Research![]() | Volume 8, Article 16, 03 Apr 2025
| Volume 8, Article 16, 03 Apr 2025
Belinda Nsiah Opoku1, Ebenezer Kofi Mensah1, Joseph Asamoah Frimpong1, Delia Akosua Bandoh1, Gyesi Razak Issahaku1, Ernest Kenu1
1Ghana Field Epidemiology Training Programme, Accra, Ghana
&Corresponding author: Delia Bandoh, Africa Field Epidemiology(AFENET), Accra, Ghana, Email address: deliabandoh@st.ug.edu.gh
Received: 18 Sept 2024 – Accepted: 10 Mar 2025 – Published: 03 Apr 2025
Domain: Surveillance System Evaluation, Infectious Disease Epidemiology
Keywords: Cholera, Evaluation, Surveillance, Ghana
©Belinda Nsiah Opoku et al Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Belinda Nsiah Opoku et al Evaluation of cholera surveillance system, Kumasi Metropolis, Ashanti Region, Ghana, 2020. Journal of Interventional Epidemiology and Public Health. 2025;8:16. https://doi.org/10.37432/jieph.2025.8.2.165
Introduction: In 2014, Ghana experienced a cholera outbreak with 28,975 cases and 247 deaths from the then 10 regions. To monitor, detect early, respond, and reduce the burden of cholera, a standard operating procedure was designed as a guide for cholera surveillance. We evaluated the cholera surveillance system in Ghana’s second most populated city – Kumasi metropolis, to determine whether the system is meeting its objectives, and assessed its attributes and usefulness.
Methods: We reviewed 2015-2019 cholera surveillance data sourced from health facilities and the health directorate of the Kumasi Metropolis. Stakeholders were interviewed using a semi-structured questionnaire. The Centers for Disease Control Updated Guidelines for Evaluating Public Health Surveillance Systems, 2001 was used to assess the system’s attributes and usefulness. Data was entered and analyzed using Microsoft Excel and Epi Info. Findings were described in comparison with the CDC Guidelines and presented as frequencies, percentages and tables.
Results: A total of eight confirmed cases of cholera were reported. Bantama South sub-metro recorded 75% (6/8) of the cholera cases. The system uses a simple case definition which is easy to understand and well-integrated with other systems. Missing values and incomplete data reporting were identified, with overall completeness calculated at 60%. The system had 45.7% timeliness and 47.4% acceptability, with adequate back-up for storage and power.
Conclusion: The cholera surveillance system in Kumasi metropolis is sub-optimal. Data quality, timeliness and acceptability need improvement, to prevent future outbreaks. Personnel were guided to rectify gaps with data reporting and clinicians sensitized on cholera case definition.
Keywords: Cholera, Evaluation, Surveillance, Ghana
Cholera poses serious public health threats globally. Its transmission is closely associated with areas of poor sanitation and limited water supply [1] Osei FB, Duker AA. Spatial and demographic patterns of Cholera in Ashanti region – Ghana. Int J Health Geogr [Internet]. 2008 Aug 12 [cited 2025 Mar 12];7(1):44. Available from: http://ij-healthgeographics.biomedcentral.com/articles/10.1186/1476-072X-7-44 https://doi.org/10.1186/1476-072X-7-44 . Environmental interventions towards cholera are therefore targeted at ensuring use of safe water, basic sanitation and good hygiene practices which align with the sustainable development goals (SGDs) [2] Ministry of Health (GH) National Surveillance Unit. Technical Guidelines for Integrated Disease Surveillance and Response in Ghana [Internet]. Accra (GH): Ministry of Health, National Surveillance Unit (GH); 2002 April [cited 2025 Mar 12]; 222 p. Available from: https://www.moh.gov.gh/wp-content/uploads/2016/02/Integrated-Disease-Surveillance-and-Response-Ghana-Guidelines.pdf .
