Research | Open Access | Volume 9 (2): Article 80 | Published: 21 May 2026

Views: 1,002
Menu, Tables and Figures
| Socio-demographic characteristics | Frequency (N=424) | Percent (%) |
|---|---|---|
| Age (years) | ||
| 18–30 | 14 | 3.3 |
| 31–45 | 102 | 24.1 |
| >45 | 308 | 72.6 |
| Gender | ||
| Female | 308 | 72.6 |
| Male | 116 | 27.4 |
| Marital Status | ||
| Married | 335 | 79.0 |
| Non married | 89 | 21.0 |
| Residence | ||
| Rural | 227 | 53.5 |
| Urban | 197 | 46.5 |
| Schooling status | ||
| Not schooled | 310 | 73.1 |
| Schooled* | 114 | 26.9 |
| Employment | ||
| Employed | 186 | 43.9 |
| Unemployed | 238 | 56.1 |
| Socio-economic Status | ||
| Above the poverty line | 96 | 22.6 |
| Below the poverty line | 328 | 77.4 |
| Family history of type 2 diabetes | ||
| No | 322 | 75.9 |
| Yes | 102 | 24.1 |
| Duration of diabetes (years) | ||
| 1-5 | 339 | 80.0 |
| 6-10 | 53 | 12.5 |
| 10+ | 32 | 7.5 |
| * Can read and write | ||
Table 1: Socio-demographic characteristics of patients suffering from type 2 Diabetes in Assaba, Mauritania, 2022
| Variables | Knowledge of type 2 DM Complications | cOR [95%CI] | P-value | |
|---|---|---|---|---|
| Inadequate n (%) | Adequate n (%) | |||
| Age (years) | ||||
| 18-30 | 6 (2.01) | 8 (6.35) | 1 | — |
| 31-45 | 77 (25.84) | 25 (19.84) | 4.1 [1.30 — 12.98] | 0.018 |
| >45 | 215 (72.15) | 93 (73.81) | 3.1 [1.04 — 9.13] | 0.04 |
| Gender | ||||
| Female | 226 (75.84) | 82 (65.08) | 1 | — |
| Male | 72 (24.16) | 44 (32.92) | 1.7 [1.07 — 2.65] | 0.02 |
| Marital status | ||||
| Not married | 76 (25.5) | 13 (10.32) | 1 | — |
| Married | 222 (74.5) | 113 (89.68) | 0.34 [0.18 — 0.63] | <0.001 |
| Residence | ||||
| Urban | 113 (37.92) | 84 (66.67) | 1 | — |
| Rural | 185 (62.08) | 42 (33.33) | 3.3 [2.11 — 5.07] | <0.001 |
| Schooling status | ||||
| Schooled* | 47 (15.77) | 67 (53.17) | 1 | — |
| Not schooled | 251 (84.23) | 59 (46.83) | 6.06 [3.8 — 9.7] | <0.001 |
| Employment | ||||
| Employed | 98 (32.89) | 88 (69.84) | 1 | — |
| Unemployed | 200 (67.11) | 38 (30.16) | 4.73 [3.01 — 7.42] | <0.001 |
| Socio-economic status | ||||
| Above the poverty line | 45 (15.1) | 51 (40.48) | 1 | — |
| Below the poverty line | 253 (84.9) | 75 (59.52) | 3.83 [2.4 — 6.16] | <0.001 |
| Family history of type 2 diabetes | ||||
| Yes | 35 (11.74) | 67 (53.17) | 1 | — |
| No | 263 (88.26) | 59 (46.83) | 8.53 [5.2 — 14.02] | <0.001 |
| Duration of diabetes (years) | ||||
| >10 | 6 (2.01) | 26 (20.63) | 1 | — |
| 1-5 | 279 (93.62) | 60 (47.62) | 20.15 [7.95 — 51.09] | <0.001 |
| 6-10 | 13 (4.36) | 40 (31.75) | 1.4 [0.48 — 4.17] | 0.4 |
| COR: crude odds ratio; CI: 95% confidence interval; n: frequency. *Can read and write Odds ratios (OR) were calculated considering inadequate knowledge as the outcome variable. | ||||
Table 2: Factors associated with inadequate knowledge of chronic complications of type 2 diabetes: Univariate logistic regression analysis
| Variables | aOR (95%CI) | P-value |
|---|---|---|
| Marital status | ||
| Not married | 1 | |
| Married | 0.26 [0.11 — 0.6] | 0.001 |
| Residence | ||
| Urban | 1 | |
| Rural | 2.13 [1.2 — 3.8] | 0.009 |
| Schooling status | ||
| Schooled* | 1 | |
| Unschooled | 2.3 [1.24 — 4.2] | 0.008 |
| Employment | ||
| Unemployed | 1 | |
