Review | Open Access | Volume 9 (2): Article 77 | Published: 18 May 2026

Views: 2,152
Menu, Tables and Figures
| Database | Initial hits | After duplicates removed | Relevant articles (title/abstract screening) | Final included |
|---|---|---|---|---|
| PubMed | 12 | 12 | 4 | 2 |
| Google Scholar | 23 | 21 | 8 | 3 |
| Web of Science | 10 | 10 | 6 | 3 |
| NIH | 8 | 6 | 3 | 2 |
| AJOL | 7 | 6 | 2 | 2 |
| Total | 52 | 49 | 23 | 12 |
| Author (Year) | Study Design | MMAT Category | Criteria Met (out of 5) | Rating (%) | Quality Level |
|---|---|---|---|---|---|
| Saleh et al. (2022) | Cross-sectional | Quantitative descriptive | 4/5 | 80% | Moderate–High |
| Olumade et al. (2022) | Case study | Mixed Methods | 5/5 | 100% | High |
| Otu et al. (2017) | Mixed-methods | Mixed Methods | 5/5 | 100% | High |
| Wolicki et al. (2016) | Case study | Quantitative descriptive | 4/5 | 80% | Moderate–High |
| Jacobs & Okeke (2022) | Systematic review | Not Applicable | N/A | N/A | Included for synthesis only |
| Olumade et al. (2020b) | Prospective cohort | Quantitative non-random | 3/5 | 60% | Moderate |
| Elimian et al. (2019) | Retrospective analysis | Quantitative descriptive | 5/5 | 100% | High |
| Atanda et al. (2021) | Case-control | Quantitative non-random | 4/5 | 80% | Moderate–High |
| Orji et al. (2023) | Cross-sectional | Quantitative descriptive | 5/5 | 100% | High |
| CDC (2014) | Qualitative | Qualitative research | 4/5 | 80% | Moderate–High |
| Adeoye et al. (2013) | Case study | Quantitative descriptive | 3/5 | 60% | Moderate |
| Okeke et al. (2022) | Retrospective | Quantitative descriptive | 4/5 | 80% | Moderate–High |
Table 2: MMAT 2018 Quality Assessment of Included Studies
| Partner Category | Specific Actors | Reported Contributions | Outbreaks Where Documented |
|---|---|---|---|
| International Agencies | WHO, U.S. CDC, MSF, UNICEF, Africa CDC, Resolve to Save Lives, UKHSA (and their implementing/field partners) | Technical expertise; deployment of personnel; diagnostic support; funding; logistical support; direct implementation of surveillance, case management, and training | Ebola, Lassa Fever, COVID-19, Cholera, Diphtheria |
| Local Civil Society | Traditional Rulers, religious leaders, community-based organizations, local NGOs/implementing partners (e.g., local CSOs funded by UNICEF/WHO/MSF, community health volunteers) | Mobilizing community trust & participation; facilitating contact tracing; countering misinformation; promoting safe practices; field-level implementation of risk communication, vaccination, and WASH activities | Ebola, Lassa Fever, COVID-19, Cholera, Measles |
| Private Sector | Telecom Companies, Domestic Pharmaceutical Firms, Banks | Mass SMS/public health messaging, donation of PPE/medical supplies, financial donations/logistical support | COVID-19 |
| Academic/Research Institutions | Nigerian Universities, International Research Collaboratives | Operational research; data analysis; technical support as part of EOC teams and AARs | Multiple Outbreaks |
Table 3: Categorization and documented contributions of multisectoral partners in Nigeria’s outbreak responses
Attahir Abubakar1,&, Comfort Kingsley-Randa2, Ni’ima Abubakar Fage3
1Department of Public Health Distance Learning Centre, Ahmadu Bello University, Zaria, Kaduna, Nigeria, 2Technical Assistance Connect (TAConnect), Abuja, Nigeria, 3Kano State Centre for Disease Control, Kano, Nigeria
&Corresponding author: Attahir Abubakar, Department of Public Health Distance Learning Centre, Ahmadu Bello University, Zaria, Kaduna State, Nigeria, Email: attahirabubakar@live.com ORCID: https://orcid.org/0000-0002-9916-3971
Received: 14 Jul 2025, Accepted: 11 May 2026, Published: 18 May 2026
Domain: Infectious Disease Epidemiology
Keywords: Infectious disease outbreaks, Nigeria, public health response, epidemic preparedness, health systems, outbreak response
©Attahir Abubakar et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Attahir Abubakar et al., Lessons learned from Nigeria’s public health responses to infectious disease outbreaks: A systematic review. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):77. https://doi.org/10.37432/jieph-d-25-00157
1Department of Clinical Research, Training, and Consultancy, Southern Zone Referral Hospital, Mtwara, Tanzania, 2Department of Clinical Laboratory, Southern Zone Referral Hospital, Mtwara, Tanzania, 3Department of Clinical Laboratory, Southern Zone Referral Hospital, Mtwara, Tanzania
Introduction: Nigeria has experienced repeated outbreaks of infectious diseases, such as Lassa fever, cholera, Ebola, and COVID-19, which have consistently challenged its public health response capabilities. This systematic review sought to consolidate evidence regarding the successes, challenges, and insights derived from Nigeria’s outbreak responses from 2010 to 2023 to enhance future preparedness.
