Research![]() | Volume 8, Article 24, 22 Apr 2025
| Volume 8, Article 24, 22 Apr 2025
Cyril Kwami Azornu1,2,&, Abubakari Ibrahim3, Adjei Kwabena Sarfo3, Magdalene Akos Odikro4, George Akowuah4, Gyesi Razak Issahaku4,5, Abdul-Jaleel Mumuni6, Delia Akosua Bandoh4, Ernest Kenu4, Chrysantus Kubio3
1Salaga Municipal Hospital, Savannah Region, Ghana Health Service, Salaga, 2Catholic University of Ghana, School of Public Health & Allied Sciences, Fiapre-Sunyani, 3Regional Health Directorate, Ghana Health Service, Damongo, Savannah Region, Ghana, 4Ghana Field Epidemiology and Laboratory Training Program, School of Public Health, College of Health Sciences, University of Ghana, Legon, Accra, 5Tamale Teaching Hospital, Ministry of Health, Tamale, Ghana, 6North East Gonja District Health Directorate, Kpalbe, Savannah Region, Ghana
&Corresponding author: Cyril Kwami Azornu, Salaga Municipal Hospital, Savannah Region, Ghana Health Service, Salaga, Ghana. Email address: cyrilazornu23@gmail.com
Received: 18 Dec 2024, Accepted: 03 Mar 2025, Published: 22 Apr 2025
Domain: Maternal and Child Health, Nutrition
Keywords: Undernutrition; stunting; children under five; Savannah Region
©Cyril Kwami Azornu et al Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Cyril Kwami Azornu et al Five-year review on prevalence of stunting among children under five years in Savannah Region, Ghana. Journal of Interventional Epidemiology and Public Health. 2025;8:24. https://doi.org/10.37432/jieph-d-24-02056
Introduction: Undernutrition, specifically stunting, continues to be a major public health concern, especially in Africa and Asia. The World Health Organization targets a 40% reduction in stunting by 2025. However, there has been no known scholarly work to assess the stunting situation in the Savannah Region in line with the WHO’s target. This study described the trends and geographical distribution of stunting among children under five in the Savannah region of Ghana from 2017 to 2021.
Method: A cross-sectional prevalence study was conducted to analyze secondary data on stunting from routine service provision from 2017-2021. Data extracted from the District Health Information Management Systems version 2 was cleaned and analyzed with Microsoft Excel version 2021 and ArcMap version 10.3. Proportions were calculated and the results were presented as tables, charts, and geospatial maps.
Results: The proportion of children under five measured for stunting increased from 14.6% (14,694/100,417) in 2017 to 70.7% (92,309/130,653) in 2021. Over the period, the prevalence of stunting among children under five was 1.1% (2591/246691). There was a decreasing trend in the prevalence of stunting from 1.80% (265/14,694) in 2017 to 0.85% (782/92309) in 2021. The West Gonja, Central Gonja, and North-East Gonja districts recorded the highest prevalence of stunting while the East Gonja municipality recorded the lowest prevalence.
Conclusion: The prevalence of stunting in this study was very low compared to the global and national prevalence. A decreasing trend was observed over the period. Measures should be put in place to ensure all stunting cases are detected early.
Undernutrition among children remains a significant public health challenge in developing countries. Worldwide, undernutrition is responsible for over a third of child mortalities which can be avoided through public health interventions [1]. Stunting, or being too short for one’s age, is defined as a height that is more than two standard deviations below the World Health Organization (WHO) child growth standards median [2]. A joint report by the United Nations Children’s Fund (UNICEF), WHO, and World Bank indicated that globally, 149.2 million children, representing 22.0% of children below five years suffered from stunting in 2020 [3]. Undernutrition is especially common in developing countries, specifically in Asia and Africa, which account for the greatest share of undernutrition worldwide. In 2020, 53% and 41% of all stunted children under the age of five lived in Asia and Africa respectively [3]. Undernutrition has both short- and long-term effects on the health of children and affects economic productivity as it leads to serious consequences in adult life [4]. Therefore, sufficient nutrition must be provided during the early years of life to promote healthy growth, organ development and function, a strong immune system, and the growth and development of the nervous system and the brain [1].
