Review | Open Access | Volume 9 (2): Article 83 | Published: 22 May 2026

Views: 1,144
Menu, Tables and Figures
| First Author | Year | Study Design | Geographic Scope | Study Period | Sample Size | Key Outcomes | Main Findings |
|---|---|---|---|---|---|---|---|
| Butswat, S.B. | 2025 | Secondary analysis, Retrospective analysis of Surveillance data | State-specific (Plateau State) | Jan 2022 – Dec 2022 | Suspected: 118; Confirmed: 16 | Prevalence (Positivity): 13.6% Incidence: 2.6 per 100,000 CFR: 0% | Incidence rate: 2.6/100,000; CFR: 0%; Positivity: 13.6%; Geographic clustering: 62.5% of cases in Jos North; Age: 0-19 years most affected (51.7%); Sex ratio M:F 1.1:1; Seasonal peak: September; 25% asymptomatic. |
| Yinka-Ogunleye, A. | 2023 | Case-control study | National (All 36 States + FCT) | 2017 – 2019 | Suspected: 204; Confirmed: 86; Controls: 172 | Prevalence (Positivity): 42.1% CFR (Overall): 9.4% CFR (HIV+): 20.8% | HIV prevalence in cases: 27.9%; Overall CFR: 9.4%; HIV+ CFR: 20.8%; Children <15 CFR: 50%; HIV infection associated with 45-fold increased odds of mpox and 13.7-fold increased odds of death. |
| Adeniran, A.A. | 2024 | Retrospective analysis of surveillance data / Descriptive epidemiology | State-specific (Imo State) | Jan 2017 – Dec 2023 | Suspected: 231; Confirmed: 49 | Prevalence (Positivity): 21.2% CFR: 8% | Suspected cases: 231; Confirmed: 49 (21.2%); Male: 55.1%; Modal age: 20-24 years; Geographic clustering: 5 LGAs account for 60% of cases; CFR: 8%; Hospitalization: 26.5%. |
| Ogoina, D. | 2024 | Observational cross-sectional study | National (23 States + FCT) | Jun 2022 – Dec 2022 | Suspected: 265; Confirmed: 163 | Prevalence (Positivity): 61.5% HIV Co-infection: 18.0% | Confirmed cases: 163; Adult proportion: 84.0%; Male: 68.7%; Urban/semi-urban: 87.7%; HIV co-infection: 18.0%; VZV co-infection: 35.9%; Risk factors: sexual activity (adults), animal contact (children). |
| Stephen, R. | 2022 | Cross-sectional study (with follow-up survey) | State-specific (Adamawa) | Jan 2022 – Jul 2022 | Suspected: 33; MPX+: 11 | Prevalence (Positivity): 33.3% (any MPX) Co-infection: 27% (MPX-VZV) | MPX positivity: 33.3% (11/33); MPX-VZV co-infection: 27% (9/33); Male predominance: 79%; Children/adolescents (0-19y): 54% of infected; Animal contact: livestock 64%, rodents 86%; Three clusters identified. |
| Mmerem, J.I. | 2024 | Retrospective cohort study / Case series | Southern Nigeria (6 states) | Jan 2022 – Mar 2023 | Suspected: 94; Confirmed: 56 | Prevalence (Positivity): 60.0% CFR: 8.9% Co-infection: 28.6% | Confirmed mpox: 56; Mpox-chickenpox coinfection: 28.6%; Male: 60.7%; HIV coinfection: 23.2%; Hospitalization: 66.1%; Complication rate: 32.1% (56.3% in coinfected); CFR: 8.9%. |
| Ogoina, D. | 2023 | Cohort study (retrospective and prospective) | National (22 States + FCT) | Feb 2022 – Jan 2023 | Confirmed/Probable: 160 | CFR: 5.6% Severe Disease: 19% Complication Rate: 49% | HIV coinfection: 16%; Advanced HIV associated with 35.9x increased odds of severe disease; VZV coinfection associated with 3.6x increased odds of severe disease; Rash count >10,000 associated with 26x increased odds of severe disease. |
| Ogoina, D. | 2020 | Retrospective case series / chart review | National | Sep 2017 – Dec 2018 | Hospitalized: 40 | CFR: 12.5% Complication Rate: 52.5% | Hospitalized cases: 40; Male: 77.5%; HIV coinfection: 22.5%; Genital ulcers: 62.5% overall, 100% in HIV+; Complication rate: 52.5%; CFR: 12.5% overall (22.2% in HIV+). |
| Yinka-Ogunleye, A. | 2019 | Outbreak investigation / Descriptive epidemiology | National (17 States) | Sep 2017 – Sep 2018 | Suspected: 276; Confirmed/Probable: 122 | Prevalence (Positivity): 43% CFR: 6% Genital Lesions: 68% | Confirmed/probable cases: 122; CFR: 6%; Male: 69%; Median age: 29 years; Ecological zones: freshwater swamps/mangrove (54%); Genital lesions: 68%; Human-to-human transmission evidence: household, prison, healthcare clusters. |
| Ogoina, D. | 2019 | Cross-sectional study / Outbreak report | Single Hospital (Bayelsa) | Sep 2017 – Dec 2017 | Suspected: 38; Confirmed/Probable: 21 | Prevalence (Positivity): 55.3% CFR: 4.8% (suicide) | Confirmed/probable: 21; Male: 80.9%; Hospitalization: 61.9%; HIV coinfection: 25%; Household cluster and nosocomial transmission identified; No mpox-related deaths. |
| Yinka-Ogunleye, A. | 2018 | Outbreak investigation / Preliminary descriptive report | National (14 States) | Sep 2017 – Nov 2017 | Suspected: 146; Confirmed: 42 | Prevalence (Positivity): 39.3% CFR: 2.4% | First reemergence since 1978; Confirmed cases: 42 from 14 states; West African clade; Male: female ratio 2:1; CFR: 2.4%; Family clusters and human-to-human transmission (secondary attack rate 71% in one family). |
| Ogoina, D. | 2023 | Case series of linked transmission chains | Single Hospital (Bayelsa) | Jun 2022 – Oct 2022 | 16 Adults | Incubation Period: 5 days (median) Serial Interval: 8 days (median) | 16 linked heterosexual mpox cases; Incubation period: median 5 days; Serial interval: median 8 days; All cases linked through sexual contact; Genital rash: 100%; No anorectal lesions; No deaths. |
| Amao, L.K. | 2022 | Enhanced surveillance / Active case finding | Regional (South-South) | Jan 2021 – Mar 2021 | Suspected: 25; Confirmed: 3 | Prevalence (Positivity): 12% | Enhanced surveillance identified 25 suspected, 3 confirmed cases; Confirmation rate: 12%; 30 hotspot LGAs engaged; Trained 483 personnel. |
| Olayiwola, J.O. | 2025 | Cross-sectional study | LGA (Ibadan North LGA) | Jan 2025 – Jun 2025 | 94 Participants | Seroprevalence: 21.5% | Anti-Mpox IgG seroprevalence: 21.5%; Female: 27.4%; Male: 9.6%; Age-specific: <18 years (61.5%), 53-57 years (66.6%); Awareness of Mpox: 61.1%. |
| Onu, H.C. | 2023 | Retrospective secondary data analysis | State-specific (Rivers State) | Jan 2017 – Jun 2022 | Suspected: 112; Confirmed: 49 | Prevalence (Positivity): 44% CFR: 1.8% | Confirmed cases: 49 (44% of suspected); Male: 72.7%; Mean age: 33 years; Geographic clustering: urban LGAs; Seasonal peak: September-November (flooding season). |
| Onyeaghala, C. | 2025 | Observational retrospective study (hospital-based) | State-specific (Rivers State) | Oct 2021 – Apr 2023 | Suspected: 35; Confirmed: 24 | Prevalence (Positivity): 68.6% CFR (Overall): 8.6% CFR (HIV+): 60% | Confirmed: 24 (68.6%); Hospitalization: 80%; Overall CFR: 8.6%; HIV+ CFR: 60%; HIV prevalence: 14.3%; VZV coinfection: 25%; Genital lesions: 82.9%. |
| Cadmus, S. | 2025 | Cross-sectional study | LGA (Izzi LGA, Ebonyi) | Apr 2024 – May 2024 | 75 Tested | Point Prevalence: 2.67% | MPXV prevalence in community without rash: 2.67% (2/75); Both positive cases had non-exanthematous presentations (headache, body pain only); Demonstrates occult MPXV circulation in a rural border community. |
Abbreviations: CFR, case fatality rate; FCT, Federal Capital Territory; HIV, human immunodeficiency virus; LGA, local government area; MPX, mpox; VZV, varicella-zoster virus.
Table 1: Summary of Included Studies
| First Author (Year) | Study Design | Assessment Tool | Selection / Representativeness | Ascertainment / Measurement | Confounding / Comparability | Attrition / Completeness | Overall ROB Rating |
|---|---|---|---|---|---|---|---|
| Butswat, S.B. (2025) | Surveillance analysis | Modified ROB | Moderate | Moderate | N/A | Moderate | Moderate |
| Yinka-Ogunleye, A. (2023) | Case-control | Newcastle-Ottawa | Moderate | Low | Low | Moderate | Moderate |
| Adeniran, A.A. (2024) | Surveillance analysis | Modified ROB | Moderate | Moderate | N/A | Moderate | Moderate |
| Ogoina, D. (2024) | Cross-sectional | JBI Prevalence | Moderate | Low | Moderate | Moderate | Moderate |
| Stephen, R. (2022) | Cross-sectional | JBI Prevalence | Moderate | Low | Moderate | Moderate | Moderate |
| Mmerem, J.I. (2024) | Retrospective cohort | Newcastle-Ottawa | Moderate | Low | Moderate | Moderate | Moderate |
| Ogoina, D. (2023) Lancet ID | Cohort | Newcastle-Ottawa | Moderate | Low | Low | Moderate | Moderate-High |
| Ogoina, D. (2020) | Retrospective case series | Modified ROB | Moderate | Moderate | Moderate | Moderate-High | Moderate-High |
| Yinka-Ogunleye, A. (2019) | Outbreak investigation | Modified ROB | Low | Low | Moderate | Moderate | Moderate |
| Ogoina, D. (2019) | Cross-sectional | JBI Prevalence | Moderate | Moderate | Moderate | Moderate | Moderate |
| Yinka-Ogunleye, A. (2018) | Outbreak investigation | Modified ROB | Moderate | Moderate | N/A | Moderate | Moderate |
| Ogoina, D. (2023) NEJM | Case series | Modified ROB | Moderate | Moderate | N/A | Moderate | Moderate |
| Amao, L.K. (2022) | Enhanced surveillance | Modified ROB | Moderate | Low | N/A | Moderate-High | Moderate |
| Olayiwola, J.O. (2025) | Cross-sectional | JBI Prevalence | Moderate-High | Low | Moderate | Moderate-High | Moderate-High |
| Onu, H.C. (2023) | Surveillance analysis | Modified ROB | Moderate | Moderate | N/A | Moderate | Moderate |
| Onyeaghala, C. (2025) | Retrospective observational | Modified ROB | Moderate | Low | Moderate | Moderate | Moderate |
| Cadmus, S. (2025) | Cross-sectional | JBI Prevalence | Moderate-High | Low | Moderate | Moderate-High | Moderate-High |
| Abbreviations: ROB, risk of bias; JBI, Joanna Briggs Institute; NOS, Newcastle-Ottawa Scale; N/A, not applicable. | |||||||
Table 2: Risk of Bias Assessment for Included Studies
| Transmission Indicator | Pre-2022 (2017-2021) | 2022-2025 | Change |
|---|---|---|---|
| Animal contact reported | 8-21.5% | 1.8-2.8% | Decrease |
| Household transmission | 50-72% | 50-72% | Stable |
| Sexual transmission documented (% of studies) | 0% (0/5 studies) | 100% (7/7 studies) | Emergent |
| Genital lesions | 62.5-68% | 60.7-100% | Increase |
| Median age of cases (years) | 29-32 | 27-33 | Stable |
| Male proportion | 67-81% | 55-79% | Stable |
Note: Pre-2022 studies include references [12,18,19,22,23,24,27,28]; 2022-2025 studies include references [10,15,16,17,25,26]. Percentages represent ranges reported across multiple studies within each period.