Methods: We conducted a systematic review following the PRISMA 2020 guidelines. A thorough search of five databases (PubMed Central, Web of Science, Google Scholar, Africa Journals Online, and NIH Library) was conducted for peer-reviewed English articles published between 2010 and 2023. Studies were included if they focused on Nigeria’s outbreak response strategies. The methodological quality of the included studies was evaluated utilizing the Mixed Methods Appraisal Tool (MMAT 2018).
Results: Out of 52 identified records, 12 studies met the inclusion criteria. The findings were synthesized around four core objectives. Identified key strengths encompassed the efficient implementation of rapid case detection, contact tracing, and the coordinating function of national and state-level Emergency Operations Centers (EOCs). However, significant challenges persist, including critical subnational coordination delays averaging 5-7 days, fragile community trust leading to high refusal rates (15-20%) for contact tracing and vaccination, and a heavy reliance on multisectoral partners to fill systemic gaps in funding and logistics.
Conclusion: Although Nigeria has established a comprehensive array of response strategies and coordination mechanisms at the national level, the efficacy of its outbreak response is persistently compromised by subnational operational impediments and diminished community trust. To build a resilient health security architecture, Nigeria must prioritise decentralising response capacity, institutionalising sustainable trust-building community engagement, and securing predictable domestic financing for preparedness.
Nigeria, Africa’s most populous country, persistently faces frequent and severe outbreaks of infectious diseases that continually strain its public health infrastructure. The nation’s ability to detect, prepare for, and respond in a coordinated manner has been persistently challenged by endemic diseases like malaria and Lassa fever, alongside epidemics such as the 2014 Ebola virus outbreak and the COVID-19 pandemic [1, 2]. The constraints are particularly evident in resource-constrained settings and have led to significant consequences even during localized epidemics, thereby highlighting potential risks during global public health emergencies. A systematic review of Nigeria’s response to major disease outbreaks is crucial for identifying operational strengths, highlighting persistent gaps, and guiding future epidemic preparedness.
Lassa fever, an endemic rodent-transmitted viral illness, continues to be a significant national health issue. From 2020 to 2023, there were 28,780 suspected cases and 4,036 confirmed cases reported, leading to 762 fatalities (CFR 18.9%); as of November 2025, 7,673 suspected cases and 166 deaths have been recorded across 21 states [3, 4]. Surveillance records from 2016 to 2023 indicated 8,978 suspected cases and 1,227 confirmed fatalities, with the 2023 transmission season alone reporting over 1,070 cases and 227 deaths, illustrating its increasing geographical distribution [3, 5].
Cholera, closely associated with insufficient water, sanitation, and hygiene (WASH) conditions, persists in triggering extensive epidemics. The 2010 outbreak yielded 41,787 suspected cases and 1,716 fatalities (CFR 4.1%), succeeded by 44,471 cases and 830 deaths (CFR 1.9%) in 2018. As of September 2025, there were 10,353 reported cases and 244 fatalities (CFR 2.4%) across 32 states. The 2021 cholera epidemic underscored the magnitude of the issue, recording 111,062 suspected cases and 3,604 fatalities (CFR 3.2%), making it one of the largest outbreaks globally that year [6, 7].
The 2014 Ebola virus disease outbreak, originating from Liberia, was contained within 93 days, resulting in 20 confirmed cases and 8 fatalities (CFR 40%) due to effective contact tracing and international cooperation [8, 9]. Conversely, the COVID-19 pandemic (2020–2023) revealed significant systemic vulnerabilities, especially at subnational tiers. Restricted testing capabilities, insufficient medical oxygen availability, and disjointed coordination impeded the national response. As of mid-2023, there were 266,283 confirmed cases and 3,155 fatalities (CFR 1.2%), although under-reporting likely obscured the actual impact.
Measles outbreaks have persisted, primarily due to inadequacies in routine immunization in northern Nigeria. From 2012 to 2016, there were 131,732 suspected cases and 817 fatalities (CFR 0.62%), followed by over 28,000 cases in 2019 and 4,034 confirmed cases with 33 deaths (CFR 0.81%) in 2023; roughly 83% of cases involved zero-dose children [10, 11]. Recently, a significant resurgence of diphtheria from December 2022 to March 2024 led to over 24,000 suspected cases, 15,147 confirmed cases, and 1,522 fatalities. By early 2025, cumulative totals reached 42,642 suspected and 25,812 confirmed cases, resulting in 1,319 fatalities (CFR 5.1%), predominantly among children aged 1–14 years (63% of cases), highlighting significant deficiencies in immunization coverage.
These recurring epidemics transpire within a broader context of health system inadequacies, characterized by chronic underfunding, substantial workforce deficits, and fragmented surveillance systems [12, 13]. The Nigeria Centre for Disease Control (NCDC) has helped Nigeria improve its emergency coordination, risk communication, and rapid containment. However, there are still big problems with how things are done at the local level and how involved the community is. A comprehensive analysis of Nigeria’s outbreak-response strategies is crucial to identify transferable lessons, enhance preparedness systems, and strengthen national health security and resilience against future epidemics and pandemics.
Nigeria, being the most populous country in Africa, has faced numerous public health challenges over the years. From endemic diseases such as malaria to epidemics like the Ebola outbreak in 2014 and the recent COVID-19 pandemic, Nigeria’s public health response mechanisms have been put to the test [14]. These gaps are especially evident in resource-limited settings and have posed challenges during relatively localized epidemics, with dire implications for what may happen during a full-fledged global pandemic. A systematic review of Nigeria’s public health response across various health challenges will provide insights into areas of strength and potential improvement. Understanding the lessons learned can inform both Nigeria and other countries on effective strategies and pitfalls to avoid in future public health crises.