In Ghana, a review of the Ghana Demographic and Health Survey (GDHS) conducted from 1993 to 2014 revealed a statistically significant reduction in childhood stunting for the years 2008 and 2014 compared to 1993, 1998, and 2003 [5]. Nonetheless, the proportion of stunting is still high as reviews of the 2008 GDHS and the fourth Ghana Multiple Indicator Cluster Survey (MICS4) conducted in 2011 data revealed that 27.5% of children under five years of age in Ghana are stunted [6,7]. Reviews of data from the 2014 GDHS however reported the prevalence of stunting to range between 18.4% and 19.6% (8–11). This brings to light the evidence of a decline in the prevalence of stunting among children in Ghana [5,12]. Similar to the findings from the GDHS 2008 and MICS4, stunting prevalence ranged between 15.0% to 27.2% in northern Ghana [13-14]. Further, the GDHS 2022 found that 17.5% of children under five years were stunted nationwide and the prevalence of stunting in the Savannah region was 21.0% [15]. On the other hand, studies from other African countries including the Democratic Republic of Congo (DRC), Kenya, Mozambique, and Nigeria found the prevalence of stunting to range between 20.0% and 50.0% [16–18]
In 2012, WHO set a target to reduce by 40% the number of stunted children under five years of age by 2025 [19]. Ghana started measuring length/height as part of routine service provision in 2017 to track the progress of linear growth in children under five years. However, since the inception of the system, there has been no known scholarly work to assess the impact of the intervention to track the progress being made towards achieving the WHO target and also describe data generated on stunting in the Savannah region. Identifying the trend and geographical distribution of stunting cases in the region will therefore be a crucial step in helping tailor interventions towards achieving the WHO target. This study therefore described the stunting surveillance data among children under five years in the Savannah Region to determine trends and geographical distribution from 2017 to 2021.
Study Area
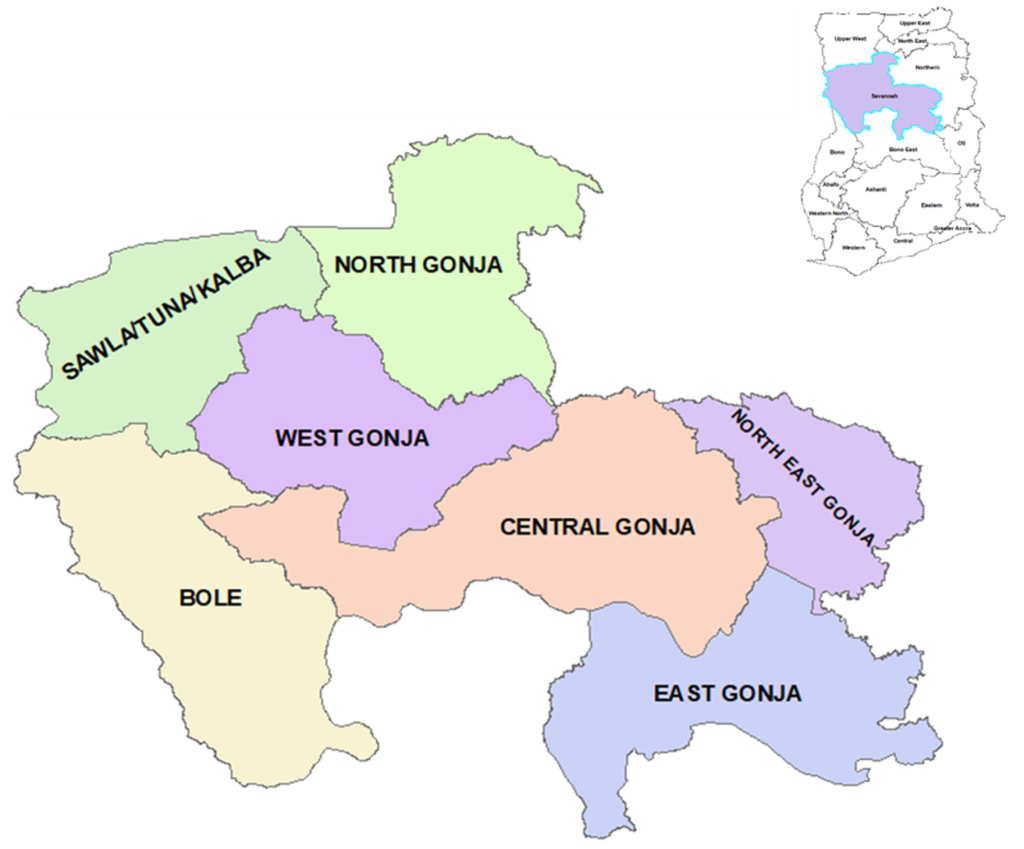
The study was conducted in the Savannah Region of Ghana. It is one of the two regions created in 2019 from the then Northern Region. With Damongo serving as the regional capital, the region is the largest in the nation in terms of land cover, spanning over 35,853 square kilometers and accounting for 15% of Ghana’s total land area. Locally, the region is bordered by the Oti Region to the East, Bono East Region to the South, and the Bono Region to the West. It also shares