Research | Open Access | Volume 9 (2): Article 74 | Published: 05 May 2026

Views: 1,142
Menu, Tables and Figures

Clara Oguji1,&, Ugochukwu Osigwe1, Adam Attahiru1, Mariam Ogo1, Lawal Sani Muhammad1, Amal Oladimeji1, Adefisoye Adewole1, Aliyu Nurudeen1, David Nyampa Barau1, Gabriel Adah2, Alex Ash3, Yusuf Yusufari4, Masduk Abdukarim4, Ndadilnasiya Endie Waziri1, Patrick Nguku1
1African Field Epidemiology Network, Abuja Country Office, Nigeria, 2National Primary Health Care Development Agency, Abuja, Nigeria, 3M & C Saatchi Group, London, United Kingdom, 4Bill and Melinda Gates Foundation, Abuja Country Office, Nigeria
&Corresponding author: Clara Oguji, African Field Epidemiology Network, Abuja Country Office, Nigeria, Email: claraoguji@gmail.com ORCID: https://orcid.org/0000-0003-2679-2766
Received: 22 Nov 2025, Accepted: 29 Apr 2026, Published: 05 May 2026
Domain: Health Informatics
Keywords: Primary Health Care, Data quality, Timely, Responsive Feedback Mechanism, behaviour change, Timely recording, falsification of data
©Clara Oguji et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Clara Oguji et al. Assessing healthcare workers’ perspectives on prompt use for timely routine data documentation in primary healthcare: A responsive feedback approach in Northern Nigeria, 2022. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):74. https://doi.org/10.37432/jieph-d-25-00298
Introduction: Poor data quality from health facilities in Nigeria remains a significant barrier to effective decision-making. One identified contributor is the delay in documenting data at the point of service. To address this, National Youth Service Corps (NYSC) members were trained and deployed as “prompts” to encourage primary health care workers (HCWs) to record data promptly. This study assessed the perceived effect of this approach and gathered HCW feedback to refine the strategy.
Methods: A descriptive observational implementation study design was conducted in Sokoto State from July 2021 to October 2022. Community informants were trained as data collectors through stakeholder engagement as data collectors through stakeholder engagement. Data were collected at multiple time points during the implementation period to assess changes in reporting timeliness and healthcare workers’ experiences with the intervention. Using a semi-structured questionnaire built on Open Data Kit (ODK), data were collected on the activities, usefulness, and adequacy of the NYSC prompts, as well as HCWs’ recommendations. Descriptive statistics and trend analysis were performed using Microsoft Excel.
Results: All facilities (100%) received at least one visit from a prompt. NYSC members facilitated timely data recording in 44% of sessions and after sessions in 22%. Additionally, 56% of HCWs noted that prompts reminded them to check for data entry errors, improving data quality. Nearly all HCWs (99%) expressed satisfaction with the visits and recommended increasing visit frequency to at least twice weekly.
Conclusion: NYSC members served as good behavioural prompts, and increased both the timeliness and quality of data documentation. HCW satisfaction and recommendations highlight the value of this strategy for routine data strengthening in primary health care settings.
Strengthening Health Information Systems (HIS) is not a one-time effort but requires continuous cycles of data collection, collation, quality assessment, analysis, and use. It also involves building, strengthening, and renewing capacity at all levels within countries [1]. The Nigeria National Health Management Information System (NHMIS) is designed to capture health facility data, first through facility-based data tools and then onto the online electronic database, the District Health Information System (DHIS2). This system is primarily used to measure the efficiency of health service delivery and assist policymakers at all levels in short, medium-, and long-term advocacy, planning, and decision-making for health interventions. Despite major technological advancements in recent years, the system remains largely paper-based at the primary healthcare facility level, and health workers balance data compilation responsibilities with service provision duties. Data from health facilities are transferred to district/Local Government Area (LGA) health offices, where they are digitized, aggregated, and made accessible to state and national officers [1].