We analyzed Nigeria’s public health response to recent infectious disease outbreaks to examine public health response strategies implemented during major infectious disease outbreaks in Nigeria between 2010 and 2023 and assess their effectiveness in early detection, containment, and mortality reduction while identifying coordination and system gaps and synthesizing multi-method evidence to inform strengthened national preparedness and response.
Search strategy
This review was conducted in line with the PRISMA 2020 guidelines [15]. The literature search was conducted between January and April 2024. To identify relevant studies on Nigeria’s public health response to infectious disease outbreaks, we carried out a comprehensive and systematic search across several major academic databases. These included PubMed, Web of Science, Google Scholar, the National Institutes of Health (NIH) database, and African Journals Online (AJOL). These databases collectively cover a broad range of biomedical, public health, and region-specific literature. We used a combination of keywords such as “Nigeria,” “infectious disease,” “outbreak,” “public health,” “response,” and “strategies,” applying Boolean operators to capture a wide spectrum of relevant studies. The search was limited to articles published between 2010 and 2023 to ensure the review reflects developments in the last decade.
Search filters applied and reporting guidelines
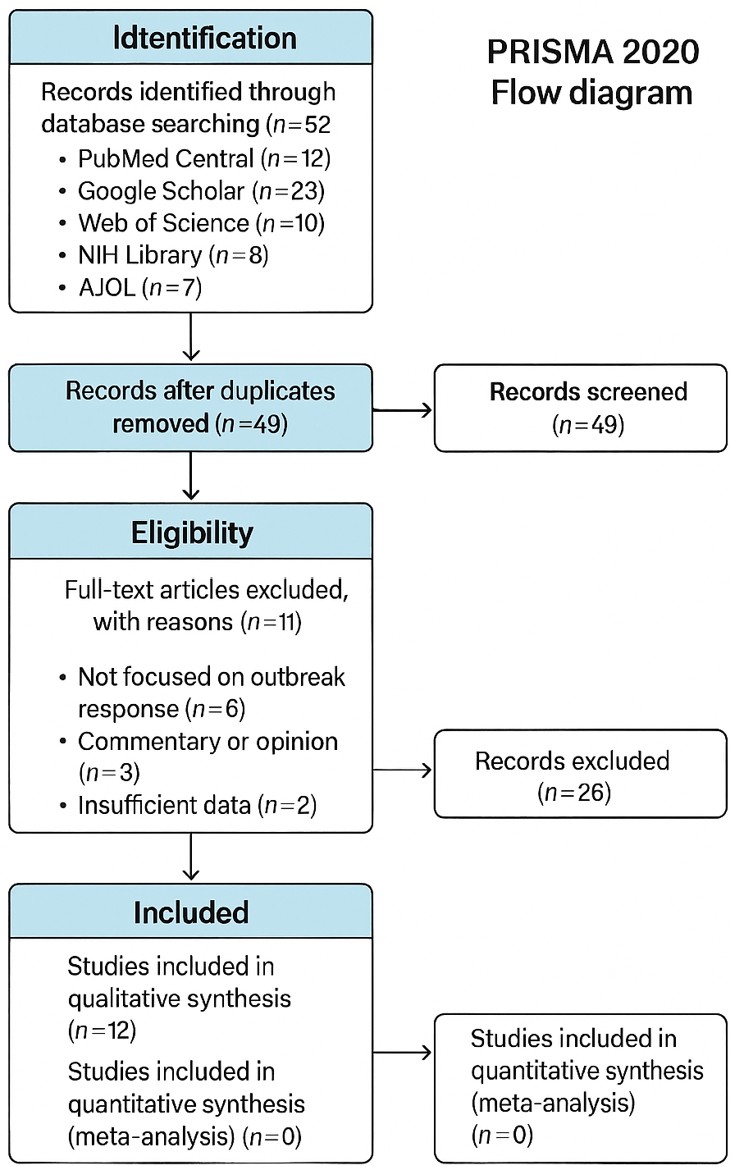
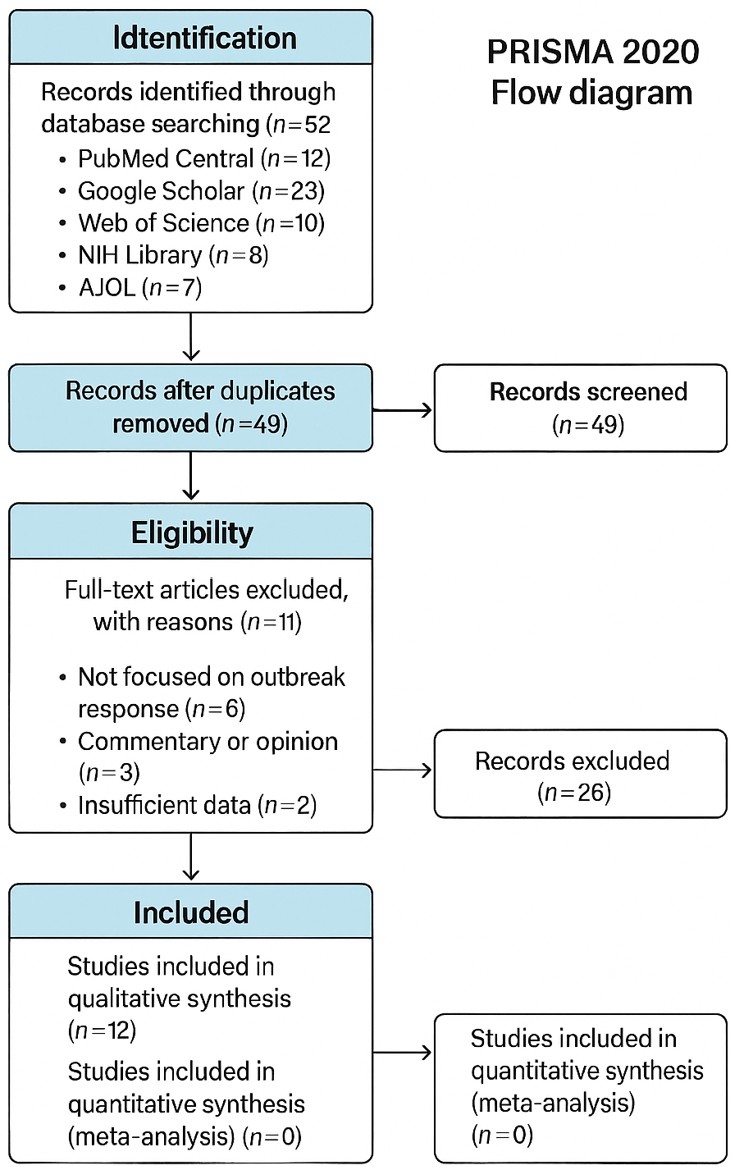
Language: English only Publication Type: Peer-reviewed journal articles; Country Context: Nigeria; Article Type: Original research (quantitative, qualitative, mixed methods). This systematic review was conducted and reported in accordance with the PRISMA 2020 guidelines. The study followed the recommended framework for identification, screening, eligibility assessment, and inclusion of relevant studies. A PRISMA flow diagram was used to illustrate the study selection process (Figure 1).
PRISMA flow of study selection
A total of 52 records were identified through database searching. After removal of duplicates (n = 3), 49 records remained for title and abstract screening. Of these, 26 records were excluded based on irrelevance to the study objectives, leaving 23 articles for full-text assessment. Following full-text review, 11 articles were excluded for not meeting the inclusion criteria, resulting in 12 studies included in the final qualitative synthesis (Table 1).
Eligibility criteria
Titles and abstracts were independently screened by two reviewers for eligibility. Full-text articles were subsequently assessed against the inclusion criteria. Discrepancies were resolved through discussion and consensus. They were original research (quantitative, qualitative, or mixed methods); published in English; and they specifically examined response strategies or interventions implemented during infectious disease outbreaks in Nigeria. Commentaries, editorials, or opinion pieces that focused solely on the epidemiology of outbreaks without discussing public health responses were excluded.
Data synthesis
Relevant data from the included studies were extracted and synthesized narratively to address the four primary objectives of the review. Findings were organized thematically around public health response strategies and interventions; effectiveness and outcomes; strengths, gaps, and bottlenecks in coordination, surveillance, resource mobilization, and community engagement; and contributions of multisectoral partners. No meta-analysis was performed due to heterogeneity in study designs, outcomes, and outbreak contexts; results are therefore presented as a qualitative synthesis supported by tables and a narrative summary.