boundaries with the North East, Northern, and Upper West Regions to the North. The region is also bordered by Burkina Faso and La Cote D’Ivoire to the West internationally. The region is made up of seven administrative districts namely Bole, East Gonja, North Gonja, North-East Gonja, West Gonja, Central Gonja, and Sawla-Tuna-Kalba Districts. Health services in the Region are provided by a network of Sub-district health facilities comprising Hospitals, Polyclinics, Health centers, Clinics and Community-based Health Planning Services (CHPS) Compounds. There are 40 sub-districts with 206 health facilities in the region which serve a population of 680,991 people of whom 136,198 (20%) are children under five years. Agriculture is the main economic activity in the region with over 90% of the productive age group being peasant farmers. The main food crops produced are cereals, tubers, and groundnuts [20].
Study Design
We employed a descriptive cross-sectional prevalence study to describe the trend and geographical distribution of stunting among children under five from 2017-2021 in the Savannah Region using data abstracted from the District Health Information Management Systems version 2 (DHIMS2).
Study Population
The study population consisted of children aged 0-59 months who were measured for stunting in the Savannah Region from 2017-2021.
Data Abstraction and Cleaning
Aggregate data on stunting among children 0-59 months was abstracted from all health facilities in the Savannah Region reporting into DHIMS2. Data was abstracted on the number of children 0-59 months who were evaluated for stunting and the number who were stunted from 2017-2021. The stunting data entered into the DHIMS is generated using the WHO procedure which involves using a calibrated wooden or plastic board with a headpiece and a movable footpiece which is used in measuring the height or length of children 0-59 months of age. A child with a height-for-age Z-score (HAZ) less than -2 SDs was classified as moderate stunting whereas a HAZ less than -3 SDs was classified as severe stunting [21]. Data was extracted on the number of children measured and the number who were stunted. Also, population data for the Savannah region for the same period was extracted. The abstracted data was exported into Microsoft Excel software version 2021 for cleaning.
Inclusion and Exclusion Criteria
All health facilities in the Savannah Region that reported data on stunting for 2017 to 2021 in the DHIMS were included in the study. However, facilities with incomplete or missing data on stunting for the period under study were excluded from the study.