| Employed | 2.41 [1.34 — 4.32] | 0.003 |
| Family history of type 2 diabetes | ||
| Yes | 1 | |
| No | 2.37 [1.21 — 4.6] | 0.011 |
| Duration of diabetes (years) | ||
| >10 | 1 | |
| 1-5 | 9.33 [2.98 — 29.23] | <0.001 |
| 6-10 | 0.82 [0.23 — 2.91] | 0.41 |
| AOR: adjusted odds ratio; CI: 95% confidence interval. *Can read and write | ||
Table 3: Factors associated with inadequate knowledge of type 2 chronic complications: Multivariate logistic regression
Boushab Mohamed Boushab1,2,&, Pauline Kiswendsida Yanogo2, Oumar Sangho3, Ismaël Diallo4, Nicaise Lépri Aka5, Nicolas Meda2
1Division of Internal Medicine and Infectious Diseases, Hospital of Kiffa, Assaba, Mauritania, 2Burkina Field Epidemiology and Laboratory Training Program; Joseph KI-ZERBO University, 3Department of Biological and Medical Sciences, Faculty of Pharmacy (FAPH), USTTB, Bamako, Mali, 4Department of Medicine and Medical Specialities, Faculty/School of Health Sciences, Joseph Ki-Zerbo University, Ouagadougou – Burkina Faso, 5Ministry of Health, Public Hygiene and Universal Health Coverage, Abidjan, Côte d’Ivoire
&Corresponding author: Boushab Mohamed Boushab, Division of Internal Medicine and Infectious Diseases, Hospital of Kiffa, Assaba, Mauritania, Email: bboushab@gmail.com ORCID: https://orcid.org/0000-0001-8932-1027
Received: 30 Apr 2025, Accepted: 03 May 2026, Published: 21 May 2026
Domain: Non-Communicable Disease Epidemiology
Keywords: Knowledge, chronic complications, Type 2 Diabetes, Assaba, Mauritania
©Boushab Mohamed Boushab et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Boushab Mohamed Boushab et al. Factors associated with knowledge of chronic complications of type 2 diabetes in Assaba, Mauritania, 2022. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):80. https://doi.org/10.37432/jieph-d-25-00107
Introduction: Knowledge of chronic complications of type 2 diabetes mellitus (T2DM) is essential for prevention, yet data remain limited in Mauritania. This study identified factors associated with inadequate knowledge of chronic complications of T2DM among patients in the Assaba region.
Methods: A hospital-based cross-sectional analytic study was conducted among 424 patients with T2DM attending Kiffa Hospital between March and December 2022. Knowledge of chronic complications was assessed using a structured questionnaire and categorised as adequate or inadequate. Logistic regression analyses were performed to identify factors associated with inadequate knowledge. Adjusted odds ratios (aORs) with 95% confidence intervals (95% CI) were calculated. Statistical significance was set at p < 0.05.
Results: A total of 424 participants were included in the study. A majority of participants (70.3%, n=298/424; 95% CI: 65.9–74.6%) demonstrated inadequate knowledge of chronic complications of T2DM. Being married (aOR = 0.26; 95%CI: 0.11–0.59), residing in rural area (aOR = 2.13; 95%CI: 1.21–3.77), being unable to read or write (unschooled) (aOR = 2.29; 95%CI: 1.24–4.22), employed (aOR = 2.41; 95%CI: 1.34–4.32), having no previous family history of diabetes (aOR = 2.37; 95%CI: 1.22–4.62), and living with diabetes for 1-5 years (aOR = 9.33; 95%CI: 2.98–29.23) were significantly associated with inadequate knowledge of chronic complications of type 2 diabetes.