Globally, roughly 1.3 to 4 million cases of cholera, with 21000 to 143000 deaths are estimated every year [3] WHO. Cholera [Internet]. Geneva (CH): WHO; 2024 Dec 5 [cited 2025 Mar 12]; [about 15 screens]. Available from: https://www.who.int/news-room/fact-sheets/detail/cholera . In 2017, over 1 million cases were notified from 34 countries, with about 6000 deaths. Africa contributed to up to 54% of global cholera cases in 2016 [3] WHO. Cholera [Internet]. Geneva (CH): WHO; 2024 Dec 5 [cited 2025 Mar 12]; [about 15 screens]. Available from: https://www.who.int/news-room/fact-sheets/detail/cholera . The cholera burden in Africa is largely related to limited water and sanitation facilities in the continent, as well as socio-demographic factors such as urbanization, population density and socio-economic status [4] Ali M, Emch M, Donnay JP, Yunus M, Sack RB. Identifying environmental risk factors for endemic cholera: a raster GIS approach. Health & Place [Internet]. 2002 Jan 9 [cited 2025 Mar 12];8(3):201–10. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1353829201000430 https://doi.org/10.1016/S1353-8292(01)00043-0 Subscription or purchase required to view full text , [5] Emch M, Yunus M, Escamilla V, Feldacker C, Ali M. Local population and regional environmental drivers of cholera in Bangladesh. Environ Health [Internet]. 2010 Jan 14 [cited 2025 Mar 12];9(1):2. Available from: http://ehjournal.biomedcentral.com/articles/10.1186/1476-069X-9-2 https://doi.org/10.1186/1476-069X-9-2 , [6] Ohene-Adjei K, Kenu E, Bandoh DA, Addo PNO, Noora CL, Nortey P, Afari EA. Epidemiological link of a major cholera outbreak in Greater Accra region of Ghana, 2014. BMC Public Health [Internet]. 2017 Oct 11 [cited 2025 Mar 12];17(1):801. Available from: http://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-017-4803-9 https://doi.org/10.1186/s12889-017-4803-9 .
In Ghana, cholera has consistently been a public health concern since 1970, when it surfaced. The Ghana Health Service reports that, about 26000 cholera cases and 600 related deaths were recorded between 2000 and 2005. In 2014-2015, Ghana experienced one of its biggest outbreak of cholera in the country’s history. Up to 28,975 cases of cholera were recorded, with 247 deaths from all over the country [2] Ministry of Health (GH) National Surveillance Unit. Technical Guidelines for Integrated Disease Surveillance and Response in Ghana [Internet]. Accra (GH): Ministry of Health, National Surveillance Unit (GH); 2002 April [cited 2025 Mar 12]; 222 p. Available from: https://www.moh.gov.gh/wp-content/uploads/2016/02/Integrated-Disease-Surveillance-and-Response-Ghana-Guidelines.pdf . Cholera outbreaks place a high burden of morbidity and mortality on individuals and countries. Economically, they further cause a decline in tourism and trade in a country [7] Global Taskforce for Cholera Control (GTFCC): About Cholera [Internet]. Geneva (CH): GTFCC; c2025. Cholera is a disease of inequity that afflicts the world’s poorest and most vulnerable populations. c2025 [cited 2025 Mar 25]. Available from: https://www.gtfcc.org/about-cholera/ .
The Kumasi Metropolis has notable overcrowded areas due to urbanization, slums, as well as places with water, sanitation and hygiene problems. These conditions have been known to exacerbate the spread of Vibrio Cholerae bacteria. The metropolis was one of the hardest hit districts in the Ashanti region during the 2014/2015 cholera outbreak in Ghana. Similar to the surveillance systems of other notifiable diseases in the Kumasi metropolis, the cholera surveillance system is set up with the objectives of detecting, responding promptly and appropriately to cases and outbreaks of watery diarrhoea; immediately reporting cases and deaths when an outbreak is suspected and investigating and responding to suspected cases within 48 hours [2] Ministry of Health (GH) National Surveillance Unit. Technical Guidelines for Integrated Disease Surveillance and Response in Ghana [Internet]. Accra (GH): Ministry of Health, National Surveillance Unit (GH); 2002 April [cited 2025 Mar 12]; 222 p. Available from: https://www.moh.gov.gh/wp-content/uploads/2016/02/Integrated-Disease-Surveillance-and-Response-Ghana-Guidelines.pdf . The Kumasi metropolis, according to available records, has seen no evaluation of the cholera surveillance system over the years; hence the need for this evaluation.
We evaluated the cholera surveillance system in the Kumasi metropolis to assess its usefulness, and attributes and determine if its objectives are being met.
