Research | Open Access | Volume 9 (2): Article 75 | Published: 11 May 2026

Views: 1,136
Menu, Tables and Figures
| Table 1: Distribution of key respondents, AHFS surveillance system Sawla Tuna Kalba District, 2024 | ||
|---|---|---|
| Key Informant | Frequency (%) | Percentage |
| Median years of service 6 (Range= 3–30)years | ||
| Disease Control Officers | 9 | 32.2 |
| Community Health Nurse | 6 | 21.4 |
| Community Based Surveillance Volunteer | 4 | 14.2 |
| Nurse (clinical) | 4 | 14.2 |
| District Director of Health Services | 1 | 3.6 |
| Health Promotion Officer | 1 | 3.6 |
| Medical Officer | 1 | 3.6 |
| Physician Assistant | 1 | 3.6 |
| Regional Surveillance Officer | 1 | 3.6 |
| Total | 28 | 100 |
Table 1: Distribution of key respondents, AHFS surveillance system Sawla Tuna Kalba District, 2024
| Table 2: Key findings from assessment of attributes of AHFS surveillance system in Sawla Tuna Kalba district, 2024 | |||||
|---|---|---|---|---|---|
| SYSTEM ATTRIBUTE | INDICATOR | How it was assessed | KEY FINDINGS | Assessment Score | Percentage |
| Simplicity | Respondent’s knowledge of the case definition and perception of how easy it is. | Ability of respondents to state the case definition for acute hemorrhagic fever syndromes and perception of ease of use of the case definition | The majority, 85 % (24/28), of the respondents knew the AHFS case definition, and a total of 87.5% (21/24) of them could state at least two signs and symptoms for a suspected case. Most, 83.3% (20/24), of the respondents who knew the case definition deemed it easy | 1 | 40% |
| The ease in filling case-based forms for AHFS | Time taken to fill case-based form | An average of 5 minutes is needed to fill the case-based form | 1 | ||
| Ease of reporting | Whether one reporting format existed for the same information or not. | Numerous reporting formats existed: weekly IDSR, Monthly IDSR, and SORMAS | 0 | ||
| Synchronization of various data reporting systems | Evidence of various reporting systems being synchronized. | The various reporting systems being used were not synchronized with each other | 0 | ||
| Proximity of testing laboratory to district | The closeness of the testing laboratory to the district, and whether samples can be transported within 2 hours | Samples need to be transported to an external Laboratory for confirmation, which takes about 12 hours. | 0 | ||
| Stability | Funding for surveillance activities | Evidence of funding commitments on surveillance by various stakeholders | The government supports through the payment of salaries. The central government bears the cost of sample testing. Also, the cost of surveillance trainings borne by donors and the government | 1 | 100% |
| Integration of acute haemorrhagic syndrome surveillance system with the IDSR system | Whether the surveillance system is being integrated with the broader IDSR* system | AHFS surveillance system is integrated with IDSR system | 1 | ||
| Availability of surveillance focal persons at each level | Evidence of availability of surveillance focal persons at community, facility, district, and regional levels | All levels of the surveillance system had focal persons All facilities visited had persons who acted as surveillance focal persons at those levels | 1 | ||
| Representativeness | Health facilities involved in surveillance | Number of health facilities reporting on weekly and monthly IDSR | All health facilities reporting on weekly and monthly IDSR. | 1 | 100% |
| Sub-districts suspecting and reporting cases including zero reporring | The number of sub-districts that are submitting surveillance reports on acute hemorrhagic fever syndromes | All eight (8) sub-districts were submitting weekly and monthly reports, including zero reporting | 1 | ||
| Distribution of cases by sex, age | Whether cases being suspected were fairly distributed by age and sex | Suspected cases consisted of both genders (4 females and 3 males) Median age is 8 years. Range = (10 months – 35 years) Cases consisted of both adults and children | 1 | ||
| Acceptability | Proportion of completed case-based forms available. | Whether case-based forms for all suspected cases were available for reference | All seven case-based forms for cases suspected within the evaluation period were available. | 1 | 60% |
| *CBSVs monthly report submissions 2023 | The number of CBSVs reports for the year 2023 that were available at the various sub-district levels. | Community-based surveillance reporting was not part of the DHIMS* dataset, though a reporting form was available for compilation of monthly reports. For the year 2023, only one (1/8) sub-district had complete CBSVs reports available | 0 | ||
| Outbreak investigation and contact tracing conducted for outbreaks | Availability of outbreak investigation reports and contact tracing reports for any outbreaks reported within the period | Outbreak investigation reports for an outbreak that occurred in 2022 were available. Contact tracing lists for 88 contacts were available (list captured contacts by person, place, and time characteristics). | 1 | ||
| SORMAS entries | Whether all suspected cases were entered into the SORMAS system | Entry of cases into SORMAS was not done. | 0 | ||
| Willingness by stakeholders to continue with AHFS surveillance | Whether all stakeholders were willing to continue working effectively in their role as surveillance persons at their various levels | All stakeholders interviewed expressed willingness to continue working efficiently on AHFS surveillance. | 1 | ||
| Flexibility | Ability to modify case definition to meet prevailing demands | Whether an outbreak case definition exists | The case definition can be modified during outbreaks. An outbreak case definition is used during outbreak situations to help capture more cases. | 1 | 100% |
| System integrated with the IDSR surveillance system | Whether the system is integrated with the IDSR system | System integrated with IDSR system | 1 | ||
| Changes in the mode of reporting to meet current surveillance updates | Evidence of new changes that have been implemented to improve the system without causing major distortions. | The SORMAS system was introduced in 2020, which served as a surveillance tool for real-time data reporting of surveillance data. | 1 | ||
| Sensitivity | Number of cases detected by the system | The sensitivity of the surveillance system was assessed at the level of case detection through retrospective review of routine surveillance data. Suspected cases were identified based on the established case definition captured in the reporting systems. | Seven (7) cases were suspected over the period of evaluation. | N/A | N/A |
| Positive Predictive Value | Proportion of cases that were positive for AHFS | Two cases were confirmed, giving a PPV of 29% (2/7) | N/A | N/A | |
| Timeliness | Average reporting timeliness for the past five years (2019-2023) | Whether the timeliness of reporting is more than 90% | The average timeliness of reporting for weekly IDSR was 91.1%. | 1 | 50% |
| Time between the onset of symptoms and case detection | Whether all confirmed cases were detected within 24 hours | The two confirmed cases were not promptly detected within 24 hours of symptom onset. These were detected 21 days and 5 days after date of onset, respectively | 0 | ||
| Time taken to receive sample feedback from testing laboratories | Whether feedback for all samples transported was received within 48 hours upon sample transportation. | Laboratory results from NMIMR were received within 48 hours for only 28.5% (2/7) of the samples transported for testing | 0 | ||