Quality assessment and protocol registration
The methodological quality of the 12 included studies was evaluated using the Mixed Methods Appraisal Tool (MMAT) 2018 [16]. Each study was categorized according to its primary design and appraised against the relevant five methodological criteria (out of five possible). Ratings are expressed as percentages of criteria met (e.g., 4/5 = 80%). Studies meeting ≥80% were rated high quality; 60–79%, moderate; and below 60%, low (none fell below 60% in this review). For the systematic review by Jacobs & Okeke (2022), no MMAT scoring was applied, as it served synthesis purposes only. The quality ratings for each included study are presented in Table 2. The review protocol was registered with Prospero (CRD420251102766).
Ethics consideration
This study is a systematic review of publicly available literature and does not involve human participants or identifiable personal data. As such, ethical approval was not required. The review adhered to the PRISMA 2020 guidelines and was conducted with academic integrity.
The literature reviewed provides important insights into the strengths and persistent weaknesses of Nigeria’s public health preparedness systems, particularly in relation to laboratory infrastructure, surveillance coordination, and operational capacity at subnational levels. Across outbreaks of Ebola, cholera, measles, Lassa fever, COVID-19, and diphtheria, three broad themes emerge following a systematic search and screening process of 12 studies that met the inclusion criteria: surveillance systems and coordination in outbreak response, persistent gaps in diagnostic and laboratory capacity, and implementation challenges across health systems at different levels. These themes are directly relevant to the present study, which seeks to examine how diagnostic system capacity influences outbreak detection and response effectiveness in Nigeria. In addition, context is also provided for disease-specific insights, structural determinants, and the implications for strengthening diagnostic systems.
Surveillance systems and coordination in outbreak response
Several studies reviewed highlight the role of strengthened surveillance and coordination mechanisms in improving outbreak preparedness and response. Analyses of Nigeria’s surveillance architecture within the Global Health Security Agenda demonstrate that the institutionalization of a national public health institute significantly improved coordination between surveillance, laboratory, and response functions [17]. This integration strengthened early outbreak detection and enhanced the ability of response agencies to coordinate public health interventions across diseases. Evidence from Nigeria’s response to the 2014 Ebola outbreak further illustrates the importance of coordinated incident management systems. Rapid activation of an emergency operations center, supported by intensive contact tracing and coordinated surveillance activities, enabled the country to contain the outbreak within ninety-three days [18]. Similarly, mixed-methods evaluations of the Ebola response emphasize that rapid incident management activation and effective contact tracing were central to containment efforts [19].