Study Site
The study was conducted in the Kumasi metropolis which is the biggest district in the Ashanti Region of Ghana, with an estimated population of 1,041,747. It has 10 sub-metros. Seven of them are newly established and are being overseen and managed by the existing three (Bantama, Manhyia and Subin) until they become independent. The metropolis has 68 facilities: seven governments (including Komfo Anokye Teaching Hospital (KATH)), fifty-two private, four Christian Health Association of Ghana (CHAG) and five quasi government facilities. It is a largely urbanized district with few slums around Yalewa Zongo and Dakodwom; these areas are overcrowded and have challenges with sanitation and hygiene. The most common water source is pipe-borne water followed by bore holes and wells. Waste disposal methods at the community level include dumping at communal containers and pick-up by waste management companies. Culturally, the metropolis is well noted for its attention to flamboyant funerals, characterised by practices such as mass food preparation and sharing, handshaking, handling of dead bodies; all of which may influence the spread of cholera.
Study design
We conducted a cross-sectional study to evaluate the cholera surveillance system in the Kumasi metropolis between the period of 2015 to 2019. The evaluation lasted from January 7 to February 11, 2020. The CDC Updated Guidelines for Evaluating Public Health Surveillance Systems, 2001 was adopted for the evaluation.
We interviewed key stakeholders including the deputy director of public health, metropolitan director of health services, public health nurses, disease control officers, health information officers and field technicians at the regional and metro, sub-metro and facility levels.
Data collection methods
Data (from 2015 to 2019) was collected at the regional, district and facility levels. We visited and assessed three health facilities, namely Manhyia Government Hospital, Suntreso Hospital and Mother and Child Health Hospital. The Kumasi Public Health Reference Laboratory was also visited. We conducted interviews using a paper-based, interviewer-administered semi-structured questionnaire among individuals at the facility, district and regional levels. Records, line lists, case-based forms, consulting room registers, annual reports, action plans and data on DHIMS were reviewed to assess the system’s achievements and fallbacks. Observations were made to check on facilities’ posting of and access to case definitions, flow charts and information flow.
Data collection tools
We used a paper-based checklist and interview guide, as developed from CDC’s 2001 Updated Guidelines for Evaluating Public Health Surveillance Systems[8]
CDC. Updated Guidelines for Evaluating Public Health Surveillance Systems: Recommendations from the Guidelines Working Group. MMWR [Internet
. 2001 Jul 27 [cited 2024 Nov 11
; 50 (RR13):1-35. Available from: https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5013a1.htm
to collect the information on attributes of the surveillance system.
Simplicity: Evaluating simplicity of the system was done by determining ease of understanding and use of case definition and ease of understanding the system’s flow chart. It also assessed the time involved in entering, storing, backing up, editing and transferring data.
Flexibility: To assess flexibility, information was collected on changes that have occurred in the system (including changes to case definition, reporting mechanisms among others), procedures involved in making changes and how fast the system adapted to the changes.
Data Quality: Data quality of the system was assessed by gathering information on completeness of data collected and validity of data collected in the system.
Acceptability: Acceptability was assessed by obtaining information on willingness on the part of stakeholders to participate in the system, general completeness and timeliness of reporting of data by stakeholders.
Sensitivity: To assess sensitivity, information on number of cases and outbreaks identified by the system per the target of the system was collected.
Predictive Value Positive: PVP was assessed by collecting information on true positives reported.
PVP was calculated using the formula: \(\text{PVP} = \frac{\text{Confirmed Cholera cases}}{\text{Reported Cholera Cases}} \times 100\%\)
Representativeness: Records were reviewed and stakeholders were interviewed to identify how many sub-metros report, how many facilities and what kind of facilities report.
Timeliness: To assess the timeliness of the system, the times of reporting to facilities, the timeliness of lab tests, and feedback to and from facilities, sub-metros, the metropolis and the region were observed and assessed. Timeliness was calculated as:
Timeliness for reporting cholera cases=\(\frac{\text{Facilities that met deadline}}{\text{Total number of facilities that submitted}}\)
Stability: Information was collected on the challenges of the system. These include challenges with data collection and entry, data analysis, transport of data, availability of a computerized system, regularity of servicing of computers, the use and quality of the internet, and how power outages affect the system. We also assessed if the system is donor-dependent or not.
Assessing usefulness of the Cholera Surveillance System
To acquire information on the usefulness of the surveillance system, semi-structured interviews were conducted with stakeholders at the metropolitan and regional levels for the translation of knowledge into services, solving health problems and prevention and control of cholera. We assessed if the system improved clinical practice, if it is able to estimate the magnitude of morbidity and mortality and if it is able to measure the effectiveness of prevention and control programs.
Case Definition for Cholera
The Integrated Disease Surveillance and Response defines cholera at two levels – suspected case and confirmed case. A suspected case is defined as a patient aged 5 years or more, with severe dehydration or death from acute watery diarrhoea (rice water stool). If there is a cholera epidemic, a suspected case is a person aged 5 years or more with acute watery diarrhoea, with or without vomiting. A confirmed case is defined as a suspected case in which Vibrio cholerae O1 or O139 has been isolated in the stool [2].
Data Analysis
Data sets and case-based forms from the regional, metro and facility levels were analysed using Microsoft Excel 2019 and Epi Info version 7. Findings were described in comparison with the CDC Descriptive Guidelines and presented as frequencies, percentages and in tables.
Ethical consideration
The Ghana Health Service granted approval for the evaluation to be conducted as part of its surveillance mandate. Informed consent was sought from participants before their engagement. The evaluation process and purpose were explained to all participants before interviews were conducted. We ensured anonymity by taking off names of all participants. We stored data using password – protected computers.
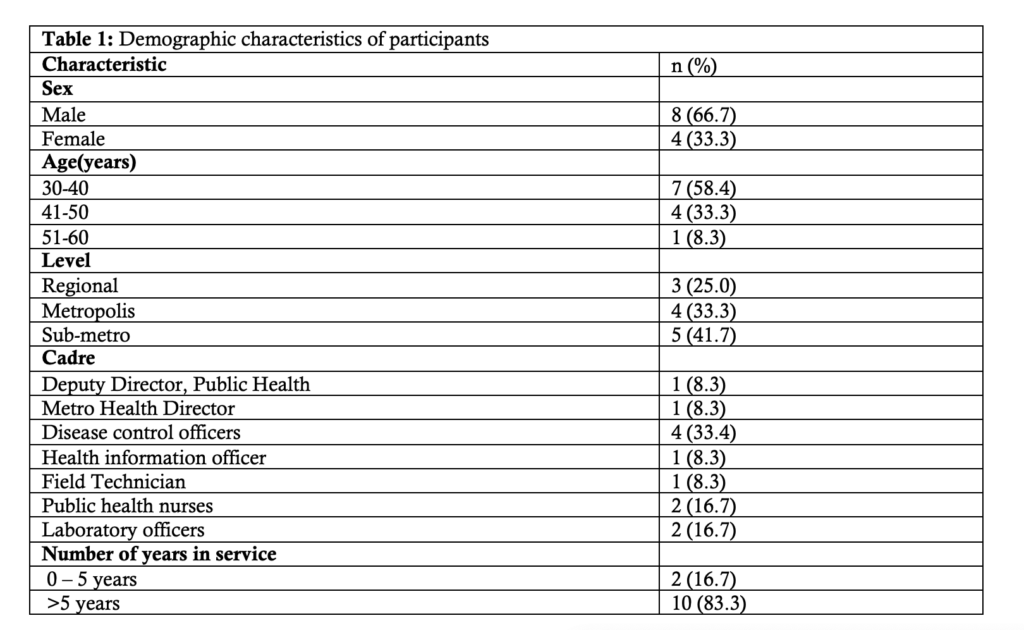
Demographic Characteristics of Participants interviewed
A total of 12 health workers were interviewed during the evaluation. Males contributed 66. 7% (8/12) while age group 30-40 years formed 58.4% (7/12). Most (83.3% (10/12) participants had more than 5years of work experience (Table 1).
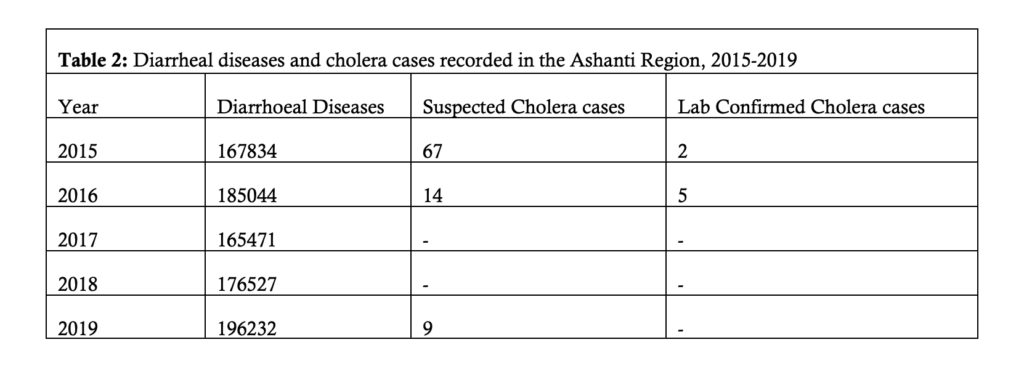
Cholera Cases
The highest number of confirmed cholera cases recorded in the Ashanti region annually has been 5 which was reported in 2016 (Table 2). The Kumasi Metropolis, according to DHIMS 2, recorded one confirmed case of cholera between the period of 2015 and 2019. However, supporting data from the sub-metro levels showed there had been 8 confirmed cases. The highest number of cases (six) was reported in the Bantama-South sub-metro.
Flow Chart of Reporting Process
Figure 1 describes how cholera is reported in the country. The process usually starts at the community level and ends with the World Health Organisation (WHO). The community level employs the use of trained community-based health volunteers (who are uncommon in urban communities) to report suspected cases of cholera to the health facilities. The community/public health nurses, health information officers and surveillance officers then take charge of reporting cases at the health facility level to the district level directly or through the sub-district to the district. At the district, cases are collated from the various facilities and sub-districts to the regional surveillance officer who eventually communicates with the disease surveillance department of the Ghana Health Service (at national level) and finally to WHO. The public health reference laboratories which are responsible for the confirmation of cholera in most regions reports to both the regional and national levels and gives feedback to the districts. Feedback is sent from the higher levels to the lower levels. Reporting is usually done through digital platforms including WhatsApp, e-mails, Telegram, among others. Cholera reporting at every level is expected to be immediate (within 24 hours), so that the necessary prompt response is initiated (Figure 1).
Operation of the Cholera Surveillance System
Case detection
In detecting cases of cholera, both active and passive surveillance are employed in the Kumasi metropolis. For active surveillance, the use of community-based surveillance volunteers is not common in the metro. Health workers (community health nurses, field technicians) through routine home visits and outreaches do active search for cases and refer them to health facilities. There have been instances in the metropolis where patients reported to the health facilities themselves by virtue of the education they have received on cholera. Passive surveillance is done by reviewing records of patients using case definitions. Suspected cholera cases are registered using the cholera case-based form and a copy is sent together with sample for laboratory testing at the Public Health Reference Lab, Kumasi.
Data Reporting
The cholera case-based form has three main parts – demographic information of suspected case, the clinical history of patient and laboratory-related information.
Three copies of the form are usually made after filling it completely. One is kept at the facility, another goes to the metropolitan health directorate and the last copy goes with the sample to the Public Health Reference Laboratory, Kumasi. The lab reports back to the facility on the results through phone calls and WhatsApp messages. Suspected and confirmed cholera cases are reported weekly and monthly (IDSR) on DHIMS 2 and collation is done at the metropolitan health directorate, usually by the health information manager and/or the metropolitan disease control officer. Written copies of reports on cases are also kept at the facility level. The metro disease control unit keeps a line list of all suspected cases.
Data Analysis
Analysis of data is hardly done at the facility level. The sub-metro, metro and regional health directorates however do monthly and quarterly analysis of data by age, sex, time and place, comparing trends and assessing possibility of outbreaks.
Resources
All logistics (including antibiotic medications, intravenous infusions, testing kits, personal protective equipment) for managing cholera, especially in outbreak situations are freely provided by the Government of Ghana through the Ghana Health Service and other partners.
No funding allocation is specifically made for cholera surveillance in the budgets of the Metropolitan Health Directorate. Rather, funds for cholera surveillance are catered for in the general allocation made for surveillance of priority diseases (IDSR).
Personnel involved in the cholera surveillance include the director for health services, disease control officers, public and community health nurses, clinicians, field technicians, health information officers, administrators, laboratory officers, environmental officers, among others. All these personnel are employed by the Ghana Health Service to assist surveillance activities.
Laboratory confirmation
The laboratory is important in the running of the cholera surveillance system as it helps confirm the presence of the Vibrio cholera bacteria to diagnose cholera. Only few (1/3) facilities visited had cholera RDT kits. All samples are sent to the Public Health Reference Lab (PHRL), Kumasi to test for cholera. The Komfo Anokye Teaching Hospital Laboratory helps in testing cholera samples.