| Time taken to transport the sample to the testing laboratory | Whether samples collected were transported within 24 hours | All samples transported within 24 hours of collection | 1 | ||
| Data Quality | Availability of the linelist of cases at district and regional levels | Whether reported cases were line-listed | All cases suspected within the evaluation period were line listed, with copies of the linelist available at the district and regional levels | 1 | 67% |
| Completeness of variable fields in the linelist and case-based forms | The number of variable fields in the linelist and case-based forms that were completed | A proportion of 338/344 fields were completed in line-list, thus (98.2%) completeness. A total of 93% (163/175) of the fields were completed for all seven(7) case report forms available | 1 | ||
| Data variations across reporting sources | Whether the same number of cases was reported among the various reporting channels | Variations existed across sources; Linelist contained 7 suspected and 2 confirmed cases, The DHIMS system had 8 suspected and 1 confirmed case while there were zero entries in the SORMAS system | 0 | ||
| *IDSR – Integrated Disease Surveillance and Response *SORMAS – Surveillance Outbreak Response Management and Analysis System *CBSVs – Community-based Surveillance Volunteers *DHIMS – District Health Information Management System | |||||
Table 2: Key findings from assessment of attributes of AHFS surveillance system in Sawla Tuna Kalba district, 2024
Isaac Issah1,2, George Akowuah2,&, Mavis Osafo2, Cyril Kwami Azornu2,3, Alhassan Abukari1, Michael Biredu4, Thomas Nang Suuri4, Seth Owusu-Agyei5, Samuel Oko Sackey2, Ernest Kenu2
1Sawla Tuna Kalba District Health Directorate, Ghana Health Service, Savannah Region, Sawla, Ghana, 2Ghana Field Epidemiology and Laboratory training Program (GFELTP), School of Public Health, University of Ghana, Accra, Ghana, 3Salaga Municipal Hospital, Ghana Health Service, Savannah Region, Salaga, Ghana, 4Savannah Regional Health Directorate, Ghana Health Service, Damango, Ghana, 5Institute of Health Research, University of Health and Allied Sciences, Ho, Ghana
&Corresponding author: George Akowuah, Ghana Field Epidemiology and Laboratory Training Program (GFELTP), School of Public Health, University of Ghana, Accra, Ghana, Email: CirJorge@gmail.com ORCID: https://orcid.org/0000-0002-0519-5738
Received: 04 Nov 2025, Accepted: 04 May 2026, Published: 11 May 2026
Domain: Infectious Disease Epidemiology
Keywords: Viral hemorrhagic fever, surveillance system evaluation, attributes, Sawla Tuna Kalba District
©Isaac Issah et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Isaac Issah et al., Evaluation of acute hemorrhagic fever syndrome surveillance system in Sawla Tuna Kalba District, Ghana, 2024. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):75. https://doi.org/10.37432/jieph-d-25-00267
Introduction: In 2022, Ghana recorded an acute hemorrhagic fever syndrome (AHFS) outbreak of Marburg disease, with reported cases in the Sawla Tuna Kalba district. The study therefore evaluated the AHFS surveillance system in Sawla Tuna Kalba district to determine whether it met its objectives, evaluate the performance of system attributes, and assess its usefulness.
Methods: We conducted an evaluation of the AHFS surveillance system in Sawla Tuna Kalba District in 2024 for the period 2019-2023. The US-CDC Updated Guidelines for Evaluating Public Health Surveillance Systems was adapted for the evaluation. Semi-structured questionnaire, checklist and interview guides were used to collect data through observations, interviews and record reviews. Twenty-eight key stakeholders were interviewed. Attributes were scored based on key indicators classified into poor (<50%), moderate (50% – 70%) and good (>70%). Findings were presented in tables and text.
Results: Two Marburg cases, 29% (2/7), were confirmed over the period. Only 14.2% (1/7) of cases were detected within the recommended 24-hour interval. Outbreak investigation, including follow-up of 88 contacts, was done. About 85% (24/28) of respondents knew the case definition. Timeliness of weekly reports was 91.1%, and data completeness on case-based forms was 93% (163/175). Unintegrated multiple data reporting systems existed, causing data inconsistencies. Seven sub-districts did not report on community-based surveillance activities. Attribute scores were simplicity (40%), acceptability (60%), data quality (67%), timeliness (50%), flexibility (100%), stability (100%) and representativeness (100%). Data generated from the system was used for planning community health education and awareness programs and simulation trainings for staff.
Conclusion: The surveillance system was useful, partially met its objectives, but scored poorly on simplicity. Integration of the various reporting systems will help improve its operations.
The largest recorded global outbreak of acute hemorrhagic fever syndromes (AHFS), which is among the viral hemorrhagic fevers, occurred between 2014 and 2016 in six West African countries, resulting in 28,600 cases and 11,325 deaths [1] . Isolated cases were subsequently reported beyond Africa, with reported cases recorded in the United States, the United Kingdom and Italy, which led to a global public health emergency [2] . AHFSs are of particular public concern due to their capacity for large outbreaks, high fatality rates, and potential for global public health emergencies [1,3]. Hemorrhagic fevers such as Ebola, Lassa fever, Marburg virus disease and Crimean Congo fever are a group of illnesses caused by distinct families of ribonucleic acid viruses [4,5] . They are usually zoonotic in origin, with case fatalities ranging between 25% and 90% [1,5,6].
More than a third of the world’s population resides in regions at risk of these conditions, which come with significant macroeconomic implications [7]. Following the aftermath of the West Africa Ebola outbreak in 2014, the economy of the region was impacted, resulting in an estimated negative impact of USD2.8–32.6 billion on GDP and an overall cost of USD53.2 billion from mortalities, morbidities and socio-economic disruptions [8]. In addition, a 36% decline in gross domestic product was reported [8] . In Ghana, AHFS surveillance is part of the Integrated Disease Surveillance and Response (IDSR) system, which is geared toward early detection and response. This system employs the syndromic surveillance system approach using standard case definitions for case detection [9] . Cases presenting with AHFS-like symptoms have been suspected in Ghana. However, the country recorded its first-ever Marburg virus disease cases in July 2022 [10] .
All surveillance systems require periodic evaluations to improve effectiveness and quality. Weak surveillance systems have been linked to AHFS outbreaks [11-13] . An evaluation in Sierra Leone identified poor data quality, a lack of integration with other surveillance systems and poor stability as gaps of the AHFS surveillance system [11]. In Ghana, there remains limited research on AHFS surveillance system evaluations. A study which evaluated the AHFS surveillance system in Bawku Municipality in Ghana revealed that the system achieved its objectives; however, poor data quality, inadequately trained surveillance officers and inadequate financial support were factors that impeded the effectiveness of the system [14] .
Between 2019 and 2023, no documented evaluation of the AHFS surveillance system was conducted in the Sawla Tuna Kalba district. This evaluation was therefore conducted to assess the AHFS surveillance system. Specifically, we examined whether the system met its objectives, evaluated its performance based on key attributes and assessed its overall usefulness.