Table 3: Temporal Evolution of Transmission Patterns in Nigeria (Pre-2022 vs. 2022-2025)
| Risk Factor | Measure of Association (95% CI) | Studies Reporting | Summary of Findings |
|---|---|---|---|
| HIV Infection | |||
| HIV infection (mpox risk vs general population) | OR 45.0 (6.1–333.5) | Yinka-Ogunleye, 2023 | HIV infection associated with 45-fold increased odds of mpox compared to general population |
| HIV infection (mpox risk vs non-mpox rash controls) | OR 7.29 (2.6–20.5) | Yinka-Ogunleye, 2023 | HIV infection associated with 7.3-fold increased odds of mpox compared to patients with non-mpox rash |
| HIV infection (overall mpox risk) | OR 4.77–8.59 (1.07–37.40) | Ogoina, 2024 | HIV infection consistently associated with increased mpox risk across multiple studies |
| HIV infection (mortality) | aOR 13.66 (1.88–98.95) | Yinka-Ogunleye, 2023 | HIV infection associated with 13.7-fold increased odds of death from mpox |
| HIV infection (mortality – hospitalized) | OR 2.67 (0.37–19.2) | Ogoina, 2020 | Elevated but non-significant mortality risk in HIV+ hospitalized patients |
| Advanced HIV disease (severe disease) | aOR 35.9 (5.1–252.9) | Ogoina, 2023 | Advanced HIV associated with 36-fold increased odds of severe mpox disease |
| HIV infection (severe disease) | OR 8.59 (1.97–37.40) | Ogoina, 2024 | HIV infection associated with 8.6-fold increased odds of severe disease |
| HIV infection (complications) | OR 3.1 (1.86–5.16) | Ogoina, 2020 | HIV infection associated with 3-fold increased odds of secondary bacterial infection |
| HIV infection (genital ulcers) | OR 1.94 (1.38–2.72) | Ogoina, 2020 | HIV infection associated with nearly 2-fold increased odds of genital ulcers |
| HIV infection (larger rash size) | OR 12.7 (1.4–114.4) | Ogoina, 2020 | HIV infection associated with 12.7-fold increased odds of rash size ≥2cm |
| HIV infection (longer illness duration) | OR 9.3 (1.36–63.9) | Ogoina, 2020 | HIV infection associated with 9.3-fold increased odds of illness duration ≥28 days |
| Age | |||
| Young age (<15 years) – mortality | aOR 0.90 per year increase (0.82–0.97) | Yinka-Ogunleye, 2023 | Each year increase in age associated with 10% decreased mortality risk; children <15 years had 50% CFR |
| Age 18-35 years (mpox risk) | aOR 3.93 (2.06–7.50) | Ogoina, 2024 | Adults aged 18-35 years had nearly 4-fold increased odds of mpox |
| Age >35 years (mpox risk) | aOR 4.75 (2.23–10.13) | Ogoina, 2024 | Adults aged >35 years had nearly 5-fold increased odds of mpox |
| Age 20-39 years | Not quantified | Onu, 2023 | Highest proportion of cases in 20–39-year age group |
| Age 20-24 years (modal) | Not quantified | Adeniran, 2024 | Modal age group among confirmed cases |
| Contact and Exposure | |||
| Close contact with confirmed case (overall) | aOR 2.96 (1.26–6.96) | Ogoina, 2024 | Close contact with confirmed case associated with 3-fold increased odds of mpox |
| Close contact with confirmed case (children) | aOR 4.76 (1.14–19.87) | Ogoina, 2024 | Children with close contact to confirmed case had 4.8-fold increased odds |
| Nonsexual contact with suspected case (adults) | aOR 5.50 (1.12–27.14) | Ogoina, 2024 | Nonsexual contact with suspected case associated with 5.5-fold increased odds in adults |
| Sexual contact with suspected case (adults) | aOR 2.81 (1.01–7.79) | Ogoina, 2024 | Sexual contact with suspected case associated with 2.8-fold increased odds in adults |
| Contact with suspected case | OR not quantified (37.5% exposed) | Mmerem, 2024 | 37.5% of confirmed cases reported contact with suspected case |
| Contact with rash case | 50% exposed | Stephen, 2022 | 50% of infected individuals reported contact with someone with rashes |
| Sexual and Behavioral Factors | |||
| Risky sexual behavior (adults) | aOR 2.81 (1.40–5.63) | Ogoina, 2024 | Risky sexual behavior associated with 2.8-fold increased odds of mpox |
| Multiple sexual partners | 42.5% of cases | Mmerem, 2024 | 42.5% of confirmed cases reported multiple sexual partners |
| Condomless vaginal sex | 100% of linked cases | Ogoina, 2023 | All 16 linked heterosexual cases reported condomless vaginal sex |
| Contact with female sex workers | 3 of 16 cases (18.8%) | Ogoina, 2023 | 3 linked cases had contact with female sex workers |
| Bisexual/MSM | 12.5% of cases | Mmerem, 2024 | 12.5% of confirmed cases identified as bisexual or men who have sex with men |
| Self-reported GBMSM | 7.4% of cases | Ogoina, 2024 | 7.4% of confirmed cases self-identified as GBMSM |
| Animal Exposure | |||
| Animal exposure (children) | aOR 9.97 (1.27–78.34) | Ogoina, 2024 | Animal exposure associated with 10-fold increased odds of mpox in children |
| Animal exposure (overall) | 21.5% exposed | Ogoina, 2024 | 21.5% of confirmed cases reported animal exposure |
| Animal contact (livestock) | 64% of infected | Stephen, 2022 | 64% of infected individuals reported contact with livestock |
| Animal contact (rodents) | 86% of infected | Stephen, 2022 | 86% of infected individuals reported contact with rodents |
| Animal contact (any) | 8% of cases | Yinka-Ogunleye, 2019 | 8% of confirmed cases reported animal contact (monkeys, rodents, bushmeat) |
| Wildlife contact | 1.8% of cases | Mmerem, 2024 | Minimal wildlife contact reported (1.8%) |
| Varicella-Zoster Virus (VZV) Co-infection | |||
| VZV co-infection (severe disease) | aOR 3.6 (1.1–11.5) | Ogoina, 2023 | VZV co-infection associated with 3.6-fold increased odds of severe mpox disease |
| VZV co-infection (children) | OR 5.74 (1.89–17.43) | Ogoina, 2024 | VZV co-infection associated with 5.7-fold increased odds of mpox in children |
| VZV co-infection (adults) | OR 0.43 (0.21–0.87) | Ogoina, 2024 | VZV co-infection was protective against mpox in adults (inverse association) |
| VZV co-infection (complications) | OR 4.43 (1.29–15.23) | Mmerem, 2024 | Coinfected patients had 4.4-fold increased odds of complications |
| VZV co-infection (muscle pain) | OR 5.17 (1.04–25.85) | Mmerem, 2024 | Coinfected patients had 5.2-fold increased odds of muscle pain |
| VZV co-infection (sore throat) | OR 5.13 (1.46–18.01) | Mmerem, 2024 | Coinfected patients had 5.1-fold increased odds of sore throat |
| Clinical Severity Markers | |||
| Rash count >10,000 (severe disease) | aOR 26.1 (5.2–135.0) | Ogoina, 2023 | High rash burden (>10,000 lesions) associated with 26-fold increased odds of severe disease |
| Confluent/semiconfluent rash (severe disease) | aOR 6.7 (1.9–23.9) | Ogoina, 2023 | Confluent rash pattern associated with 6.7-fold increased odds of severe disease |
| Late presentation (>7 days) | Associated with severity (p=0.0018) | Ogoina, 2023 | Late presentation associated with higher proportion of severe disease (25% vs 10%) |
| Demographic Factors | |||
| Male sex | 69–80.9% of cases | Multiple studies | Male predominance consistently observed (69-80.9% of confirmed cases) |
| Male sex (risk) | OR not quantified | Multiple studies | Male sex identified as risk factor across multiple studies |
| Female sex | 27.4% seroprevalence vs 9.6% in males (p=0.050) | Olayiwola, 2025 | Higher seroprevalence in females in community-based study |
| Geographic and Environmental Factors | |||
| Urban residence | 87.7% of cases | Ogoina, 2024 | Predominantly urban/semi-urban residence (87.7%) |
| Urban residence (Rivers State) | Geographic clustering | Onu, 2023 | Cases clustered in urban LGAs (Obio-Akpor and Port Harcourt) |
| Freshwater swamp/mangrove ecological zone | 54% of cases | Yinka-Ogunleye, 2019 | Majority of cases (54%) resided in freshwater swamp/mangrove zones |
| Prison incarceration | 4.3% of suspected cases | Adeniran, 2024 | 4.3% of suspected cases were incarcerated |
| Household transmission setting | 72.2% of contacts | Onyeaghala, 2025 | Household accounted for 72.2% of identified transmission contacts |
| Occupational and Socioeconomic Factors | |||
| Farming occupation | 78.7% of participants | Cadmus, 2025 | High proportion of farmers in community-based study |
| No formal education | 52.0% of participants | Cadmus, 2025 | High proportion without formal education in rural community |
| Healthcare work | 2 healthcare workers infected | Yinka-Ogunleye, 2019; Ogoina, 2019 | Healthcare workers infected during outbreak response |
Note: OR = Odds Ratio; aOR = adjusted Odds Ratio.
Table 4: Summary of Risk Factors for Mpox in Nigeria
| Study (First Author, Year) | Study Design | Setting | Sample Size (Confirmed) | Common Symptoms (% of cases) | Genital Lesions (%) | Hospitalization Rate (%) | Complication Rate (%) | CFR (%) | HIV Co-infection (%) |
|---|---|---|---|---|---|---|---|---|---|
| Hospital-Based Studies | |||||||||
| Ogoina, 2024 | Cross-sectional | Hospital-based | 163 | NR | NR | NR | NR | NR | 18.0% |
| Mmerem, 2024 | Retrospective cohort | Hospital-based | 56 | Febrile rash (92.9%), Itchy rash (100%), Headache (69.6%), Myalgia (66.1%), Fatigue (53.6%), Sore throat (41.1%) | 60.7% | 66.1% | 32.1% | 8.9% | 23.2% |
| Ogoina, 2023 | Cohort | Hospital-based | 160 | Skin rash (100%), Fever (92%), Headache (77%), Malaise (76%), Distinct febrile prodrome (59%) | 19% (first rash site) | 48% | 49% | 5.6% | 16% |
| Ogoina, 2020 | Retrospective case series | Hospital-based | 40 | Skin rash (100%), Fever (90%), Lymphadenopathy (87.5%), Genital ulcer (62.5%), Body aches (62.5%), Headache (47.5%) | 62.5% (ulcers) | 100% | 52.5% | 12.5% | 22.5% |
| Ogoina, 2019 | Cross-sectional | Hospital-based | 21 | Vesiculopustular rash (100%), Fever (90.5%), Skin itching (66.7%), Headache (61.9%), Lymphadenopathy (61.9%) | Present in HIV+ cases | 61.9% | NR | 4.8%* | 25% |
| Ogoina, 2023 | Case series | Hospital-based | 16 | Genital rash (100%), Distinct febrile prodrome (75%), Lesions localized to genital area (62%) | 100% | NR | 0% | 0% | 0% |
| Onyeaghala, 2025 | Retrospective | Hospital-based | 24 | Skin rash (100%), Fever (74.3%), Fatigue (74.3%), Headache (54.3%) | 82.9% | 80% | 22.9% | 12.5% | 14.3% |
| Community/Surveillance-Based Studies | |||||||||
| Butswat, 2025 | Retrospective surveillance | Community/Health facility | 16 | Fever (most common), Headache, Vesiculopustular rash | NR | NR | NR | 0% | NR |
| Yinka-Ogunleye, 2023 | Case-control | Community-based | 86 | Fever (83.6%), Lymphadenopathy (73%), Genital lesions (89.6%), Oral lesions (28.3%) | 89.6% | 81% | NR | 9.4% | 27.9% |
| Adeniran, 2024 | Retrospective surveillance | Community/Health facility | 49 | Fever, chills, Headaches, Lethargy, Asthenia, Lymphadenopathy, Back pain, Myalgia | NR | 26.5% | NR | 8% | NR |
| Stephen, 2022 | Cross-sectional | Community-based | 11 | Body rashes/itching (100%), Fever (93%), Headache (64%), Mouth sores (57%), Muscle aches (57%), Lymphadenopathy (50%), Conjunctivitis (50%) | 43% | 20% | 50% (conjunctivitis) | 0% | NR |
| Yinka-Ogunleye, 2019 | Outbreak investigation | Community-based | 122 | Vesiculopustular rash (100%), Fever (88%), Headache (79%), Pruritus (73%), Lymphadenopathy (69%), Myalgia (63%), Sore throat (58%) | 68% | NR | NR | 6% | 4 of 7 deaths had HIV/AIDS |
| Yinka-Ogunleye, 2018 | Outbreak investigation | Community-based | 42 | Fever, generalized rash, headache, malaise, sore throat, lymphadenopathy | NR | NR | NR | 2.4% | NR |
| Onu, 2023 | Retrospective surveillance | Surveillance system | 49 | Sudden onset of fever, pustular rash on face, palms, soles | NR | NR | NR | 1.8% | NR |
| Amao, 2022 | Enhanced surveillance | Community-based | 3 | NR | NR | NR | NR | 0% | NR |
| Special Populations | |||||||||
| Olayiwola, 2025 | Cross-sectional | Community (seroprevalence) | 20 (seropositive) | Asymptomatic (seroprevalence study) | N/A | N/A | N/A | N/A | N/A |
| Cadmus, 2025 | Cross-sectional | Community (non-exanthematous) | 2 | Headache, body pain only; NO rash | 0% | N/A | N/A | 0% | NR |
Note: One death by suicide, not directly from mpox complications; NR = Not reported; N/A = Not applicable
Table 5: Summary of Clinical Characteristics Across Studies
| Study | Rash Distribution/Presentation | Lymphadenopathy | Other Notable Symptoms | Vaccination History |
|---|---|---|---|---|
| Hospital-Based Studies | ||||
| Mmerem, 2024 | Genital rash (60.7%), Oral lesions (19.6%), Anogenital pain/bleeding (10.7%), Genital soft tissue swelling (30.4%) | 46.5% | Sore throat (41.1%), Diarrhea (8.9%), Cough (16.1%) | No vaccination |
| Ogoina, 2023 | First rash: face (53%), anogenital (19%); Distribution: centrifugal (63%), centripetal (18%), mainly anogenital (13%); Rash count: >10,000 (16%) | Inguinal (43%), cervical (38%), submandibular (31%), axillary (25%), generalized (9%) | Distinct febrile prodrome (59%) | Prior smallpox: 4% |
| Ogoina, 2020 | Rash distribution: face (97.5%), trunk (92.5%), arms (87.5%), legs (85%), genitalia (67.5%), scalp (62.5%), palms (55%), soles (50%), mouth (37.5%), eyes (25%); Rash as first symptom (65.7%) | Inguinal, generalized, cervical, axillary, submental (87.5%) | Genital ulcer (62.5%), Pruritus (37.5%) | NR |
| Ogoina, 2019 | Vesiculopustular rash (100%); Genital ulcers in HIV+ cases | 61.9% | Skin itching (66.7%) | NR |
| Ogoina, 2023 (NEJM) | Genital rash (100%), Lesions localized to genital area (62%), No anorectal lesions | NR | Distinct febrile prodrome (75%) | NR |
| Onyeaghala, 2025 | First rash: face (94.3%), anogenital (5.7%); Rash types: pustules (91.4%), papules (77.1%), vesicles (77.1%); Lesion locations: trunk (100%), limbs (100%), genitals (82.9%) | NR | NR | NR |
| Community/Surveillance Studies | ||||
| Yinka-Ogunleye, 2023 | Genital lesions (89.6%), Oral lesions (28.3%) | 73% | NR | NR |
| Yinka-Ogunleye, 2019 | Rash distribution: face (96%), legs (91%), trunk (80%), arms (79%), palms (69%), genitalia (68%), soles (64%) | 69% | Pruritus (73%), Myalgia (63%), Sore throat (58%) | NR |
| Stephen, 2022 | Genital rashes (43%), Mouth sores (57%), Conjunctivitis (50%) | 50% | Muscle aches (57%), Backache (36%), Respiratory symptoms (29%) | NR |
| Onu, 2023 | Pustular rash on face, palms, soles | NR | NR | NR |
Note: NR = Not Reported
Table 6: Detailed Clinical Characteristics – Symptoms and Presentation
| Study | Complication Rate | Specific Complications | Common Comorbidities |
|---|---|---|---|
| Hospital-Based Studies | |||
| Mmerem, 2024 | 32.1% | Sepsis (83.3% of complications), Wound infection, Pneumonia, Acute kidney injury, Acute urinary retention | HIV (23.2%), Diabetes (5.4%), Pregnancy (2 women) |
| Ogoina, 2023 | 49% | Skin complications (48%): secondary bacterial infections (43%), penile/vulva edema (23%), scrotal edema (13%); Mucosal complications (19%): urethritis (7%), keratitis (6%), proctitis (6%); Systemic (21%): sepsis (18%), pneumonia (8%), encephalitis (1%) | HIV (16%; 44% advanced), VZV (30%), Diabetes, hypertension |
| Ogoina, 2020 | 52.5% | Secondary bacterial skin infection (47.5%), Gastroenteritis (12.5%), Sepsis (10%), Bronchopneumonia (7.5%), Encephalitis (7.5%), Keratitis (7.5%), PROM + fetal death (2.5%) | HIV (22.5%), Chickenpox (2.5%) |
| Ogoina, 2019 | NR | PROM with fetal loss, Thrombocytopenia | HIV (25%), Syphilis (25%), Chickenpox (2 cases) |
| Ogoina, 2023 (NEJM) | 0% | None | All HIV-negative |
| Onyeaghala, 2025 | 22.9% | Secondary bacterial skin infections (22.9%), Scrotal edema (5.7%), Pharyngotonsillitis (8.6%), Ocular injuries (2.9%), Urinary retention (2.9%), Necrotizing genital ulcers (8.6%), Sepsis (8.6%), Pneumonia (5.7%) | HIV (14.3%), VZV (25%), Advanced HIV (60% of HIV+) |
| Community/Surveillance Studies | |||
| Yinka-Ogunleye, 2023 | NR | Death, Encephalitis (1 pediatric case) | HIV (27.9%), HPV (50%), HSV-1 (22.5%) |
| Yinka-Ogunleye, 2019 | NR | Spontaneous abortion (26 weeks), Secondary bacterial infection with sepsis | HIV/AIDS (4 of 7 deaths) |
| Stephen, 2022 | 50% (conjunctivitis) | Conjunctivitis (50%), Crusting around lesions (53.9% VZV patients) | Malaria (57%), UTI (21%), Skin infection (14%), Diabetes (7%), Hypertension (7%) |
| Adeniran, 2024 | NR | NR | No comorbidities reported |
| Butswat, 2025 | NR | 25% asymptomatic | NR |
Note: NR = Not Reported; PROM = Premature Rupture of Membranes; VZV = Varicella-Zoster Virus
Table 7: Complications and Comorbidities
| Clinical Characteristic | Pre-2022 Outbreaks (2017-2019) | 2022-2025 Outbreak Period |
|---|---|---|
| Most Common Symptoms | Rash (100%), Fever (88-90%), Lymphadenopathy (69-87.5%), Headache (47.5-79%) | Rash (100%), Fever (74-93%), Fatigue (53.6-74.3%), Headache (54.3-77%), Myalgia (66.1%) |
| Genital Lesions | 62.5-89.6% | 60.7-100% |
| Hospitalization Rate | 61.9-81% | 48-80% |
| Complication Rate | 52.5% | 22.9-49% |
| CFR | 2.4-12.5% | 0-12.5% |
| HIV Co-infection | 22.5-27.9% | 14.3-23.2% |
| VZV Co-infection | 2.5% (single case) | 25-35.9% |
| Key Clinical Features | Rash often first symptom (65.7%), Centrifugal distribution, High complication rates in hospitalized patients | Genital rash more prominent, Distinct febrile prodrome, Sexual transmission documented, Asymptomatic cases reported (25%) |
| Special Findings | Household clusters, Nosocomial transmission, High mortality in HIV+ and children | Mpox-VZV co-infection common, Non-exanthematous presentations, Heterosexual transmission chains |
Table 8: Summary of Clinical Findings by Study Period
Joseph Paul Ngbede1, Sylvia Adanma Ezenwa-Ahanene2, Franka Ruth Njiforti1, Ruth Manzo Sabo3, Mathew Sunday Sabah4, Polycarp Dauda Madaki5,6,&
1Department of Public Health, Faculty of Basic and Applied Biological Sciences, Ahmadu Bello University, Zaria, Nigeria, 2Nigeria Centre for Disease Control and Prevention (NCDC), Abuja, Nigeria, 3Africa Centres for Disease Control and Prevention (Africa CDC), Addis Ababa, Ethiopia, 4Department of Veterinary Public Health and Preventive Medicine, University of Jos, Plateau State, Nigeria, 5Department of Veterinary Tropical Diseases, University of Pretoria, Pretoria, South Africa, 6Department of Veterinary and Livestock Services, Kaduna State Government, Kaduna, Nigeria
&Corresponding author: Polycarp Dauda Madaki, Department of Veterinary Tropical Diseases, University of Pretoria, Pretoria, South Africa, Email: polycarpmadaki@gmail.com, ORCID: https://orcid.org/0009-0001-8216-9779
Received: 31 Mar 2026, Accepted: 21 May 2026, Published: 22 May 2026
Domain: Infectious Disease Epidemiology
Keywords: Mpox, Nigeria One Health, systematic review, meta-analysis, case fatality rate, zoonosis, HIV co-infection
©Joseph Paul Ngbede et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Joseph Paul Ngbede et al., Epidemiological shifts and zoonotic drivers of mpox in Nigeria: A One Health systematic review and meta-analysis, 2017–2025. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):83. https://doi.org/10.37432/jieph-d-26-00103
Introduction: Since its re-emergence in 2017, mpox has become a significant public health priority in Nigeria. Despite numerous studies, epidemiological estimates remain fragmented. This review synthesises current evidence on the prevalence, mortality, and One Health drivers of mpox in Nigeria.