However, data quality remains a long-standing challenge for both the government and its partners, significantly impacting effective and transformative decision-making (Nigeria Routine Immunization Data Quality Improvement Plan (DQIP), 2019–2023 Internal Document). Evidence indicates that routine health information is used minimally for decision-making at all administrative levels in Nigeria, primarily due to poor data quality [2]. This has led to a lack of trust in the reliability of data [3]. Healthcare workers (HCWs) frequently report low data utilization for planning, despite their involvement in data collection, aggregation, and reporting [4]. This could affect the uptake of immunization services and Awareness of adverse events following immunization (AEFI) with varied management practices for adverse events following immunization [5].
Additionally, research suggests that motivation and the attitude of HCWs contribute to poor data quality within the primary healthcare system [6]. Despite the negative implications of poor-quality data on evidence-based decision-making in healthcare, there is limited research on interventions aimed at improving routine primary healthcare data quality in Nigeria. This paper assessed the perceived effects of human prompts in enhancing timely data recording and ensuring that feedback from HCWs is instrumental in refining data collection approaches.
Program description
Behavioural drivers of data quality
Data quality could be affected by the behavioural factors of those collecting the data, including their attitudes, values, and motivation. The completeness, accuracy, and consistency of administrative data generated at the point of entry (health facilities) and across all levels of the health system are influenced by social and behavioural factors [6]. Several studies have linked the “culture” of poor data, characterized by inadequate data collection practices, reporting, and use in low-income countries, to the attitudes and behaviours of healthcare workers, as well as weak accountability measures for enforcing data quality. Motivation, or the lack thereof, has been identified as a key determinant of healthcare workers’ performance at the point of data entry and remains a major factor in ensuring good data quality.
Intervention framework based on Fogg Behaviour Model
Healthcare workers play a critical role in the Health Information System (HMIS) functioning at the point of entry, and broader issues affecting staff performance and efficiency within health systems inevitably influence information systems. For example, HCWs’ perceptions of the rationale and motivations for data collection have been found to directly impact the accuracy of data recording and reporting practices [7,8]. Interventions aimed at addressing data quality gaps, such as electronic reporting platforms, short message service (SMS) reminders, data quality assessments, and health worker training in data management, have not yielded the desired results.
To enhance data quality, we implemented a non-traditional approach to modifying HCW behaviours while leveraging ongoing technical strategies (e.g., review meetings and quarterly data quality assessments). The Fogg Behaviour Model was adopted to strengthen motivation (e.g., progress recognition and acknowledgement of good data quality), ability (e.g., capacity-building in data management), and prompts (e.g., the physical presence of NYSC Corps members serving as a cue for timely data recording). However, this responsive feedback mechanism focused primarily on the prompt aspect of the intervention.
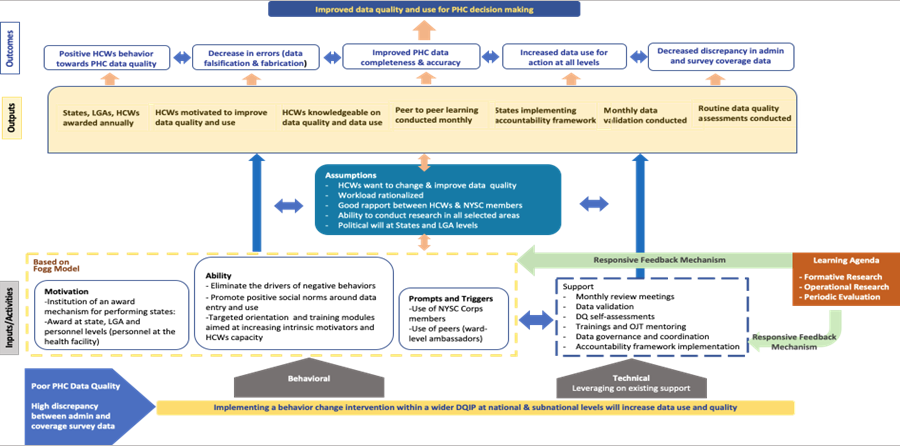
The goal of the project was to enhance the quality and acceptability of primary healthcare data to support effective programmatic decision-making through both behavioural and technical approaches. The Theory of Change (ToC) for the program is based on the premise that addressing the behavioural, technical, and organizational factors contributing to poor data quality using human-centred design (HCD) methods will lead to improved data quality and its utilization in public health decision-making. The ToC (Figure 1) illustrates how the proposed activities will generate specific outputs and outcomes, ultimately guiding us towards achieving the project’s main objective. Below is a schematic representation of the intervention’s ToC, which also includes assumptions regarding how these components interact with both behavioural and technical aspects of the intervention.