Evaluation design and setting
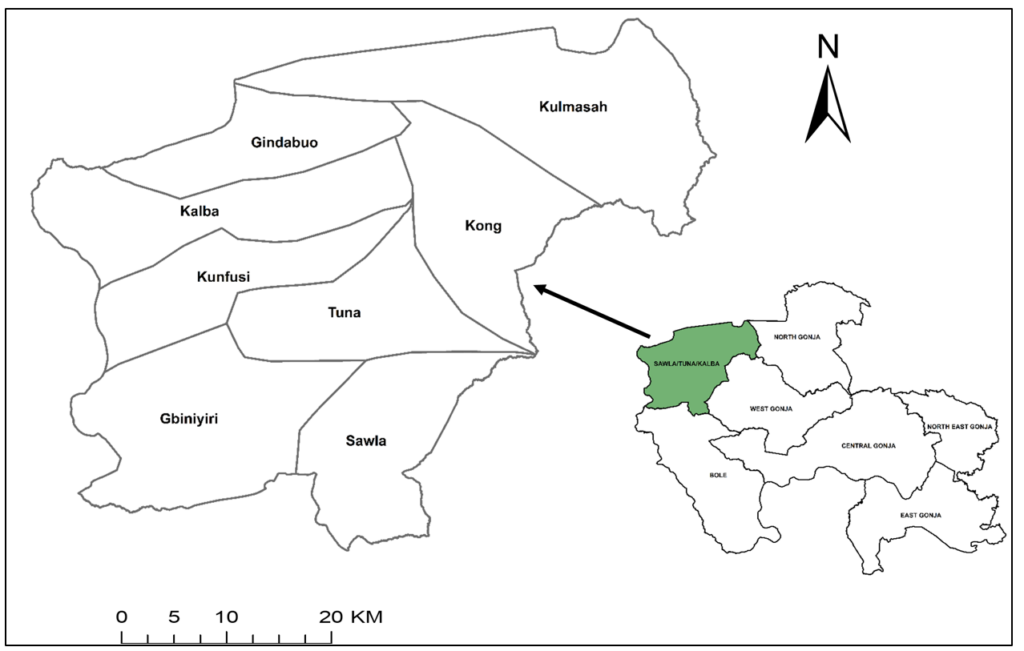
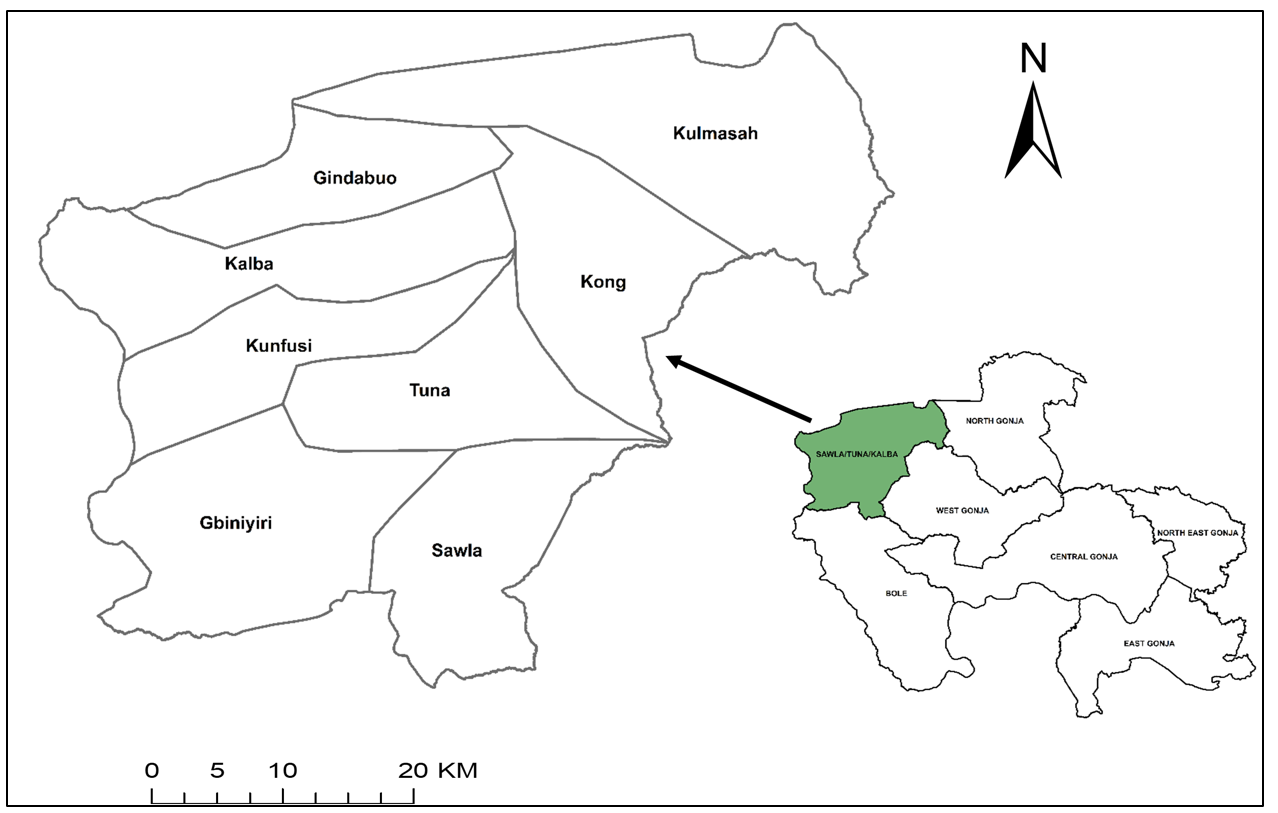
An evaluation of the acute haemorrhagic fever syndrome surveillance system was conducted in the Sawla Tuna Kalba District in 2024, for the period 2019-2023. The US-CDC Updated Guideline for Evaluating Public Health Surveillance Systems was adapted for this study [15]. Sawla-Tuna-Kalba District is located in the Savannah Region of Ghana, which is in the northern part of the country (Figure 1). The estimated population of the district for 2024 is 119,912, projected from the 2021 Ghana population and housing census. The major economic activities of the indigenes are farming and trading. The Black Volta River flows through the district and serves as a border between Ghana and most communities in the Ivory Coast [16] . The district is bordered by three other districts in the region and also shares international borders with the Ivory Coast and Burkina Faso [17] . Sawla Tuna Kalba District is divided into eight sub-districts. It has 25 health facilities comprising one district hospital, five health centres, one polyclinic, 16 Community-based Health Planning Services (CHPS) facilities and 2 private owned maternity homes [17] . Each sub-district has a disease surveillance unit responsible for monitoring and reporting all Integrated Disease Surveillance and Response (IDSR) diseases, including viral hemorrhagic fevers. The constant movement of people across these international borders raises concerns for the international spread of diseases. Sawla Tuna Kalba is close to the Mole Game Reserve, the largest game reserve in Ghana. This reserve may serve as a habitat for the transmission of some zoonotic conditions such as AHFSs and other diseases through various human and animal interactions [18] .