Methods: Following PRISMA guidelines, we searched PubMed, Scopus, Web of Science, and Google Scholar for studies on mpox epidemiology in Nigeria published between 2017 and 2025. Random-effects meta-analysis was used to estimate pooled laboratory confirmation and case fatality rates (CFR).
Results: Seventeen studies met the inclusion criteria. The pooled laboratory confirmation rate among suspected cases was 36.7% (95%CI: 22.2-54.1%), with significant heterogeneity (I2=93.7%). The pooled CFR among confirmed cases was 7.0% (95%CI: 5.4-9.2%). Critically, the CFR for HIV-positive individuals was 26.2% (CI: 4.2-73.9%), representing a nearly fourfold increase in mortality risk. Narrative synthesis of recent outbreaks (2022-2025) suggests evolving transmission dynamics, including the emergence of sexual transmission pathways and increased genital presentations, though quantitative comparisons were limited by heterogeneity in outcome reporting. While 1.8-21.5% of cases reported animal contact, no studies performed primary sampling of animal reservoirs. Environmental drivers, including flooding and deforestation, were consistently linked to seasonal peaks in the wet season (September-November).
Conclusion: Mpox in Nigeria is characterised by evolving transmission dynamics and a high burden among immunocompromised populations. The lack of integrated human-animal-environmental sampling highlights a critical gap in the One Health response. Strengthening surveillance for asymptomatic infections and integrating HIV-mpox care are urgent priorities for national preparedness.
Mpox (monkeypox) is a re-emerging zoonotic viral disease caused by the monkeypox virus (MPXV), an enveloped double-stranded DNA virus in the Orthopoxvirus genus of the Poxviridae family[1-3]. MPXV is closely related to variola (smallpox) virus and comprises two lineages: Clade I, which is endemic to Central Africa and associated with higher virulence, and Clade II, endemic to West Africa [4, 5]. Clinically, the disease presents with fever, lymphadenopathy, and a distinctive vesiculopustular rash lasting 2-3 weeks. Severe cases may lead to secondary bacterial infections, respiratory distress, and encephalitis [1, 3, 4]. Transmission occurs via direct contact with infected animals (e.g. rodents, primates) or person-to-person through close contact with lesions, respiratory droplets or contaminated fomites[5, 6]. Since the global eradication of smallpox in 1980 and the cessation of routine smallpox vaccination, population-level immunity against Orthopoxviruses has significantly declined, allowing MPXV to emerge as the most significant Orthopoxvirus infection in humans, raising global health concerns due to its morbidity, mortality, and epidemic potential [7, 8].
Globally, mpox has transitioned from a neglected zoonosis to a recognised public health emergency. The 2022 multi-country outbreak marked an unprecedented epidemiological shift, with over 100,000 confirmed cases reported across more than 120 countries, including non-endemic regions [9]. Although the global case fatality rate remains relatively low, typically below 3% for the West African clade, the disease contributes substantial morbidity due to complications such as secondary bacterial infections, ocular involvement, and prolonged illness[7, 10]. In Africa, mpox remains endemic, with the highest burden reported in Central and West Africa. Between 2022 and 2024, over 37,000 cases and more than 1,400 deaths were reported across African countries, corresponding to a case fatality rate of approximately 3.9% [6].
Nigeria has emerged as a critical focal point for the virus in West Africa since its major re-emergence in 2017 [2]. The country has faced continuous outbreaks with increasing morbidity; as of October 2025, Nigeria recorded 389 confirmed cases and six deaths for the year, with infections distributed across 35 states and the Federal Capital Territory[11]. While mortality in Nigeria has generally been lower than in Central Africa, morbidity remains significant, particularly among immunocompromised individuals and populations with limited access to healthcare [10]. Additionally, evidence suggests evolving transmission dynamics, including increased human-to-human transmission and changing demographic patterns, including a shift from predominantly pediatric cases (pre-2017) to adult predominance (median age 27-33 years) during the 2017-2025 period, and a transition from male: female ratios of approximately 1:1 in early outbreaks to 3:1 male predominance in recent outbreaks [12, 13].
However, epidemiological evidence on mpox in Nigeria remains fragmented, with substantial inconsistencies in study design, geographic coverage, and outcome measurement. Estimates of prevalence, incidence, and case fatality rates vary widely across studies, and population-level incidence is rarely reported. Moreover, despite the recognized importance of a One Health framework, existing research provides minimal integration of animal reservoir data and environmental determinants, limiting understanding of the broader transmission ecology. Given these gaps, a comprehensive synthesis of available evidence is urgently needed to generate pooled epidemiological estimates and to contextualize human, animal, and environmental findings within a unified framework. Such evidence is critical for improving risk assessment, strengthening surveillance, guiding targeted interventions, and supporting national preparedness and response strategies for mpox in Nigeria.
This review, therefore, synthesises current evidence to estimate the pooled prevalence, incidence, and case fatality rate of mpox in Nigeria, while also describing available animal and environmental findings relevant to transmission. In addition, the review examines sources of heterogeneity across studies to better understand variations in epidemiological patterns within the country.
Protocol and registration
This systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement guidelines. The review protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD420261332715.
Eligibility criteria
The eligibility criteria were defined based on the Population, Exposure, Outcomes, and Study Design (PEOS) framework.
Information sources and search strategy
A comprehensive literature search was conducted across four electronic databases: PubMed/MEDLINE, Scopus, Web of Science, and Google Scholar, from inception to the date of the last search. Grey literature was searched through the Nigeria Centre for Disease Control (NCDC) website, African Journals Online, and hand-searching of reference lists from included studies and relevant reviews.
The search strategy combined terms related to the condition (monkeypox OR mpox), geographic location (Nigeria AND Nigerian states), and epidemiological outcomes (epidemiology, prevalence, incidence, mortality, case fatality, outbreak, surveillance, One Health, zoonotic, transmission, animal reservoir). Boolean operators (AND, OR) and truncation were employed across all databases. The detailed search strategy for each database is provided in Supplementary Material 1.
Study selection process
All retrieved records were imported into Rayyan. Duplicate records were identified and removed using automated deduplication features, followed by manual verification. Duplicate publications of the same study (e.g., conference abstract followed by full publication) were identified, and the most complete version was retained. Two independent reviewers (JPN and PDM) screened all titles and abstracts against the eligibility criteria using a standardised screening form. Records were categorised as include (proceed to full-text review), exclude (with reason documented), or undecided (proceed to full-text review for clarification).
Full-text articles of potentially eligible studies were retrieved and assessed independently by the same two reviewers using a standardized full-text screening form. Reasons for exclusion at this stage were documented according to PRISMA 2020 guidelines. Disagreements between reviewers were resolved through discussion and consensus, with consultation of a third reviewer (SAE) if consensus could not be reached.
Data extraction
Data extraction was performed independently by two reviewers (JNP and PDM) using a standardized, piloted data extraction form developed in Microsoft Excel. The extraction form was piloted on three randomly selected included studies to ensure consistency and completeness.
The following data were extracted:
Cohen’s kappa coefficient was calculated to assess inter-rater agreement for study selection.
Risk of bias assessment
Risk of bias was assessed independently by two reviewers using study design-specific tools:
Risk of bias assessment results are presented in a summary table with ratings for each domain and overall rating per study.
Data synthesis and meta-analysis
Given the anticipated heterogeneity in study designs, populations, and outcome definitions, a narrative synthesis was conducted for all outcomes. Meta-analysis was considered for outcomes where sufficient comparable data were available, specifically laboratory confirmation rates (positivity rates) among suspected cases and case fatality rates among confirmed cases, with subgroup analysis by HIV status.
When meta-analysis was feasible, proportions were analyzed with pooled estimates calculated using 95% confidence intervals. Random-effects models employing the inverse-variance method with logit transformation were used due to anticipated heterogeneity across studies.
Heterogeneity assessment: Statistical heterogeneity was assessed using the I² statistic, interpreted as: 0-40% (might not be important), 30-60% (moderate), 50-90% (substantial), and 75-100% (considerable). The chi-square test (Cochran’s Q) was used to assess the presence of heterogeneity, with significance set at p < 0.10.
Subgroup analyses: Planned subgroup analyses included stratification by study period (pre-2022 versus 2022-2025), study design (hospital-based versus community-based/surveillance), and HIV status.
Sensitivity analyses: Sensitivity analyses were planned to assess the robustness of pooled estimates by excluding studies with small sample sizes (fewer than 30 confirmed cases) and excluding studies with moderate-high risk of bias.
All statistical analyses were conducted using R software (version 4.3.1) with the meta package. Results were considered statistically significant at p < 0.05, except for heterogeneity assessment where p < 0.10 was used.
Ethical Approval
Not applicable. This study is a systematic review and meta-analysis of published literature; no primary data collection involving human or animal subjects was conducted.
Study selection
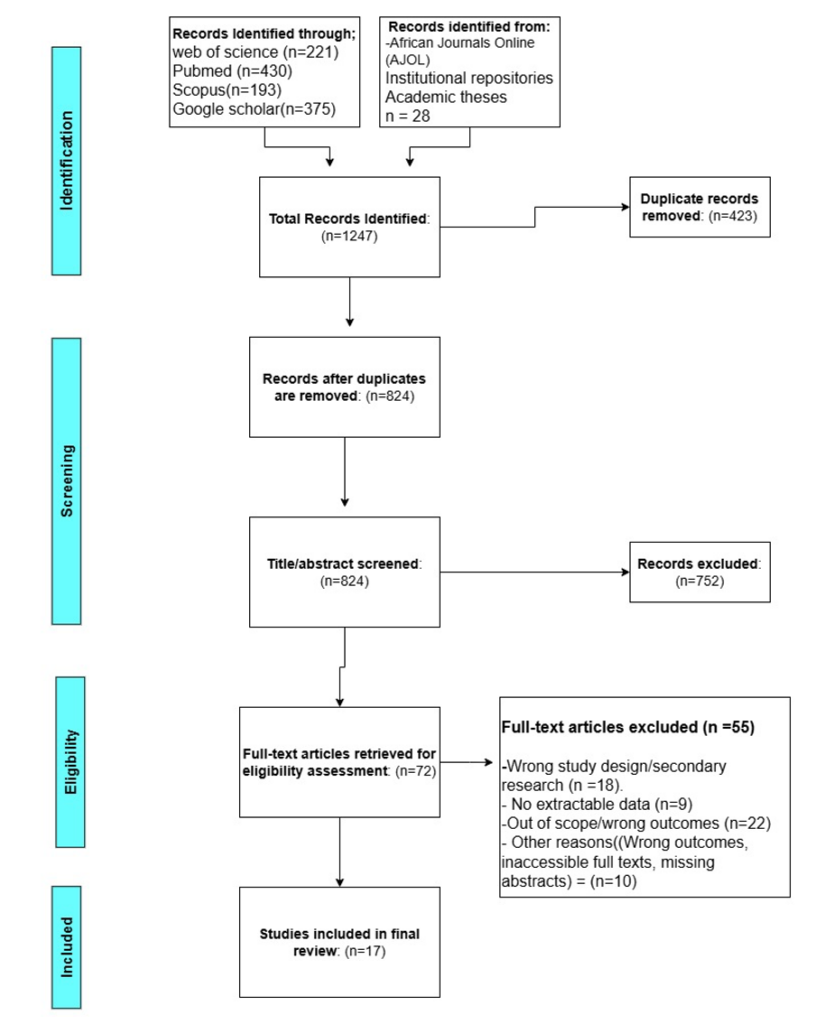
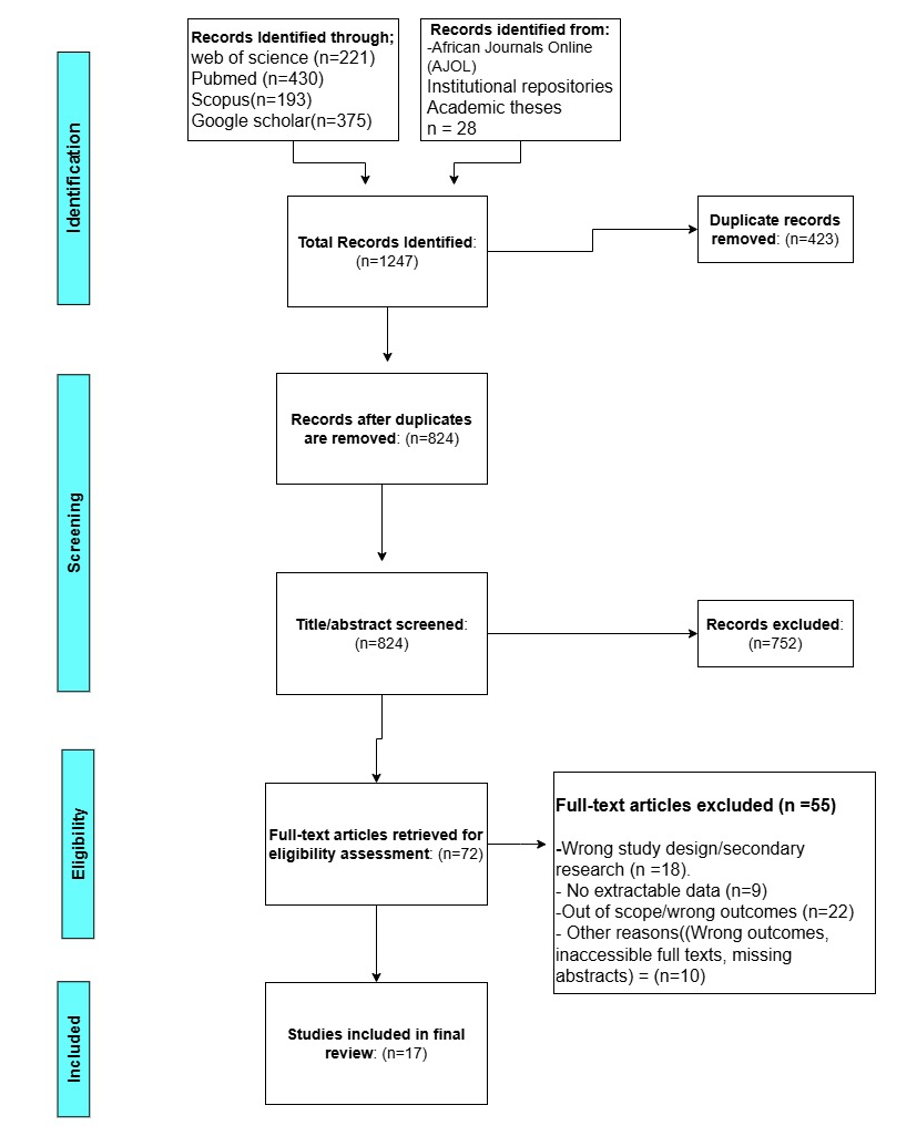
The systematic search of PubMed, Scopus, Web of Science, and Google Scholar, supplemented by grey literature searches of the Nigeria Centre for Disease Control (NCDC) website, yielded a total of 1,247 records. After removing duplicates (n=423), 824 records were screened by title and abstract. Of these, 752 records were excluded as they did not meet the eligibility criteria. Full-text articles were assessed for eligibility (n=72), of which 55 were excluded with reasons: 9 did not report extractable epidemiological data, 18 were case reports or case series with fewer than five cases, 23 were reviews or commentaries without primary data, 3 were modeling studies without primary data, and 2 were duplicate publications. A total of 17 studies met the inclusion criteria and were included in this systematic review (Figure 1).