Conclusion: Inadequate knowledge of chronic complications of T2DM was highly prevalent among patients in the Assaba region. Targeted educational interventions focusing on vulnerable groups are urgently needed to improve awareness and reduce complications.
Diabetes mellitus is a major public health concern all over the world [1]. According to the International Diabetes Federation (IDF), 463 million people are suffering from the disease, and 374 million have glucose intolerance (GI) or a prediabetic state. These numbers will reach 700 million of diabetic people with diabetes and 548 million suffering from glucose intolerance by the year 2045, giving an increase rate of 51% as compared to 2019 [2]. Among the regions of the IDF, the Pacific West has the greatest number of people living with diabetes (163 million), followed by Southeast Asia (88 million), Europe (59 million), the Middle East and North Africa (55 million), and North America and the Caribbean (47.6 million) [2].
The prevalence of diabetes is not uniform in the different countries due to social, economic, and genetic disparities [3–5]. The circumstances of disease diagnosis vary according to the level of diagnostic and treatment capacity available and the degree of interest the population shows in healthcare issues [6].
According to recent reports from the Ministry of Health of Mauritania, the prevalence of diabetes is estimated between 6 and 8% among adults, with a notable increase in urban areas. Studies conducted in southern Mauritania have shown a rising prevalence of type 2 diabetes, especially among individuals over 40 years old. The Assaba region, including Kiffa, is experiencing a gradual increase in non-communicable diseases, including diabetes, but local epidemiological data remain scarce, which justifies the conduct of this study.
Those who are affected by the disease are also at risk of developing other health conditions [2,7,8], which could be lethal, namely micro and macrovascular complications such as cardiovascular diseases, retinopathy, end-stage kidney disease, and neuropathy [4,9]. Diabetes is a severe disease in the long term and has a major impact on one’s life, and the well-being of individuals, families and communities worldwide [10,11].
Knowledge of diabetes complications is important for recognising early signs and symptoms, which are required for implementing appropriate preventive interventions aimed at slowing the onset of complications [12]. To our knowledge, there is no study on the knowledge of chronic diabetes complications in Mauritania. These data are important for political leaders and health professionals to develop and implement appropriate strategies to control and prevent the disease’s consequences. These strategies aim at reaching and maintaining personalised glycemic targets, reaching management targets on lipids and weight, slowing and preventing cardiovascular risk factors for all people living with Diabetes and in a prediabetic state [13]. This study identified the factors that influence the knowledge of diabetes chronic complications among people who live with type 2 DM in the region of Assaba in Eastern Mauritania.
Study settings and period
We conducted a cross-sectional analytic study among patients living with type 2 Diabetes from March 1st to October 31st 2022, in the Kiffa Hospital in the southeast of Mauritania. The hospital is located in the city of Kiffa, which is a central town for the Assaba region and is 600 km south-east of Nouakchott.
Study population and inclusion criteria
All patients living with type 2 diabetes followed up at Kiffa Hospital and attended for a medical visit during the data collection period constituted our study population. Although Kiffa is urban, most patients come from rural areas. We included in our study all patients living with type 2 diabetes who were taking treatment and aged ≥18 years. All patients living with type 2 diabetes who were severely ill, and all health professionals, were excluded from the study.
Sample size and sampling process
The determination of the sample size was based on the hypothesis that the disease prevalence in the population was set at 50% with a precision of 5% and a level of confidence at 95%. This sample is increased by 10% in order to take into account the non-response.
Formula for determining the sample size (Schwartz formula):
\[
\mathbf{n} = z^2 \times p(1-p) \;/\; m^2
\]
n = sample size
z = test of low standard deviation according to the low-centred normal law (for a level of confidence at 95% and a margin of error at 5%, z = 1.96)
p =estimated population size that has the feature (when unknown, we use p=0.5, which is the highest sample size)
m = desired precision.
n = (1.96) ² x (0.5) (1-0.5) / (0.05) ² = 384.16 ≈ 385.
A non-response rate of 10% was determined, and the size was increased by 38.4 ≈ 39. Consequently, the sample size was set at 424 participants.