Evaluation population
The evaluated population included stakeholders involved in AHFS surveillance, namely the District Health Management Team (DHMT) members, regional surveillance focal persons, surveillance officers at the health facilities, clinicians at the various facilities and community-based surveillance volunteers (CBSVs). The evaluation population were persons resident in the Sawla Tuna Kalba district within the study period, irrespective of age or sex.
Stakeholders in AHFS surveillance
Stakeholders for the viral haemorrhagic fever surveillance system for the district consisted of the DHMT members, surveillance representative at the district hospital, surveillance focal persons at various health facilities and community-based surveillance volunteers at the various communities. External stakeholders included the Savannah Regional Health Directorate and the Noguchi Memorial Institute for Medical Research (NMIMR). Case investigators who were usually clinicians and surveillance focal persons at health facilities, were the first responders to all alerts at the various facilities. These stakeholders are responsible for policy implementation on surveillance activities in the district.
Operations of the surveillance system
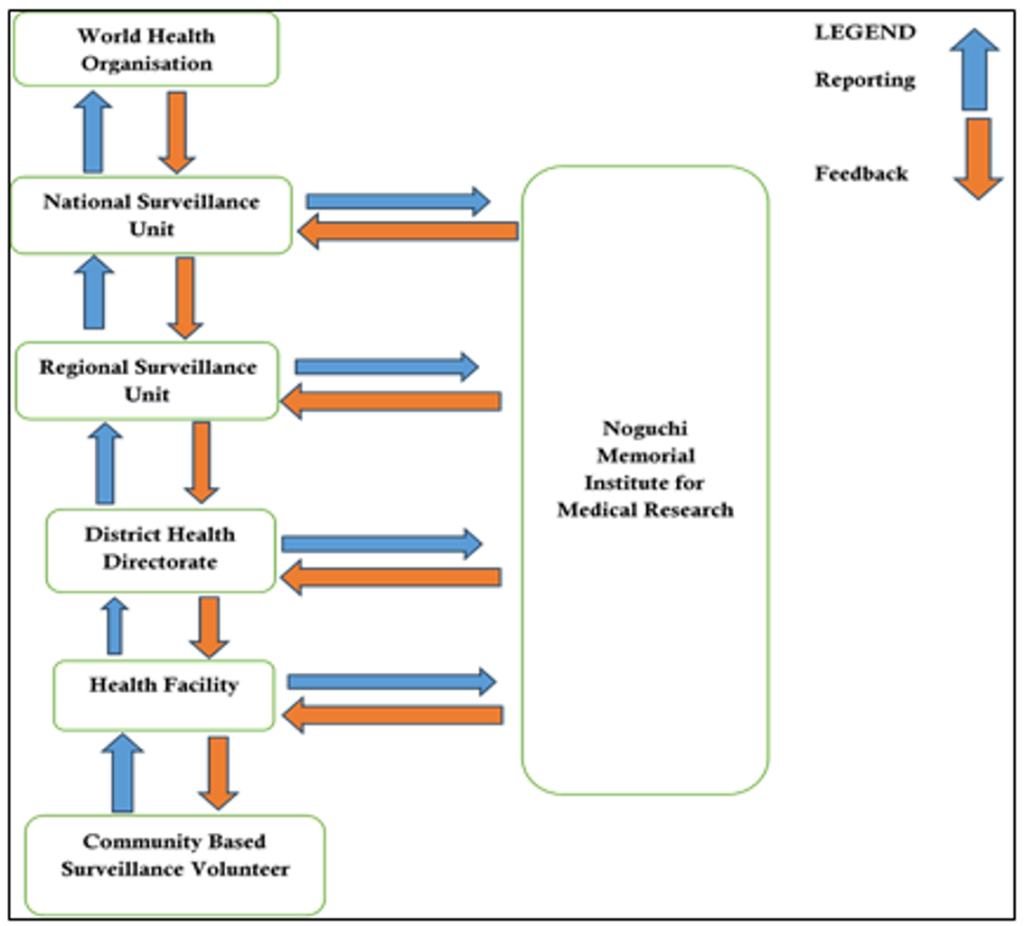
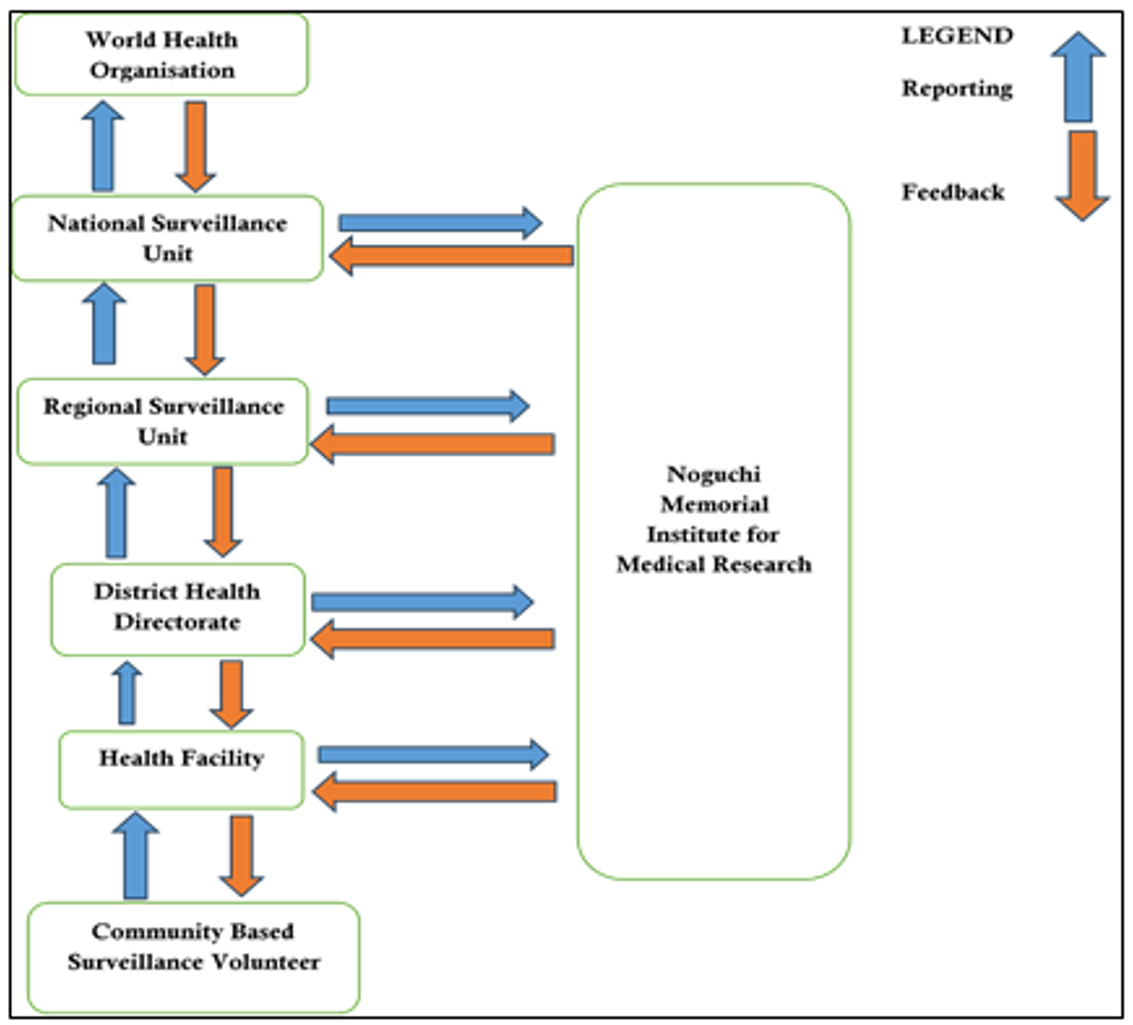
The Government of Ghana, through the health management system, mainly provides support for all health activities. This comes in the form of capacity building, payment of salaries and logistical support. This support mainly covers sample transport, contact tracing, case search and the purchase of logistics. The flow of information in the surveillance system follows the principles of the integrated disease surveillance and response system. This entails collaborative operation and transmission of information between community-based surveillance volunteers to facilities, district, regional, national and international communities. Case detection is done through active and passive surveillance.