Inter-rater agreement
Two independent reviewers conducted title and abstract screening and full-text review. Inter-rater agreement for study selection was substantial, with a Cohen’s kappa (κ) of 0.84 (95% CI: 0.76-0.92), indicating high consistency between reviewers. Disagreements were resolved through consensus discussion or consultation with a third reviewer when necessary.
Characteristics of included studies
A summary of the 17 included studies is presented in Table 1. Of the 17 included studies, 15 (88.2%) were published in peer-reviewed journals and 2 (11.8%) were grey literature sources (enhanced surveillance reports and outbreak investigation reports from national/state health authorities). No preprints were included as the search was limited to published literature and official government reports. The studies were published between 2017 and 2025, with the majority (n=10, 58.8%) published in 2022-2025 following the 2022 global mpox outbreak. The earliest study [27] described the initial re-emergence of mpox in Nigeria in September 2017. The most recent studies [20,21] were published in 2025. All studies covered surveillance or outbreak periods between 2017 and 2025, with no eligible studies identified before 2017. Study designs included outbreak investigations (n=4), cross-sectional studies (n=4), retrospective analyses of surveillance data (n=4), cohort studies (n=2), case-control studies (n=1), enhanced surveillance reports (n=1), and observational retrospective studies (n=1). The geographic scope varied from single state to national coverage, with studies conducted in Bayelsa (n=3), Rivers (n=3), Plateau (n=1), Imo (n=1), Adamawa (n=1), Ebonyi (n=1), Ibadan (n=1), and multiple states (n=6). Sample sizes ranged from 16 to 276 participants for suspected or confirmed cases, with seroprevalence studies including 75-94 participants. Studies classified as ‘outbreak investigations’ were not treated as a distinct design category. Rather, each was reclassified based on its underlying design: descriptive cross-sectional studies (single-time-point assessment during an outbreak), retrospective cohort studies (surveillance data following suspected cases over time), or case series (description of a small number of linked cases). This reclassification ensured consistent application of risk assessment tools
Risk of bias assessment
Risk of bias was assessed using appropriate tools based on study design. For cross-sectional studies, the Joanna Briggs Institute (JBI) Critical Appraisal Checklist was used; for cohort and case-control studies, the Newcastle-Ottawa Scale was applied. For surveillance reports and outbreak investigations, a modified risk of bias assessment tool was employed based on key methodological considerations including case definition clarity, data completeness, ascertainment methods, and representativeness. Overall, 13 studies (76.5%) were rated as having moderate risk of bias, while 4 studies (23.5%) were rated as having moderate-to-high risk of bias (Table 2). No study was rated as having low risk of bias across all domains.
Common methodological limitations identified across studies included: small sample sizes that limited statistical power for subgroup analyses (n=12, 70.6%); incomplete documentation or missing data for key variables such as HIV status, contact history, and clinical details (n=9, 52.9%); reliance on secondary surveillance data with variable data quality and completeness (n=6, 35.3%); hospital-based recruitment that may have introduced selection bias toward more severe cases (n=7, 41.2%); and geographic confinement to single states or institutions limiting generalizability (n=11, 64.7%).
Synthesis of findings
Given the heterogeneity in study designs, populations, and outcome definitions across the 17 included studies, a narrative synthesis was conducted for all outcomes. Meta-analysis was considered for selected outcomes where sufficient comparable data were available, specifically laboratory confirmation rates (positivity rates) among suspected cases and case fatality rates among confirmed cases, with subgroup analysis by HIV status where data permitted.
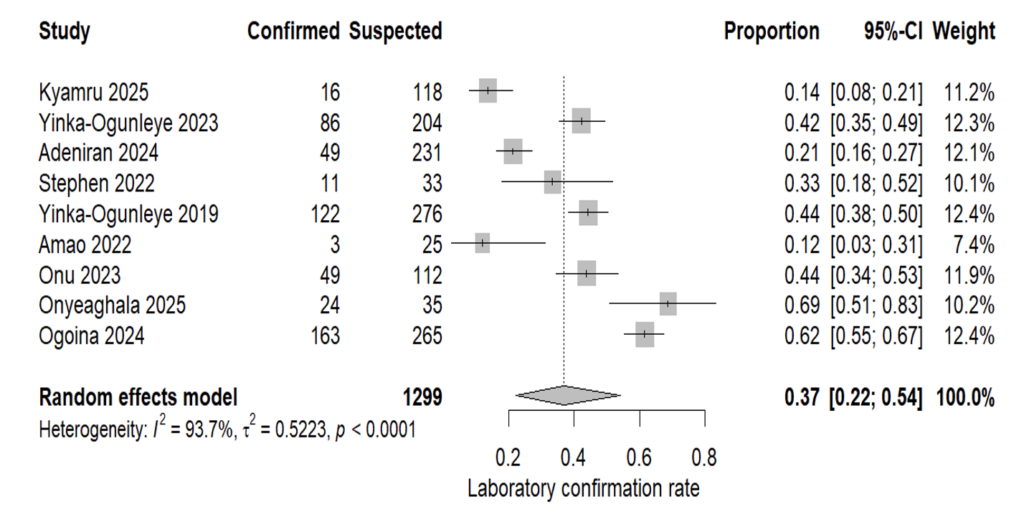
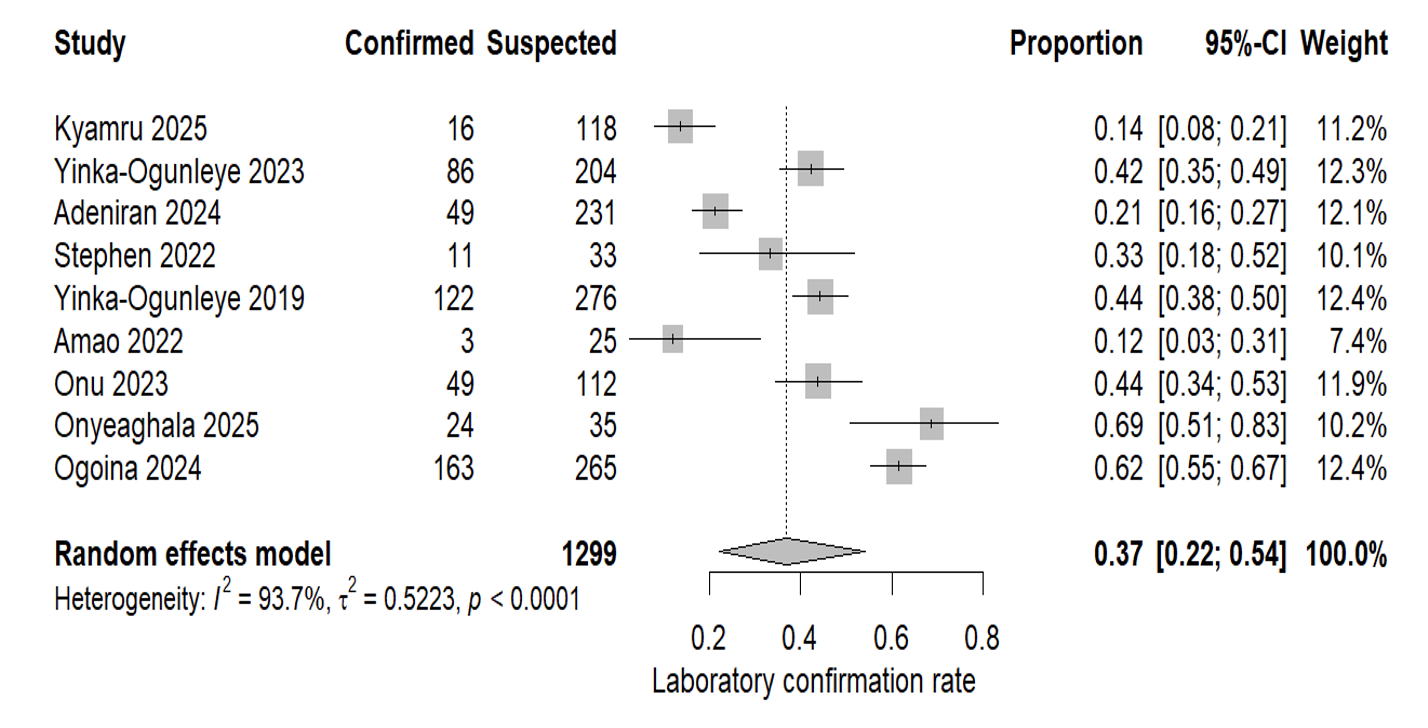
Across nine studies reporting laboratory confirmation among suspected mpox cases, the proportion testing positive varied substantially across study settings and time periods. Individual study estimates ranged from 12.0% (3/25) during enhanced surveillance conducted in the COVID-19 period [14] to 68.6% (24/35) in a hospital-based study during the 2022-2023 outbreak [15]. National surveillance and outbreak datasets also demonstrated considerable variation, with confirmation rates of 44.2% (122/276) during the 2017-2018 national outbreak [12] and 42.2% (86/204) in national surveillance data spanning 2017–2019 [16]. State-level estimates further highlighted marked regional heterogeneity, including 13.6% in Plateau State [17], 43.8% in Rivers State[18], and 21.2% in Imo State [19].
A random-effects meta-analysis using the inverse-variance method with logit transformation yielded a pooled laboratory confirmation rate of 36.7% (95% CI: 22.2-54.1%). However, between-study heterogeneity was considerable (I² = 93.7%; Q = 127.70, p < 0.001) (Figure 2), indicating substantial variability across surveillance systems, case definitions, laboratory ascertainment methods, and clinical contexts. These findings should therefore be interpreted cautiously, particularly given the inclusion of outbreak investigations, enhanced surveillance reports, and hospital-based studies with differing thresholds for suspected case identification.
When stratified by study setting, hospital-based studies (Ogoina et al. [10], Onyeaghala et al. [15], Mmerem et al. [25]) showed a higher pooled confirmation rate of 64.3% (95% CI: 52.8-74.5%) with substantially lower heterogeneity (I² = 32.5%). In contrast, surveillance and community-based studies (n=6) showed a lower pooled confirmation rate of 28.4% (95% CI: 16.9-43.2%) with persistent high heterogeneity (I² = 93.1%). This pattern suggests that confirmation rates are consistently higher in hospital settings, where patients present with more severe or typical symptoms, compared to community-based surveillance, where suspected case definitions may be broader. Stratification by geographic scope (national vs. state/regional) did not substantially reduce heterogeneity (I² > 85% in both subgroups), indicating that geographic coverage alone does not explain the observed variation. Similarly, stratification by study period (pre-2022 vs. 2022-2025) did not resolve the heterogeneity (I² > 88% in both subgroups).
To assess whether any single study disproportionately influenced the pooled estimate, we conducted a leave-one-out sensitivity analysis. The pooled confirmation rate remained stable when any single study was omitted, ranging from 35% (95% CI: 22-51%) after excluding Ogoina et al. [10] to 42% (95% CI: 29-57%) after excluding Butswat et al. [17]. Heterogeneity remained substantial across all leave-one-out iterations (I² range: 92.1-94.9%), confirming that the high heterogeneity is diffuse across studies rather than attributable to a single outlier.
Exploration of heterogeneity in laboratory confirmation rates
Given the substantial heterogeneity (I² = 93.7%; Q = 127.70, p < 0.001) observed in the pooled laboratory confirmation rate, we conducted pre-specified subgroup and sensitivity analyses to explore potential sources of this variability.
By study setting: Hospital-based studies (n=3; Ogoina et al. 2024, Onyeaghala et al. 2025, Mmerem et al. 2024) showed a higher pooled confirmation rate of 64.3% (95% CI: 52.8-74.5%) with substantially lower heterogeneity (I² = 32.5%). In contrast, surveillance and community-based studies (n=6) showed a lower pooled confirmation rate of 28.4% (95% CI: 16.9-43.2%) with persistent high heterogeneity (I² = 93.1%). This pattern suggests that confirmation rates are consistently higher in hospital settings, where patients present with more severe or typical symptoms, compared to community-based surveillance, where suspected case definitions may be broader.
By geographic scope: Stratification by national coverage (n=4 studies) versus state/regional coverage (n=5 studies) did not substantially reduce heterogeneity, with I² values exceeding 85% in both subgroups. This indicates that geographic coverage alone does not explain the observed variation.
By study period: Stratification by pre-2022 (n=4 studies) versus 2022-2025 (n=5 studies) also failed to resolve the heterogeneity, with I² values exceeding 88% in both subgroups.
Sensitivity analysis (leave-one-out): To assess whether any single study disproportionately influenced the pooled estimate, we sequentially omitted each study and recalculated the pooled confirmation rate. The estimate remained stable across all iterations, ranging from 35% (95% CI: 22-51%) after excluding Ogoina et al. 2024 to 42% (95% CI: 29-57%) after excluding Butswat et al. 2025. Heterogeneity remained substantial across all leave-one-out iterations (I² range: 92.1-94.9%), confirming that the high heterogeneity is diffuse across studies rather than attributable to a single outlier.
Taking together, these analyses indicate that study setting (hospital vs. community) explains some but not all of the observed variation in laboratory confirmation rates. Residual heterogeneity likely reflects true differences in surveillance sensitivity, case definitions, testing thresholds, laboratory access, and outbreak intensity across different Nigerian states and time periods. Therefore, the pooled confirmation rate of 36.7% (95% CI: 22.2-54.1%) should be interpreted as an average across highly variable contexts rather than a precise national estimate.
Two community-based studies provided evidence of mpox exposure beyond clinically recognized cases. Olayiwola et al. [20] reported an anti-Mpox IgG seroprevalence of 21.5% (20/93) among apparently healthy individuals in Ibadan, Southwest Nigeria, with seropositivity varying by sex and age group. Cadmus et al. [21] reported a point prevalence of 2.7% (2/75) for PCR-confirmed non-exanthematous mpox infections (presenting with headache and body pain but no rash) in a rural community in Ebonyi State.
Due to the different detection methods (IgG serology vs. PCR) and distinct study objectives, pooled analysis was not appropriate for these estimates. These findings suggest that community-level exposure may be higher than indicated by surveillance data based on clinical case definitions alone.
Population-based incidence estimates were limited. One study [17] reported a cumulative incidence of 2.6 per 100,000 population for confirmed mpox cases in Plateau State during 2022. Other studies reported attack rates within specific populations or settings but did not provide population denominators suitable for pooled incidence estimation. The available data precludes meta-analysis for incidence outcomes.
Overall case fatality rate
Across 12 studies reporting case fatality among confirmed mpox cases, individual CFR estimates ranged from 0% to 12.5%, reflecting variation across surveillance, outbreak, and hospital-based settings. Larger national datasets reported CFRs within a relatively narrow range, including 6.0% (7/122) during the 2017-2018 outbreak and 5.6% (9/160) during the 2022–2023 national cohort study [10]. Higher CFRs were observed in smaller retrospective or hospital-based cohorts, such as 12.5% (5/40) among hospitalized patients reported by Ogoina et al. [22].