Data analysis
A descriptive analysis of the cleaned data was conducted using Microsoft Excel software version 2021 and ArcGIS software version 10.3. A total of 246,691 records representing 43.5% of the target population over the 5 years was used in this study. Data was analyzed according to place and time. The 0-59 months’ population was computed by calculating 20% of the general population data that was abstracted. The percentage of children 0-59 months who were evaluated for stunting was computed by dividing the under-five population by the number of children evaluated to identify the coverage of measurement of stunting. Also, the prevalence of both moderate and severe stunting among children 0-59 months was computed by dividing the number of children 0-59 months who were stunted by the total number of children 0-59 months who were evaluated for stunting. The results were presented using tables, charts, and maps.
Ethical Consideration
Administrative clearance to use the data in DHIMS2 was obtained from the Savannah Regional Health Directorate. Ethical clearance was not needed for this work because the data was generated from routine service provision. All data and records were secured on a computer with a password that was made available to only authorized persons who were working on the study.
The proportion of children under five years evaluated for stunting
A total of 246,691 children were evaluated for stunting from 2017-2021. Of these, 1.1% (2,591/246,691) were stunted. The proportion of children under five years evaluated for stunting in the Savannah region increased progressively across the period from 14.6% (14,694/100,417) in 2017 to 70.7% (92,309/130,653) in 2021. Among the children evaluated, the proportion of moderate stunting in 2017 was 1.70% (249/14,694) while the proportion of severe stunting was 0.11% (16/14,694). Also, in 2021, the proportion of moderate stunting was 0.77% (709/92,309) while the proportion of severe stunting was 0.08% (73/92,309) (Table 1)
Trend of Stunting in the Savannah Region