At the community level, community-based surveillance volunteers conduct daily searches for any unusual health events. Any such event identified is promptly reported to the nearest health facility, either through phone calls or in person. Additionally, patients who visit any department within a health facility and exhibit signs and symptoms that meet the case definition for viral hemorrhagic fevers (AHFSs) are suspected by a clinician and recorded in the consulting room register.
A suspected case is immediately isolated, and the surveillance officer at the facility completes a case-based form for the case. The District Health Directorate is then notified, and a scanned copy of the case report form is promptly sent via WhatsApp to the district surveillance officer, who subsequently forwards it to the regional surveillance unit.
Upon detection at the district level, real-time data entry for these cases is conducted in the SORMAS system, and a laboratory test request is created by selecting the appropriate laboratory within the system. Blood samples are then taken from the patient for laboratory investigation. Laboratory testing for viral hemorrhagic fevers (AHFSs) is conducted at the Noguchi Memorial Institute for Medical Research (NMIMR). To prevent delays, blood samples together with hard copies of case-report forms are transported directly by the District Health Directorate to NMIMR for laboratory investigations within 48 hours of suspecting a case. Feedback on laboratory findings is reported to the national surveillance department for onward transmission to the regional surveillance department, through to the district within three days. Laboratory results are also immediately updated by NMIMR in SORMAS, which can be assessed by national, regional, and district-level users.
Case definitions
Suspected case: Anyone with acute onset of fever of less than three weeks duration in a severely ill patient/or a dead person AND any two of the following; haemorrhagic or purpuric rash, epistaxis (nose bleed), haematemesis (blood in vomitus), haemoptysis (blood in sputum), blood in stool, other haemorrhagic symptoms and no known predisposing factors for haemorrhagic manifestations OR clinical suspicion of any of the viral diseases [19].
Confirmed case: A suspected case with laboratory confirmation or epidemiologic link to confirmed cases or outbreak [19].
Data collection tools and methods
Data were collected using a semi-structured questionnaire developed using indicators adapted from the US-CDC Updated Guidelines for Evaluating Public Health Surveillance Systems. A key informant interview guide was also utilised to solicit qualitative responses from key stakeholders. Quantitative and qualitative data were collected, and these were primarily obtained through observations, face-to-face interviews and record reviews. Additionally, surveillance data from electronic data repositories, such as SORMAS (Surveillance Outbreak Response Management and Analysis System) and DHIMS (District Health Information Management System), were abstracted for review and analysis. The district hospital was purposively selected for the evaluation, while nine other health facilities were randomly sampled through balloting. We wrote all facility names on pieces of paper and drew nine at random. Surveillance officers and clinicians involved in surveillance activities at these facilities were purposively selected and interviewed on the viral haemorrhagic fever surveillance system in the district. We also purposively selected key stakeholders who were involved in surveillance activities at the district health directorate and regional health directorate for interviews on the AHFS surveillance system. Surveillance volunteers from four randomly selected communities in the district were also selected for interviews.
Data management and analysis
The data was entered, cleaned and analysed using Microsoft Excel version 2016. Descriptive statistics was used to analyse quantitative data, while qualitative data were analysed using directed content analysis. Nine attributes of the system were assessed in this evaluation. This included simplicity, acceptability, data quality, timeliness, flexibility, stability and representativeness. Except for the sensitivity and positive predictive value of the system, all other attributes in the evaluation were scored to assess performance. An indicator was scored zero if the key finding from the evaluation did not meet the standard requirement. For an indicator that met the standard required, a score of one was given. The assessment scores for each attribute were summed and divided by the total number of indicators assessed in order to determine the proportional score. For this evaluation, attributes with a proportional score less than 50% were considered poor, those between 50%-70% as moderate and scores above 70% as good.
Assessment of surveillance system objectives
To detect cases early for prompt management and control: Cases of this nature are expected to be detected within 24 hours of symptom onset. We assessed this objective by determining the mean time from the date of onset of clinical symptoms of cases and the time the health system was able to detect those cases. We further assessed this indicator by reviewing available contact tracing reports. These were assessed through interviews and record reviews.
To monitor the pattern of spread and burden of the disease in the population: This objective was evaluated using the availability of key indicators such as AHFS monitoring charts, spot maps and person, place and time analysis of AHFS data at the district surveillance unit. These were obtained through data review.
Investigate reported viral hemorrhagic fever cases and implement public health interventions: To assess this objective, the availability of outbreak investigation reports for confirmed cases, including evidence of public health interventions initiated for AHFS outbreaks, was analysed. This was obtained through record reviews and interviews.
Assessment of attributes: During the evaluation, nine key attributes were assessed, consisting of both qualitative and quantitative attributes. The qualitative attributes that were evaluated included simplicity, stability, representativeness, acceptability, and flexibility. Quantitative attributes assessed were sensitivity, positive predictive value, timeliness and data quality. Each of these attributes was assessed using specific indicators and a structured scoring criterion. Sensitivity and positive predictive values were, however, not assessed based on the scoring criteria (Table 2).
Usefulness of the system: We assessed the usefulness of the system by determining whether the system had been able to contribute to the rapid detection of reported AHFS cases, public health interventions taken during outbreaks and the use of the surveillance data for public health decisions. These were obtained through interviews and record reviews.
Ethical considerations
The study protocol was approved by the Ghana Health Service Ethical Review Committee (GHS-ERC: 023/05/24). Permission was also obtained from the Savannah Regional Health Directorate and the Sawla Tuna Kalba District Health Directorate to conduct the evaluation. The confidentiality of study participants was assured, and no information provided by them was divulged to any third party without approval.
