 1 | 0 | 44 | 2+Booster | 72.7 |
| Abdala | 0 | 0 | 2 | 1 | 0 | 3 | 3+Booster | 100 |
| Moderna | 0 | 2 | 0 | 0 | 0 | 2 | 2+Booster | 100 |
| Sputnik | 0 | 1 | 0 | 0 | 1 | 2 | 2+Booster | 50 |
| Not Indicated | 6 | 13 | 8 | – | 7 | 34 | – | – |
| Total | 248 | 588 | 84 | 2 | 102 | 1024 | – | – |
| Table 5: Unadjusted and adjusted Generalized Estimating Equation analysis of factors associated with COVID-19 vaccine uptake among health workers in Namibia, 2020-2023 | ||||||
|---|---|---|---|---|---|---|
| Variables | Vaccination status | Crude odds Ratio (95% CI) | p-value | Adjusted Odds Ratio (95% CI) | p-value | |
| Yes N=1024(%) | No N=1540(%) | |||||
| Gender | ||||||
| Female | 709(69.2) | 1132(73.5) | 0.81 (0.68-0.96) | 0.015 | 0.89 (0.74 -1.07) | 0.214 |
| Male | 315(30.8) | 408(26.5) | Reference | |||
| Age (years) | ||||||
| 15-24 | 47(4.5) | 150(9.7) | 0.44 (0.30 -0.66) | < 0.001 | 0.56 (0.37 -0.85) | 0.006* |
| 25-34 | 439(42.9) | 680(44.2) | 0.91 (0.69 -1.20) | 0.503 | 0.95 (0.71-1.27) | 0.736 |
| 35-44 | 272(26.6) | 373(24.2) | 1.03 (0.76 -1.39) | 0.846 | 1.08 (0.79-1.48) | 0.621 |
| 45-55 | 179(17.5) | 214(13.9) | 1.18 (0.84 -1.67) | 0.336 | 1.08 (0.79 -1.67) | 0.431 |
| 55+ | 87(8.4) | 123(8.0) | Reference | |||
| Occupation | ||||||
| Nurses | 344(33.6) | 597(38.8) | 0.95 (0.61 -1.48) | 0.816 | 0.92 (0.58-1.45) | 0.714 |
| Medical doctor | 184(18.0) | 163(10.6) | 1.86 (1.14 -3.03) | 0.013 | 1.71(1.02-2.87) | 0.041 |
| Others | 429(41.9) | 673(43.7) | 1.05 (0.72 -1.55) | 0.790 | 1.02 (0.69-1.51) | 0.929 |
| Environmental Health practitioners | 12(1.2) | 20(1.3) | 0.99 (0.44 -2.19) | 0.975 | 0.96 (0.43-2.16) | 0.923 |
| Emergency care practitioners (Paramedics) | 14(1.4) | 15(1.0) | 1.54 (0.69 -3.41) | 0.289 | 1.42 (0.63-3.18) | 0.394 |
| Laboratory personnel | 10(0.9) | 21(1.3) | 0.78 (0.35 -1.74) | 0.546 | 0.81 (0.36- 1.82) | 0.607 |
| Pharmacy personnel | 31(3.0) | 51(3.3) | Reference | |||
| Number of Comorbidities | ||||||
| Zero Comorbidities | 880(85.9) | 1418(91.1) | Reference | |||
| One Comorbidity | 66(6.4) | 54(3.5) | 1.97 (1.35 -2.87) | < 0.001 | 1.72 (1.16-2.55) | 0.007* |
| Two – Three Comorbidities | 76(7.4) | 63(4.1) | 1.94 (1.36 -2.77) | < 0.001 | 1.69 (1.17-2.45) | 0.005* |
| > three Comorbidities | 2(0.2) | 5(0.3) | 0.64(0.12 -3.31) | 0.593 | 0.58 (0.11-3.06) | 0.521 |
| Table 6: Regional health facility distribution of COVID-19 case fatality rate among health workers in Namibia, 2020-2023 | |||
|---|---|---|---|
| Region | Cases | Deaths | CFR (%) |
| Erongo | 480 | 2 | 0.42 |
| Hardap | 211 | 0 | 0 |
| Karas | 258 | 1 | 0.39 |
| Kavango East | 268 | 1 | 0.37 |
| Kavango West | 53 | 0 | 0 |
| Khomas | 1686 | 8 | 0.47 |
| Kunene | 153 | 0 | 0 |
| Ohangwena | 228 | 0 | 0 |
| Omaheke | 81 | 0 | 0 |
| Omusati | 288 | 2 | 0.69 |
| Oshana | 578 | 3 | 0.52 |
| Oshikoto | 299 | 2 | 0.67 |
| Otjozondjupa | 309 | 1 | 0.32 |
| Zambezi | 83 | 0 | 0 |
| Total | 4975 | 20 | 0.40 |