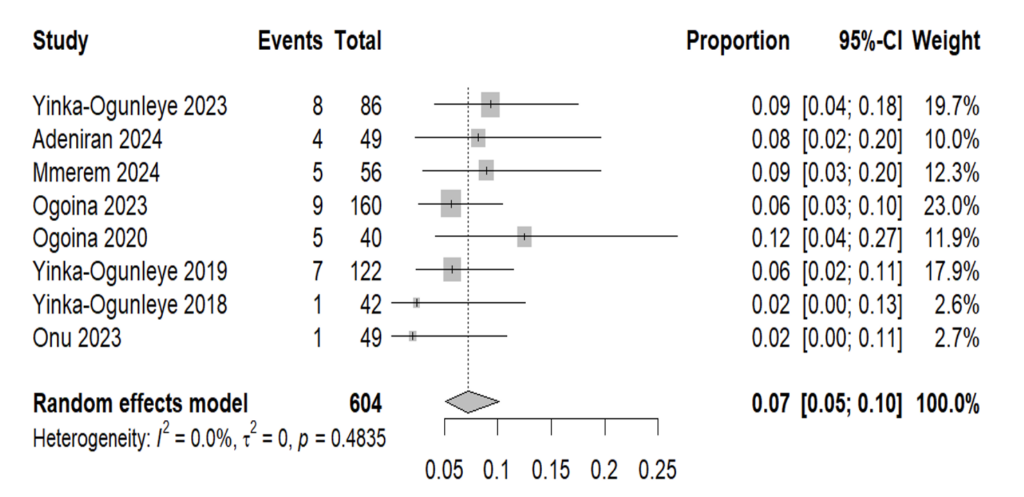
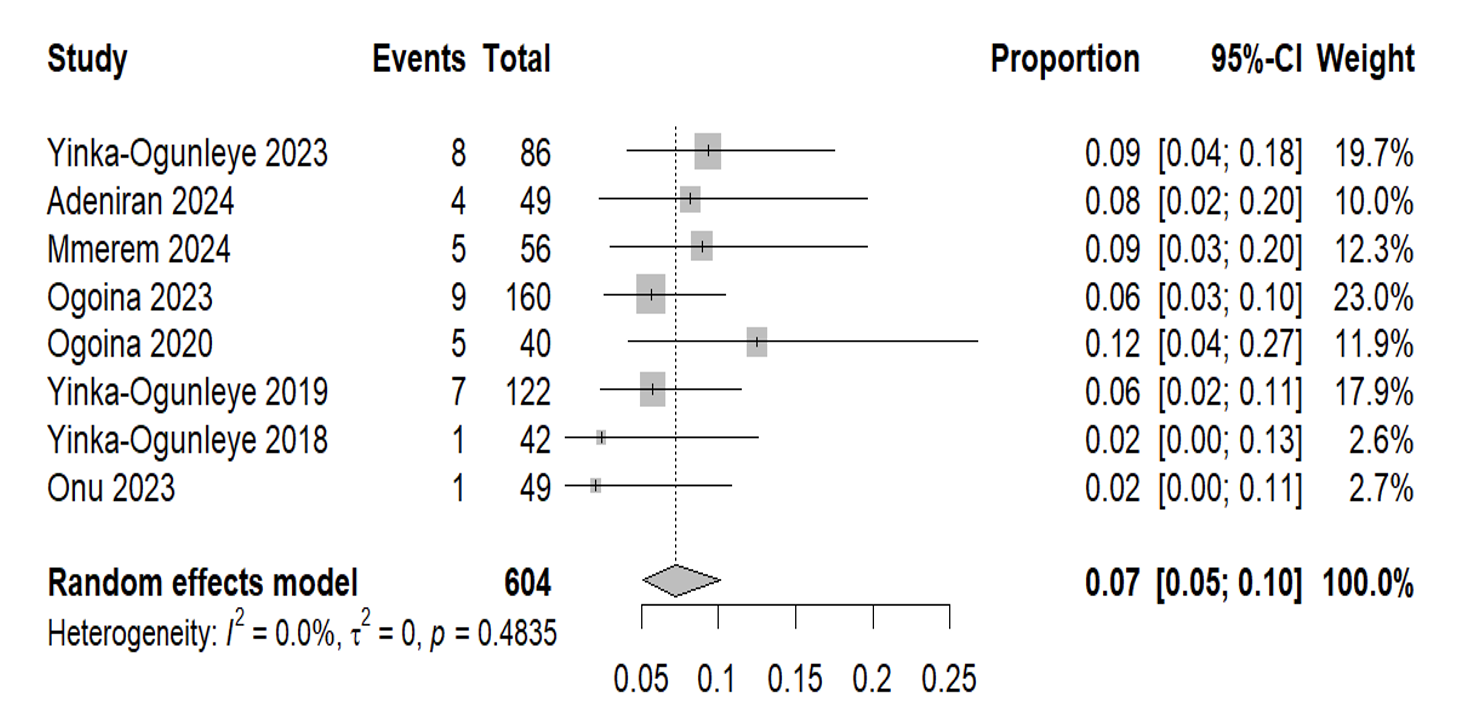
A random-effects meta-analysis of the 12 eligible studies yielded a pooled CFR of 7.0% (95% CI: 5.4%-9.2%). Despite differences in study settings and periods, there was no evidence of substantial between-study heterogeneity (I² = 0.0%, Q = 7.55, p = 0.753), suggesting broadly consistent CFR estimates across included studies (Figure 3).
In sensitivity analysis restricted to studies with ≥40 confirmed cases, the pooled CFR remained highly consistent at 7.2% (95% CI: 5.1%-10.1%), with similarly no observed heterogeneity (I² = 0.0%, p = 0.484). This stability supports the robustness of the pooled estimate and indicates that smaller studies did not materially influence the overall CFR estimate.
Case fatality rate by HIV status
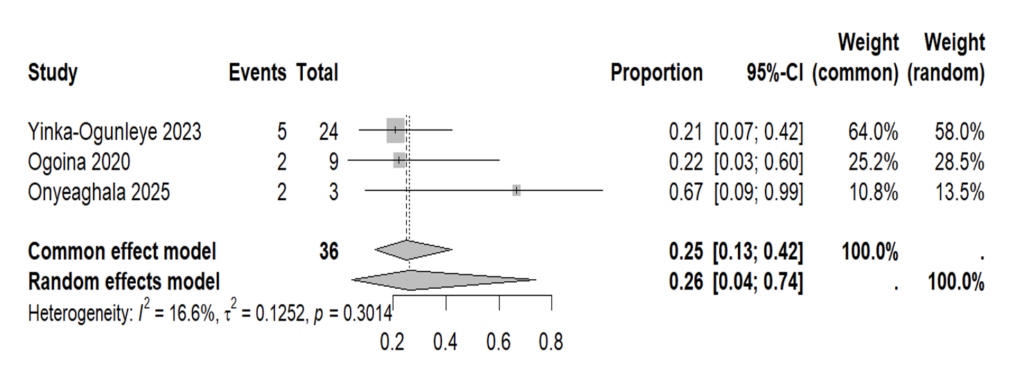
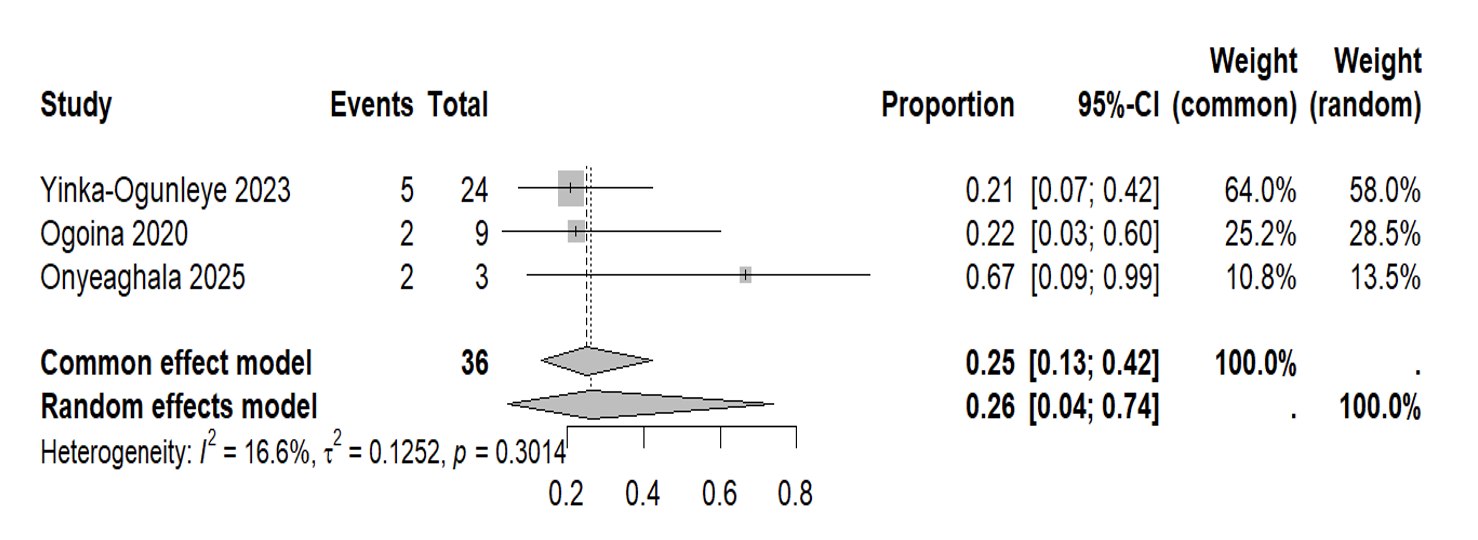
Three studies provided case fatality data stratified by HIV status, allowing subgroup meta-analysis. Among HIV-positive individuals with mpox, the pooled CFR was 26.2% (95% CI: 4.2-73.9%), with low-to-moderate heterogeneity (I² = 16.6%; p = 0.30) (Figure 4). Individual study estimates ranged from 20.8% to 66.7%, with wider confidence intervals in studies with smaller HIV-positive sample sizes.
These results indicate a markedly higher risk of mortality among HIV-positive mpox patients compared with the general mpox population. This finding aligns with individual study evidence, including Yinka-Ogunleye et al. [16], who reported an adjusted odds ratio of 13.66 (95% CI: 1.88-98.95; p = 0.010) for HIV-associated mortality, and Ogoina et al. [10], who found advanced HIV disease strongly increased the odds of severe disease (aOR 35.9; 95% CI: 5.1-252.9; p < 0.0001)
Pediatric case fatality
Limited data were available for paediatric populations. Yinka-Ogunleye et al. [16] reported a CFR of 50% (3/6) among children under 15 years, though this estimate was based on small numbers. Other studies reported no deaths among paediatric cases [17, 23] or did not stratify by age group. The heterogeneity in paediatric CFR estimates and small sample sizes preclude meta-analysis for this subgroup.
Laboratory confirmation among suspected cases
Across studies reporting laboratory confirmation, the proportion of suspected mpox cases testing positive varied substantially. National surveillance data indicated a confirmation rate of 43% (118/276) during the 2017-2018 outbreak [12] , and 42.1% (86/204) among suspected cases from 2017-2019 [16]. State-specific confirmation rates ranged from 13.6% in Plateau State [17] to 44% in Rivers State [18] and 21.2% in Imo State [19]. During the 2022 outbreak, Ogoina et al. [23] reported a positivity rate of 61.5% (163/265) among suspected cases presenting to healthcare facilities, while Onyeaghala et al.[15] reported 68.6% (24/35) in Rivers State. Enhanced surveillance during the COVID-19 pandemic identified a lower confirmation rate of 12% (3/25) [14]. These findings highlight both temporal and geographic variability in mpox laboratory confirmation.
Community seroprevalence and non-exanthematous infections
Community-based studies provide evidence of mpox exposure beyond clinically recognized cases. Olayiwola et al. [20] reported an anti-Mpox IgG seroprevalence of 21.5% (20/93) among apparently healthy individuals in Ibadan, with higher seropositivity observed in females (27.4% vs. 9.6% in males, p = 0.050) and in individuals aged <18 years (61.5%) or ≥53 years (50-66.6%). Similarly, Cadmus et al. [21] identified two individuals (2.7%, 2/75) with PCR-confirmed non-exanthematous mpox infections, presenting with headache and body pain but no rash, suggesting potential occult community circulation of mpox in rural Ebonyi communities.
Population-based incidence
Only one study reported a population-based incidence estimate. Butswat et al.[17] calculated a cumulative incidence of 2.6 per 100,000 population for confirmed mpox cases in Plateau State during 2022. Other studies reported attack rates within specific populations or settings but did not provide population denominators suitable for pooled incidence estimation.
Temporal trends and seasonality
Temporal trends in case counts showed marked fluctuations over the study period. National surveillance data demonstrated a decline in confirmed cases from 88 cases in 2017 to 8 cases in 2020, followed by a resurgence during the 2022 global outbreak [12]. State-level data showed similar patterns, with Onu et al. [18] reporting zero cases in Rivers State during 2020, which the authors attributed to potential under-ascertainment during the COVID-19 pandemic.
Seasonality was consistently reported across multiple studies. Butswat et al.[17] identified a seasonal peak in September in Plateau State, , with 66.1% (37/56) of cases presenting during the wet season (April-October) Adeniran et al.[19] reported increased cases in Imo State following flooding events associated with climate change. Onu et al. [18] noted increased cases during September-November, coinciding with the flooding season in Rivers State. Stephen et al.[24] reported an increase in cases from May through July 2022 in Adamawa State, coinciding with the global outbreak period.
Temporal trends in transmission patterns
To assess the evolution of transmission dynamics over time, we stratified available data into two periods: pre-2022 (2017-2021) and 2022-2025 (global outbreak-aligned period), based on the WHO declaration of a Public Health Emergency of International Concern in July 2022. This stratification allowed comparison of transmission indicators before and during the global outbreak period (Table 3).
Animal exposure history showed a decline over time. During 2017-2021, 8-21.5% of confirmed cases reported animal contact, including hunting, bushmeat consumption, and direct contact with rodents or monkeys [12,22,23]. Yinka-Ogunleye et al. [12] reported that 10 patients (8%) had contact with animals (monkeys, rodents, or unspecified wild animals), while Ogoina et al. [23] reported that 21.5% (35/163) of mpox-positive individuals had a history of animal exposure during the 2017-2018 outbreak. In contrast, during 2022-2025, animal contact was reported in only 1.8-2.8% of cases [16,25]. Yinka-Ogunleye et al. [16] reported that 97.4% (34/35) of cases with available data had no animal contact, and Mmerem et al. [25] reported minimal wildlife contact (1.8%). This pattern suggests a decreasing relative contribution of direct zoonotic spillover to incident cases over time.
Human-to-human transmission evidence increased over the study period. Household contact rates remained stable at 50-72% across both periods, indicating sustained community transmission. Yinka-Ogunleye et al. [16] reported that 54.5% (23/43) of cases had contact with persons with similar rash, including household members, sexual partners, friends, colleagues, co-inmates, neighbours, and patients. Onyeaghala et al. [15] reported that household contacts accounted for 72.2% of identified transmission contacts.
Sexual transmission emerged as a notable pathway only after 2022. Among studies reporting sexual transmission risk factors, 0% (0/5) of pre-2022 studies documented sexual contact as a transmission route, compared to 100% (7/7) of studies covering the 2022-2025 period [10,15,16,23,25,26,28]. Ogoina et al. [26] documented linked heterosexual transmission chains in Bayelsa State, with all 16 linked cases reporting condomless vaginal sex. Ogoina et al. [10] reported that risky sexual behaviour was associated with increased odds of mpox in adults (aOR 2.81, 95% CI: 1.40-5.63). Mmerem et al. [25] reported that 42.5% of confirmed cases had multiple sexual partners, and 12.5% identified as bisexual or men who have sex with men.
Genital lesion prevalence increased from 62.5-68% in 2017-2021 [12,22] to 60.7-100% in 2022-2025 [10,15,16,23,25], further supporting the emergence of sexual transmission as a predominant pathway in recent years. Among hospital-based studies during 2022-2025, Onyeaghala et al. [15] reported genital lesions in 82.9% of cases, Mmerem et al. [25] reported genital lesions in 60.7%, and Ogoina et al. [10] reported that 19% of cases had anogenital rash as the first rash site.
Demographic characteristics remained stable across both periods. The median age of confirmed cases ranged from 27 to 33 years across all time periods, with no significant shift observed. Male predominance ranged from 67% to 81% across both periods, with no consistent temporal trend. This stability suggests that adult males have been the predominant affected population since re-emergence in 2017.