Two Marburg cases, 29% (2/7), were confirmed over the period. Only 14.2% (1/7) of cases were detected within the recommended 24-hour interval. Only two samples, 28.5% (2/7), received feedback within 48 hours of being sent to the laboratory. The mean time taken to receive sample feedback was (5 ± 3.02) days. Participants highlighted the delay challenges in laboratory feedback to the surveillance system. One of them stated, “Sometimes we don’t receive laboratory results for these conditions early. Confirmation for some of these cases occurs outside the country. However, Noguchi sometimes confirms viral hemorrhagic fevers, but specific diseases such as Marburg need to be confirmed outside Ghana. This sometimes delays the surveillance system”. (Respondent 05, Savannah Regional Health Directorate)
Laboratory feedback is communicated to all the hospitals and health facilities through phone calls and durbar. The durbar is generally a community gathering that is organised to brief key stakeholders about a disease condition in the event of an outbreak and further seek community views and concerns to help tackle the outbreak effectively. Additionally, the regional surveillance department informs all district health directorates within the region through weekly epidemiological bulletins (Figure 2).
Resources used to operate the surveillance system
Funding for surveillance activities is mainly from the Government of Ghana through the District Health Directorate. This is needed especially in areas of sample transport, contact tracing, case search and the purchase of logistics. The government supports the system through the payment of regular salaries of various stakeholders involved in the system. Personal protective equipment (PPEs) such as surgical coveralls, face shields and gloves serve as crucial resources in infection prevention and control, which are highly needed especially when one is suspected of the condition. Other resources include Ethylene Diamine Tetracetic Acid tubes, which are used to collect suspected AHFS blood samples for confirmation.
To ensure these samples are kept within appropriate temperatures, transportation is done using reverse cold chain sample carriers under the triple packaging concept. Data management tools like the SORMAS tablets and computers for DHIMS entries are also essential resources used to operate the AHFS system. Cases of viral haemorrhagic fever are highly transmissible and require a structure mostly dedicated to the isolation of AHF cases when they occur due to their lethal condition. Trained personnel on integrated disease surveillance and response are human resources needed in the system. In Viral Haemorrhagic Fever Surveillance, diverse cadres of people are involved in its effective operations, who offer their expert knowledge depending on the level of surveillance. These include disease control officers, medical officers, nurses and community-based surveillance volunteers.
Assessment of surveillance system objectives
Early detection of cases for prompt management and control
The average time between the onset of symptoms and case detection was six (6 ± 6.9) days. Only one case was detected within 24 hours of symptom onset per the World Health Organisation’s recommended guidelines. Respondents identified several factors contributing to delays in seeking early treatment at healthcare facilities. These included reliance on home remedies, 82.1% (23/28), spiritual healing camps, 53.5% (15/28) and usage of traditional medicine, 92.9% (26/28).
Additionally, hard-to-reach communities and cultural beliefs further contributed to the late detection of cases. Participants shared their opinions regarding some reasons that could have contributed to the late detections encountered. A volunteer who was interviewed stated, “Conditions that present with signs and symptoms of acute haemorrhagic fevers are often seen by our people as spiritual illnesses and not a hospital sickness. Most people will therefore go to a herbalist or a prayer camp for treatment instead of seeking medical care. They may only go to the hospital when the condition has worsened”. (Respondent 19, Gbiniyiri Sub-district).
Specifically, the resort to traditional and spiritual methods of treatment when persons present with signs and symptoms of acute hemorrhagic fever syndromes was reported by respondents as one key contributor impeding early detection by the surveillance system. A key respondent recounted how it was hectic to trace one of the reported cases after getting a hint that the person was presenting with signs and symptoms. He stated, “We had a difficult task with tracking the index case during the outbreak. The case had left her house and was camped at a prayer camp. All efforts to get her whereabouts were fruitless for some time until we got the hint that she was camped there”. (Respondent 03, Sawla Tuna Kalba District Health Directorate)
Monitoring the pattern of spread and burden of the disease among the population
Contact tracing records for two confirmed cases were available at the district surveillance unit. A total of 88 contacts were followed up for two incubation periods. A contact who developed signs and symptoms during the follow-up period had their sample collected for testing, which subsequently returned a negative result. Additionally, weekly Integrated Disease Surveillance and Response (IDSR) monitoring charts were displayed at the surveillance unit to track trends in acute hemorrhagic fever syndromes (AHFSs). Furthermore, a research study on the seroprevalence of the Marburg virus among the population was conducted in the district, with support from the Kumasi Centre for Collaborative Research (KCCR).
Investigate reported viral hemorrhagic fever cases and implement public health interventions
Regional and district surveillance units conducted an outbreak investigation for an outbreak that occurred within the period. An outbreak report detailing the process and findings was available. A Social and Behavioural Change Communication (SBCC) report on various channels used to inform the public about the condition was also available.
Assessment of system attributes
Within the review period, seven cases were detected with a positive predictive value of 29%. Positive cases were confirmed for Marburg virus disease. The simplicity of the system was poor, with a score of 40%. Acceptability, timeliness and data quality of the system demonstrated moderate performances. Stability, flexibility and representativeness of the system were good. Various data reporting systems existed, and these were not synchronised with each other, which led to data disparities. There was poor reporting of community-based surveillance volunteers’ activities, with seven sub-districts not submitting reports. The system was flexible with the ability to modify the case definition during outbreak situations. Attribute scores were simplicity (40%), acceptability (60%), data quality (67%), timeliness (50%), flexibility (100%), stability (100%) and representativeness (100%) (Table 2).
Usefulness of the system
The information gathered from the surveillance system contributed to the detection of two cases of Marburg Virus Disease. The data generated was used to develop a comprehensive epidemic preparedness plan for the district. Additionally, the data generated from the system was used in planning public health education programs on Marburg and other AHFSs in communities. One of the respondents at the district level stated,
“Enhanced training through simulation exercises was carried out in the district to build the capacity of the members of the Public Health Emergency Management Committee and the Rapid Response teams in the district on emergency response. We have never had such a training here before, but because of the outbreak, we had the opportunity to be trained on viral haemorrhagic fever surveillance, which has been enlightening”. (Respondent 011, officer at District Health Directorate).
The health and economic impact of acute hemorrhagic fever outbreaks necessitate constant evaluations in order to identify gaps that need addressing. The objectives of the AHFS surveillance system are to promptly detect cases, trigger outbreak investigations and institute public health actions. The AHFS system in Sawla Tuna-Kalba could not meet the objective of prompt detection of cases. Given the devastating nature of AHFs and their tendency to cause large outbreaks, early detection of cases is crucial in informing the initiation of preventive efforts and limiting the occurrence of new infections. The surveillance system was sensitive with a high PPV. Despite these flaws, the system was useful in the detection of outbreaks. Whereas attributes such as stability, flexibility and representativeness of the system were good, the system was poor with regard to its simplicity.