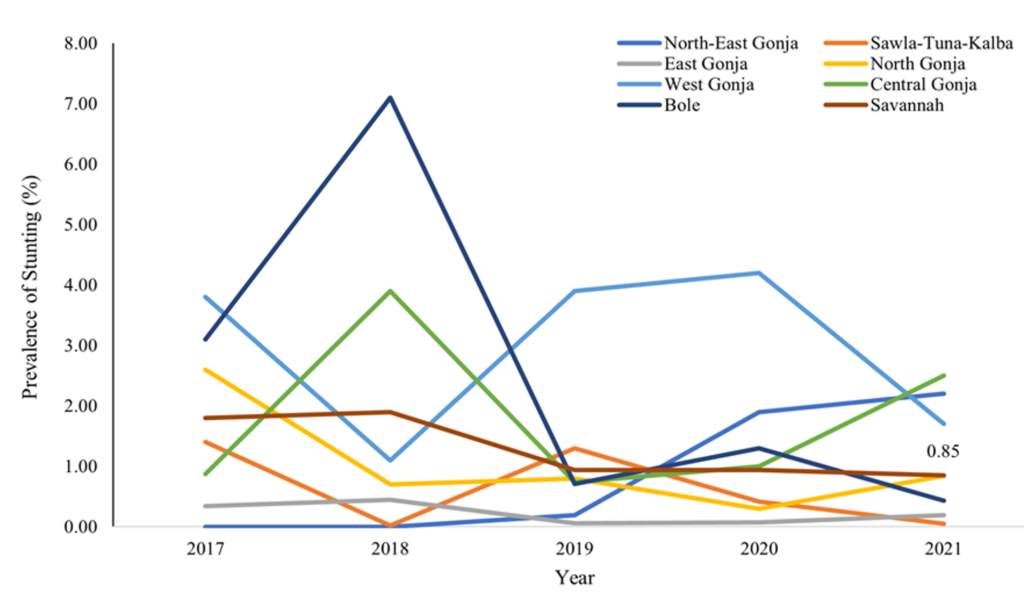
Over the period, the cumulative proportion of stunted children under 5 was 1.1% (2591/246691). The highest proportion of stunted children [446/22886 (1.9%)] was recorded in 2018 and the lowest proportion of stunted children [782/92309 (0.85%)] was recorded in 2021. The Bole and Central Gonja districts recorded a sharp increase in stunting prevalence from 2017 to 2018, followed by a sharp decrease in 2019. On the other hand, the West Gonja, North Gonja, and Sawla-Tuna-Kalba districts recorded a sharp decrease in stunting prevalence from, 2017 to 2018 followed by an increase in 2019. Also, the North-East Gonja district recorded a steady increase in stunting prevalence from 2017 to 2019. The highest annual stunting prevalence (7.1%) was reported by Bole district in 2018, followed by West Gonja district (4.2%) in 2020, while the lowest annual prevalence of stunting (0.0%) was recorded in the North-East Gonja district in 2017 and 2018. Overall, the proportion of stunting increased slightly between 2017 to 2018 in the region. This was followed by a sharp decline in 2019 and a further slight decline in 2021. (Figure 2)
Geo-Spatial Distribution of Stunting among Children under five
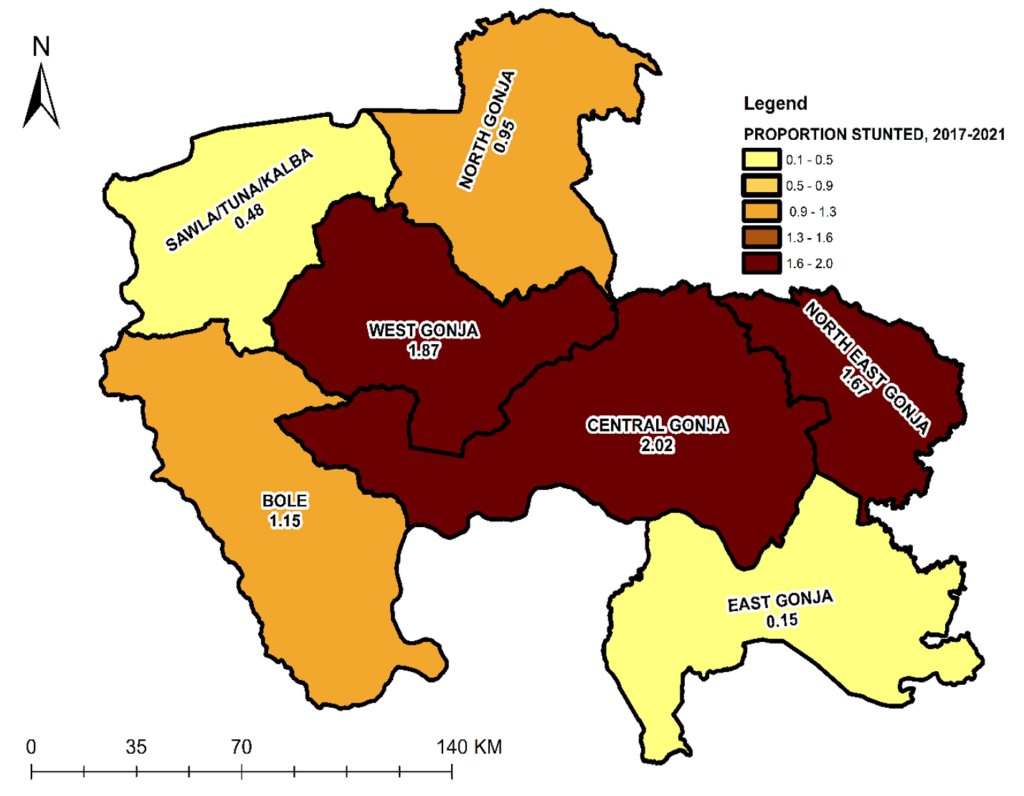
Over the five-year period, the highest prevalence of stunting among children measured was recorded in the Central Gonja (2.02%), West Gonja (1.87%), and North-East Gonja (1.67%) districts while the lowest prevalence was recorded in the East Gonja municipality (0.15%) and Sawla/Tuna/Kalba district (0.48%). (Figure 3)
This study analysed stunting surveillance data among children under five years old in the Savannah Region from 2017 to 2021. Overall, the prevalence of stunting among children under five years in the Savannah region was low. This prevalence was observed to decrease as the years progressed. The Central Gonja, West Gonja and North-East Gonja districts reported the highest prevalence of stunting and the East Gonja Municipality reported the lowest prevalence of stunting among children measured.