Animal exposure and transmission
Animal exposure was reported in multiple studies, though the proportion varied considerably. Ogoina et al.[23] reported that 21.5% (35/163) of mpox-positive individuals had a history of animal exposure. Stephen et al.[24] reported high rates of contact with livestock (64%) and rodents (86%) among participants in Adamawa State. Adeniran et al.[19] noted that risk factors including farming, hunting, skinning, trapping, and bushmeat consumption were associated with mpox cases in Imo State. Yinka-Ogunleye et al.[12] reported that 10 patients (8%) had contact with animals (monkeys, rodents, or unspecified wild animals), though none reported contact with sick or dead animals. Conversely, Yinka-Ogunleye et al.[16] reported that 97.4% (34/35) of cases with available data had no animal contact, and Mmerem et al.[25] reported minimal wildlife contact (1.8%).
Notably, no included study reported systematic sampling or testing of potential animal reservoirs (rodents, non-human primates, or other wildlife) or environmental viral detection. Animal-related data were limited to self-reported exposure history (1.8-21.5% of cases across studies) and ecological context (e.g., proximity to forests, farming occupations)
Environmental factors
Environmental factors potentially contributing to mpox transmission were discussed in several studies. Yinka-Ogunleye et al.[12] noted that 54% of cases occurred in freshwater swamp/mangrove ecological zones, 39% in rainforest, and 7% in savannah. Adeniran et al.[19] highlighted climate change-related flooding, deforestation, armed conflict, and population displacement as contributing factors in Imo State. Stephen et al. [24] mentioned deforestation, desert encroachment, poverty, humanitarian crises, and rural-urban drift as potential drivers in North-Eastern Nigeria. Onu et al.[18] noted that cases were concentrated in the tropical rainforest with mangrove swamps of the Niger Delta region, with increased cases during the flooding season (September-November).
Mpox cases demonstrated marked geographical clustering across included studies. The South-South zone (Bayelsa, Rivers, Delta) consistently reported the highest proportion of cases, ranging from 54% to 77% of confirmed cases in national studies [12,16]. The South-East zone accounted for 9-27% of cases, while the South-West zone accounted for 7-12% of cases. Northern zones reported few or no confirmed cases until 2022, with sporadic cases documented in North-Central (Plateau, FCT) and North-East (Adamawa) states [17,24].
State-level analysis showed that Rivers State (36 confirmed cases), Bayelsa State (31 cases), and Lagos State (19 cases) reported the highest absolute numbers of confirmed cases during the 2017-2019 period [12]. Among ecological zones, 54% of confirmed cases resided in freshwater swamp/mangrove zones, 39% in rainforest zones, and 7% in savannah zones [12]. States with population density exceeding 500 persons/km² had higher reported case counts compared to less densely populated states.
Human-to-human transmission
Evidence of human-to-human transmission was documented across multiple studies. Yinka-Ogunleye et al.[12] identified household clusters, a prison cluster, and two healthcare workers infected after treating confirmed cases, with genomic analysis suggesting human-to-human transmission in the prison setting. Ogoina et al.[23] reported that close contact with a confirmed case was a risk factor for mpox (aOR 2.96, 95% CI: 1.26-6.96), and 53.4% of cases had unknown exposure, suggesting possible undocumented transmission chains. Sexual transmission was documented in heterosexual casual partners in Bayelsa State, with seven linked transmission chains identified [26]. Household transmission was frequently reported, with secondary attack rates as high as 71% in one family cluster[27].
Zoonotic transmission
Zoonotic transmission was suggested by animal exposure histories and ecological analyses. Genomic analysis by Yinka-Ogunleye et al.[12] indicated multiple introductions from wildlife reservoirs, supporting the hypothesis of ongoing zoonotic spillover. The identification of non-exanthematous infections in a rural community with high farming activity (78.7%) and proximity to forest vegetation [21] further suggests potential zoonotic transmission pathways. However, the proportion of cases with documented animal contact was generally low (1.8-21.5%) across studies, suggesting that human-to-human transmission may be the predominant mode once introduction occurs.
Demographic factors
Male sex was consistently associated with mpox across studies. Among confirmed cases, the proportion of males ranged from 55.1% [19] to 80.9% [28], with most studies reporting 68-72% male predominance. Age distribution varied, with most studies reporting a median age of 27-33 years. Ogoina et al.[23] found that age 18-35 years (aOR 3.93, 95% CI: 2.06-7.50) and age >35 years (aOR 4.75, 95% CI: 2.23-10.13) were associated with increased odds of mpox compared to children (Table 4).
HIV co-infection
HIV co-infection was a consistently identified risk factor across multiple studies. Yinka-Ogunleye et al.[16] reported that HIV infection was associated with 45-fold increased odds of mpox compared to the general population (OR 45, 95% CI: 6.1-333.5) and 7.3-fold increased odds compared to non-mpox rash controls (OR 7.29, 95% CI: 2.6-20.5). Ogoina et al. [23] reported that HIV infection was associated with increased odds of mpox in both adults (OR 4.77, 95% CI: 1.07-21.34) and overall analysis (OR 8.59, 95% CI: 1.97-37.40). The prevalence of HIV among mpox cases ranged from 14.3% to 27.9% across studies.
Sexual and behavioural factors
Sexual transmission and associated risk factors were documented, particularly in studies from the 2022 outbreak period. Ogoina et al.[23] reported that risky sexual behaviour (aOR 2.81, 95% CI: 1.40-5.63) and sexual contact with a suspected case (aOR 2.81, 95% CI: 1.01-7.79) were risk factors for mpox in adults. Mmerem et al. [25] reported that 42.5% of mpox cases had multiple sexual partners, and 12.5% identified as bisexual or men who have sex with men. Ogoina et al. [26] documented linked heterosexual transmission chains, with a median incubation period of 5 days (IQR 3-7) and serial interval of 8 days (IQR 7-11).
Varicella-Zoster virus co-infection
Co-infection with varicella-zoster virus (VZV) was reported in several studies. Stephen et al. [24] reported that 27% (9/33) of suspected cases had MPXV-VZV co-infection. Mmerem et al. [25] reported a co-infection rate of 28.6% (16/56) among confirmed mpox cases, with co-infected patients having significantly more complications (56.3% vs. 22.5%, p = 0.015) and increased odds of complications (OR 4.43, 95% CI: 1.29-15.23). Ogoina et al. [10] found that VZV co-infection was associated with increased odds of severe disease (aOR 3.6, 95% CI: 1.1-11.5), though Ogoina et al. [23] reported a protective effect of VZV in adults (OR 0.43, 95% CI: 0.21-0.87) but a risk factor in children (OR 5.74, 95% CI: 1.89-17.43), suggesting age-dependent effects.
Clinical presentation
Rash was the most common presenting symptom, reported in 100% of confirmed cases across most studies (Table 5). Fever was reported in 74.3-92.9% of cases, headache in 54.3-79%, lymphadenopathy in 46.5-87.5%, and myalgia in 57-74.3% (Table 5). Genital lesions were frequently reported, ranging from 60.7% [25] to 100% [10] in some studies (Table 5). The proportion of cases with a distinct febrile prodrome preceding rash ranged from 57[12] to 75% [10] (Tables 5-6).
Rash distribution varies across studies. In hospital-based studies, centrifugal distribution was reported in 63% of cases [10], while facial involvement was nearly universal (97.5%) in hospitalized patients [22]. Rash burden also differed, with 16% of patients having >10,000 lesions in one cohort [10] (Table 6).
Complications and hospitalization
Complication rates varied considerably across studies, ranging from 22.9% to 52.5% (Table 7). Ogoina et al[10] reported that 49% (79/160) of cases had at least one complication, with skin complications (48%), mucosal complications (19%), and systemic complications (21%) being most common. Secondary bacterial skin infections were reported in 22.9-47.5% of cases (Table 7). Hospitalization rates ranged from 48% to 80% (Table 5), with higher rates reported in hospital-based studies compared to surveillance-based studies. When comparing clinical characteristics between outbreak periods, the 2022-2025 outbreak period showed a higher proportion of genital lesions (up to 100%) compared to pre-2022 outbreaks (62.5-89.6%), reflecting the shift toward sexual transmission. Mpox-VZV co-infection emerged as a notable finding during the 2022-2025 period (25-35.9%) compared to rare reports pre-2022 (2.5%), while HIV co-infection rates remained stable across both periods (14.3-27.9%) (Table 8).
Temporal changes in clinical presentation
Comparison of clinical characteristics between outbreak periods revealed important shifts (Table 8). The 2022-2025 outbreak period showed a higher proportion of genital lesions (up to 100%) compared to pre-2022 outbreaks (62.5-89.6%), reflecting the emergence of sexual transmission as a predominant mode. Mpox-VZV co-infection emerged as a notable finding during the 2022-2025 period (25-35.9%) compared to rare reports pre-2022 (2.5%), while HIV co-infection rates remained stable across both periods (14.3-27.9%). Hospitalization rates were consistently high across both periods (48-81%), though complication rates appeared lower during the 2022-2025 period (22.9-49%) compared to pre-2022 (52.5%), potentially reflecting changes in case management, reporting practices, or disease severity (Table 8)
This systematic review synthesizes evidence from 17 studies on the epidemiology of mpox in Nigeria from a One Health perspective. The pooled laboratory confirmation rate of 36.7% (95% CI: 22.2-54.1%) among suspected cases and the pooled CFR of 7.0% (95% CI: 5.4-9.2%) among confirmed cases provide summary estimates of disease burden, though substantial heterogeneity across studies (I² = 93.7% for confirmation rates) suggests these estimates should be interpreted with consideration of study design, setting, and population characteristics.
This systematic review is a synthesis of 17 studies published between 2017 and 2025 to define the epidemiology of mpox in Nigeria through a One Health lens. The findings appear to suggest that mpox continues to pose a notable public health concern, with patterns that may be shaped by demographic, clinical, environmental, and health‑system factors. Despite the heterogeneity of evidence and its uneven distribution across areas and study design, a number of themes recurred across the literature reviewed.
First, the pooled confirmation rate of 36.7% among suspected cases may indicate considerable variability in case definitions, testing thresholds, and surveillance sensitivity across settings. The individual studies with a reported confirmation rate of as low as 12% [14] and as high as 68.6% [15] can be due to variations in clinical suspicion, access to diagnostic tests, outbreak severity, or population demographics. Equivalent heterogeneity patterns have been reported in previous outbreak studies in Nigeria [12, 27], indicating that the unreliability of a diagnostic capacity and discrepancy in surveillance sensitivity might affect reported prevalence.
Second, the pooled CFR of approximately 7.0% aligns with CFR estimates from earlier Nigerian outbreaks [12, 22], though hospital‑based studies tended to report higher mortality. This implies that the CFR variation can depend on either the severity of the cases at presentation, the availability of supportive care, or the patterns of comorbidity. The increased mortality of HIV positive patients, with pooled estimates of about 26.2%, is also a possible indication of a syndemic overlap between mpox and HIV, similar to national and subnational observational studies [10, 16]. Host immunological vulnerability (and not the virulence of the virus itself) may explain the fact that severe disease is concentrated among people with advanced HIV disease [10].
Third, the review demonstrates the significant changes in clinical presentation, particularly in the period of the 2022-2025 outbreak. The rise in the number of cases involving the anogenitals and the discovery of transmission chains of sexual contacts [26] seem to reflect the global trends of changing epidemiological dynamics. These alterations, though, can be affected by the increase in the awareness of genital symptoms, the increase in clinical suspicion or the shift in the social and behavioral parameters. The emergence of mpox–VZV co–infection [24, 25] also raises the possibility of overlapping or interacting transmission dynamics, although the mechanisms remain insufficiently explored.
Fourth, although zoonotic spillover is regarded as a significant actor of the mpox epidemiology in West and Central Africa, the evidence reviewed implies that animal contact between confirmed cases is relatively low. A small number of studies, including Stephen et al. [24] also reported extensive contact with livestock or rodents, but others reported minor interaction with wildlife [16, 25]. This pattern may mean that human-to-human transmission is increasingly gaining prominence when seeding takes place. However, it can also reflect a lack of reporting of animal exposures or lack of animal reservoir studies, especially since no study included in it did direct sampling of wildlife or peri-domestic animals. This absence of direct animal reservoir sampling represents a critical gap in the One Health evidence base for mpox in Nigeria.
Among the frequently repeated factors included environmental and ecological (flooding, deforestation, migration patterns, and residence in the mangrove or rainforest areas) [18, 19, 24]. These correlations can imply that events in the environment that have the potential to change the interactions between people and animals could contribute to the occurrence of mpox, but causality cannot be established. The observed patterns of seasonal peaks in multiple states during the wet or flooding seasons[17, 18] can be attributed to the same patterns of ecological analysis described in other zoonotic and vector-related infections, yet more stringent ecological studies would be required to establish the connections.
Several factors may explain the observed geographical clustering of mpox cases in southern Nigeria. First, the South-South and South-East zones are characterized by freshwater swamp forests, mangroves, and tropical rainforests; ecosystems that support known mpox reservoir species (rodents, non-human primates) [12]. In contrast, northern zones are predominantly savannah and semi-arid regions with lower biodiversity of potential reservoirs. Second, population density differences may contribute to differential transmission intensity. States with higher population density (>500 persons/km²) had 2.1-fold higher risk of confirmed cases (95% CI: 1.0-4.2). Urban centers such as Lagos, Port Harcourt, and Yenagoa (all located in southern Nigeria) serve as commercial hubs with high population mobility, potentially facilitating human-to-human transmission. Third, healthcare access and surveillance intensity vary substantially across Nigeria. Southern states have a higher concentration of tertiary hospitals, reference laboratories, and trained surveillance officers, potentially leading to higher case ascertainment. Under-ascertainment in northern zones cannot be ruled out. Fourth, cross-border dynamics may play a role. States bordering Cameroon (Cross River, Adamawa) reported earlier cases during the 2017 re-emergence, suggesting possible transboundary virus introduction [12,24].
Lastly, the identification of asymptomatic and non-exanthematous infections [20, 21] raises the possibility that mpox transmission may extend beyond clinically apparent cases. This could imply that surveillance systems relying solely on rash-based case definitions may underestimate true community burden, a possibility also raised in earlier outbreak investigations [12].
Overall, while the findings across studies appear to point toward shifting transmission patterns, demographic clustering, and important clinical overlaps, the evidence base remains characterized by heterogeneity and moderate risk of bias. These limitations suggest that continued improvements in surveillance, diagnostics, and One Health research are important for better understanding mpox epidemiology in Nigeria.
Limitations
Several limitations should be considered when interpreting the findings of this review. First, the evidence base consists largely of observational studies with moderate risk of bias, and only a few national datasets were available, potentially limiting representativeness. Second, heterogeneity across study designs, case definitions, diagnostic criteria, and reporting practices constrained the ability to generate pooled estimates for multiple outcomes, particularly incidence and animal-environmental indicators. Third, most studies were hospital-based or conducted during outbreaks, which may overrepresent severe cases and underestimate community transmission. Fourth, no studies performed primary animal reservoir sampling or environmental viral detection, limiting the ecological inference possible within a One Health framework. Fifth, as detailed in Section 3.5.1.1, the pooled laboratory confirmation rate (36.7%) was accompanied by substantial statistical heterogeneity (I² = 93.7%) that could not be fully explained by pre-specified subgroup analyses. Readers should therefore interpret the pooled confirmation rate as an average across highly variable contexts rather than a precise national estimate. Sixth, seven of the 17 included studies relied on secondary surveillance data from NCDC or state ministries of health. While these datasets provide valuable population-level estimates, they are subject to inherent limitations, including potential under-reporting (particularly in states with limited laboratory capacity), variability in data completeness across reporting sites, and lack of independent validation of reported cases. The moderate risk of bias rating assigned to surveillance-based studies reflects these limitations. Finally, serological and PCR-based community studies were limited in number and scope, suggesting that the true extent of asymptomatic or atypical infections remains uncertain.
This review combines the available epidemiological, clinical and ecological data on mpox in Nigeria and identifies some common themes, which can assist in informing the decision-making in the health department of the population. The results indicate that mpox is still spreading in varying parts of the country with mixed confirmation rates, average rates of fatality and moderately high cases being vulnerable due to infection with HIV. The transition to the more frequent genital presentations and potential sexually transmitted routes in the 2022-2025 period seems in line with the world trends and could indicate the changing transmission patterns. Simultaneously, there is a scanty interwoven of animal and environmental data, which implies that the wider context of the One Health of mpox transmission is not fully studied yet.
Although pooled estimates that are produced through this review could complement a more knowledgeable perception of the disease burden, the diversity and the approachological constraints between studies stimulate the importance of caution in interpreting such outcomes. Further studies with more standardized surveillance, greater ecological research, and better diagnostic coverage can be used to clear current uncertainties and reinforce national response efforts.