Study design
To improve routine data documentation, National Youth Service Corps (NYSC) Members were trained and deployed to healthcare facilities to serve as prompts (reminders) for healthcare workers (HCWs) to record data promptly. To understand the perceived effect of these NYSC members, we conducted a descriptive observational implementation design study to gather insights from HCWs in Sokoto State, Nigeria, regarding the effectiveness and usefulness of these prompts in increasing timely data recording.
Sampling strategy and selection
Two local government areas (LGAs) in Sokoto State were selected using a criterion-based selection approach to represent different levels of routine reporting performance (one “high-performing” and one “low-performing”). Classification was based on DHIS2 data downloaded for Quarter 1 (Q1) 2020 (pre-implementation), using selected indicators/data elements, including reporting rate, general attendance, outpatient attendance, deliveries, and skilled birth attendance, as well as the frequency of DHIS2 validation-rule errors applied to these elements. The LGA with a higher frequency of validation-rule errors was categorized as low-performing, whereas the LGA with fewer errors was categorized as high-performing. All health facilities in the two selected LGAs were included (facility census of the selected LGAs).
Community informants
Twenty-four community informants (12 per LGA) were selected from the existing pool of government-trained surveillance community informants residing in the selected LGAs; all were familiar with local facilities and health workers, and conducted facility visits to administer the study tool.
Study instrument
Data were collected using an Open Data Kit (ODK) checklist administered by trained community informants before interviews commenced. The ODK tool was structured into modules capturing whether the NYSC prompt visit occurred and the activities performed during the visit (checklist items), healthcare workers’ perceptions of usefulness of the prompts, perceived adequacy of prompt visits (e.g., frequency/coverage), and HCWs’ recommendations for improving the prompt approach (including open-text responses where applicable). Data were collected from healthcare workers on their perception of the use of NYSC members as reminders for timely data recording. Questions were categorized by theme: occurrence, relationship between healthcare workers and NYSC members, effectiveness, usefulness, and satisfaction.
Study design and analytic approach
Data were collected during repeated facility visits over the implementation period. At each visit, community informants interviewed the facility staff responsible for routine data documentation and reporting (e.g., the RI/data focal person or officer-in-charge, as applicable), rather than interviewing any available healthcare worker. Because the same eligible staff member was not necessarily available on every visit, respondents could differ across timepoints; therefore, the analytic dataset represents repeated cross-sectional observations. We summarize responses by time point using descriptive statistics and assess trends across the study period.
Study timeline
Baseline routine reporting performance was assessed using DHIS2 data from January–March 2020 (Q1 2020) to select one high-performing and one low-performing LGA based on DHIS2 validation-rule errors and selected reporting indicators. The NYSC prompt intervention began in July 2021. Data for this analysis were collected from July 2021 to October 2022 during repeated facility visits in which community informants interviewed eligible healthcare workers responsible for routine data documentation. Although implementation continued through 2023, analyses are limited to observations collected between July 2021 and October 2022.