Late detection of AHFS cases poses great danger to families and communities at large due to devastating outbreaks. It is recommended that AHF cases be detected within 24 hours of the onset of symptoms [20] . The surveillance system in Sawla Tuna Kalba district fell short in early detection, with most of the cases detected after 24 hours. Factors that were stated as contributory factors to these late detections in our evaluation included resort to home treatment, resort to spiritual camps for healing, hard-to-reach communities, poor community-based surveillance system and cultural beliefs. A systematic review on the Ebola viral disease outbreak in West Africa identified that the widespread embracing of certain traditional and religious practices among West African communities had tremendous negative effects on the spread of the disease [21] . Proper implementation of early warning alert mechanisms and effective surveillance response systems has been shown to contribute significantly to early detection [22] . The community-based surveillance system, which could help in early detection, was also not well functioning in the district. Revamping the community-based surveillance approach can help identify cases presenting with AHFS symptoms early, thereby preventing devastating outbreaks.
We adjudged the simplicity of the surveillance system to be poor. A key contributor to this shortfall was the existence of unsynchronised multiple reporting systems, resulting in data variations. Synchronisation is essential in building a system of good medical information exchange that is compatible with each other [23] . The SORMAS system, which had been launched in 2020, had not been synchronised with DHIMS, resulting in data disparities. Additionally, the transport of samples to the nation’s capital, which is about 500km for testing, is also a major complexity of the system. Despite the existence of a public health reference laboratory in the northern part of the country, it is not well-equipped to carry out tests for AHFSs. The arduous task of sample transportation could affect the commitment of surveillance officers in case of suspicion. In Bawku Municipality, Ghana, an AHF surveillance system evaluation also cited the system as complex, which is in line with our present findings [14] . Simple surveillance makes it easier for active participation by all stakeholders, which will in the long run, help increase the sensitivity of a system.
Overall, the surveillance system demonstrated notable strengths, particularly in attributes such as flexibility, representativeness, and stability, which received good performance scores. The introduction of the SORMAS system provided a robust platform for real-time data collection and management, thereby increasing the flexibility of the system. Additionally, the system’s capacity to modify case definitions during outbreak situations underscored its flexible nature, ensuring that all suspected cases are captured and not left out during outbreaks. During outbreaks, outbreak case definitions are often employed to broaden case detection, ensuring that a wide range of potential cases are identified. The stability of the system was strengthened through the goodwill shown by the government in funding surveillance activities. Sample transport and testing came at no cost to the patients. Insufficient funding has been identified as a significant barrier that can lead to poor surveillance outcomes. Poor surveillance funding can affect areas such as case detection, laboratory testing and sample transportation, among others [24] . In Nigeria, system evaluation identified transport and logistical challenges as factors that impeded the systems stability thereby making it poor [24] . Additionally, the availability of surveillance personnel at the various levels contributed effectively to the systems stability in the district over the period underscoring the strong surveillance workforce in the district.
Acceptability and data quality of the system were moderate. All stakeholders expressed willingness to actively continue AHFS surveillance, and they cited no misgivings. However, this evaluation identified various lapses in the CBSV system in the district, especially with report submissions. Seven sub-districts had poor CBSV systems with no report or follow-up on the activities of these volunteers. Community-based surveillance has been shown to improve early detection of cases and response to disease outbreaks by leveraging the capacity of community members to carry out surveillance activities within their communities [25] . Given that most of the communities in the Sawla Tuna Kalba District are far from health facilities, it is prudent that the CBSVs system be relied on to effectively monitor health events happening at the community level. A break in this system may result in missing cases, which may result in dire consequences. Motivations such as stipends for volunteers, award schemes for staff and the recognition of the hard work of community surveillance officers can help improve the acceptability of the surveillance operations by these volunteers. Studies have shown that a focus on the importance of intrinsic motivation promotes sustained involvement in volunteering and offers much to communities, and can be satisfied when their activities match their motivations [26] . Factors which could have accounted for the low surveillance activities by community volunteers could be the low motivations associated with volunteerism work and the limited supervisory activities carried out on the activities of these volunteers. In addition, it was realised that the CBS report form was not part of the data sets in DHIMS, which made sub-districts reluctant to follow up for reports since they would not be inputted. Studies in Liberia and Ghana revealed similar findings to our study on acceptability levels [14,27] . In contrast, a study in Tonkolili District, Sierra Leone, an assessment of the AHFS surveillance system found that the acceptability of the EVD surveillance system was poor, with most stakeholders not showing willingness in surveillance operations [11].
Limitations
The main limitation of this study was that stakeholders from the testing laboratories and the national surveillance unit were not interviewed, which could have given much clearer insights into the AHF surveillance system. The absence of interviews with these stakeholders may have introduced bias in the assessment of certain attributes, such as stability and data quality. Stability of the system could have been under-scored or over-scored due to limited insights on laboratory capacities and workforce capacity at the national level. Data quality issues such as data completeness, data transmission and incomplete data on the surveillance system, identified at the national level, could have also given more insights on how to improve the AHFS surveillance at the district level. Additionally, the cost of management of the AHFS surveillance system was not assessed in this evaluation due to the limited availability of data to assess the indicators of this attribute. A cost assessment could have provided a more detailed assessment of the stability of the system by quantifying financial commitments to critical areas of the surveillance system, such as personnel, logistics, and laboratory testing. This could potentially inform stakeholders on resource allocation and distribution for the system’s improvement. Despite these limitations, the findings from this study provide useful insights on improving the AHFS surveillance system in the Sawla Tuna Kalba District.
The acute hemorrhagic fever surveillance system in the Sawla Tuna Kalba District is well structured and useful. The system partially met its objectives. The system is flexible, stable, and representative. The simplicity of the system was found to be poor and needs to be made less complex. Acceptability, timeliness and data quality of the system were moderate in performance and need to be improved. The system was sensitive with a high PPV. We recommend that the Ghana Health service Health Information Department at the national level take steps to synchronize the DHIMS and SORMAS systems. Additionally, the CBSV report dataset should be incorporated into the DHIMS to enhance reporting.