The overall prevalence of stunting in the Savannah Region was very low compared to what was found in studies in DRC, Kenya, Mozambique, and Nigeria, which reported stunting prevalences from 20.0% to 50.0% [16–18] and the global prevalence of 21.3% and 22.0% reported in joint reports by UNICEF, WHO, and World Bank for 2019 and 2020 respectively [3,22]. Similarly, compared with other nationally representative samples in Ghana, the prevalence of stunting was low in the Savannah region. Analysis of data from the 2014 GDHS reported the prevalence of stunting to range between 18.4% and 19.6% [8–11] and the 2022 GDHS reported the prevalence of stunting to be 17.5% (16). Also, studies by individuals in different parts of Ghana found the prevalence of stunting ranging from 3% to 15% [4,14,23]. This finding also differs from the prevalence of 21.0% reported for the Savannah region from the 2022 GDHS [15]. The difference in the prevalence of stunting between the current study and other studies conducted in Ghana and other African countries could be due to the study design. While the other studies employed a prospective method to collect primary data, this study employed a retrospective method using secondary data. The collection of primary data could allow the researchers to have a better control over the quality of the data collected by observing strict precautions. Further, when stunting was measured using Mat and WHO procedures in the Tain District, a prevalence of 3.7% and 11.7% respectively was found [24]. This brings to light the impact of the measurement procedure used on the outcome of interest. It was reported that the WHO procedure for measuring stunting was more sensitive than the Mat procedure [24]. It is however worth noting that the measurements during routine service provision are done using the WHO procedure. This therefore raises concerns regarding the level of precautions followed by service providers when measurements are being done during routine service provision. While the low prevalence of stunting in the Savannah region may seem good, there is a cause for concern as there could be more cases of stunting undetected through measurement during routine service provision.
The proportion of children under five years evaluated for stunting increased year after year throughout the period under consideration. Overall, the prevalence of stunting among children measured reduced progressively from 2018 to 2021 after it increased slightly between 2017 and 2018 in the region. The decreasing trend in stunting observed is consistent with what was found by Amoako and colleagues who reported a decreasing trend in the prevalence of childhood stunting in their reviews of data from GDHS conducted from 1993 to 2014 [5,12]. A similar decreasing trend was also reported in Uganda, Rwanda, Tanzania, and Nepal [25–29]. While this study found an overall decreasing trend in the prevalence of stunting among children under five, the Central Gonja, East Gonja, and North-East Gonja districts observed an increasing trend from 2019 to 2021. The increasing trend observed in these districts could be associated with the increase in coverage of children being measured for stunting hence increasing the rate of detection.
The geographic disparity in health outcomes is of significant concern to the Ghana Health Service as it helps target interventions [30–32]. Geographically, stunting cases were reported in all the districts with spatial variations in the region. This implies all the districts in the region are affected by stunting. Though there are spatial variations, other studies reported stunting being predominantly present in the northern regions compared to the southern regions [5,11]. The geographical distribution observed in this study could be due to a mix of demographic and socioeconomic characteristics in the northern regions [5] such as high fertility rate, low access to health services, high poverty levels, poor infant-feeding practices, inadequate sanitation facilities, and low levels of maternal education compared to the southern regions [10, 28–35]. The spatial variations observed in this study could be used to target public health nutrition interventions in the districts with a higher prevalence of stunting.
Strengths and Limitations
The data used for this study was retrieved from a trusted reporting system used in Ghana Health Service which ensures data validation at the various levels of service provision and administration. Also, data for the whole region was available for use thereby increasing the power of the study.