Strengthened surveillance approaches have also improved outbreak monitoring in the context of vaccine-preventable diseases. Case-based surveillance introduced during measles outbreaks significantly improved case detection and monitoring compared with passive surveillance approaches [10]. These findings underscore the value of robust surveillance systems in supporting early identification of outbreaks and guiding timely response activities.
Although these studies provide important evidence on the effectiveness of surveillance and coordination systems, much of the literature focuses primarily on institutional arrangements and response structures. Less attention has been given to the operational role of diagnostic capacity within these surveillance systems, particularly at subnational levels where initial case detection often occurs.
Persistent gaps in diagnostic and laboratory capacity
Despite improvements in surveillance and coordination mechanisms, limitations in diagnostic capacity remain a consistent finding across outbreak investigations. Studies examining Nigeria’s response to concurrent outbreaks, including Lassa fever and COVID-19, indicate that delays in sample processing and confirmation remain a major constraint for timely outbreak detection [14]. Diagnostic confirmation frequently relies on national reference laboratories, while many states and local government areas lack adequate laboratory infrastructure to support rapid testing. The COVID-19 pandemic further exposed these diagnostic constraints. During the early stages of the pandemic, testing capacity was limited and concentrated in a small number of laboratories, resulting in substantial under-detection of cases [13]. Although testing capacity expanded through the establishment of zonal laboratory networks, supply chain challenges, including shortages of reagents and testing materials, continued to affect diagnostic operations [20].
Similar diagnostic challenges have been documented in other outbreaks. Retrospective analyses of cholera outbreaks found that fragile sample referral systems and delays in laboratory confirmation slowed outbreak verification and response coordination across states [6]. Broader reviews of outbreak responses in Nigeria, therefore, consistently identify laboratory infrastructure and diagnostic capacity limitations as key bottlenecks affecting early outbreak detection [21]. However, much of the existing literature describes these diagnostic gaps in broad terms without systematically examining how diagnostic capacity at different levels of the health system influences outbreak response outcomes. This gap highlights the need for further analysis of the role of laboratory systems within broader outbreak preparedness frameworks.
Implementation challenges across health systems at different levels
Another recurring theme in the literature is the gap between national policy frameworks and implementation capacity at the subnational level. Systematic reviews of Nigeria’s pandemic response highlight a disconnect between federal-level policies and the operational capacity of state and local health systems responsible for implementing response activities [20]. Limited laboratory infrastructure, uneven distribution of resources, and logistical constraints have contributed to delays in outbreak detection and containment in several states.
Operational learning approaches have further documented these challenges. After-Action Reviews conducted following urban outbreak responses have proven useful in identifying operational gaps and informing preparedness improvements [22]. However, these reviews frequently highlight delays in diagnostic confirmation and prolonged laboratory turnaround times as recurring weaknesses in outbreak response systems.
Studies examining healthcare workforce preparedness also reveal important implementation constraints. Surveys assessing healthcare workers’ knowledge, attitudes, and practices during the COVID-19 pandemic identified significant deficiencies in infection prevention and control practices, largely attributable to inadequate training and resource limitations [26]. While these studies focus primarily on workforce preparedness, they also indirectly underscore the importance of reliable diagnostic support systems for confirming suspected cases and guiding clinical and public health responses.
Disease-specific insights and structural determinants
Disease-specific outbreak investigations provide additional insight into structural determinants shaping outbreak dynamics in Nigeria. Analyses of cholera outbreaks consistently identify poor water, sanitation, and hygiene infrastructure as a major driver of transmission, while weaknesses in real-time data reporting complicate coordination across affected states [7]. Similarly, recent analyses of diphtheria outbreaks in northern Nigeria demonstrate a strong association between low routine immunization coverage and outbreak severity [23]. In several high-burden states, laboratory confirmation rates were low, with many cases classified on clinical or epidemiological grounds due to delays in sample transport and testing. These delays undermine early detection and limit the accuracy of outbreak response strategies.
Implications for strengthening diagnostic systems
Overall, the literature suggests that Nigeria has made considerable progress in strengthening surveillance systems and national coordination mechanisms for outbreak response. Nevertheless, the effectiveness of these systems continues to be constrained by weaknesses in diagnostic infrastructure, particularly at subnational levels where initial case detection occurs [21].
Strengthening laboratory networks, improving sample referral systems, and expanding diagnostic capacity outside national reference laboratories will be essential for improving early detection and response to infectious disease outbreaks. Addressing these challenges requires sustained investments in laboratory infrastructure, workforce capacity, supply chain systems, and integrated surveillance platforms. Importantly, the current body of literature highlights the need for more systematic analysis of how diagnostic capacity influences outbreak detection and response performance across different levels of the health system. By examining these relationships, the present study contributes to the growing evidence base on strengthening diagnostic systems as a core component of national health security and outbreak preparedness.