Outcome definitions
Timeliness of routine reporting was defined using the WHO Data Quality Review (DQR) metric as the proportion of reports submitted by the reporting deadline, calculated as the number of reports submitted on time divided by the number of reports received for the specified reporting period. Data quality was assessed using DHIS2 validation rules applied to selected routine data elements (reporting rate, general attendance, outpatient attendance, deliveries, and skilled birth attendance); data quality errors were defined as validation-rule violations, summarized as the frequency of validation-rule errors within the DHIS2 dataset for the specified period
Description of the responsive feedback mechanism
Before designing our evidence-gathering process, we utilized the CURVE process for Responsive Feedback [9] (Figure 2). This involved identifying key stakeholders and beneficiaries, conducting formative research to understand the underlying causes of poor data quality, and developing a project-specific Theory of Change. This Theory of Change helped us uncover assumptions and formulate learning questions, leading us to identify relevant data sources for answering those questions. Responsive feedback mechanisms (RFMs) are tools designed to facilitate continuous learning by collecting timely data that can provide feedback to planners and implementers during an ongoing intervention. This allows for real-time adjustments to improve the intervention’s effectiveness while it is still in progress. RFMs build on previous work in social and behavioural sciences that have proposed various frameworks for optimizing implementation, as well as management literature that integrates implementation sciences with improvement sciences [10-13]. The following section details the CURVE process and maps out how the process was applied to this specific RFM.
Ethical consideration
This activity was conducted as a public health program operational implementation and was reviewed and technically supported by the Federal Ministry of Health (FMOH) and the National Primary Health Care Development Agency (NPHCDA). Healthcare worker participation was voluntary; informed consent was obtained using a consent script embedded in the Open Data Kit (ODK) tool. Facility level operational data were used in aggregate form without personal identifiers, and responses were handled confidentially
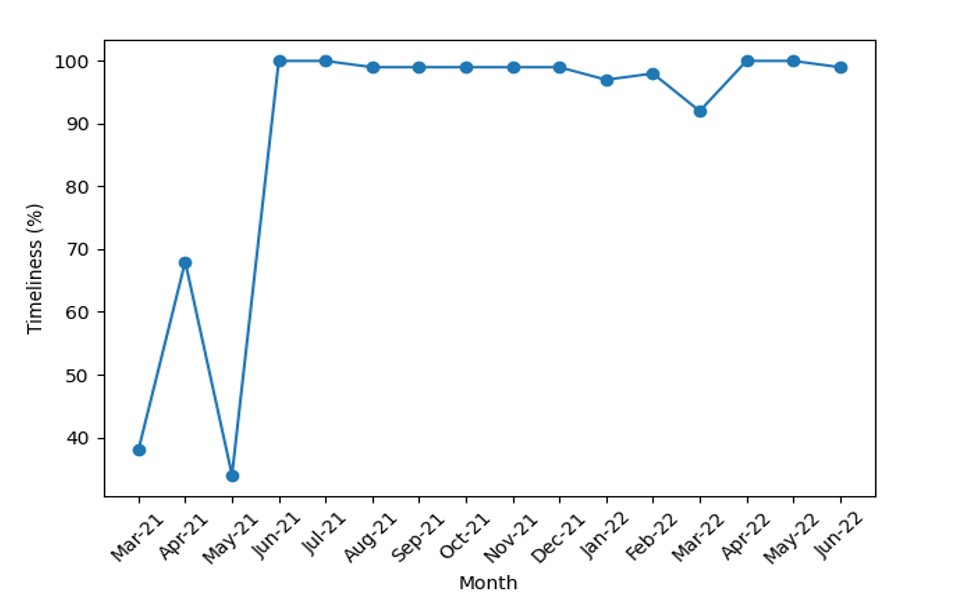
Overall, there was an increase in the timeliness of data for the selected LGAs in Sokoto State (Figure 3). Timeliness increased from 38% in March 2021 to 99% in September 2022. A total of 461 responses were received from July 2021 to October 2022, of which 97% (449) agreed and gave their consent to participate in the interview. The community informants are from the communities where the health facilities are located; therefore, the expectation is that there is an existing level of trust between the healthcare workers and these community informants. Hence, we were surprised to see that 4% – 11 % HCWs declined to be interviewed by the community informants between September 2021 and April 2022. However, the decrease from 0% from May 2022 to October 2022 shows acquired trust.