What is already known about this topic
What this study adds
| Table 1: Distribution of key respondents, AHFS surveillance system Sawla Tuna Kalba District, 2024 | ||
|---|---|---|
| Key Informant | Frequency (%) | Percentage |
| Median years of service 6 (Range= 3–30)years | ||
| Disease Control Officers | 9 | 32.2 |
| Community Health Nurse | 6 | 21.4 |
| Community Based Surveillance Volunteer | 4 | 14.2 |
| Nurse (clinical) | 4 | 14.2 |
| District Director of Health Services | 1 | 3.6 |
| Health Promotion Officer | 1 | 3.6 |
| Medical Officer | 1 | 3.6 |
| Physician Assistant | 1 | 3.6 |
| Regional Surveillance Officer | 1 | 3.6 |
| Total | 28 | 100 |
| Table 2: Key findings from assessment of attributes of AHFS surveillance system in Sawla Tuna Kalba district, 2024 | |||||
|---|---|---|---|---|---|
| SYSTEM ATTRIBUTE | INDICATOR | How it was assessed | KEY FINDINGS | Assessment Score | Percentage |
| Simplicity | Respondent’s knowledge of the case definition and perception of how easy it is. | Ability of respondents to state the case definition for acute hemorrhagic fever syndromes and perception of ease of use of the case definition | The majority, 85 % (24/28), of the respondents knew the AHFS case definition, and a total of 87.5% (21/24) of them could state at least two signs and symptoms for a suspected case. Most, 83.3% (20/24), of the respondents who knew the case definition deemed it easy | 1 | 40% |
| The ease in filling case-based forms for AHFS | Time taken to fill case-based form | An average of 5 minutes is needed to fill the case-based form | 1 | ||
| Ease of reporting | Whether one reporting format existed for the same information or not. | Numerous reporting formats existed: weekly IDSR, Monthly IDSR, and SORMAS | 0 | ||
| Synchronization of various data reporting systems | Evidence of various reporting systems being synchronized. | The various reporting systems being used were not synchronized with each other | 0 | ||
| Proximity of testing laboratory to district | The closeness of the testing laboratory to the district, and whether samples can be transported within 2 hours | Samples need to be transported to an external Laboratory for confirmation, which takes about 12 hours. | 0 | ||
| Stability | Funding for surveillance activities | Evidence of funding commitments on surveillance by various stakeholders | The government supports through the payment of salaries. The central government bears the cost of sample testing. Also, the cost of surveillance trainings borne by donors and the government | 1 | 100% |
| Integration of acute haemorrhagic syndrome surveillance system with the IDSR system | Whether the surveillance system is being integrated with the broader IDSR* system | AHFS surveillance system is integrated with IDSR system | 1 | ||
| Availability of surveillance focal persons at each level | Evidence of availability of surveillance focal persons at community, facility, district, and regional levels | All levels of the surveillance system had focal persons All facilities visited had persons who acted as surveillance focal persons at those levels | 1 | ||
| Representativeness | Health facilities involved in surveillance | Number of health facilities reporting on weekly and monthly IDSR | All health facilities reporting on weekly and monthly IDSR. | 1 | 100% |
| Sub-districts suspecting and reporting cases including zero reporring | The number of sub-districts that are submitting surveillance reports on acute hemorrhagic fever syndromes | All eight (8) sub-districts were submitting weekly and monthly reports, including zero reporting | 1 | ||
| Distribution of cases by sex, age | Whether cases being suspected were fairly distributed by age and sex | Suspected cases consisted of both genders (4 females and 3 males) Median age is 8 years. Range = (10 months – 35 years) Cases consisted of both adults and children | 1 | ||
| Acceptability | Proportion of completed case-based forms available. | Whether case-based forms for all suspected cases were available for reference | All seven case-based forms for cases suspected within the evaluation period were available. | 1 | 60% |
| *CBSVs monthly report submissions 2023 | The number of CBSVs reports for the year 2023 that were available at the various sub-district levels. | Community-based surveillance reporting was not part of the DHIMS* dataset, though a reporting form was available for compilation of monthly reports. For the year 2023, only one (1/8) sub-district had complete CBSVs reports available | 0 | ||
| Outbreak investigation and contact tracing conducted for outbreaks | Availability of outbreak investigation reports and contact tracing reports for any outbreaks reported within the period | Outbreak investigation reports for an outbreak that occurred in 2022 were available. Contact tracing lists for 88 contacts were available (list captured contacts by person, place, and time characteristics). | 1 | ||
| SORMAS entries | Whether all suspected cases were entered into the SORMAS system | Entry of cases into SORMAS was not done. | 0 | ||
| Willingness by stakeholders to continue with AHFS surveillance | Whether all stakeholders were willing to continue working effectively in their role as surveillance persons at their various levels | All stakeholders interviewed expressed willingness to continue working efficiently on AHFS surveillance. | 1 | ||
| Flexibility | Ability to modify case definition to meet prevailing demands | Whether an outbreak case definition exists | The case definition can be modified during outbreaks. An outbreak case definition is used during outbreak situations to help capture more cases. | 1 | 100% |
| System integrated with the IDSR surveillance system | Whether the system is integrated with the IDSR system | System integrated with IDSR system | 1 | ||
| Changes in the mode of reporting to meet current surveillance updates | Evidence of new changes that have been implemented to improve the system without causing major distortions. | The SORMAS system was introduced in 2020, which served as a surveillance tool for real-time data reporting of surveillance data. | 1 | ||
| Sensitivity | Number of cases detected by the system | The sensitivity of the surveillance system was assessed at the level of case detection through retrospective review of routine surveillance data. Suspected cases were identified based on the established case definition captured in the reporting systems. | Seven (7) cases were suspected over the period of evaluation. | N/A | N/A |
| Positive Predictive Value | Proportion of cases that were positive for AHFS | Two cases were confirmed, giving a PPV of 29% (2/7) | N/A | N/A | |
| Timeliness | Average reporting timeliness for the past five years (2019-2023) | Whether the timeliness of reporting is more than 90% | The average timeliness of reporting for weekly IDSR was 91.1%. | 1 | 50% |
| Time between the onset of symptoms and case detection | Whether all confirmed cases were detected within 24 hours | The two confirmed cases were not promptly detected within 24 hours of symptom onset. These were detected 21 days and 5 days after date of onset, respectively | 0 | ||
| Time taken to receive sample feedback from testing laboratories | Whether feedback for all samples transported was received within 48 hours upon sample transportation. | Laboratory results from NMIMR were received within 48 hours for only 28.5% (2/7) of the samples transported for testing | 0 | ||
| Time taken to transport the sample to the testing laboratory | Whether samples collected were transported within 24 hours | All samples transported within 24 hours of collection | 1 | ||
| Data Quality | Availability of the linelist of cases at district and regional levels | Whether reported cases were line-listed | All cases suspected within the evaluation period were line listed, with copies of the linelist available at the district and regional levels | 1 | 67% |
| Completeness of variable fields in the linelist and case-based forms | The number of variable fields in the linelist and case-based forms that were completed | A proportion of 338/344 fields were completed in line-list, thus (98.2%) completeness. A total of 93% (163/175) of the fields were completed for all seven(7) case report forms available | 1 | ||
| Data variations across reporting sources | Whether the same number of cases was reported among the various reporting channels | Variations existed across sources; Linelist contained 7 suspected and 2 confirmed cases, The DHIMS system had 8 suspected and 1 confirmed case while there were zero entries in the SORMAS system | 0 | ||
| *IDSR – Integrated Disease Surveillance and Response *SORMAS – Surveillance Outbreak Response Management and Analysis System *CBSVs – Community-based Surveillance Volunteers *DHIMS – District Health Information Management System | |||||