Research | Open Access | Volume 8 (2): Article 42 | Published: 06 Jun 2025
Williams Azumah Abanga1,&, Adjei Sarfo Kwabena2, Jonas Adodoo2, Gyesi Razak Issahaku3, George Akowuah4, Magdalene Akos Odikro4, Delia Akosua Bandoh4, Ernest Kenu4, Chrysantus Kubio2
1Saboba District Health Directorate, Ghana Health Service, Saboba, Ghana, 2Savannah Regional Health Directorate, Ghana Health Service, Damongo, Ghana, 3Laboratory Department, Tamale Teaching Hospital, Tamale, Ghana, 4Ghana Field Epidemiology and Laboratory Training Programme (GFELTP), School of Public Health, University of Ghana, Accra, Ghana.
&Corresponding author: Williams Azumah Abanga, Saboba District Health Directorate, Ghana Health Service, Saboba, Ghana, Email: willabanga@gmail.com, ORCID: https://orcid.org/0009-0003-6523-3171
Received: 01 Feb 2025, Accepted: 04 Jun 2025, Published: 06 Jun 2025
Domain: Neglected Disease Epidemiology; Environmental Health
Keywords: Snakebite, incidence, Savannah Region, DHIMS 2, Neglected Tropical Disease
©Williams Azumah Abanga et al Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Williams Azumah Abanga et al Geospatial and temporal pattern of reported snakebite cases to health facilities in the Savannah Region, Ghana, 2018 – 2022. Journal of Interventional Epidemiology and Public Health. 2025;8:42. https://doi.org/10.37432/jieph-d-25-00040
Introduction: Snakebite is a neglected public health issue in tropical regions. Snakebite incidents in Sub-Saharan Africa are underreported. There is inadequate information on the snakebite burden in the Savannah Region of Ghana. Analysing snakebite surveillance data will help in planning appropriate control and prevention strategies. This study determined the magnitude, distribution and geographical variation of snakebites in the Savannah Region.
Methods: We conducted a descriptive secondary data analysis of snakebites in the Savannah Region using 2018 to 2022 surveillance data extracted from the District Health Information Management System 2 database. Snakebite morbidity and mortality data on age, sex, district of reported bite, month and year were extracted. Statistical analyses were performed using Microsoft Excel version 2016 and ArcGIS version 10.4. Results were presented in tables, graphs and maps.
Results: A total of 3,013 snakebite cases were recorded over the five-year period with an average incidence of 101 cases per 100,000 population [95% CI: 92.7 – 108.9]. Young adults aged 20-34 years were more affected, 30.8% [95% CI: 29.2 – 32.5]. The majority of snakebite cases were males, 67.3% [95% CI: 65.5 – 69.0]. The incidence declined over the period, with the highest, 118 per 100,000, recorded in 2019 and the lowest, 84 per 100,000, reported in 2022. The district cumulative incidence varied from 312 to 626 cases per 100,000 population in the East Gonja and Central Gonja Districts, respectively. The majority of snakebites occurred in the rainy season, 54.8% [95% CI: 53.0 – 56.6]. Eleven snakebite deaths were recorded with a case fatality rate of 0.4% (11/3,013).
Conclusions: Snakebite incidence over the five-year period was high. Males and young adults were the most affected. Central Gonja District recorded the highest incidence of snakebites. The majority of snakebites occurred in the rainy season. Health workers should sensitize community members on the dangers of snakebites across the region and continue to enhance prevention initiatives during both dry and rainy seasons.
Snakebite is a neglected public health issue that mostly affects poor rural farmers and children in tropical regions of Africa, Asia and Latin America [1–4]. An estimated 5.4 million snakebites occur annually worldwide, resulting in 81,410 to 137,880 deaths. Approximately 435,000 to 580,000 snakebite victims in Africa require medical attention each year [5–7]. Human-snake interactions are influenced by geographic and environmental factors as well as subsistence farming practices and housing architecture [8,9]. Studies have shown that the majority of snakebite victims are males, children and middle-aged persons, with cases occurring mostly in the rainy season [10–12]. Additionally, the highest proportion of snakebites occurs in rural areas where most people engage in agricultural activities such as farming, fishing and/or hunting [3,9].
A study in the Volta and Oti Regions of Ghana reported the five-year average of snakebite incidence to be 24 cases per 100,000 population [10]. The incidence of snakebite in the Bole District of the Savannah Region was also found to be 110 cases per 100,000 population. These victims and/or witnesses classified snakes using black, black and white, and green colours, with cobras and vipers identified as the common species [13]. Traditional medicine practitioners play essential roles in the management of snakebites in Ghana [14], providing treatment to 40% of snakebite victims in the Northern Region [12]. There have been variations in mortalities associated with snakebites in Ghana, with some studies reporting 2.8% and 0.7% case fatality rates [11,12].