Occurrence
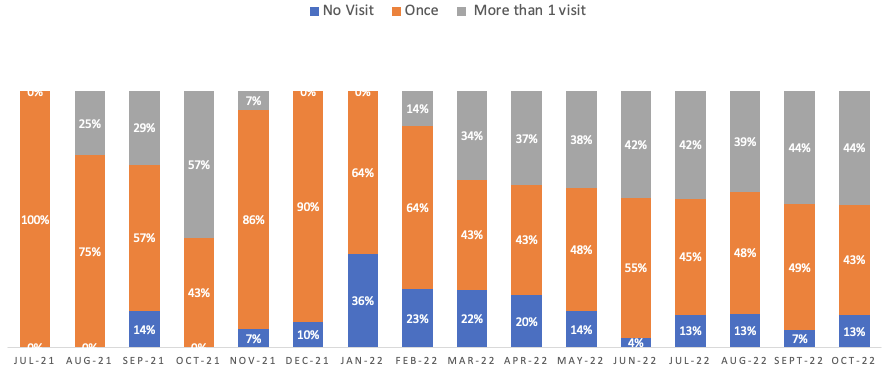
The original plan for project implementation was for the NYSC corps members to visit health facilities in their assigned wards once a week (Figure 4). Feedback was collected from the healthcare workers on whether the NYSC members visited, the number of visits received from NYSC members, and what the members do when they visit. Data collected showed that NYSC Corp members initially visited once a month, but the frequency of visits increased steadily from March 2022. This was due to the feedback from healthcare workers who said they wanted the NYSC members to visit more often than just once a week. Data showed that there were no visits from NYSC members in some months; January 2022 had the highest proportion of “No visit” due to the holiday during which NYSC members go back to their home states. In addition to the regular actions taken from the healthcare workers’ feedback, we also recommended that the State primary health care board collaborate with the NYSC state secretariat for NYSC members to be posted directly to PHC for their place of primary assignment, which will enable them to be more present in health facilities and act as daily prompts to healthcare workers. One important feedback from healthcare workers was that the frequency of the visit should be increased due to the positive impact of the presence of the NYSCs as prompts. The frequency of visits to health facilities has increased with fewer facilities per Corp member.
“To give them more time for visiting our health facilities, because it is very important to us”. Selected Facility Healthcare Worker
Relationship between healthcare workers and NYSC members
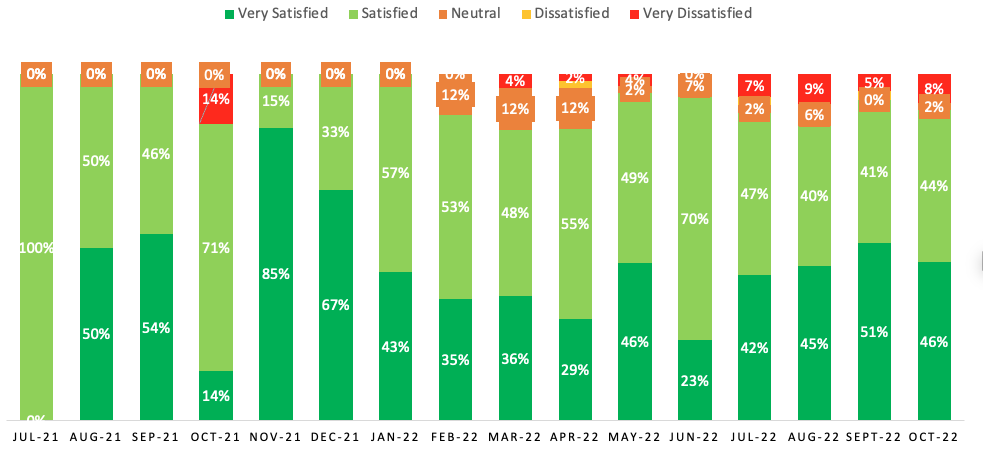
The study aimed to assess the nature of engagement between NYSC members and healthcare workers, focusing on appropriateness, respectfulness, and satisfaction levels among HCWs regarding these interactions. Across the months, an average of 41.6% of HCWs were very satisfied with their interactions, while 51.2% were satisfied (Figure 5). Overall, the results indicate a positive perception among HCWs regarding their engagement with NYSC members while also identifying areas for improvement. During the interviews, if the HCW says they are satisfied with the NYSC, a follow-up probe is asked to understand why they are satisfied. Reasons for their satisfaction include:
“They help me recognize errors in my registers, such as missing data and calculation mistakes. They always remind me to use the appropriate registers in recording and use my defaulters’ registers/tickler boxes to track children who missed their vaccination.” Health Care Worker, Selected Facility Healthcare Worker
Health care workers’ perspective on the usefulness of NYSC members
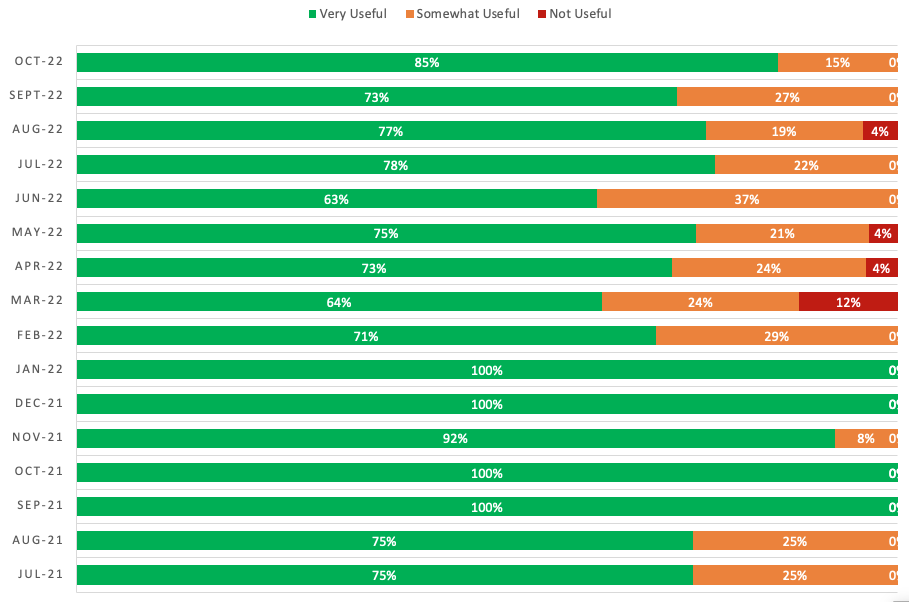
The community informants also collected information on how useful the NYSC members are for improving data quality. Across the months, an average of 81.3% HCWs reported that the NYSC members are useful. However, the month with the lowest score (64.0%) for usefulness was March 2022, which coincided with a decline in the deployment of NYSC members due to an ongoing strike (Figure 6). Healthcare workers said they were reminded of data recording and reporting during service delivery. HCWs mentioned that the presence of the NYSC Members reminded them to record data in a timely and accurate way, and recommended that the NYSC members visit every health facility.
Those who expressed dissatisfaction were further interviewed, and the reasons mentioned included that NYSC members did not provide assistance with health facility tasks or that they expected them to carry out healthcare worker responsibilities, which was not the goal of the project. These concerns were addressed by implementing communication and awareness strategies to help healthcare workers understand the project design and the purpose of having NYSC members in their facilities.
Some quotes from the interviews include: “Is better for you to get some that can work and help us out in our work”, “My only advice here is that you assign someone who will be with the health post”. HCW
For those satisfied, reasons included NYSC members serving as motivation for the hard work they are doing,
“They help me recognize errors in my registers, such as missing data and calculation mistakes”, HCW
“They always remind me to use the appropriate registers in recording and use my defaulters’ registers/tickler boxes to track children who missed their vaccination”. HCW
Strengthening the quality of routine primary health care data is essential, as quality health information is one of the six building blocks of a health information system. Improving health quality depends on the timely recording of data during service delivery. In this intervention, NYSC members were used to remind healthcare workers to enter their data on time and to review and correct any inaccuracies. The study focused on using RFM to assess healthcare workers’ perceived effect of NYSC members as prompts.