This study however had a limitation in the quality of the data. The data reported is only aggregated data hence it was not possible to determine age- and sex-specific variations in the analysis. Also, it cannot be ascertained whether the recommended measurement procedures were used throughout the period under consideration at all facilities that reported data into the DHIMS 2.
The prevalence of stunting under five years in the Savannah region from 2017 to 2021 was below the global and national prevalence. The prevalence of stunting decreased progressively over the five year study period. The West Gonja, Central Gonja, and North-East Gonja districts recorded the highest prevalence of stunting among children under five measured.
We recommend an improvement in undernutrition surveillance by Ghana Health Service to ensure proper levels of precautions are used during measurements to ensure all stunted children are identified early. Proper feeding practices and programs to improve childhood nutrition should also be scaled up in districts with high prevalence of stunting. The Ghana Health Service should modify the reporting format to include age- and sex-specific variables. Future studies should use primary data to confirm what was found in this study and further investigate the disparities in stunting by districts observed.
What is already known about the topic
What this study adds
| 2017 | 2018 | 2019 | 2020 | 2021 | Total | |
|---|---|---|---|---|---|---|
| Target Population | 100,417 | 105,273 | 105,161 | 125,060 | 130,653 | 556,564 |
| Total 0-11 months measured | 5,605 | 14,986 | 19,832 | 30,881 | 41,634 | 112,938 |
| Total 12-23 months measured | 4,668 | 4,680 | 14,737 | 23,143 | 29,190 | 76,418 |
| Total 24-59 months measured | 4,421 | 3,220 | 11,449 | 16,760 | 21,485 | 57,335 |
| Total measured 0-59 months [n(%)] | 14,694 (14.6%) | 22,886 (21.7%) | 46,018 (43.8%) | 70,784 (56.6%) | 92,309 (70.7%) | 246,691 (44.3%) |
| Total moderate stunting 0-59 months [n(%)] | 249 (1.70%) | 378 (1.70%) | 395 (0.86%) | 548 (0.77%) | 709 (0.77%) | 2,279 (0.92%) |
| Total severe stunting 0-59 months [n(%)] | 16 (0.11%) | 68 (0.30%) | 38 (0.08%) | 117 (0.17%) | 73 (0.08%) | 312 (0.13%) |
| Total stunting 0-59 months [n(%)] | 265 (1.80%) | 446 (1.90%) | 433 (0.94%) | 665 (0.94%) | 782 (0.85%) | 2,591 (1.1%) |
Views: 4,928
Menu, Tables and Figures
| 2017 | 2018 | 2019 | 2020 | 2021 | Total | |
|---|---|---|---|---|---|---|
| Target Population | 100,417 | 105,273 | 105,161 | 125,060 | 130,653 | 556,564 |
| Total 0-11 months measured | 5,605 | 14,986 | 19,832 | 30,881 | 41,634 | 112,938 |
| Total 12-23 months measured | 4,668 | 4,680 | 14,737 | 23,143 | 29,190 | 76,418 |
| Total 24-59 months measured | 4,421 | 3,220 | 11,449 | 16,760 | 21,485 | 57,335 |
| Total measured 0-59 months [n(%)] | 14,694 (14.6%) | 22,886 (21.7%) | 46,018 (43.8%) | 70,784 (56.6%) | 92,309 (70.7%) | 246,691 (44.3%) |
| Total moderate stunting 0-59 months [n(%)] | 249 (1.70%) | 378 (1.70%) | 395 (0.86%) | 548 (0.77%) | 709 (0.77%) | 2,279 (0.92%) |
| Total severe stunting 0-59 months [n(%)] | 16 (0.11%) | 68 (0.30%) | 38 (0.08%) | 117 (0.17%) | 73 (0.08%) | 312 (0.13%) |
| Total stunting 0-59 months [n(%)] | 265 (1.80%) | 446 (1.90%) | 433 (0.94%) | 665 (0.94%) | 782 (0.85%) | 2,591 (1.1%) |