Study variables and operational definitions
The dependent variable was the knowledge of diabetes complications. The independent variables were age, gender, marital status, residence, schooling status, employment status, socio-economic status, family history of diabetes and the time span since the diagnosis of diabetes.
Complications of diabetes mellitus: knowledge of one or several of the following diabetes complications: retinopathy, diabetic foot, kidney complications, stroke, heart complications, neuropathy, hypertension, tooth decay and erectile dysfunction.
Marital status: this variable was dichotomised into two groups: “married” and “not married”, meaning those who are single, widowed, or separated.
Schooling status: the participants were classified as “does not read or write” and “can read and write” (Koranic school, elementary school, secondary school and beyond). The essential point was to know whether they could read and write in order to fully grasp the beneficial results of reading and writing on their knowledge of type 2 diabetes. When the participants had been through elementary school but could not read and write, they were classified in the category “not capable of reading and writing”. In Mauritania, several people go through non-formal or religious education programs, but not through elementary school and can read and write. In such a situation, we gathered these participants in the category “know how to read and write (schooled)”.
Employment status: diabetic patients were gathered in two groups: (those who work, “employed ” or those who do not work, “unemployed “.
Socio-economic standards: This variable uses the score of Evaluation of Precariousness and Health Inequalities in Health Examination Centers (EPICES). These variables include the traditional socio-economic determinants such as education, income, and profession, but also features related to family structure and housing, social advantages and leisure activities. Each question has a coefficient of regression; the score varies from 0 (no precarity) to 100 (maximum precarity). For each patient, we calculated the EPICES score (validated as precarity score) and ran a questionnaire on the knowledge of diabetes. Participants were labelled as ” below the poverty line ” and ” above the poverty line ” according to the median EPICES score of this population (at 36.7) [14].
Rural residence: people who live in the suburbs, outside of big towns, are called “rural residents”.
Family history of diabetes: having at least one first-degree relative who suffers from diabetes.
Good knowledge: knowledge score greater than or equal to the average. The participants were questioned on the chronic complications of type 2 diabetes that they were aware of. Each question had one correct answer among three suggested answers. The possible answer choices for each question were “Yes”, “No” and “I don’t know”. The option ” I don’t know” was added to minimise the explanations. We had assumed that the different questions were equal in value and that the responses were exclusive from one to another. Each correct answer scores “1” and “0” for each incorrect answer or “I don’t know”. The individual knowledge score was calculated and summed up to generate an overall knowledge score. The participants who had correctly responded to > 50% of the questions on knowledge were considered as having adequate knowledge, while those who had a score < 50% were considered as having inadequate knowledge.
Data collection tools and procedure
The participants were contacted during the two days of outward checkup visits in Medicine (Diabetes medical visits) to collect data. Before responding, simple explanations were given on the procedure and an example of the response choice. The participants who could not read or write were helped by assistants who translated the questions into their mother tongues. The assistants had been trained on how to translate questions in order to guarantee the uniformity of each encounter. We conducted a face-to-face interview. The study questionnaire was adapted from questionnaires used in other studies [15–26]. The team for data collection was made up of three nurses who were trained and supervised by the investigating doctor. The objectives and the procedures of the study were explained to participants in Arabic, French, and the local dialect in order to guarantee the validity of the collection tools. From the questionnaire, data were typed into a database using the Excel® 2021 software. The questionnaire was tested in 5% of our sample outside of the study site in order to verify its content and clarity. The modification of the questionnaire with the intent of improving its quality was made prior to the main data collection. The questionnaire was administered in a face-to-face interview with participants.
Data management and analysis
Data were verified daily in order to make sure that they were complete and coherent. Wrong data were identified and corrected through the available data sources. The variables were coded in order to facilitate analysis. Data were secured and anonymised to ensure confidentiality. Data analysis was made by using the SAS® version 9.4 software. Descriptive statistics were performed and presented through tables of frequency for qualitative variables and the mean± standard deviation for quantitative variables. A simple logistic regression was conducted to generate crude odds ratios for each variable with a confidence interval at 95% and a p-value. Thereafter, variables associated with the dependent variable at a p-value < 0.2 in the simple logistic regression were included in the multiple logistic regression model. A significance threshold of p < 0.05 was applied in all multivariate analyses. The goodness-of-fit of the final multivariable logistic regression model was assessed using the Hosmer-Lemeshow test.
Ethical considerations
The study was approved by the ethics committee and the scientific committee of the Kiffa hospital through a written notice in February 2023 with the reference number (No. CS CHK/02/2023. Written informed consent was obtained from each participant before data collection.
A total of 424 participants responded, giving a participation rate of 100%. The mean age for participants of our population was 54.4 ± 12.6 years. The average duration of type 2 diabetes was 4.02 ± 3.03 years, ranging from 1 to 17 years, and the female: male ratio was 2.56. The majority of participants were older than 45 years (72.6%). More than half (79%) were married, and 53.5% were living in rural areas (53.5%). Approximately 73.1% had not been through formal schooling. Most participants (56.13%) were unemployed, and 77.7% were living below the poverty line. Also, 24.1% of participants had a family history of type 2 diabetes. The participants who had lived with the disease for one to five years represented 80% of cases (Table 1).
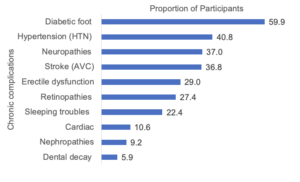
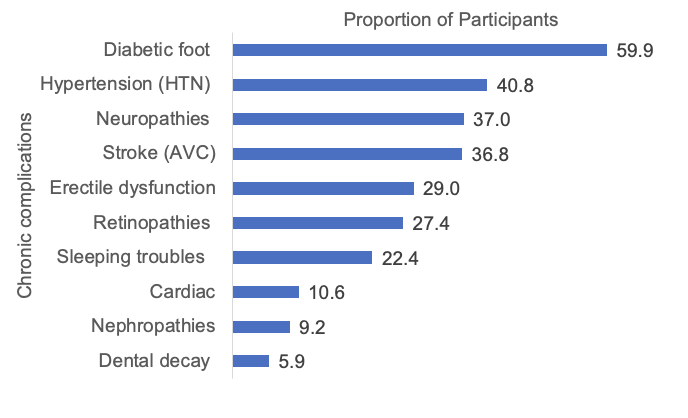
The commonly known complications among participants were diabetic foot (59.9%), hypertension (40.8%), neuropathy (37.0%) and stroke (36.8%) (Figure 1). Overall, a total of 298 participants (70.3%, 95%CI: 65.9–74.6%) had inadequate knowledge of type 2 diabetes chronic complications.
Factors Associated with Knowledge of Chronic Complications
The age, gender, marital status, living area, education level, employment status, socio-economic standard, and family history of Type 2 diabetes were significantly associated with the knowledge of diabetes complications after a simple logistic regression analysis (Table 2). In multivariate logistic regression analysis, marital status, place of residence, schooling status, employment status, family history of diabetes, and duration of diabetes remained independently associated with inadequate knowledge (Table 3). Married participants were less likely to have inadequate knowledge, whereas rural residence, lack of formal education, unemployment, absence of family history of diabetes, and shorter duration of diabetes were significantly associated with higher odds of inadequate knowledge.
This study revealed that most type 2 diabetic patients at Kiffa Hospital had inadequate knowledge of chronic complications. Similar findings have been reported in Ghana [25], Saudi Arabia [27], and India [28], underscoring a broader public health challenge in resource-limited settings like Mauritania. Poor knowledge may lead to delayed recognition of complications and suboptimal disease management.
Schooling status was significantly associated with knowledge of complications. As reported in several studies [15,18,25,29,30], being able to read and write (schooling) facilitates access to health information and healthcare services. Likewise, urban residence was associated with better knowledge, possibly due to greater exposure to mass media, health campaigns, and healthcare infrastructure [17,25,31–33]. Marital status and family history of diabetes were also linked to better knowledge, suggesting that social environment and shared experiences can play a role in informal health education [22,23,34]. Similar associations were found in studies from Brazil [34] and Ethiopia [24,35], supporting the idea that involving relatives in patient education may enhance knowledge and self-care practices.
Longer duration of diabetes was associated with better knowledge, as observed in South Africa [36], Bangladesh [29] and Iran [37]. This could be due to greater cumulative exposure to healthcare providers and educational messages over time. However, in Mauritania, access to healthcare—especially in rural areas—is limited. This may explain why some long-term patients still demonstrated poor understanding of complications.
Unlike studies in Ghana [25] and India [38] that reported better knowledge among men, our study found that women had lower knowledge scores. This aligns with findings from Iran [29] and Ethiopia [35] and may reflect greater health-seeking behaviour among women in our context. Gender disparities in knowledge seem to be context-specific and highlight the need for gender-sensitive health education strategies.
These findings highlight the urgent need to strengthen patient education in Mauritania. Efforts should prioritise rural populations, those with low literacy levels, and individuals with limited access to care. Community-based awareness programs involving families, delivered through locally accessible media (e.g., radio, local languages), could help bridge knowledge gaps. Training community health workers may also enhance outreach in underserved areas.
Study limitations
This study was conducted at a single hospital, which may limit the generalizability of the findings. Additionally, self-reported data may be subject to social desirability bias. Nevertheless, this study provides a foundational understanding of knowledge gaps that can inform future educational interventions.
The overall results of our study indicate that participants had limited knowledge regarding the chronic complications of type 2 diabetes. Addressing this gap requires a multisectoral approach involving not only healthcare authorities in Mauritania but also sectors such as education and local communities. Such collaboration is essential to develop diabetes education programs tailored to the local context, to promote self-care behaviours and prevent diabetes and its complications. Healthcare providers should play a central role in reinforcing patient education on diabetes, its treatment, and its potential complications. This can be achieved through the use of educational resources that are both linguistically and culturally appropriate, thereby improving patient knowledge and empowering individuals to better manage their condition.
What is already known about the topic
What this study adds
The authors would like to express their sincere gratitude to all the patients who participated in this study. We also thank the medical and paramedical staff of the Department of Internal Medicine and Infectious Diseases at Kiffa Hospital for their invaluable support in data collection and patient management.
Writing – original draft: Boushab Mohamed Boushab.
Writing – review and editing: Boushab Mohamed Boushab, Pauline Kiswendsida Yanogo, Oumar Sangho, Ismaël Diallo, Nicaise Lépri Aka, Nicolas Meda.
Conceptualization: Boushab Mohamed Boushab, Pauline Kiswendsida Yanogo, Oumar Sangho.
Data curation: Boushab Mohamed Boushab, Pauline Kiswendsida Yanogo, Oumar Sangho.
Formal analysis: Boushab Mohamed Boushab, Oumar Sangho, Ismaël Diallo, Nicaise Lépri Aka, Nicolas Meda.
Investigation: Boushab Mohamed Boushab.
Methodology: Boushab Mohamed Boushab, Pauline Kiswendsida Yanogo, Oumar Sangho, Nicolas Meda.
Project administration: Boushab Mohamed Boushab, Pauline Kiswendsida Yanogo.
Resources: Boushab Mohamed Boushab, Pauline Kiswendsida Yanogo, Nicolas Meda.
Software: Boushab Mohamed Boushab.
Supervision: Boushab Mohamed Boushab, Oumar Sangho, Ismaël Diallo.
Validation: Boushab Mohamed Boushab, Pauline Kiswendsida Yanogo, Oumar Sangho, Ismaël Diallo, Nicaise Lépri Aka, Nicolas Meda.
Visualization: Boushab Mohamed Boushab, Pauline Kiswendsida Yanogo, Oumar Sangho, Ismaël Diallo, Nicaise Lépri Aka, Nicolas Meda.