At the beginning of the project, stakeholders raised concerns about the acceptance of NYSC members by healthcare workers due to cultural differences, language barriers, and insecurity (insurgencies and community clashes) in some areas where health facilities are located. Based on interviews, community informants provided context-specific feedback that guided changes to the prompting approach. This feedback included gender inclusion (most healthcare workers preferred female NYSC members to visit their facilities compared to male members due to culturally accepted norms in northern Nigeria), frequency of visits (healthcare workers requested an increase in NYSC visits), clarification on roles and responsibilities (healthcare workers assumed that NYSC members were visiting health facilities as data collectors), respectfulness of NYSC members, and inclusion of private health facilities. Over time, 81.3% of healthcare workers interviewed reported that visits from NYSC members were very useful, 14% found them somewhat useful, and 2% said the visits were not useful.
However, private health facility staff exhibited poor acceptance of NYSC members; they viewed them as “spies” and often sent them away. This was attributed to inadequate communication between the LGA team and managing directors (MDs) of the private health facilities. Consequently, timely information was provided to MDs before posting NYSC members there. Due to the handover strategy involving NYSC members, we were interested in understanding the quality of relationships between healthcare workers and these prompts. We were pleased to find that most healthcare workers reported being either satisfied or very satisfied with their interactions.
A substantial increase in timeliness was observed during the implementation period, coinciding with the deployment of NYSC prompts. Timely data entry increased from 38% in March 2021 to 99% in September 2022, largely due to the feedback provided to healthcare workers (data generators). It also facilitated prompt adjustments and responses by the project team, in contrast to the traditional monitoring and evaluation (M&E) approach, which typically allows for updates or changes to project strategies only at specific intervals. This aligns with the findings of Randriamiarana et al., who argued that the presence of regular feedback facilitates positive outcomes in interventions [14]. Oxfam implemented responsive listening through improved feedback mechanisms, capitalizing on face-to-face feedback and utilizing information and communication technology (ICT) tools to foster a change in accountability culture in Iraq and Lebanon [15]. The study shows that responsive feedback mechanisms appear to be a good approach for correcting interventions when they are ongoing, in our case, improving data timeliness, accuracy, and quality.
Limitations
This study has several limitations. First, the absence of a comparison group limits the ability to attribute observed improvements solely to the NYSC prompt intervention. Second, the repeated cross-sectional design means that different respondents may have contributed data at different time points, introducing variability. Third, external factors such as supervision activities or parallel programs may have influenced reporting performance. Therefore, findings should be interpreted as operational associations rather than causal effects
The use of a responsive feedback mechanism at primary health care facilities in Sokoto State has provided programmatic tools for collecting data to improve intervention effectiveness. The ultimate result was to increase timeliness and data quality through the use of the feedback gathered via the RFM. Healthcare workers were critical in the process of the feedback mechanism flow. This study revealed novel findings in reducing variance in data documentation at the health facility level due to changes made to the intervention based on feedback from the RFM. The RFM has provided the opportunity to gather much-needed evidence, which will inform course correction while the project is still live, using what we have learned to make our programs better and helping us to arrive at distilled lessons and an action plan. We reviewed the feedback from HCWs and acted on it by increasing the number of visits by NYSC members. However, the importance of ensuring stakeholders continued buy-in cannot be underestimated and has likely increased the sustainability of the project in the longer term.
What is already known about the topic
What this study adds
Conceptualization: Clara Oguji, Ugochukwu Osigwe, Adam Attahiru, Mariam Ogo, Lawal Sani Muhammad, Amal Oladimeji.
Methodology: Clara Oguji, Ugochukwu Osigwe, Adam Attahiru, Mariam Ogo, Lawal Sani Muhammad, Amal Oladimeji.
Data collection and supervision: Clara Oguji, Ugochukwu Osigwe, Adam Attahiru, Mariam Ogo, Lawal Sani Muhammad, Amal Oladimeji, Aliyu Nurudeen, David Nyampa Barau, Gabriel Adah, Alex Ash.
Data analysis and interpretation: Clara Oguji, Ugochukwu Osigwe, Adam Attahiru, Mariam Ogo, Lawal Sani Muhammad
Manuscript drafting: Clara Oguji, Ugochukwu Osigwe.
Manuscript review and editing: All authors.