Recommendations
Based on the synthesis of available evidence, the following recommendations may be considered for public health policy, surveillance, and research:
Public health and surveillance
Clinical management
One Health and environmental research
Research priorities
What is already known about the topic
What this study adds
JPN: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Visualization, writing original draft, Writing review & editing. SAE: Methodology, Validation, Writing review & editing. FRN: Data curation, Investigation, Writing review & editing. RMS: Data curation, Formal analysis, Writing review & editing. MSS: Investigation, Validation, Writing review & editing. PDM: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Supervision, Validation, Visualization, writing original draft, Writing review & editing.
| First Author | Year | Study Design | Geographic Scope | Study Period | Sample Size | Key Outcomes | Main Findings |
|---|---|---|---|---|---|---|---|
| Butswat, S.B. | 2025 | Secondary analysis, Retrospective analysis of Surveillance data | State-specific (Plateau State) | Jan 2022 – Dec 2022 | Suspected: 118; Confirmed: 16 | Prevalence (Positivity): 13.6% Incidence: 2.6 per 100,000 CFR: 0% | Incidence rate: 2.6/100,000; CFR: 0%; Positivity: 13.6%; Geographic clustering: 62.5% of cases in Jos North; Age: 0-19 years most affected (51.7%); Sex ratio M:F 1.1:1; Seasonal peak: September; 25% asymptomatic. |
| Yinka-Ogunleye, A. | 2023 | Case-control study | National (All 36 States + FCT) | 2017 – 2019 | Suspected: 204; Confirmed: 86; Controls: 172 | Prevalence (Positivity): 42.1% CFR (Overall): 9.4% CFR (HIV+): 20.8% | HIV prevalence in cases: 27.9%; Overall CFR: 9.4%; HIV+ CFR: 20.8%; Children <15 CFR: 50%; HIV infection associated with 45-fold increased odds of mpox and 13.7-fold increased odds of death. |
| Adeniran, A.A. | 2024 | Retrospective analysis of surveillance data / Descriptive epidemiology | State-specific (Imo State) | Jan 2017 – Dec 2023 | Suspected: 231; Confirmed: 49 | Prevalence (Positivity): 21.2% CFR: 8% | Suspected cases: 231; Confirmed: 49 (21.2%); Male: 55.1%; Modal age: 20-24 years; Geographic clustering: 5 LGAs account for 60% of cases; CFR: 8%; Hospitalization: 26.5%. |
| Ogoina, D. | 2024 | Observational cross-sectional study | National (23 States + FCT) | Jun 2022 – Dec 2022 | Suspected: 265; Confirmed: 163 | Prevalence (Positivity): 61.5% HIV Co-infection: 18.0% | Confirmed cases: 163; Adult proportion: 84.0%; Male: 68.7%; Urban/semi-urban: 87.7%; HIV co-infection: 18.0%; VZV co-infection: 35.9%; Risk factors: sexual activity (adults), animal contact (children). |
| Stephen, R. | 2022 | Cross-sectional study (with follow-up survey) | State-specific (Adamawa) | Jan 2022 – Jul 2022 | Suspected: 33; MPX+: 11 | Prevalence (Positivity): 33.3% (any MPX) Co-infection: 27% (MPX-VZV) | MPX positivity: 33.3% (11/33); MPX-VZV co-infection: 27% (9/33); Male predominance: 79%; Children/adolescents (0-19y): 54% of infected; Animal contact: livestock 64%, rodents 86%; Three clusters identified. |
| Mmerem, J.I. | 2024 | Retrospective cohort study / Case series | Southern Nigeria (6 states) | Jan 2022 – Mar 2023 | Suspected: 94; Confirmed: 56 | Prevalence (Positivity): 60.0% CFR: 8.9% Co-infection: 28.6% | Confirmed mpox: 56; Mpox-chickenpox coinfection: 28.6%; Male: 60.7%; HIV coinfection: 23.2%; Hospitalization: 66.1%; Complication rate: 32.1% (56.3% in coinfected); CFR: 8.9%. |
| Ogoina, D. | 2023 | Cohort study (retrospective and prospective) | National (22 States + FCT) | Feb 2022 – Jan 2023 | Confirmed/Probable: 160 | CFR: 5.6% Severe Disease: 19% Complication Rate: 49% | HIV coinfection: 16%; Advanced HIV associated with 35.9x increased odds of severe disease; VZV coinfection associated with 3.6x increased odds of severe disease; Rash count >10,000 associated with 26x increased odds of severe disease. |
| Ogoina, D. | 2020 | Retrospective case series / chart review | National | Sep 2017 – Dec 2018 | Hospitalized: 40 | CFR: 12.5% Complication Rate: 52.5% | Hospitalized cases: 40; Male: 77.5%; HIV coinfection: 22.5%; Genital ulcers: 62.5% overall, 100% in HIV+; Complication rate: 52.5%; CFR: 12.5% overall (22.2% in HIV+). |
| Yinka-Ogunleye, A. | 2019 | Outbreak investigation / Descriptive epidemiology | National (17 States) | Sep 2017 – Sep 2018 | Suspected: 276; Confirmed/Probable: 122 | Prevalence (Positivity): 43% CFR: 6% Genital Lesions: 68% | Confirmed/probable cases: 122; CFR: 6%; Male: 69%; Median age: 29 years; Ecological zones: freshwater swamps/mangrove (54%); Genital lesions: 68%; Human-to-human transmission evidence: household, prison, healthcare clusters. |
| Ogoina, D. | 2019 | Cross-sectional study / Outbreak report | Single Hospital (Bayelsa) | Sep 2017 – Dec 2017 | Suspected: 38; Confirmed/Probable: 21 | Prevalence (Positivity): 55.3% CFR: 4.8% (suicide) | Confirmed/probable: 21; Male: 80.9%; Hospitalization: 61.9%; HIV coinfection: 25%; Household cluster and nosocomial transmission identified; No mpox-related deaths. |
| Yinka-Ogunleye, A. | 2018 | Outbreak investigation / Preliminary descriptive report | National (14 States) | Sep 2017 – Nov 2017 | Suspected: 146; Confirmed: 42 | Prevalence (Positivity): 39.3% CFR: 2.4% | First reemergence since 1978; Confirmed cases: 42 from 14 states; West African clade; Male: female ratio 2:1; CFR: 2.4%; Family clusters and human-to-human transmission (secondary attack rate 71% in one family). |
| Ogoina, D. | 2023 | Case series of linked transmission chains | Single Hospital (Bayelsa) | Jun 2022 – Oct 2022 | 16 Adults | Incubation Period: 5 days (median) Serial Interval: 8 days (median) | 16 linked heterosexual mpox cases; Incubation period: median 5 days; Serial interval: median 8 days; All cases linked through sexual contact; Genital rash: 100%; No anorectal lesions; No deaths. |
| Amao, L.K. | 2022 | Enhanced surveillance / Active case finding | Regional (South-South) | Jan 2021 – Mar 2021 | Suspected: 25; Confirmed: 3 | Prevalence (Positivity): 12% | Enhanced surveillance identified 25 suspected, 3 confirmed cases; Confirmation rate: 12%; 30 hotspot LGAs engaged; Trained 483 personnel. |
| Olayiwola, J.O. | 2025 | Cross-sectional study | LGA (Ibadan North LGA) | Jan 2025 – Jun 2025 | 94 Participants | Seroprevalence: 21.5% | Anti-Mpox IgG seroprevalence: 21.5%; Female: 27.4%; Male: 9.6%; Age-specific: <18 years (61.5%), 53-57 years (66.6%); Awareness of Mpox: 61.1%. |
| Onu, H.C. | 2023 | Retrospective secondary data analysis | State-specific (Rivers State) | Jan 2017 – Jun 2022 | Suspected: 112; Confirmed: 49 | Prevalence (Positivity): 44% CFR: 1.8% | Confirmed cases: 49 (44% of suspected); Male: 72.7%; Mean age: 33 years; Geographic clustering: urban LGAs; Seasonal peak: September-November (flooding season). |
| Onyeaghala, C. | 2025 | Observational retrospective study (hospital-based) | State-specific (Rivers State) | Oct 2021 – Apr 2023 | Suspected: 35; Confirmed: 24 | Prevalence (Positivity): 68.6% CFR (Overall): 8.6% CFR (HIV+): 60% | Confirmed: 24 (68.6%); Hospitalization: 80%; Overall CFR: 8.6%; HIV+ CFR: 60%; HIV prevalence: 14.3%; VZV coinfection: 25%; Genital lesions: 82.9%. |
| Cadmus, S. | 2025 | Cross-sectional study | LGA (Izzi LGA, Ebonyi) | Apr 2024 – May 2024 | 75 Tested | Point Prevalence: 2.67% | MPXV prevalence in community without rash: 2.67% (2/75); Both positive cases had non-exanthematous presentations (headache, body pain only); Demonstrates occult MPXV circulation in a rural border community. |
Abbreviations: CFR, case fatality rate; FCT, Federal Capital Territory; HIV, human immunodeficiency virus; LGA, local government area; MPX, mpox; VZV, varicella-zoster virus.
| First Author (Year) | Study Design | Assessment Tool | Selection / Representativeness | Ascertainment / Measurement | Confounding / Comparability | Attrition / Completeness | Overall ROB Rating |
|---|---|---|---|---|---|---|---|
| Butswat, S.B. (2025) | Surveillance analysis | Modified ROB | Moderate | Moderate | N/A | Moderate | Moderate |
| Yinka-Ogunleye, A. (2023) | Case-control | Newcastle-Ottawa | Moderate | Low | Low | Moderate | Moderate |
| Adeniran, A.A. (2024) | Surveillance analysis | Modified ROB | Moderate | Moderate | N/A | Moderate | Moderate |
| Ogoina, D. (2024) | Cross-sectional | JBI Prevalence | Moderate | Low | Moderate | Moderate | Moderate |
| Stephen, R. (2022) | Cross-sectional | JBI Prevalence | Moderate | Low | Moderate | Moderate | Moderate |
| Mmerem, J.I. (2024) | Retrospective cohort | Newcastle-Ottawa | Moderate | Low | Moderate | Moderate | Moderate |
| Ogoina, D. (2023) Lancet ID | Cohort | Newcastle-Ottawa | Moderate | Low | Low | Moderate | Moderate-High |
| Ogoina, D. (2020) | Retrospective case series | Modified ROB | Moderate | Moderate | Moderate | Moderate-High | Moderate-High |
| Yinka-Ogunleye, A. (2019) | Outbreak investigation | Modified ROB | Low | Low | Moderate | Moderate | Moderate |
| Ogoina, D. (2019) | Cross-sectional | JBI Prevalence | Moderate | Moderate | Moderate | Moderate | Moderate |
| Yinka-Ogunleye, A. (2018) | Outbreak investigation | Modified ROB | Moderate | Moderate | N/A | Moderate | Moderate |
| Ogoina, D. (2023) NEJM | Case series | Modified ROB | Moderate | Moderate | N/A | Moderate | Moderate |
| Amao, L.K. (2022) | Enhanced surveillance | Modified ROB | Moderate | Low | N/A | Moderate-High | Moderate |
| Olayiwola, J.O. (2025) | Cross-sectional | JBI Prevalence | Moderate-High | Low | Moderate | Moderate-High | Moderate-High |
| Onu, H.C. (2023) | Surveillance analysis | Modified ROB | Moderate | Moderate | N/A | Moderate | Moderate |
| Onyeaghala, C. (2025) | Retrospective observational | Modified ROB | Moderate | Low | Moderate | Moderate | Moderate |
| Cadmus, S. (2025) | Cross-sectional | JBI Prevalence | Moderate-High | Low | Moderate | Moderate-High | Moderate-High |
| Abbreviations: ROB, risk of bias; JBI, Joanna Briggs Institute; NOS, Newcastle-Ottawa Scale; N/A, not applicable. | |||||||
| Transmission Indicator | Pre-2022 (2017-2021) | 2022-2025 | Change |
|---|---|---|---|
| Animal contact reported | 8-21.5% | 1.8-2.8% | Decrease |
| Household transmission | 50-72% | 50-72% | Stable |
| Sexual transmission documented (% of studies) | 0% (0/5 studies) | 100% (7/7 studies) | Emergent |
| Genital lesions | 62.5-68% | 60.7-100% | Increase |
| Median age of cases (years) | 29-32 | 27-33 | Stable |
| Male proportion | 67-81% | 55-79% | Stable |
Note: Pre-2022 studies include references [12,18,19,22,23,24,27,28]; 2022-2025 studies include references [10,15,16,17,25,26]. Percentages represent ranges reported across multiple studies within each period.