Even though snakebites can result in disability and death, timely access to healthcare and anti-snake venom can reduce these effects [15]. Snakebite incidents in Sub-Saharan Africa (SSA) are underreported because the majority of snake bite victims dwell in rural areas and seek herbal/traditional treatment, whilst others die before reporting to health facilities [16–18]. The prevention and control of snakebites mostly depend on routine surveillance, awareness creation, improved housing designs and the use of protective clothing by farmers [8,19–21].
Despite the routine surveillance on snakebites by health facilities in the Savannah Region, there is an inadequate review of the data, leading to limited knowledge by healthcare workers, stakeholders and community members on its burden in the region. Analysing snakebite surveillance data will provide adequate information to the Savannah Regional Health Directorate on the morbidity and mortality of snakebites in the region and help in planning appropriate control and prevention strategies. Also, the findings may help the Neglected Tropical Disease Program Managers to formulate interventions to reduce the burden of snakebites across the country. Hence, this study determined the magnitude, distribution and potential geographical variation of snakebite in the Savannah Region.
Study Design
This was a cross-sectional study that utilized secondary data analysis of snakebite surveillance data in the Savannah Region from 2018 to 2022. The data was extracted from the District Health Information Management System 2 (DHIMS-2) database.
Study site
The study was carried out in the Savannah Region, one of the newly created regions in Ghana. It occupies an area of about 35,853 km2 in the northern part of the country. There are an estimated 680,991 inhabitants projected from the 2021 population and housing census [22]. There are seven administrative districts in the region with a total of 203 health facilities comprising hospitals, polyclinics, health centers, maternity homes, clinics and Community-based Health Planning and Services (CHPS) compounds. The majority of the population lives in rural communities. Farming is the major occupation in the region and some people living in riverine communities engage in fishing. The region has the Mole National Park, which serves as a habitat for wild animals, including various species of snakes. Carpet viper (Echis ocellatus), black-necked spitting cobra (Naja nigricollis), night adder (Causus rhombeatus) and elegant sand racer (Psammophis elegans) have been identified as the most common snake species biting humans in the Northern and Savannah Regions [12,13], with the prevalent venomous snakes in Ghana being snakes in the Viperidae family [23]. There are two climatic seasons in the region: namely rainy and dry seasons. The rainy season starts in May and ends in October, whilst the dry season is between November and April [24]. The region’s rainfall peaks in September with no significant annual trend. The estimated average rainfall ranges below 10mm to about 200mm in the dry and rainy seasons respectively. The rainy season is a regular climatic feature, occurring at alternating intervals with the dry season [25].
Data collection and processing
Snakebite morbidity and mortality data were extracted from the DHIMS2 for the period 2018-2022. DHIMS2 is a web-based database used by the Ghana Health Service to capture diseases and health events, including snakebite cases and deaths. New snakebite cases are documented at the Outpatient Departments (OPDs) of health facilities and entered into DHIMS 2 through the monthly OPD morbidity reporting form. In contrast, the severe cases are admitted and reported through the inpatient morbidity and mortality report form in the event database. The age groups of cases are pre-determined based on male and female by the database. The pivot table function under the data visualizer of DHIMS 2 was used to extract the snakebite cases whereas the deaths were retrieved using the cause of death component of the database. DHIMS 2 captures only aggregated data and does not include individual identifiers. The variables retrieved were age and sex of snakebite cases, deaths, district, month and year of the bite. The extracted data was exported to Microsoft Excel 2016 for cleaning and processing. Cleaning involved removing blank cells. The text-to-columns function of Microsoft Excel was used to generate age group and sex variables from the pre-categorized data.
Data analysis
Microsoft Excel 2016 was used to perform descriptive data analysis by person, place and time. Age and sex variables are presented in frequencies and proportions. The incidence of snakebites was determined by dividing the total number of reported snakebite cases per year by the mid-year projected population per 100,000 population. The average incidence was determined by dividing the five-year average of reported snakebites by the average mid-year population per 100,000 population. The cases by month for each year were categorized into rainy and dry seasons to determine the seasonality of snakebites. ArcGIS software 10.3 was used to illustrate the distribution of snakebite cases by district (place). ArcGIS was used to generate a choropleth map showing the incidence rate of snakebites per district. A choropleth map utilizes colour gradient to represent disparities in a qualitative variable across different geographical locations. We obtained the district shapefiles from the Ghana Demographic and Health Survey report, 2022 [26.] The district names and estimated snakebite incidences were linked to the shapefiles using the join tool in ArcGIS. The symbology tool of ArcGIS was further used in displaying the estimated district snakebite incidences using graduated colours. Results were presented in tables, graphs and geospatial maps.
Ethical clearance
The Ghana Health Service is mandated by the Public Health Act (Act 851), 2012, of the country to routinely report diseases and health events, including snakebite [30], into DHIMS 2 and analyse as part of Disease Surveillance and Response. In addition, de-identified aggregated snakebite data were used for the analysis. