Research | Open Access | Volume 8 (4): Article 83 | Published: 14 Oct 2025
Views: 1,758
Menu, Tables and Figures
Table 1: Criteria of the evaluation’s attributes of the Community-Based Surveillance of poliomyelitis in Tillabéri Health Region, Niger, 2020–2021
| Attributes | Criteria of evaluation | Expected Answer/Value | Evaluation findings | Evaluation decision |
|---|---|---|---|---|
| Usefulnesss | Non-Polio AFP Rate (NPAFP-R) during the Enhanced Community Based Surveillance (E-CBS) is higher than the NPAFP-R before the implementation of the E-CBS | Yes | Yes | Useful |
| Percentage of AFP cases notified through CBS | ≥ 80.0% | 87.7% | ||
| Detection of Poliomyelitis epidemics | Yes | Yes | ||
| CBS personnel trained on Acute Flaccid Paralysis surveillance | Yes | Yes | ||
| Notification of other Vaccine Preventable Diseases | Yes | Yes (Measles: 125, Meningitis: 03, COVID-19: 22) | ||
| Sensitivity | NPAFP-R ≥ 3.0/100,000 under 15 children in the districts implementing CBS | Yes | Yes | Sensitive |
| Simplicity | Each level reports only to another one and no biological criteria to confirm poliomyelitis case | Yes | No | Complex |
| Completion of the investigation form and stool specimen collection don’t require field visit and no constraints in sample collection and transport | Yes | No | ||
| Availability of data management equipment at district level | Yes | Yes | ||
| Ability for focal point to present CBS in person, place, and time | Yes | Yes | ||
| Acceptability | Proportion of Community Relays having alerted on at least one AFP | ≥80.0% | 86.7% (130/150) | Not acceptable |
| Proportion of Heads of Health Facilities participating in CHW supervision | ≥80.0% | 85% (68/80) | ||
| Percentage of AFP alerts verified | ≥80.0% | 88.6% (101/114) | ||
| Percentage of AFP cases notified within seven days after paralysis onset | ≥80.0% | 65.1% (69/106) | ||
| Percentage of AFP cases with adequate stool samples | ≥80.0% | 100.0% (102/102) | ||
| Proportion of AFP surveillance priority sites adequately visited | ≥80.0% | • Highest priority sites: 83.5% • High priority sites: 72.0% • Medium priority sites: 92.2% • Low priority sites: 95.0% | ||
| Timeliness | Percentage of AFP cases notified by Community Relays within 7 days after paralysis onset investigated within 48 hours and whose stool samples were received at National laboratory in good condition within 72 hours | ≥80.0% | 65.1% (69/106) | Not reactive |
| Representativeness | Non-Polio AFP Rate in each district implementing CBS | ≥3.0 AFP cases per 100,000 under 15 children | • Abala: 15.0/100,000 • Ayorou: 66.0/100,000 • Gothèye: 13.0/100,000 • Kollo: 16.0/100,000 | Representative |
| Proportion of children aged less than one year, one to four years and five to fourteen years within AFP cases notified | >0.0% in each age group | • [0 – 1[: 13.1% (15/114) • [1-4]: 84.3% (96/114) • [5-14]: 2.6% (3/114) | ||
| Positive Predictive Value | Percentage of biologically confirmed cases out of those tested in laboratory | <5.0% | 1.4% | Appropriate |
Table 1: Criteria of the evaluation’s attributes of the Community-Based Surveillance of poliomyelitis in Tillabéri Health Region, Niger, 2020–2021
Agballa Mébiny-Essoh Tchalla Abalo1&, Issifou Djibo2, Hamani Samba2, Aboubacar Ali Harouna2, Mumeh Cletus Fumbi3, Tassiou Ibrahim4, Hamidou Harouna4, Ibrahima Hamadou5, Oumarou Maidadji6, Mountari Kollé6, Sayadi Sani6, Ibrahima Na Andy Chaïbou6, Kevin Mugenyi7, Yaya Ballayira7, Rebecca Babirye7, Simon Antara7
1African Field Epidemiology Network (AFENET), Kinshasa, Democratic Republic of Congo, 2African Field Epidemiology Network (AFENET), Niamey, Niger, 3African Field Epidemiology Network (AFENET), Maroua, Cameroon, 4Direction de la Surveillance et de la Riposte aux Epidémies (DSRE), Niamey, Niger, 5Direction Régionale de la Santé, Tillabéri, Niger, 6Bien Être pour la Femme et l’Enfant au Niger (BEFEN). 7African Field Epidemiology Network (AFENET), Kampala, Uganda
&Corresponding author: Agballa Mébiny-Essoh Tchalla Abalo, African Field Epidemiology Network (AFENET), Regional Office of Central Africa and Indian Ocean, Avenue Pierre Mulele, Imeuble Infinity Centre, Gate 104. Kinshasa, DRC, Email: tchanaldinio@yahoo.fr tchanaldinio1234@gmail.com ORCID: https://orcid.org/0000-0003-1896-0272
Received: 14 Jun 2025, Accepted: 13 Oct 2025, Published: 14 Oct 2025
Domain: Vaccine Preventable Disease, Polio Elimination
Keywords: Evaluation, Community-Based Surveillance, Tillabéri, Niger
©Agballa Mébiny-Essoh Tchalla Abalo et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Agballa Mébiny-Essoh Tchalla Abalo et al., Evaluation of community-based surveillance for acute flaccid paralysis cases in a security-compromised setting, Tillabéri Health Region, Niger, 2021. Journal of Interventional Epidemiology and Public Health. 2025;8(4):83. https://doi.org/10.37432/jieph-d-25-00138
Introduction: Community-based surveillance (CBS) is based on community engagement in disease and public health event surveillance. Enhancing the CBS project has been implemented since 2020 through a Community Relays’ network in a security-compromised setting of Tillabéri Health Region in Niger to ensure progress towards poliomyelitis eradication. The study aimed at describing the CBS system and assessing its usefulness, simplicity, sensitivity, acceptability, timeliness, representativeness and determining its positive predictive value.
Methods: This was a descriptive cross-sectional study that included all alerts and acute flaccid paralysis (AFP) cases reported, as well as the selected surveillance system personnel from January 2017 to December 2021. Data were collected via desk reviews and individual face-to-face interviews to describe the CBS’ organisation and operation and assess its usefulness and attributes using the US Center for Disease Control and Prevention, Atlanta, 2001 guidelines. Usefulness were assessed by the Non Polio Acute Flaccid Paralysis Rate (NPAFP-R) before and during CBS, simplicity: no constraint in cases investigation, sensitivity: NPAFP-R≥3.0 cases/100,000 under 15 children in CBS districts, acceptability: ≥80.0% Community Relays reporting alerts associated with ≥80.0% priority sites adequately visited, ≥80.0% cases notified within 7 days after paralysis onset and ≥80.0% adequate cases, timeliness: ≥80.0% AFP cases notified within 7 days after paralysis onset investigated within 48 hours and received at National lab in good condition within 72 hours, representativeness: expected NPAFP-R with both sex and associated with the expected age groups within AFP cases in the CBS districts, Positive Predictive Value: percentage of Poliomyelitis cases among cases notified. Results are presented in proportions and ratios.
Results: Community Relays report to the health system through a free fleet mobile phone network involving all CBS stakeholders from the operational to the central level. The overall NPAFP-R rose from 1.3 to 18.0 cases/100,000 under 15 in CBS districts. AFP cases should be notified within 7 days after paralysis onset, investigated within 48 hours, and specimens should be collected 14 days after paralysis onset. The proportion of AFP cases notified within 7 days was 42.1% (8/19) and 65.1% (69/106) in 2020 and 2021 respectively. The NPAFP-R (Number of AFP cases/100,000 under 15) was 15.0 in Abala, Ayorou: 66.0, Gothèye: 13.0 and Kollo: 16.0. M/F sex ratio: 0.96. Age groups (years) distribution of cases was as follows: <1: 13.1% (15/114), 1-4: 84.3% (96/114), and 5-14: 2.6% (3/114). The overall Positive Predictive Value was 1.4% (2/141).
Conclusion: The enhanced CBS in Tillabéri Region was useful, sensitive, representative, complex, neither reactive nor acceptable. Its timeliness and acceptability could be improved if Community Relays were established and introduced to their respective communities and if the early detection indicator were systematically monitored on a monthly basis.
Since 1988, when the Global Polio Eradication Initiative (GPEI) was launched, the burden of Wild Poliovirus (WPV) decreased from 350,000 cases reported in 125 countries to 33 cases reported worldwide in Afghanistan and Pakistan in 2018 [1]. In 2023, only one case of WPV was reported worldwide from Afghanistan [2], indicating a reduction by 99% of poliomyelitis within one generation [3, 4, 5].
In the World Health Organisation (WHO) African region, the last case of WPV was notified in 2016 in Nigeria; and since no other case was reported thereafter, the region was certified free of WPV in 2020 [6]. However, in 2022, Malawi notified one WPV case and Mozambique eight cases [2,7], whose strains were linked to the case that was notified in Pakistan in 2019 [5]. In 2020, 20 countries, the majority African, notified 323 circulating Poliovirus Vaccine Derived type-2 (cVDPV2) [4]. New WPV cases added to the preexisting cVDPV2 epidemics compromise GPEI agenda achievement, especially in Africa and have led to strategic orientations that have been integrated into action plans and strategies towards poliomyelitis eradication.
Major challenges compromising progress towards poliomyelitis eradication, are difficult access to conflict or insecure areas, geographical zones with difficult accessibility and localities whose communities cultures, religions and social constructs constitute a barrier to health services, weak capacity of surveillance systems to manage the polio surveillance information system, weak capacity of the GPEI laboratory network to ensure environmental surveillance, and inadequate supervision, coordination, monitoring and evaluation of polio surveillance systems [1]. In settings where insecurity prevails, Community-Based Surveillance (CBS) of Acute Flaccid Paralysis (AFP) constitutes one of the resilient strategies through poliomyelitis eradication [8 – 14]. It’s an active process of community participation in detection, systematic notification, early response and follow-up of public health events in the community [15, 16, 17]. Its implementation can either temporarily supplement a collapsed surveillance system, as in areas of insecurity and conflict, or strengthen the existing surveillance systems [18].
Acute Flaccid Paralysis surveillance is one of the strategies recommended by WHO for poliomyelitis eradication. It is performed through the Integrated Disease Surveillance and Response recommended by WHO to African countries since 1998. The Poliomyelitis Eradication Strategy 2022 – 2026 recommends enhancing detection and response through sensitive surveillance that provides the program with critical information for action and recalls implementing CBS to sustain the progress to eradication.
Since 2011, Tillabéri has been among the regions in Niger that have encountered serious terrorist attacks resulting in the displacement of populations, according to the global terrorism database reports [19]. The insecurity in that region threatens the sustainability of the results achieved by the country towards poliovirus eradication.
To maintain these results and progress towards poliovirus eradication, a project aiming at strengthening CBS of AFP was initiated in four districts of the Tillabéri region. The objectives of this project were to increase the number of AFP cases notified by the project’s target districts and to increase the proportion of AFP cases with adequate stool samples. Since its launch in 2020, the achievements and performance, as well as its relevance and the compliance of stakeholders involved in CBS, have never been assessed and documented for use in advocating for scaling up and sharing best practices and lessons learned with other partners involved in poliomyelitis surveillance. This study aimed at describing the CBS system in place, as well as its usefulness, acceptability, simplicity, representativeness, timeliness and positive predictive value.
Study setting
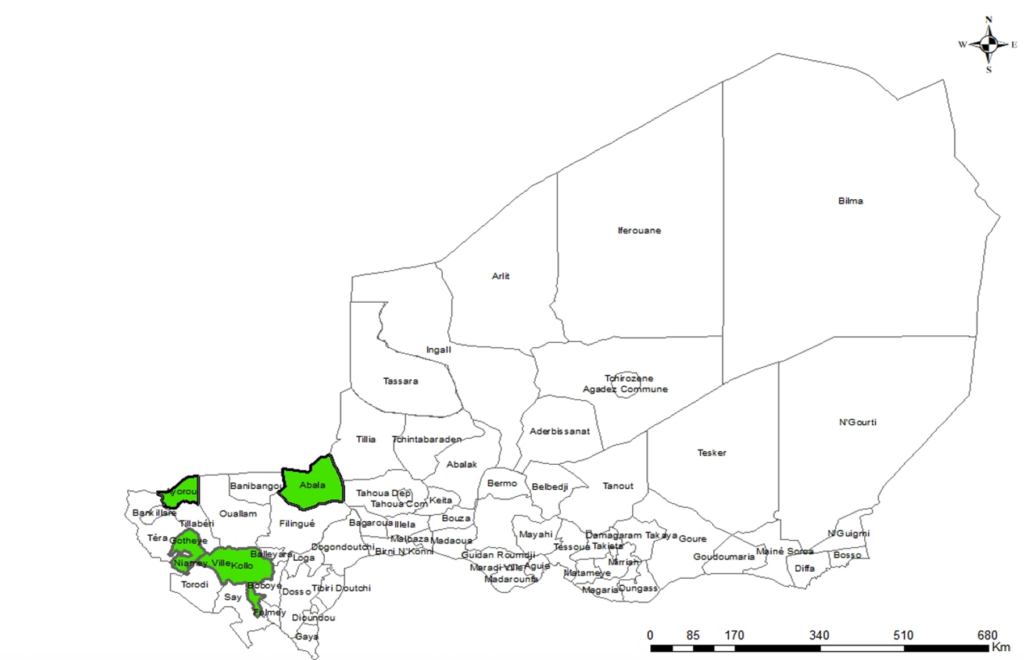
Tillaberi region is in southwestern Niger (Figure 1) with an estimated population of 1,006,612 and 118 per square kilometre population density in 2021. Its dry season covers from November to June, and the rainy one from July to October. The region has 13 health districts, with 227 Primary Care Units and 161 Health Facilities that implement the indicators-based semi-passive Integrated Diseases Surveillance and Response activities. AFP cases are detected and reported by the Primary Care Units and Health Facilities to districts, the region, and the national surveillance directorate.Four districts, including Abala, Ayorou, Gothèye and Kollo were jointly selected by health authorities and partners according to their performance in AFP surveillance to implement the CBS that began in August 2020. In CBS districts, there were 64 Health Facilities, 131 Primary Care Units and 655 Community Relays trained and involved in CBS. Two cell phone networks in addition to the wireline system, serve the region, and the internet connection provided is unstable.
Niger health system has a pyramidal structure. At the operational level, a network of volunteers called “Relais Communautaires” (Community Relays) operates in each village and depends on a Primary Care Unit led by a Community Health Worker (CHW) who supervises the Community Relays. Above the Primary Care Unit, there is the “Centre de Santé Intégré”, a Health Facility led by a nurse or a Medical Doctor. Above the Health Facility, there are the district hospital and the regional hospital, respectively. In this study, Community Relays were referred to as the volunteers identified and trained for the active case research of AFP alerts, while CHW was the direct Community Relays’ supervisor, and the head of Health Facility was the CHW’s direct supervisor.
Study design and period
This was a mixed-method descriptive cross-sectional study conducted from June to August 2022.
Study population
Quantitative data included all AFP cases notified in the Tillaberi region from January 2017 to July 2020. This covers a period before CBS and from September 2020 to December 2021, during the CBS period. Qualitative data were extracted from health facilities as the primary source, health personnel, as well as district and regional disease surveillance focal points. All the heads of the 64 health facilities and the seven district focal points were included. Considering security, accessibility to some areas and resources availability, 150 CHWs and 80 heads of Primary Care Units were also included.
Operational definitions, study variables and evaluation indicators
The “CDC Atlanta, 2001” guide for evaluating epidemiological surveillance systems was used to define the variables to be evaluated by attribute [20]. Given the security constraints and the available data, the attributes evaluated were the usefulness, the sensitivity, the simplicity, the acceptability, the representativeness and the positive predictive value.
The organization and operation of the CBS was explained through the presentation of the CBS’s goal and its objectives, the definitions of alerts, AFP cases and confirmed poliomyelitis cases, as well as the description of data sources, the frequency of data transmission and reporting, and the profile of the stakeholders engaged.
Usefulness: CBS were useful if the NPAFP-R before CBS was less than NPAFP-R during the CBS, with at least 80.0% AFP cases notified through CBS associated with or not associated with the training of the personnel, outbreak detection and notification of other VPD.
Sensitivity: CBS was sensitive if the NPAFP-R in the implementing districts reached at least 3.0 AFP cases per 100,000 children under 15.
Simplicity: The system was considered simple if each of the following criteria are applicable to the CBS in place: i) each level reports only to another one, ii) completion of investigation form and specimen collection don’t require field visit and no constraints in sample collection and transport, iii) inexistence of areas forbidden for field visits, iv) no biological criteria to confirm poliomyelitis case, v) availability of data management equipment at district level and vi) ability for focal point to present CBS data in person, place, and time. It was complex if the system in place doesn’t match at least one of the criteria listed above.
Acceptability: CBS acceptability refers to ≥ 80.0% of Community Relays reporting alerts associated to ≥ 80.0% of AFP alerts verified, ≥ 80.0% of each category of AFP surveillance priority sites adequately visited, ≥ 80.0% cases notified within 7 days after paralysis onset, ≥ 80.0% of adequate cases among those notified by Community Relays and ≥ 80.0% of CHWs and heads of health facilities participating in Community Relays’ supervision.
Timeliness: CBS was reactive if the percentage of AFP cases notified by Community Relays within 7 days after paralysis onset, investigated within 48 hours, and if stool samples were received at the National laboratory in good condition within 72 hours was at least 80.0%.
Representativeness: CBS was representative if each CBS district had an NPAFP-R ≥ 3.0 cases per 100,000 under 15 children, with both sex within cases and the presence of the following age groups within the overall alerts notified in 2021: less than one year, one to four years old and five to fourteen years old.
Positive Predictive Value: percentage of biologically confirmed cases out of those tested in the laboratory. It was appropriate if its value ≥5.0%.
Alert on AFP: Any child under 15 years old of Tillabéri region who was walking or crawling normally and can no longer walk or crawl; or any under 15 child who presents a paralysis or a weakness of one or more of her or his limbs or is unable to move one or more of her or his limbs from January to December 2021.
Acute Flaccid Paralysis case: Any child under 15 years old of Tillabéri region who presents a flaccid acute paralysis or any person for whom a clinician suspects poliomyelitis from January 2017 to December 2021.
Acute Flaccid Paralysis cases with adequate stool samples: AFP cases with two stool samples, both collected apart within one to two days of interval and within 14 days after paralysis onset and received to the national laboratory in good condition with a completed investigation form.
Priority sites for AFP surveillance: Any place that has the potential to be visited or to host children affected by AFP. Such sites should be visited by health personnel for active research of AFP cases. Priority sites are classified in four categories and the visits frequency are presented as following. Highest priority: ≥2/week, high priority: ≥1/week, medium priority: ≥2/month and low priority: ≥1/month.
Confirmed poliomyelitis case: any case for which laboratory confirmed the presence of the circulating vaccine-derived poliovirus (cVDPV).
Data collection and tools
Data were collected by reviewing the Niger disease surveillance guide [21] and the AFP cases line lists. Community Relays, CHW, district focal point, heads of Health Facilities and Primary Care Units were interviewed using a specifically designed questionnaire on the CBS’s structure and its operation. The working environment was observed, and data were reported on an observation form.
Data analysis
The data were analyzed with Epi-Info 7.2.1.0 software. Qualitative variables were described by proportions and ratios. Quantitative variables were summarized as means and standard deviation or median and Interquartile Range (IQR). Results are presented in text, table and figures. Table 1 summarises the findings of each attribute evaluated.
Ethical considerations
The Ministry of Health of Niger approved the CBS implementation and its data dissemination for knowledge. Participants in the study have voluntarily given their written informed consent. Data were collected and processed in strict anonymity and confidentiality.
AFP CBS was implemented in a security-compromised setting characterised by armed groups’ attacks, causing displacement of the population. Ninety-one per cent (137/150) of Community Relays interviewed reported no attacks in their villages in 2021, while 6.0% (9/150) and 2.7% (4/150) reported 1 to 5 and more than 6 attacks, respectively.
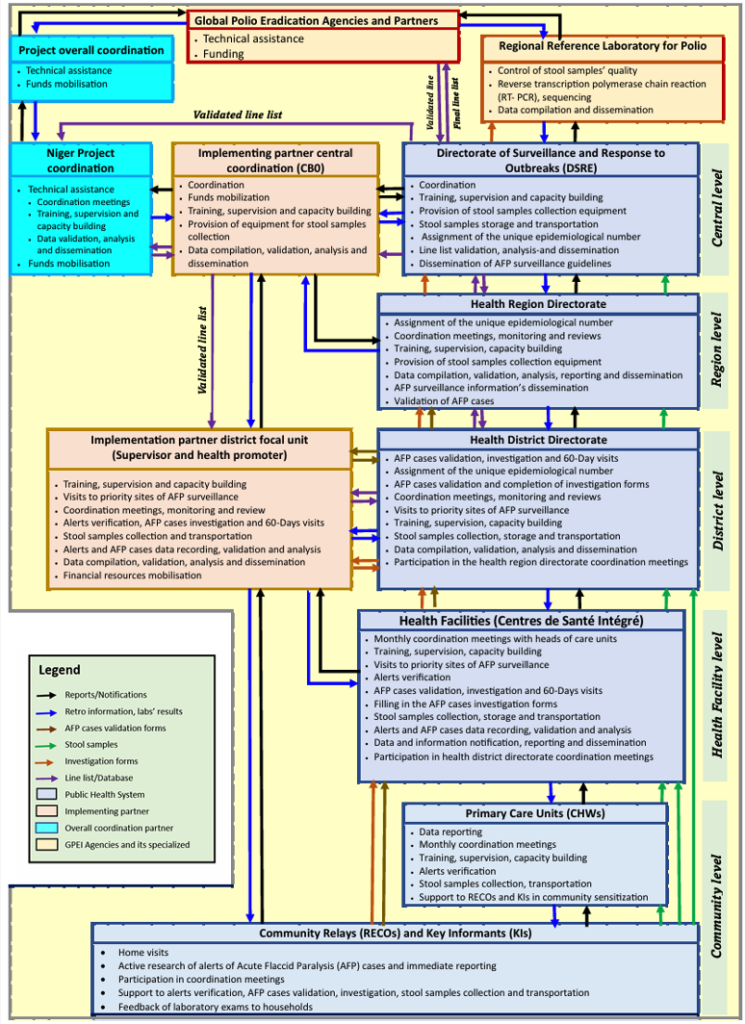
Using the community case definition, Community Relay actively searches for AFP case alerts during home visits, sensitizations and notifies alerts detected to CHW using a free phone call sponsored by the Community-Based Organization (CBO), which was the implementing partner (Figure 2). The CBO coordination office is located in Niamey, 115 kilometres far away from the Tillabéri Health region office and at an average distance of 140 kilometres from the implementation districts (35 kilometres from Kollo, the nearest district, and 248 kilometres from Abala, the farthest district). In each district, the CBO is represented by a focal point based in the capital city of the district. The project coordination team was represented in Niger by a team composed of a country coordinator and a data manager, both based in Niamey, and the overall project coordinator was based in Kinshasa, in the Democratic Republic of Congo, to oversee the project in the four implementing countries: DRC, Cameroon, Chad and Niger.
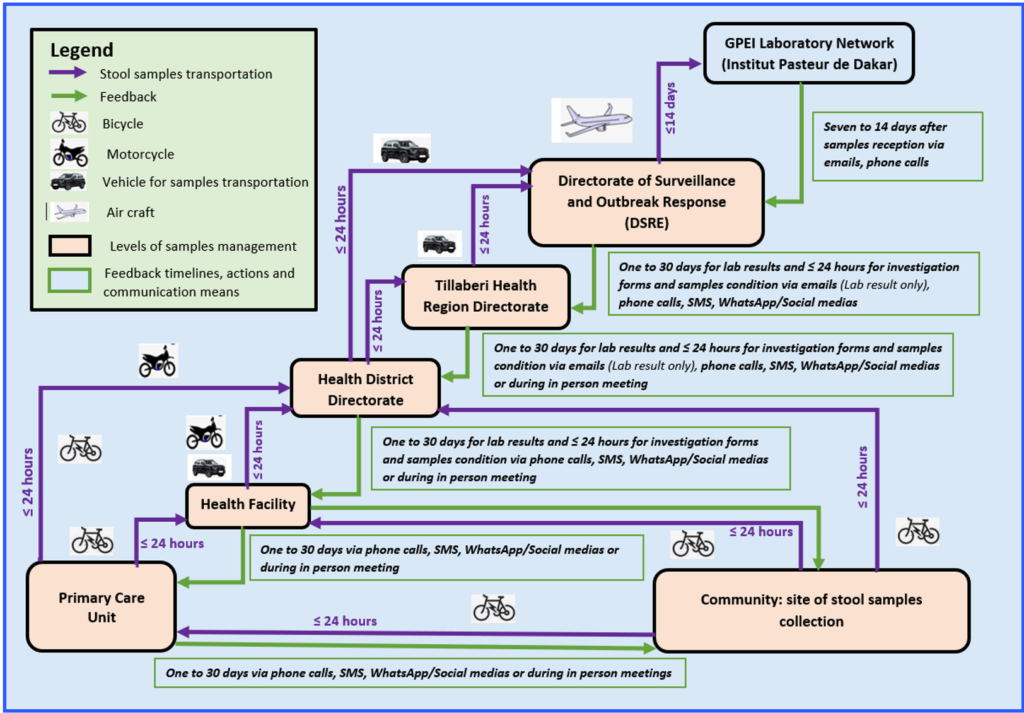
The CHW should verify the existence and conformity of the alert within 24 hours. If the alert is validated as an AFP case, the head of the Health Facility or the district surveillance focal point visits the child within 48 hours for validation, investigation, and stool samples collection (Figure 3). Two stool samples, each weighing 8 to 10 grams or equivalent to the size of an adult thumb, should be taken at 24 to 48-hour intervals within a maximum of 14 days of the paralysis onset. Samples should be kept cool between +2°C and +8°C from the sampling site until they are received at the laboratory with the completed investigation form, within 72 hours after collection of the second sample. The national laboratory is in Niamey, 35 kilometres from the nearest district, Kollo, and 248 kilometres from the farthest district, Abala.
Samples were conveyed to the national laboratory (Figure 3) within 24 to 48 hours by a vehicle positioned in the capital city of each district. Laboratory results are disseminated monthly in terms of feedback through line list sharing by email, cell phone messaging ”Short Message Service (SMS)”. In case of a positive laboratory result, the Tillabéri regional health directorate, the district and the concerned Health Facility are informed immediately. The household hosting children affected by AFP was informed only in case of a positive laboratory result, but not immediately. For AFP cases with inadequate stool samples, an additional investigation is carried out on the 60th day of paralysis onset to collect more data and submit to the National Polio Eradication Committee. Visits to priority AFP surveillance sites are carried out by the head of the Health Facility at a frequency corresponding to the category of each site.
In 2020, surveillance system notified 27 AFP cases in the four districts implementing CBS including 19 cases from August to December and 41.1% (8/19) were notified through CBS. In 2021, 114 AFP cases were reported and 93.0% (106/114) through CBS. All stool samples collected during CBS period were received in Niamey at the reference laboratory of Niger within 24 hours.
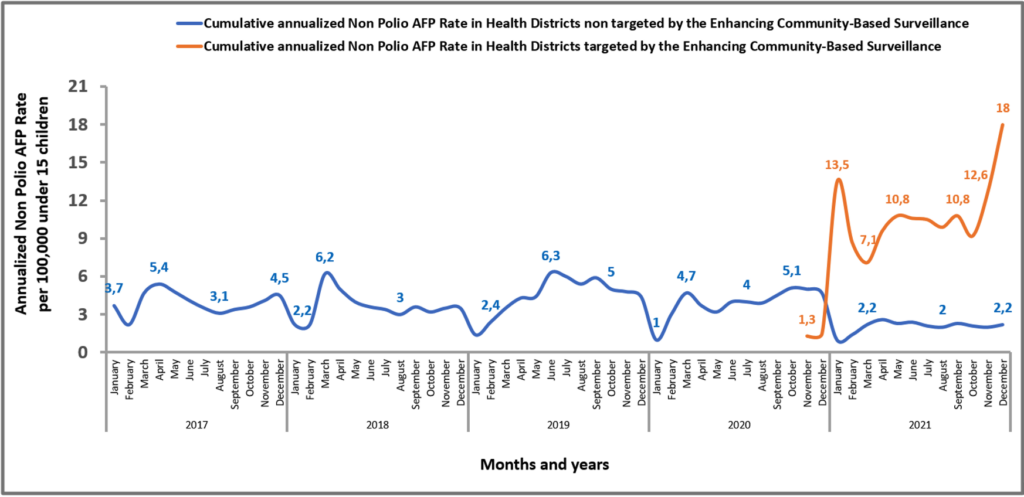
Usefulness and sensitivity
A training on AFP surveillance with a focus on CBS was carried out to build the capacity of actors. The training involved 95.3% (143/150) of Community Relays interviewed, the seven districts focal points and CBO coordination team members. Before project implementation, the annualized NPAFP-R per 100,000 under 15 children rose from 3.7 cases to 5.1 between January 2017 and October 2020, with a median of 3.9, IQR: [3.4 – 4.7] (Figure 4). During the project period (November 2020 to December 2021), it declined from 5 cases to 2.2 cases per 100,000 under 15 children with a median of 2.2, IQR: [2.0 – 2.4] in districts not covered by the project, while in districts covered, it increased from 1.3 cases to 18.0 cases per 100,000 under 15 children over the same period, with a median of 10.2, IQR:[8.7 – 10.8]. From January to December 2021, 87.7% (100/114) of AFP cases were notified by Community Relays (Table 1) and 12.3% (14/114) by Health Facilities. Community Relays notified 84.3% (43/51), 86.7% (13/15), 86.4% (19/22) and 100.0% (26/26) of AFP cases, respectively, in Kollo, Abala, Gothèye and Ayorou districts. One outbreak caused by cVDPV type 2 (cVDPV2) was detected in Kollo district in 2021. Community Relays also reported alerts on other VPD, including measles: 125, meningitis: 03 and Covid-19: 22 (Table 1).
Simplicity
The analysis of the CBS data flow chart indicates that Primary Care Units are the only health entities of the system reporting only to a single upper level. Community Relays, Health Facilities and districts, in addition to reporting at the respective hierarchy, also report to Community Based Organization. Among Community Relays interviewed, 22% (33/150) confirmed the existence of localities that were forbidden access by the authorities because of the insecurity. Poliomyelitis confirmed case includes biological criteria. Completion of some items on the investigation form requires a field visit: geographical coordinates, household socio-economic status, existence of nomadic camps within 5km from the child’s home. Two stool samples, each weighing 8 to 10 grams or equivalent to the size of an adult thumb, should be taken at 24 – 48 hours intervals within a maximum of 14 days after the onset of paralysis. The two samples should be kept cool between +2°C and +8°C from the sample collection site to the laboratory, where they should be received, together with the completed investigation form, within 72 hours of the date of collection of the second sample. The reference laboratory for poliomyelitis confirmation was not available in Niger. IT equipment was available in each district, and every district Focal Point were able to design a graph and table presenting the distribution of AFP cases in place, person, and time. Out of the six criteria defined to assess the simplicity, only two were met (Table 1).
Acceptability
In 2021, all the Community Relays notified 4,596 alerts to supervisors. Among the interviewed Community Relays, 86.7% (130/150) have prompted 1,416 alerts, ranging from 1-72 alerts per Community Relay. For the heads of Health Facilities and CHWs, 81.3% (52/64) and 85.0% (68/80), respectively, participated each month in Community Relays’ supervisions.
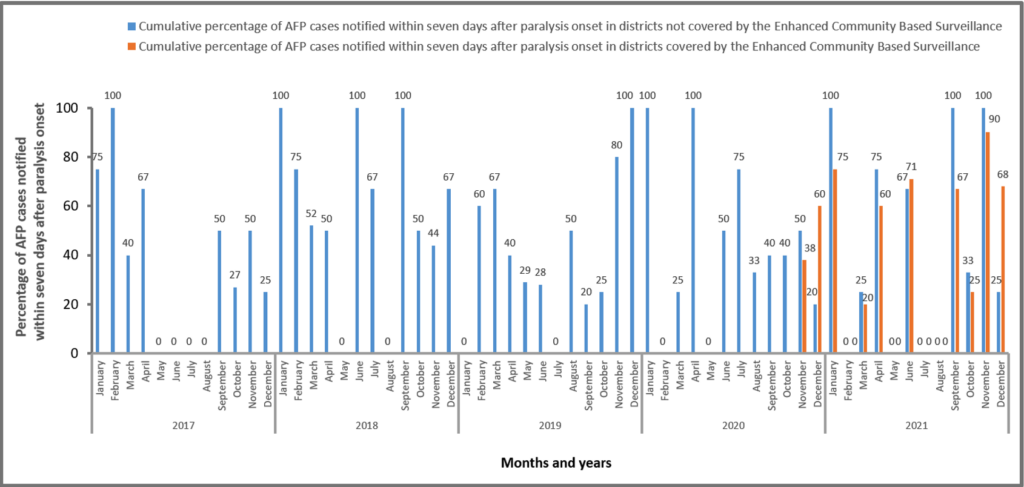
District supervisors verified 88.6% (101/114) of alerts within 48 hours. The proportion of visits to AFP surveillance priority sites performed at least two times per week was 83.5% (212/254) for the 15 highest priority sites, 72.0% (130/181) performed at least one a week for the nine high priority sites, 92.2% (651/706) performed at least twice a month for the 34 medium priority sites and 95.0% (456/480) performed at least once a month for the 32 low priority sites. During the CBS period, for overall 42.1% (8/19) and 65.1% (69/106) cases were notified within seven days after the paralysis’s onset in 2020 and 2021 respectively (Figure 5). When stratified by month and by CBS implementation status, for 82.7% (38/46) months before CBS implementation this criterion was not met, and the situation persisted after the CBS period with 92.9% (13/14) of months not matching the criterion. The percentage of AFP cases with adequate stool samples reported through both CBS’ and Health facilities’ circuits accounted for 94.7% (18/19) and 90.4% (103/114) in 2020 and 2021 respectively while especially for those notified through CBS only it was 87.5% (7/8) and 97.2% (103/106) in the same order.
Timeliness
In 2021, 65.1% (69/106) of cases were notified within seven days after the paralysis’s onset, investigated within 48 hours after notification, and stool samples were all collected within 14 days after paralysis onset and were all received at the national laboratory within 48 hours in good condition. This was less than the 80.0% target (Table 1).
Representativeness
In 2021, the NPAFP-R estimated by the number of AFP cases per 100,000 under 15 children was 15.0 in Abala district, 66.0 in Ayorou district, 13.0 in Gothèye district and 16.0 in Kollo district (Table 1). This was greater than the minimum target of 3+ cases/100,000 per CBS district. Each Primary Care Unit in CBS districts alerted on at least one AFP. Among these alerts, 13.1% (15/114) concerned under one-year children; 84.3% (96/114) were 1 to 4 years old children and 2.6% (3/114) for 5 to 14 years old. The overall male to female sex ratio was 0.96 (56/58) and was 0.86 (7/8) in Abala, 0.5 (9/18) in Ayorou, 1.75 (14/8) in Gothèye and 1.08 (26/24) in Kollo.
Positive Predictive Value
The overall Positive Predictive Value was 1.4% (2/141) (Table 1). In 2020, among the 27 AFP cases notified, one cVDPV2 was isolated, giving a Positive Predictive Value of 3.7%. In 2021, 114 AFP cases were reported, including one cVDPV2, giving a Positive Predictive Value of 1.8%.
The CBS structure shows a proper integration with the existing surveillance system. There was no parallel mechanism to the existing system, but rather a collaboration and partnership with the national surveillance directorate and its decentralized entities at each health system level.
The absence of a CBS regional coordination position based in Tillabéri could affect the activities execution, collaboration and partnership coordination with the regional health directorate and other health partners in the region. The absence of representatives of the implementing partner at Health Facility and Primary Care Unit levels is explained by their plethora, but the district focal points participated in the coordination of monthly meetings organized by the CHWs with the Community Relays. The performance achieved in stool samples management was attributable to the deployment in each district of an all-terrain vehicle dedicated exclusively to the supervision and transport of stool samples. According to the circuit, data, and reports from one level were not submitted to only the one immediately above. Community relays report to Primary Care Unit and also to the CBO’s partner district focal point and likewise the Health Facility reports to district and to CBO. In addition, it is impossible to complete the investigation form without conducting a field visit, and managing an AFP case in accordance with WHO guidelines requires deadlines to be met, making AFP surveillance a restrictive and complex system.
The intervention demonstrated a significant increase in the NPAFP-R in the CBS implementation districts, with values reaching 5 to 10 times those of districts not covered by the CBS, and 3 to 4 times those of non-polio AFP before the implementation period matching with the criteria defined for usefulness. The achievement of the expected Non-Polio AFP rate also demonstrates the sensitivity of the CBS in the district covered. The low positive predictive value obtained in the context of Community engagement, where notified alerts are validated as AFP cases prior to investigation, would also attest to the sensitivity of CBS in detecting AFP cases. The increased sensitivity of AFP surveillance through CBS has also been reported in several African countries [8-14, 22], in Cambodia [23] and by the GPEI [24]. In addition to AFP cases, the Community Relays reported other diseases under surveillance. This shows that Community Relays’ competence field can be extended to other vaccine-preventable diseases, public health events and other community-based interventions, such as newborn and child disease management, community-based contraceptive distribution, antenatal care and mortality surveillance [25-32].
There was no difference observed in the proportion of adequate stool and the proportion of stools received at the laboratory in good condition. Almost all Community Health Workers notified at least one alert, but over one fifth of cases were not notified within 7 days after paralysis onset and all priority sites were not adequately visited. These indicators reveal the gaps in the existing CBS to achieve the acceptable system criteria. In this study, the time unit for measurement of stool sample delivery was days rather than hours, and this lack of precision could have led to the current finding. However, other authors have reported an increase in the proportion of AFP cases with adequate stool samples [8-10, 14]. The notification of alerts by almost all Community Relays interviewed shows how committed and adherent they were to the established system.
The participation of CHWs and the heads of Health Facility in the verification of alerts and in supervision, the incorporation of the AFP cases notified by Community Relays in the unified unique line list of AFP cases in the country indicates that there was no parallel surveillance system and that there was a collaboration between all the stakeholders at different health system levels and constitute one of the indications for the sustainability of this approach.
The proportion of cases notified within seven days after the onset of paralysis did not increase between the non-implementation and the implementation periods of CBS, and also between the covered and non-covered districts. This indicates that there was no difference between the indicator-based detection system run by the Health Facilities and the CBS in the early detection and notification of AFP cases. The parameters that contributed to the performance of the Community Relays in notifying alerts could be the motivational mechanism in place, particularly the allocation of cell phones to each Community Relay, and the fleeting of all phones for free calls, the monthly systematic financial incentive for each Community Relay and the additional financial incentive for each alert validated as an AFP case.
Just over two-thirds of cases were notified within seven days after the onset of paralysis, and this did not meet the indicator defined for the CBS timeliness. This proportion, lower than the 80.0% expected, indicates a lack of community support for the CBS, probably linked to Community Relays’ enrolment procedures, insufficient coverage of villages and localities by Community Relay, their recognition by community and leaders as the support workforce for diseases surveillance and the lack of official installation and introduction of Community Relays in their various localities under their scope. Other studies reported shorter average notification times, ranging from 4 to 6 days in southern Sudan, and from 3.73 to 5.4 days in Somalia [10, 15]. However, alerts notified in this study were all verified within 48 hours, validated AFP cases were investigated within 48 hours, and stool samples were collected within 48 hours and received at the national laboratory in Niamey within 48 hours. This performance can be attributed to the participation of the Health Facilities and the Primary Care Unit personnel in the verification, investigation and samples collection phases; the establishment of a freephone communication fleet including all actors; the positioning of all-terrain vehicle in each covered district; the proximity of the CBS implementation districts to the capital Niamey where the national laboratory is located [33].
All age groups were represented in the reported cases and in the four districts, with most cases aged under 5 years [34-38]. The origin of AFP cases from all the implementation districts and the achievement of the NPAFP-R threshold in each of these districts demonstrate the functionality of the CBS. Overall, male cases were slightly less numerous than female cases, with an inverse trend in two of the four districts. However, the literature reports a much higher notification trend for boys than for girls, varying between 10.0% and 60.0% [12, 34-37, 39-43].
The community engagement against poliomyelitis through community leaders and Community Relays in the districts of Abala, Ayorou, Kollo and Gothèye led by a CBO have pointed out the importance of public and private partnership and collaboration for the implementation of health interventions like disease surveillance even in a context of insecurity. Through this collaboration, more AFP cases were detected, investigated, notified, and cVDPV2 epidemics were detected, making the CBS a useful strategy.
It was easy for Community Relays to use the case definition to detect alerts. It was also easy for them to communicate and notify cases, but the risk of armed group attacks was a real threat at any time and was felt daily by field actors. The existence of forbidden zones made activities in these areas more complex, and limited access for the populations living there to disease surveillance activities. The detection, investigation, notification and coordination mechanisms in place were accepted by all involved stakeholders but were limited by the security constraints and measures in place.
To strengthen the CBS, Community Relays should be officially installed and introduced to their respective communities. It is also necessary to monitor every month the indicator related to the early alerts’ notification during the periodic coordination meetings to deepen the causal analysis and provide appropriate solutions. For areas with limited access, it is possible to identify and train some residents living in these areas and build their capacities and provide them with equipment to detect and notify alerts. However, the transportation of children with AFP residing in these forbidden areas to those with free access for verification and investigations should be maintained. Furthermore, the termination of external funding represents a risk to the performance of the CBS strategy. To preserve the achievements of this CBS model and ensure its sustainability, it is essential to start establishing appropriate mechanisms in the Tillaberi context.
This may include an appropriate specific communication strategy for the local communities, administrative, political, religious and customary authorities, and other leaders, to mobilize local resources to support poliomyelitis eradication activities and the control of other diseases and public health events. Consultations with all stakeholders is also essential to reach a consensus on the nature and consistency of incentives, including financial ones that can be mobilized locally to support surveillance. Consideration should also be given to the possibility of integrating all CBS activities into the districts action plans and Health Facilities micro plans. All these actions could be the subject of a multi-sectoral action plan drawn up in a participatory and inclusive manner, which could serve as an advocacy document to mobilize external resources.
What is already known about the topic
What this study adds
A.M.T.A developed the protocol of the study, supervised data collection, data processing and analysis, developed and reviewed the manuscript. I.D, H.S and A.A.H supervised data collection, participated in data processing and analysis, participated in manuscript development and review. M.C.F. T.I., H.H., I.H., O.M, M.K, S.S, I.n.A.C facilitated data collection and compilation. K.M, Y.B, R.B and S.A participated in protocol and manuscript preparation and review. All authors read and approved the final manuscript.
Table 1: Criteria of the evaluation’s attributes of the Community-Based Surveillance of poliomyelitis in Tillabéri Health Region, Niger, 2020–2021
| Attributes | Criteria of evaluation | Expected Answer/Value | Evaluation findings | Evaluation decision |
|---|---|---|---|---|
| Usefulnesss | Non-Polio AFP Rate (NPAFP-R) during the Enhanced Community Based Surveillance (E-CBS)is higher than the NPAFP-R before the implementation of the E-CBS | Yes | Yes | Useful |
| Percentage of AFP cases notified through CBS | ≥ 80.0% | 87.7% | ||
| Detection of Poliomyelitis epidemics | Yes | Yes | ||
| CBS personnel trained on Acute Flaccid Paralysis surveillance | Yes | Yes | ||
| Notification of other Vaccine Preventable Diseases | Yes | Yes (Measles: 125, Meningitis: 03, COVID-19: 22) | ||
| Sensitivity | NPAFP-R ≥ 3.0/100,000 under 15 children in the districts implementing CBS | Yes | Yes | Sensitive |
| Simplicity | Each level reports only to another one and no biological criteria to confirm poliomyelitis case | Yes | No | Complex |
| Completion of the investigation form and stool specimen collection don’t require field visit and no constraints in sample collection and transport | Yes | No | ||
| Availability of data management equipment at district level | Yes | Yes | ||
| Ability for focal point to present CBS in person, place, and time | Yes | Yes | ||
| Acceptability | Proportion of Community Relays having alerted on at least one AFP | ≥80.0% | 86.7% (130/150) | Not acceptable |
| Proportion of Heads of Health Facilities participating in CHW supervision | ≥80.0% | 85% (68/80) | ||
| Percentage of AFP alerts verified | ≥80.0% | 88.6% (101/114) | ||
| Percentage of AFP cases notified within seven days after paralysis onset | ≥80.0% | 65.1% (69/106) | ||
| Percentage of AFP cases with adequate stool samples | ≥80.0% | 100.0% (102/102) | ||
| Proportion of AFP surveillance priority sites adequately visited | ≥80.0% |
| ||
| Timeliness | Percentage of AFP cases notified by Community Relays within 7 days after paralysis onset investigated within 48 hours and whose stool samples were received at National laboratory in good condition within 72 hours | ≥80.0% | 65.1% (69/106) | Not reactive |
| Representativeness | Non-Polio AFP Rate in each district implementing CBS | ≥3.0 AFP cases per 100,000 under 15 children |
| Representative |
| Proportion of children aged less than one year, one to four years and five to fourteen years within AFP cases notified | >0.0% in each age group |
| ||
| Positive Predictive Value | Percentage of biologically confirmed cases out of those tested in laboratory | <5.0% | 1.4% | Appropriate |