Cholera testing is done using rectal swab or a fresh stool sample. Stool culture or Polymerase Chain Reaction (PCR) is done to confirm the presence of the Vibrio cholera O1 or O139. PCR machines were not available at the Kumasi PHRL at the time of visit. Stool culture, which is more common and less expensive is used. When using stool culture, it takes a period of 24-72hrs before receiving results, depending on whether or not there is growth, and when it occurs.
Performance of the cholera surveillance attributes
Simplicity: The cholera surveillance system uses clinical manifestation, epidemiological link and laboratory confirmation to define a case. The system is so well integrated with other diseases in the IDSR such that it uses similar case-based forms as the others. Data reporting, analysis and dissemination is less complicated. It takes a maximum of a day to complete monthly/quarterly analysis. Reporting is done on the DHIMS 2 electronic platform. Reporting and feedback are done through electronic media such as WhatsApp, e-mails, among others, which takes only seconds to minutes to report.
Timeliness: When there is a suspected case of cholera at a health facility, it takes an average of 5 minutes to inform the Disease Control Unit of a facility. It also takes an average of 1minute to get the district informed through a common WhatsApp platform. At the laboratory, it takes 24 to 72 hours to confirm a suspected cholera case using stool culture. Reports are submitted weekly through DHIMS 2.
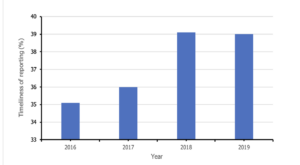
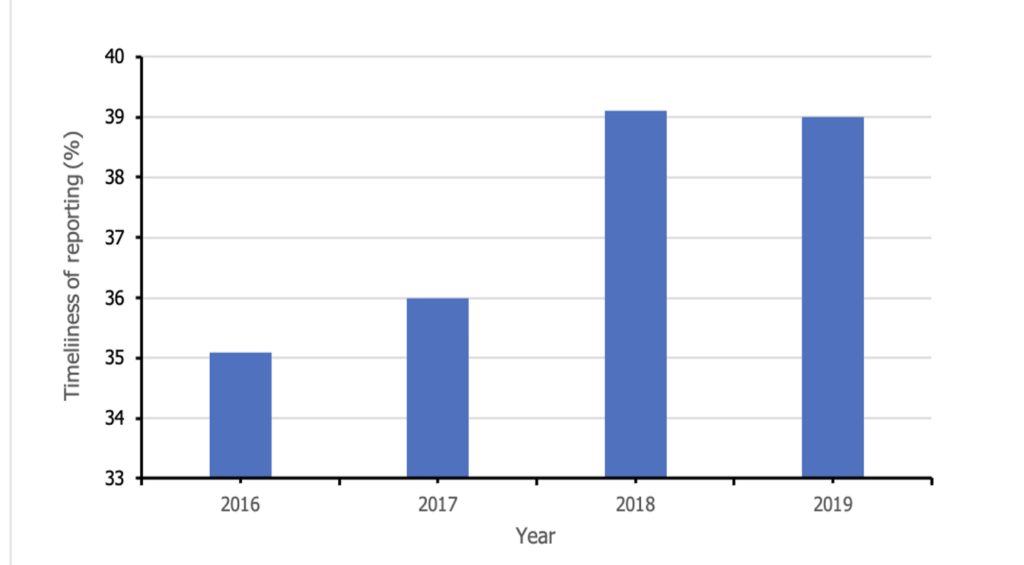
The following were timeliness percentages recorded for the various years in the metropolis: 35.1% for 2016, 36% for 2017, 39.1% in 2018 and 39% for 2019 (Figure 2). The overall percentage recorded for facilities which reported on time for the period of 2016 to 2019 is 45.7% (less than 50%).
Data quality: Among records reviewed were those with missing values, incomplete case-based forms and line lists. Completeness of records reviewed was estimated at 60%. At the metro level, case-based forms and line lists for some years (2015 and 2017) were unavailable. Also, some figures given by the sub-metro level were found to be inconsistent with the metro’s data as well as the region’s data. For instance, the overall number of cases for the period of study as reported by the Metro Health Directorate (with their available data) was one case; which was less than the total of eight cases reported by the various sub-metro health management teams. Meanwhile the Ashanti region, within which the Kumasi Metropolisis is found reported a total of seven lab-confirmed cases (Table 1). There is however a data validation team in place (made up of the metro health director, public health nurse, health information manager, disease control officer, among others) which meets monthly at the metro level to validate data. All facilities visited also had data validation teams in place.
Acceptability: Reports are expected weekly and monthly for cholera (IDSR) from 68 facilities. In 2019, 84.3% of facilities reported. 54.5% reported in 2016, 37.8% in 2017 and 42.5% in 2018. (Figure 2). The overall proportion of facilities which reported was 47.4%. The overall percentage recorded for facilities which reported on time for the period of 2016 to 2019 was 45.7%. It was noted that majority (96%) of the facilities which who do not report are privately-owned facilities; reason being they do not feel obliged to report. Case-based forms assessed were 60% complete.
Sensitivity: The system was able to detect an outbreak. An outbreak was detected in 2016 with one case of cholera, in 2018 for instance, line lists available at the sub-districts indicated that a total of 10 cases of cholera were suspected in the metropolis.
Positive predictive value is low. According to the line lists collated at sub-districts, out of the 10 cases suspected in 2018, 30% (3/10) were confirmed positive at the laboratory using stool culture.
Stability: Computers used for the system’s activities at all levels – from regional to facility were all working. The computers were as well supported by uninterrupted power supply devices. Data is backed up on external hard drives at the regional and metro level. Facilities also keep written copies of reports as back-up. The system faces some challenges including inadequate funds, apathy and inadequate training on cholera surveillance.
Representativeness: All three sub-districts report on DHIMS 2. All facilities report to the district through DHIMS 2 and other platforms such as WhatsApp. There is however low reporting from the private facilities. From data available for 2016, 2018 and 2019, a total of 18 cases were suspected from all sub-districts.
Usefulness: The zero target for cholera was met for the years, 2015 and 2017. Cholera has been under control. One-to-three-case cholera outbreaks were detected in the years 2016, 2018 and 2019 which were controlled. The cholera case definition has contributed to making good cholera diagnoses in the clinical setting. With an organised reporting system (DHIMS 2) in place, cholera-related mortalities and morbidities are easily estimated for planning purposes.
The objectives of the cholera surveillance system are being met. Personnel effectively suspect cases, report them within few seconds, confirm cases and commence control measures within 48 hours. However, cholera RDTs are unavailable in most facilities in the metropolis. These findings contrast standard operating procedures (SOPs) for the prevention and control of cholera in Ghana (2016) and a global study on cholera surveillance which stressed on the availability of cholera rapid diagnostic tests (RDTs) to help improve objective judgment in the early detection of a cholera outbreak in a local setting. The use of the cholera RDTs also becomes essential during emergency situations and when the testing centres are overburdened [9] Al Kalali FSA, Mahyoub E, Al-Hammadi A, Anam L, Khader Y. Evaluation of the national tuberculosis surveillance system in Sana’a, Yemen, 2018: Observational Study. JMIR Public Health Surveill [Internet]. 2021 Nov 30 [cited 2025 Mar 12];7(11):e27626. Available from: https://publichealth.jmir.org/2021/11/e27626 https://doi.org/10.2196/27626 , [10] Ebob T Jacqueline. Cholera prevention and control strategies; a global overview. JAMMR [Internet]. 2020 Jul 31 [cited 2025 Mar 25];32(12):27–53. Available from: https://journaljammr.com/index.php/JAMMR/article/view/3735 https://doi.org/10.9734/jammr/2020/v32i1230540 Download pdf to view full text. . The Public Health Reference Laboratory lacked PCR machines which give faster results, compared to stool culture.
Communities in the Kumasi metro do not have community-based surveillance volunteers (CBSVs) to help with social mobilization and other activities at the community level. Most studies have indicated the need for CBSVs in the control of priority diseases in both urban and rural settings [11] Abass KM, Van Der Werf TS, Phillips RO, Sarfo FS, Abotsi J, Mireku SO, Thompson WN, Asiedu K, Stienstra Y, Klis SA. Buruli ulcer control in a highly endemic district in ghana: role of community-based surveillance volunteers. The American Society of Tropical Medicine and Hygiene [Internet]. 2015 Jan 7 [cited 2025 Mar 12];92(1):115–7. Available from: https://www.ajtmh.org/view/journals/tpmd/92/1/article-p115.xml https://doi.org/10.4269/ajtmh.14-0405 Subscription or purchase required to view full text , [12] Dil Y, Strachan D, Cairncross S, Korkor AS, Hill Z. Motivations and challenges of community-based surveillance volunteers in the northern region of ghana. J Community Health [Internet]. 2012 May 22 [cited 2025 Mar 12];37(6):1192–8. Available from: http://link.springer.com/10.1007/s10900-012-9569-5 https://doi.org/10.1007/s10900-012-9569-5 Subscription or purchase required to view full text . This is most probably due to large extent of urbanization in the metropolis. The absence of CBSVs may lead to late detection of diseases and outbreaks.
Timeliness, acceptability and data quality of the system are low. These attributes are very essential to achieving an outbreak-free future. Findings of some studies in the Northern region of Ghana have indicated the need for timeliness and good data quality in ensuring rapid responses to outbreaks [13] 13. Huaman MA, Araujo-Castillo RV, Soto G, Neyra JM, Quispe JA, Fernandez MF, Mundaca CC, Blazes DL. Impact of two interventions on timeliness and data quality of an electronic disease surveillance system in a resource limited setting (Peru): a prospective evaluation. BMC Med Inform Decis Mak [Internet]. 2009 Mar 10 [cited 2025 Mar 12];9(1):16. Available from: https://bmcmedinformdecismak.biomedcentral.com/articles/10.1186/1472-6947-9-16 https://doi.org/10.1186/1472-6947-9-16 , [14] Adokiya MN, Awoonor-Williams JK, Beiersmann C, Müller O. Evaluation of the reporting completeness and timeliness of the integrated disease surveillance and response system in northern Ghana. Ghana Medical Journal [Internet]. 2016 Apr 7 [cited 2025 Mar 12];50(1):3. 8 p. Available from: http://www.ajol.info/index.php/gmj/article/view/133648 https://doi.org/10.4314/gmj.v50i1.1 Download PDF to view full text . The system has seen apathy in reporting on the part of private facilities. Most of them probably are of the opinion that they are not government facilities and are therefore not obliged to report.
Cholera is a disease of poverty, linked to poor personal and environmental hygiene and lack of safe drinking water. The standard operating procedures for the management of cholera in Ghana emphasize the importance of improving water, sanitation and hygiene in the country for effective the prevention and control of the disease. Although the Kumasi Metropolitan Assembly, together with the health directorate, is putting several measures in place to resolve sanitation issues in Kumasi, there still remains quite a number of slums and areas which lack safe drinking water. These issues affect the effective prevention and control of cholera and its outbreak in the metropolis. The poor sanitation and poor hygiene conditions in some parts of Kumasi are also found in other districts in Ghana, where cholera outbreaks have been rampant [14] Adokiya MN, Awoonor-Williams JK, Beiersmann C, Müller O. Evaluation of the reporting completeness and timeliness of the integrated disease surveillance and response system in northern Ghana. Ghana Medical Journal [Internet]. 2016 Apr 7 [cited 2025 Mar 12];50(1):3. 8 p. Available from: http://www.ajol.info/index.php/gmj/article/view/133648 https://doi.org/10.4314/gmj.v50i1.1 Download PDF to view full text .
The cholera surveillance system is meeting its objectives. It is sensitive, representative, stable and useful. However, timeliness, data quality and acceptability need improvement. As a form of public health intervention, we guided some disease control officers at facilities to correct some gaps identified with data, sensitized clinicians on the standard case definition for cholera and shared findings from the evaluation with stakeholders.
We recommended that Kumasi Metro Health Director liaises with the disease control unit to provide more cholera RDTs for facilities and organize training on data reporting and cholera surveillance for all personnel, including those from private facilities:
Although, this evaluation captured most of the vital components of the Cholera surveillance system, the environmental involvement which is a major determinant of cholera spread was not fully explored. Other evaluation studies may consider that in the future.
What is already known about the topic
What this study adds
BNO and EKM supervised and implemented the overall evaluation. BNO collected and analyzed data. BNO, JAF, EKM, DB and RG contributed to the writing of the manuscript and provided critical intellectual perspective of the evaluation. All authors read and approved the final manuscript

Views: 2,432
Menu, Tables and Figures
Table 1: Demographic characteristics of participants
Table 2: Diarrheal diseases and cholera cases recorded in the Ashanti Region, 2015-2019