Categorization of multisectoral partners
The categorization of multisectoral partners (Table 3) highlights their indispensable role in bridging critical gaps during Nigeria’s infectious disease outbreak responses. International agencies provided essential technical, diagnostic, logistical, and financial support, particularly during high-consequence events such as Ebola, Lassa fever, and COVID-19. Local civil society actors, including traditional and religious leaders, were pivotal in building community trust, facilitating contact tracing, and countering misinformation. The private sector contributed targeted logistical and communication resources (notably during COVID-19), while academic and research institutions supported operational research, data analysis, and technical input into EOCs and after-action reviews. This diverse ecosystem of partners has consistently compensated for systemic limitations in funding, subnational capacity, and community engagement; however, the heavy reliance on external and variable support underscores the need for greater domestic institutionalization of these functions to ensure sustainable and independent outbreak response capacity.
Containment and case management
For high-consequence diseases like Ebola and Lassa fever, the cornerstone of the response was rapid case detection, isolation, and contact tracing. During the 2014 Ebola outbreak, contact tracing of 894 contacts was initiated within 24–48 hours of case confirmation, which was instrumental in containing the outbreak within 93 days [18, 19, 24]. Similarly, for Lassa fever, early isolation in dedicated treatment centers was documented to reduce secondary transmission [4]. For vaccine-preventable diseases, mass immunization campaigns were a pivotal response. A targeted measles vaccination campaign in Lagos during a 2011 outbreak achieved over 80% coverage in high-risk areas [25], while reactive oral cholera vaccination in 2018 contributed to the decline of an outbreak in northern states [6].
Infection Prevention and Control (IPC) and Non-Pharmaceutical Interventions (NPIs) The COVID-19 response heavily relied on IPC and NPIs. Studies reported high adherence to hand hygiene and PPE use among healthcare workers in several states, despite resource constraints [26].
Coordination through EOCs: The effectiveness of Nigeria’s response was heavily dependent on the timeliness and efficiency of its coordination and surveillance systems, with notable disparities between federal and subnational levels. The activation of national and state-level Emergency Operations Centers (EOCs) during Ebola, Lassa fever, and COVID-19 served as a critical strength, creating hubs for real-time decision-making and inter-agency collaboration [9, 27].
Surveillance Systems: The Integrated Disease Surveillance and Response (IDSR) framework provided the backbone for routine outbreak reporting for diseases like cholera and diphtheria [12, 17]. Digital innovations, particularly the Surveillance Outbreak Response Management and Analysis System (SORMAS), significantly enhanced effectiveness; its use during COVID-19 reduced case reporting time by 48 hours in pilot areas compared to traditional systems [12].
Laboratory and diagnostic capacity
Laboratory diagnostics form the cornerstone of early detection, case confirmation, and surveillance-informed response in Nigeria’s outbreak management. During the 2014 Ebola outbreak, rapid establishment of diagnostic capacity (including mobile labs and international support for PCR confirmation) enabled timely case identification and contributed significantly to containment within 93 days, as highlighted in Ebola-focused studies [28]. For Lassa fever, expansion of molecular testing sites (e.g., National Reference Laboratory in Abuja and zonal facilities) during high-burden seasons reduced turnaround times and supported early isolation, though persistent delays in sample transport from remote areas contributed to higher case fatality rates in some cohorts [4].
The COVID-19 pandemic exposed critical limitations in initial testing scale and geographic coverage, with restricted PCR capacity leading to under-detection and delayed confirmation in subnational settings [5]. Innovations such as decentralizing testing to zonal reference laboratories and leveraging platforms like GeneXpert (originally for TB) helped scale response, but bottlenecks in reagent supply, trained personnel, and integration with digital tools (e.g., SORMAS) persisted [multiple sources]. For cholera and diphtheria, laboratory confirmation remains essential for distinguishing outbreaks from routine cases and guiding WASH-targeted interventions, yet fragile sample referral networks and limited subnational lab infrastructure often delay confirmation by days to weeks [23].
While national-level advancements (e.g., National Reference Laboratory enhancements and sequencing for variant tracking) represent key strengths, uneven subnational diagnostic access, supply chain fragility, and workforce shortages undermine early warning and containment, particularly in rural/high-burden states. Strengthening decentralized lab networks, point-of-care diagnostics, and sustainable training/integration with surveillance systems emerges as a critical lesson for resilient preparedness.
Documented Inefficiencies: Despite these tools, significant challenges in subnational coordination directly undermined efficiency. Analyses of cholera and Lassa fever responses revealed that delays in information flow and resource mobilization between federal and state EOCs averaged 5-7 days, directly impacting outbreak containment [4,7]. The evidence reveals a stark contrast between sophisticated communication efforts and persistent challenges in community trust, which directly impacted response outcomes.
Communication strategies and positive impact: The NCDC employed multi-channel risk communication during COVID-19, including daily briefings, radio jingles, and social media, which improved compliance with NPIs in urban centers [20,21]. Partnerships with community and faith-based leaders were effective in countering misinformation during both the Ebola and COVID-19 responses [2, 27]. Documented Impact Gaps: However, these efforts often failed to overcome deep-seated mistrust. Refusal rates for contact tracing and vaccination reached 15-20% in some regions for Lassa fever and COVID-19 [14]. This low trust was identified as a key factor in the delayed presentation of Lassa fever cases, which contributed to case fatality rates (CFR) as high as 23% in one cohort, exceeding the national average [10]. A survey of healthcare workers highlighted that 68% faced PPE shortages, yet targeted IPC training was shown to increase adherence from 42% to 84% within six months, indicating that resource allocation coupled with training can yield significant improvements even in challenging contexts [14].