| Socio-demographic characteristics | Frequency (N=424) | Percent (%) |
|---|---|---|
| Age (years) | ||
| 18–30 | 14 | 3.3 |
| 31–45 | 102 | 24.1 |
| >45 | 308 | 72.6 |
| Gender | ||
| Female | 308 | 72.6 |
| Male | 116 | 27.4 |
| Marital Status | ||
| Married | 335 | 79.0 |
| Non married | 89 | 21.0 |
| Residence | ||
| Rural | 227 | 53.5 |
| Urban | 197 | 46.5 |
| Schooling status | ||
| Not schooled | 310 | 73.1 |
| Schooled* | 114 | 26.9 |
| Employment | ||
| Employed | 186 | 43.9 |
| Unemployed | 238 | 56.1 |
| Socio-economic Status | ||
| Above the poverty line | 96 | 22.6 |
| Below the poverty line | 328 | 77.4 |
| Family history of type 2 diabetes | ||
| No | 322 | 75.9 |
| Yes | 102 | 24.1 |
| Duration of diabetes (years) | ||
| 1-5 | 339 | 80.0 |
| 6-10 | 53 | 12.5 |
| 10+ | 32 | 7.5 |
| * Can read and write | ||
| Variables | Knowledge of type 2 DM Complications | cOR [95%CI] | P-value | |
|---|---|---|---|---|
| Inadequate n (%) | Adequate n (%) | |||
| Age (years) | ||||
| 18-30 | 6 (2.01) | 8 (6.35) | 1 | — |
| 31-45 | 77 (25.84) | 25 (19.84) | 4.1 [1.30 — 12.98] | 0.018 |
| >45 | 215 (72.15) | 93 (73.81) | 3.1 [1.04 — 9.13] | 0.04 |
| Gender | ||||
| Female | 226 (75.84) | 82 (65.08) | 1 | — |
| Male | 72 (24.16) | 44 (32.92) | 1.7 [1.07 — 2.65] | 0.02 |
| Marital status | ||||
| Not married | 76 (25.5) | 13 (10.32) | 1 | — |
| Married | 222 (74.5) | 113 (89.68) | 0.34 [0.18 — 0.63] | <0.001 |
| Residence | ||||
| Urban | 113 (37.92) | 84 (66.67) | 1 | — |
| Rural | 185 (62.08) | 42 (33.33) | 3.3 [2.11 — 5.07] | <0.001 |
| Schooling status | ||||
| Schooled* | 47 (15.77) | 67 (53.17) | 1 | — |
| Not schooled | 251 (84.23) | 59 (46.83) | 6.06 [3.8 — 9.7] | <0.001 |
| Employment | ||||
| Employed | 98 (32.89) | 88 (69.84) | 1 | — |
| Unemployed | 200 (67.11) | 38 (30.16) | 4.73 [3.01 — 7.42] | <0.001 |
| Socio-economic status | ||||
| Above the poverty line | 45 (15.1) | 51 (40.48) | 1 | — |
| Below the poverty line | 253 (84.9) | 75 (59.52) | 3.83 [2.4 — 6.16] | <0.001 |
| Family history of type 2 diabetes | ||||
| Yes | 35 (11.74) | 67 (53.17) | 1 | — |
| No | 263 (88.26) | 59 (46.83) | 8.53 [5.2 — 14.02] | <0.001 |
| Duration of diabetes (years) | ||||
| >10 | 6 (2.01) | 26 (20.63) | 1 | — |
| 1-5 | 279 (93.62) | 60 (47.62) | 20.15 [7.95 — 51.09] | <0.001 |
| 6-10 | 13 (4.36) | 40 (31.75) | 1.4 [0.48 — 4.17] | 0.4 |
| COR: crude odds ratio; CI: 95% confidence interval; n: frequency. *Can read and write Odds ratios (OR) were calculated considering inadequate knowledge as the outcome variable. | ||||
| Variables | aOR (95%CI) | P-value |
|---|---|---|
| Marital status | ||
| Not married | 1 | |
| Married | 0.26 [0.11 — 0.6] | 0.001 |
| Residence | ||
| Urban | 1 | |
| Rural | 2.13 [1.2 — 3.8] | 0.009 |
| Schooling status | ||
| Schooled* | 1 | |
| Unschooled | 2.3 [1.24 — 4.2] | 0.008 |
| Employment | ||
| Unemployed | 1 | |
| Employed | 2.41 [1.34 — 4.32] | 0.003 |
| Family history of type 2 diabetes | ||
| Yes | 1 | |
| No | 2.37 [1.21 — 4.6] | 0.011 |
| Duration of diabetes (years) | ||
| >10 | 1 | |
| 1-5 | 9.33 [2.98 — 29.23] | <0.001 |
| 6-10 | 0.82 [0.23 — 2.91] | 0.41 |
| AOR: adjusted odds ratio; CI: 95% confidence interval. *Can read and write | ||