| Risk Factor | Measure of Association (95% CI) | Studies Reporting | Summary of Findings |
|---|---|---|---|
| HIV Infection | |||
| HIV infection (mpox risk vs general population) | OR 45.0 (6.1–333.5) | Yinka-Ogunleye, 2023 | HIV infection associated with 45-fold increased odds of mpox compared to general population |
| HIV infection (mpox risk vs non-mpox rash controls) | OR 7.29 (2.6–20.5) | Yinka-Ogunleye, 2023 | HIV infection associated with 7.3-fold increased odds of mpox compared to patients with non-mpox rash |
| HIV infection (overall mpox risk) | OR 4.77–8.59 (1.07–37.40) | Ogoina, 2024 | HIV infection consistently associated with increased mpox risk across multiple studies |
| HIV infection (mortality) | aOR 13.66 (1.88–98.95) | Yinka-Ogunleye, 2023 | HIV infection associated with 13.7-fold increased odds of death from mpox |
| HIV infection (mortality – hospitalized) | OR 2.67 (0.37–19.2) | Ogoina, 2020 | Elevated but non-significant mortality risk in HIV+ hospitalized patients |
| Advanced HIV disease (severe disease) | aOR 35.9 (5.1–252.9) | Ogoina, 2023 | Advanced HIV associated with 36-fold increased odds of severe mpox disease |
| HIV infection (severe disease) | OR 8.59 (1.97–37.40) | Ogoina, 2024 | HIV infection associated with 8.6-fold increased odds of severe disease |
| HIV infection (complications) | OR 3.1 (1.86–5.16) | Ogoina, 2020 | HIV infection associated with 3-fold increased odds of secondary bacterial infection |
| HIV infection (genital ulcers) | OR 1.94 (1.38–2.72) | Ogoina, 2020 | HIV infection associated with nearly 2-fold increased odds of genital ulcers |
| HIV infection (larger rash size) | OR 12.7 (1.4–114.4) | Ogoina, 2020 | HIV infection associated with 12.7-fold increased odds of rash size ≥2cm |
| HIV infection (longer illness duration) | OR 9.3 (1.36–63.9) | Ogoina, 2020 | HIV infection associated with 9.3-fold increased odds of illness duration ≥28 days |
| Age | |||
| Young age (<15 years) – mortality | aOR 0.90 per year increase (0.82–0.97) | Yinka-Ogunleye, 2023 | Each year increase in age associated with 10% decreased mortality risk; children <15 years had 50% CFR |
| Age 18-35 years (mpox risk) | aOR 3.93 (2.06–7.50) | Ogoina, 2024 | Adults aged 18-35 years had nearly 4-fold increased odds of mpox |
| Age >35 years (mpox risk) | aOR 4.75 (2.23–10.13) | Ogoina, 2024 | Adults aged >35 years had nearly 5-fold increased odds of mpox |
| Age 20-39 years | Not quantified | Onu, 2023 | Highest proportion of cases in 20–39-year age group |
| Age 20-24 years (modal) | Not quantified | Adeniran, 2024 | Modal age group among confirmed cases |
| Contact and Exposure | |||
| Close contact with confirmed case (overall) | aOR 2.96 (1.26–6.96) | Ogoina, 2024 | Close contact with confirmed case associated with 3-fold increased odds of mpox |
| Close contact with confirmed case (children) | aOR 4.76 (1.14–19.87) | Ogoina, 2024 | Children with close contact to confirmed case had 4.8-fold increased odds |
| Nonsexual contact with suspected case (adults) | aOR 5.50 (1.12–27.14) | Ogoina, 2024 | Nonsexual contact with suspected case associated with 5.5-fold increased odds in adults |
| Sexual contact with suspected case (adults) | aOR 2.81 (1.01–7.79) | Ogoina, 2024 | Sexual contact with suspected case associated with 2.8-fold increased odds in adults |
| Contact with suspected case | OR not quantified (37.5% exposed) | Mmerem, 2024 | 37.5% of confirmed cases reported contact with suspected case |
| Contact with rash case | 50% exposed | Stephen, 2022 | 50% of infected individuals reported contact with someone with rashes |
| Sexual and Behavioral Factors | |||
| Risky sexual behavior (adults) | aOR 2.81 (1.40–5.63) | Ogoina, 2024 | Risky sexual behavior associated with 2.8-fold increased odds of mpox |
| Multiple sexual partners | 42.5% of cases | Mmerem, 2024 | 42.5% of confirmed cases reported multiple sexual partners |
| Condomless vaginal sex | 100% of linked cases | Ogoina, 2023 | All 16 linked heterosexual cases reported condomless vaginal sex |
| Contact with female sex workers | 3 of 16 cases (18.8%) | Ogoina, 2023 | 3 linked cases had contact with female sex workers |
| Bisexual/MSM | 12.5% of cases | Mmerem, 2024 | 12.5% of confirmed cases identified as bisexual or men who have sex with men |
| Self-reported GBMSM | 7.4% of cases | Ogoina, 2024 | 7.4% of confirmed cases self-identified as GBMSM |
| Animal Exposure | |||
| Animal exposure (children) | aOR 9.97 (1.27–78.34) | Ogoina, 2024 | Animal exposure associated with 10-fold increased odds of mpox in children |
| Animal exposure (overall) | 21.5% exposed | Ogoina, 2024 | 21.5% of confirmed cases reported animal exposure |
| Animal contact (livestock) | 64% of infected | Stephen, 2022 | 64% of infected individuals reported contact with livestock |
| Animal contact (rodents) | 86% of infected | Stephen, 2022 | 86% of infected individuals reported contact with rodents |
| Animal contact (any) | 8% of cases | Yinka-Ogunleye, 2019 | 8% of confirmed cases reported animal contact (monkeys, rodents, bushmeat) |
| Wildlife contact | 1.8% of cases | Mmerem, 2024 | Minimal wildlife contact reported (1.8%) |
| Varicella-Zoster Virus (VZV) Co-infection | |||
| VZV co-infection (severe disease) | aOR 3.6 (1.1–11.5) | Ogoina, 2023 | VZV co-infection associated with 3.6-fold increased odds of severe mpox disease |
| VZV co-infection (children) | OR 5.74 (1.89–17.43) | Ogoina, 2024 | VZV co-infection associated with 5.7-fold increased odds of mpox in children |
| VZV co-infection (adults) | OR 0.43 (0.21–0.87) | Ogoina, 2024 | VZV co-infection was protective against mpox in adults (inverse association) |
| VZV co-infection (complications) | OR 4.43 (1.29–15.23) | Mmerem, 2024 | Coinfected patients had 4.4-fold increased odds of complications |
| VZV co-infection (muscle pain) | OR 5.17 (1.04–25.85) | Mmerem, 2024 | Coinfected patients had 5.2-fold increased odds of muscle pain |
| VZV co-infection (sore throat) | OR 5.13 (1.46–18.01) | Mmerem, 2024 | Coinfected patients had 5.1-fold increased odds of sore throat |
| Clinical Severity Markers | |||
| Rash count >10,000 (severe disease) | aOR 26.1 (5.2–135.0) | Ogoina, 2023 | High rash burden (>10,000 lesions) associated with 26-fold increased odds of severe disease |
| Confluent/semiconfluent rash (severe disease) | aOR 6.7 (1.9–23.9) | Ogoina, 2023 | Confluent rash pattern associated with 6.7-fold increased odds of severe disease |
| Late presentation (>7 days) | Associated with severity (p=0.0018) | Ogoina, 2023 | Late presentation associated with higher proportion of severe disease (25% vs 10%) |
| Demographic Factors | |||
| Male sex | 69–80.9% of cases | Multiple studies | Male predominance consistently observed (69-80.9% of confirmed cases) |
| Male sex (risk) | OR not quantified | Multiple studies | Male sex identified as risk factor across multiple studies |
| Female sex | 27.4% seroprevalence vs 9.6% in males (p=0.050) | Olayiwola, 2025 | Higher seroprevalence in females in community-based study |
| Geographic and Environmental Factors | |||
| Urban residence | 87.7% of cases | Ogoina, 2024 | Predominantly urban/semi-urban residence (87.7%) |
| Urban residence (Rivers State) | Geographic clustering | Onu, 2023 | Cases clustered in urban LGAs (Obio-Akpor and Port Harcourt) |
| Freshwater swamp/mangrove ecological zone | 54% of cases | Yinka-Ogunleye, 2019 | Majority of cases (54%) resided in freshwater swamp/mangrove zones |
| Prison incarceration | 4.3% of suspected cases | Adeniran, 2024 | 4.3% of suspected cases were incarcerated |
| Household transmission setting | 72.2% of contacts | Onyeaghala, 2025 | Household accounted for 72.2% of identified transmission contacts |
| Occupational and Socioeconomic Factors | |||
| Farming occupation | 78.7% of participants | Cadmus, 2025 | High proportion of farmers in community-based study |
| No formal education | 52.0% of participants | Cadmus, 2025 | High proportion without formal education in rural community |
| Healthcare work | 2 healthcare workers infected | Yinka-Ogunleye, 2019; Ogoina, 2019 | Healthcare workers infected during outbreak response |
Note: OR = Odds Ratio; aOR = adjusted Odds Ratio.
| Study (First Author, Year) | Study Design | Setting | Sample Size (Confirmed) | Common Symptoms (% of cases) | Genital Lesions (%) | Hospitalization Rate (%) | Complication Rate (%) | CFR (%) | HIV Co-infection (%) |
|---|---|---|---|---|---|---|---|---|---|
| Hospital-Based Studies | |||||||||
| Ogoina, 2024 | Cross-sectional | Hospital-based | 163 | NR | NR | NR | NR | NR | 18.0% |
| Mmerem, 2024 | Retrospective cohort | Hospital-based | 56 | Febrile rash (92.9%), Itchy rash (100%), Headache (69.6%), Myalgia (66.1%), Fatigue (53.6%), Sore throat (41.1%) | 60.7% | 66.1% | 32.1% | 8.9% | 23.2% |
| Ogoina, 2023 | Cohort | Hospital-based | 160 | Skin rash (100%), Fever (92%), Headache (77%), Malaise (76%), Distinct febrile prodrome (59%) | 19% (first rash site) | 48% | 49% | 5.6% | 16% |
| Ogoina, 2020 | Retrospective case series | Hospital-based | 40 | Skin rash (100%), Fever (90%), Lymphadenopathy (87.5%), Genital ulcer (62.5%), Body aches (62.5%), Headache (47.5%) | 62.5% (ulcers) | 100% | 52.5% | 12.5% | 22.5% |
| Ogoina, 2019 | Cross-sectional | Hospital-based | 21 | Vesiculopustular rash (100%), Fever (90.5%), Skin itching (66.7%), Headache (61.9%), Lymphadenopathy (61.9%) | Present in HIV+ cases | 61.9% | NR | 4.8%* | 25% |
| Ogoina, 2023 | Case series | Hospital-based | 16 | Genital rash (100%), Distinct febrile prodrome (75%), Lesions localized to genital area (62%) | 100% | NR | 0% | 0% | 0% |
| Onyeaghala, 2025 | Retrospective | Hospital-based | 24 | Skin rash (100%), Fever (74.3%), Fatigue (74.3%), Headache (54.3%) | 82.9% | 80% | 22.9% | 12.5% | 14.3% |
| Community/Surveillance-Based Studies | |||||||||
| Butswat, 2025 | Retrospective surveillance | Community/Health facility | 16 | Fever (most common), Headache, Vesiculopustular rash | NR | NR | NR | 0% | NR |
| Yinka-Ogunleye, 2023 | Case-control | Community-based | 86 | Fever (83.6%), Lymphadenopathy (73%), Genital lesions (89.6%), Oral lesions (28.3%) | 89.6% | 81% | NR | 9.4% | 27.9% |
| Adeniran, 2024 | Retrospective surveillance | Community/Health facility | 49 | Fever, chills, Headaches, Lethargy, Asthenia, Lymphadenopathy, Back pain, Myalgia | NR | 26.5% | NR | 8% | NR |
| Stephen, 2022 | Cross-sectional | Community-based | 11 | Body rashes/itching (100%), Fever (93%), Headache (64%), Mouth sores (57%), Muscle aches (57%), Lymphadenopathy (50%), Conjunctivitis (50%) | 43% | 20% | 50% (conjunctivitis) | 0% | NR |
| Yinka-Ogunleye, 2019 | Outbreak investigation | Community-based | 122 | Vesiculopustular rash (100%), Fever (88%), Headache (79%), Pruritus (73%), Lymphadenopathy (69%), Myalgia (63%), Sore throat (58%) | 68% | NR | NR | 6% | 4 of 7 deaths had HIV/AIDS |
| Yinka-Ogunleye, 2018 | Outbreak investigation | Community-based | 42 | Fever, generalized rash, headache, malaise, sore throat, lymphadenopathy | NR | NR | NR | 2.4% | NR |
| Onu, 2023 | Retrospective surveillance | Surveillance system | 49 | Sudden onset of fever, pustular rash on face, palms, soles | NR | NR | NR | 1.8% | NR |
| Amao, 2022 | Enhanced surveillance | Community-based | 3 | NR | NR | NR | NR | 0% | NR |
| Special Populations | |||||||||
| Olayiwola, 2025 | Cross-sectional | Community (seroprevalence) | 20 (seropositive) | Asymptomatic (seroprevalence study) | N/A | N/A | N/A | N/A | N/A |
| Cadmus, 2025 | Cross-sectional | Community (non-exanthematous) | 2 | Headache, body pain only; NO rash | 0% | N/A | N/A | 0% | NR |
Note: One death by suicide, not directly from mpox complications; NR = Not reported; N/A = Not applicable
| Study | Rash Distribution/Presentation | Lymphadenopathy | Other Notable Symptoms | Vaccination History |
|---|---|---|---|---|
| Hospital-Based Studies | ||||
| Mmerem, 2024 | Genital rash (60.7%), Oral lesions (19.6%), Anogenital pain/bleeding (10.7%), Genital soft tissue swelling (30.4%) | 46.5% | Sore throat (41.1%), Diarrhea (8.9%), Cough (16.1%) | No vaccination |
| Ogoina, 2023 | First rash: face (53%), anogenital (19%); Distribution: centrifugal (63%), centripetal (18%), mainly anogenital (13%); Rash count: >10,000 (16%) | Inguinal (43%), cervical (38%), submandibular (31%), axillary (25%), generalized (9%) | Distinct febrile prodrome (59%) | Prior smallpox: 4% |
| Ogoina, 2020 | Rash distribution: face (97.5%), trunk (92.5%), arms (87.5%), legs (85%), genitalia (67.5%), scalp (62.5%), palms (55%), soles (50%), mouth (37.5%), eyes (25%); Rash as first symptom (65.7%) | Inguinal, generalized, cervical, axillary, submental (87.5%) | Genital ulcer (62.5%), Pruritus (37.5%) | NR |
| Ogoina, 2019 | Vesiculopustular rash (100%); Genital ulcers in HIV+ cases | 61.9% | Skin itching (66.7%) | NR |
| Ogoina, 2023 (NEJM) | Genital rash (100%), Lesions localized to genital area (62%), No anorectal lesions | NR | Distinct febrile prodrome (75%) | NR |
| Onyeaghala, 2025 | First rash: face (94.3%), anogenital (5.7%); Rash types: pustules (91.4%), papules (77.1%), vesicles (77.1%); Lesion locations: trunk (100%), limbs (100%), genitals (82.9%) | NR | NR | NR |
| Community/Surveillance Studies | ||||
| Yinka-Ogunleye, 2023 | Genital lesions (89.6%), Oral lesions (28.3%) | 73% | NR | NR |
| Yinka-Ogunleye, 2019 | Rash distribution: face (96%), legs (91%), trunk (80%), arms (79%), palms (69%), genitalia (68%), soles (64%) | 69% | Pruritus (73%), Myalgia (63%), Sore throat (58%) | NR |
| Stephen, 2022 | Genital rashes (43%), Mouth sores (57%), Conjunctivitis (50%) | 50% | Muscle aches (57%), Backache (36%), Respiratory symptoms (29%) | NR |
| Onu, 2023 | Pustular rash on face, palms, soles | NR | NR | NR |
Note: NR = Not Reported
| Study | Complication Rate | Specific Complications | Common Comorbidities |
|---|---|---|---|
| Hospital-Based Studies | |||
| Mmerem, 2024 | 32.1% | Sepsis (83.3% of complications), Wound infection, Pneumonia, Acute kidney injury, Acute urinary retention | HIV (23.2%), Diabetes (5.4%), Pregnancy (2 women) |
| Ogoina, 2023 | 49% | Skin complications (48%): secondary bacterial infections (43%), penile/vulva edema (23%), scrotal edema (13%); Mucosal complications (19%): urethritis (7%), keratitis (6%), proctitis (6%); Systemic (21%): sepsis (18%), pneumonia (8%), encephalitis (1%) | HIV (16%; 44% advanced), VZV (30%), Diabetes, hypertension |
| Ogoina, 2020 | 52.5% | Secondary bacterial skin infection (47.5%), Gastroenteritis (12.5%), Sepsis (10%), Bronchopneumonia (7.5%), Encephalitis (7.5%), Keratitis (7.5%), PROM + fetal death (2.5%) | HIV (22.5%), Chickenpox (2.5%) |
| Ogoina, 2019 | NR | PROM with fetal loss, Thrombocytopenia | HIV (25%), Syphilis (25%), Chickenpox (2 cases) |
| Ogoina, 2023 (NEJM) | 0% | None | All HIV-negative |
| Onyeaghala, 2025 | 22.9% | Secondary bacterial skin infections (22.9%), Scrotal edema (5.7%), Pharyngotonsillitis (8.6%), Ocular injuries (2.9%), Urinary retention (2.9%), Necrotizing genital ulcers (8.6%), Sepsis (8.6%), Pneumonia (5.7%) | HIV (14.3%), VZV (25%), Advanced HIV (60% of HIV+) |
| Community/Surveillance Studies | |||
| Yinka-Ogunleye, 2023 | NR | Death, Encephalitis (1 pediatric case) | HIV (27.9%), HPV (50%), HSV-1 (22.5%) |
| Yinka-Ogunleye, 2019 | NR | Spontaneous abortion (26 weeks), Secondary bacterial infection with sepsis | HIV/AIDS (4 of 7 deaths) |
| Stephen, 2022 | 50% (conjunctivitis) | Conjunctivitis (50%), Crusting around lesions (53.9% VZV patients) | Malaria (57%), UTI (21%), Skin infection (14%), Diabetes (7%), Hypertension (7%) |
| Adeniran, 2024 | NR | NR | No comorbidities reported |
| Butswat, 2025 | NR | 25% asymptomatic | NR |
Note: NR = Not Reported; PROM = Premature Rupture of Membranes; VZV = Varicella-Zoster Virus
| Clinical Characteristic | Pre-2022 Outbreaks (2017-2019) | 2022-2025 Outbreak Period |
|---|---|---|
| Most Common Symptoms | Rash (100%), Fever (88-90%), Lymphadenopathy (69-87.5%), Headache (47.5-79%) | Rash (100%), Fever (74-93%), Fatigue (53.6-74.3%), Headache (54.3-77%), Myalgia (66.1%) |
| Genital Lesions | 62.5-89.6% | 60.7-100% |
| Hospitalization Rate | 61.9-81% | 48-80% |
| Complication Rate | 52.5% | 22.9-49% |
| CFR | 2.4-12.5% | 0-12.5% |
| HIV Co-infection | 22.5-27.9% | 14.3-23.2% |
| VZV Co-infection | 2.5% (single case) | 25-35.9% |
| Key Clinical Features | Rash often first symptom (65.7%), Centrifugal distribution, High complication rates in hospitalized patients | Genital rash more prominent, Distinct febrile prodrome, Sexual transmission documented, Asymptomatic cases reported (25%) |
| Special Findings | Household clusters, Nosocomial transmission, High mortality in HIV+ and children | Mpox-VZV co-infection common, Non-exanthematous presentations, Heterosexual transmission chains |