The review identified a diverse ecosystem of partners who played indispensable roles in filling critical resource, logistical, and trust gaps. Their contributions are categorized in Table 2. International Agencies: Organizations like the World Health Organization (WHO), U.S. CDC, and Médecins Sans Frontières (MSF) provided essential technical expertise, diagnostic capacity, and specialized training, particularly during the acute phases of the Ebola and Lassa fever outbreaks [1, 18].
Local Civil Society: The role of traditional and religious leaders was frequently documented as a critical success factor. They acted as trusted intermediaries, facilitating contact tracing, ensuring safe burial practices during Ebola, and improving community acceptance of public health measures [2]. Private Sector: Contributions from the private sector addressed specific logistical needs. Telecommunication companies facilitated mass SMS alerts for public health messaging, while pharmaceutical firms donated personal protective equipment during the COVID-19 pandemic [20]. Collaborative Learning Mechanisms: After-action reviews (AARs), often conducted with international partners, were highlighted as a best practice for institutional learning, systematically documenting lessons from urban outbreaks to inform future preparedness [13].
This systematic review compiled evidence from 12 studies to evaluate Nigeria’s public health responses to infectious disease outbreaks from 2010 to 2023. The results, structured around four principal objectives, demonstrate a public health system that has developed considerable technical capacity at the national level. However, its overall effectiveness is persistently impeded by operational limitations at the subnational level, fragile community trust, and reliance on a diverse array of external partners.
Synthesis of Public Health Response Strategies
Our first objective was to describe the core public health strategies deployed in Nigeria. The reviewed studies demonstrate an evolution in the country’s strategic toolkit. The foundational importance of rapid case detection, isolation, and contact tracing was overwhelmingly demonstrated during the 2014 Ebola outbreak, where their rigorous execution, as documented by Shuaib et al. [18] and the Nigerian Centers for Disease Control and Prevention [8], was the cornerstone of successful containment. This approach was successfully adapted for other high-consequence diseases, with Otu et al. [19] noting its role in managing Lassa fever. For vaccine-preventable diseases, the pivotal role of mass immunization was evident in the work of Adeoye et al. [10], who reported over 80% coverage in a targeted measles campaign, and Elimian et al. [6], who highlighted the impact of reactive oral cholera vaccination. However, the sustainability of more complex measures was often challenged. Studies on the COVID-19 response, particularly Orji et al. [14] and Olumade and Uzairue [13], revealed that while infection prevention and control (IPC) and non-pharmaceutical interventions (NPIs) were initially enforced, their long-term efficacy was compromised by PPE shortages, “pandemic fatigue,” and socio-economic pressures, indicating a strategic vulnerability to prolonged crises.
The Efficiency Gap in Coordination and Surveillance
The review’s second objective focused on the efficiency of coordination and surveillance. Our synthesis confirms that institutional coordination has been transformative. The activation of Emergency Operations Centers (EOCs), a key factor in the Ebola response per the Centers for Disease Control and Prevention [2], has become a standard practice. Digital innovation, specifically the Surveillance Outbreak Response Management and Analysis System (SORMAS), was highlighted by Silenou et al. [29] and Ozakpo et al. [30] for significantly enhancing data timeliness. Yet the most critical finding is the persistent efficiency gap between federal and subnational levels. This was quantitatively exposed in the work of Atanda et al. [22], whose analysis of after-action reviews (AARs) identified consistent 5 to 7 day delays in intergovernmental coordination and resource mobilization. This evidence indicates that technological and strategic advancements at the center are necessary but insufficient; they are critically undermined without parallel investments in subnational administrative and logistical capacity. This subnational efficiency gap extends to laboratory systems, where centralized NRL excellence contrasts with delayed sample transport and confirmation at state/peripheral levels.
The Central Role of Trust in Community Engagement
Evaluating the impact of risk communication and community engagement (RCCE), our third objective, revealed a stark dichotomy. While studies like Jacobs and Okeke [21] acknowledged the Nigeria Centre for Disease Control’s (NCDC) sophisticated multi-channel communication strategies during COVID-19, multiple studies reported that these efforts failed to overcome deep-seated mistrust Ernest-Samuel et al. [31] documented contact tracing refusal rates of 15-20% for Lassa fever and COVID-19, while Orji et al. [14] directly linked community hesitancy and resource limitations to increased nosocomial transmission risk. This trust deficit had direct clinical consequences; for instance, Duvignaud et al. [3], in their Lassa fever cohort study, linked delayed patient presentation to higher case fatality. The critical lesson, supported by the successful involvement of community leaders during the Ebola response as per Moon et al. [9], is that technical communication is not synonymous with meaningful engagement. The evidence compels a strategic shift toward long-term, trust-based partnerships with local communities.
Multisectoral Partnerships as an Indispensable Scaffold
Finally, our categorization of multisectoral partnerships illustrates that Nigeria’s outbreak response is underpinned by a complex ecosystem of support. International agencies like the World Health Organization (WHO) and the U.S. CDC were consistently cited (e.g., Centers for Disease Control and Prevention [8]; for providing indispensable technical expertise and diagnostic capacity. The irreplaceable role of local civil society in building trust and facilitating community entry was a key finding in studies of the Ebola response [1]. Furthermore, the private sector’s contribution, such as telecom companies enabling mass messaging, was noted by Orji et al. [14] during COVID-19. However, this collaborative model also reveals a systemic vulnerability. The heavy reliance on partners for essential functions, underscored by the routine use of AARs with international partners [20], suggests the core health system lacks sustainable, independent capacity for major outbreaks. Therefore, for long-term health security, policy must focus on internalizing these capabilities through sustained domestic investment.
Study limitations
This review is subject to several limitations. First, the restriction to peer‑reviewed English publications between 2010 and 2023 may have excluded valuable insights from grey literature, internal reports, and field evaluations. For example, post‑2023 developments such as the expansion of zonal public health laboratories and other infrastructural upgrades are not fully captured, even though they represent critical advances in Nigeria’s outbreak preparedness. By focusing only on peer‑reviewed sources, the review may under‑represent operational lessons documented in unpublished NCDC reports, donor evaluations, or state‑level assessments.
Second, the exclusion of studies published in local languages may have limited the diversity of perspectives, particularly those reflecting community-level experiences and indigenous knowledge systems. Third, the reliance on published literature introduces a publication bias, as studies with positive outcomes are more likely to be disseminated, while failures or operational challenges may remain undocumented. The absence of quantitative meta‑analysis means that findings are synthesized qualitatively, which, while rich in context, limits the ability to generalize effect sizes across interventions.
In conclusion, this systematic review demonstrates that Nigeria has made significant progress in developing national-level outbreak response mechanisms, including rapid case detection, contact tracing, EOC coordination, digital surveillance tools (e.g., SORMAS), and multisectoral partnerships. However, persistent subnational operational delays (averaging 5–7 days), low community trust (leading to 15–20% refusal rates for key interventions), uneven diagnostic access, and heavy dependence on variable external support continue to compromise timely containment and mortality reduction across outbreaks such as Ebola, Lassa fever, cholera, COVID-19, measles, and diphtheria.
To build a more resilient national health security architecture, Nigeria should prioritize the following strategic actions:
Recommendation
To operationalize the above policy priorities, the following actionable recommendations are proposed:
What is already known about the topic
What this study adds
AA was responsible for the conceptualization, methodology, and data curation, and contributed to writing through review and editing.
CK participated in data curation and drafted the original manuscript.
NAF contributed to data curation and performed the formal analysis. All authors read and approved the final manuscript.
Data availability statement
All data underlying the findings of this study are available in the published literature cited in this review.
| Database | Initial hits | After duplicates removed | Relevant articles (title/abstract screening) | Final included |
|---|---|---|---|---|
| PubMed | 12 | 12 | 4 | 2 |
| Google Scholar | 23 | 21 | 8 | 3 |
| Web of Science | 10 | 10 | 6 | 3 |
| NIH | 8 | 6 | 3 | 2 |
| AJOL | 7 | 6 | 2 | 2 |
| Total | 52 | 49 | 23 | 12 |
| Author (Year) | Study Design | MMAT Category | Criteria Met (out of 5) | Rating (%) | Quality Level |
|---|---|---|---|---|---|
| Saleh et al. (2022) | Cross-sectional | Quantitative descriptive | 4/5 | 80% | Moderate–High |
| Olumade et al. (2022) | Case study | Mixed Methods | 5/5 | 100% | High |
| Otu et al. (2017) | Mixed-methods | Mixed Methods | 5/5 | 100% | High |
| Wolicki et al. (2016) | Case study | Quantitative descriptive | 4/5 | 80% | Moderate–High |
| Jacobs & Okeke (2022) | Systematic review | Not Applicable | N/A | N/A | Included for synthesis only |
| Olumade et al. (2020b) | Prospective cohort | Quantitative non-random | 3/5 | 60% | Moderate |
| Elimian et al. (2019) | Retrospective analysis | Quantitative descriptive | 5/5 | 100% | High |
| Atanda et al. (2021) | Case-control | Quantitative non-random | 4/5 | 80% | Moderate–High |
| Orji et al. (2023) | Cross-sectional | Quantitative descriptive | 5/5 | 100% | High |
| CDC (2014) | Qualitative | Qualitative research | 4/5 | 80% | Moderate–High |
| Adeoye et al. (2013) | Case study | Quantitative descriptive | 3/5 | 60% | Moderate |
| Okeke et al. (2022) | Retrospective | Quantitative descriptive | 4/5 | 80% | Moderate–High |
| Partner Category | Specific Actors | Reported Contributions | Outbreaks Where Documented |
|---|---|---|---|
| International Agencies | WHO, U.S. CDC, MSF, UNICEF, Africa CDC, Resolve to Save Lives, UKHSA (and their implementing/field partners) | Technical expertise; deployment of personnel; diagnostic support; funding; logistical support; direct implementation of surveillance, case management, and training | Ebola, Lassa Fever, COVID-19, Cholera, Diphtheria |
| Local Civil Society | Traditional Rulers, religious leaders, community-based organizations, local NGOs/implementing partners (e.g., local CSOs funded by UNICEF/WHO/MSF, community health volunteers) | Mobilizing community trust & participation; facilitating contact tracing; countering misinformation; promoting safe practices; field-level implementation of risk communication, vaccination, and WASH activities | Ebola, Lassa Fever, COVID-19, Cholera, Measles |
| Private Sector | Telecom Companies, Domestic Pharmaceutical Firms, Banks | Mass SMS/public health messaging, donation of PPE/medical supplies, financial donations/logistical support | COVID-19 |
| Academic/Research Institutions | Nigerian Universities, International Research Collaboratives | Operational research; data analysis; technical support as part of EOC teams and AARs | Multiple Outbreaks |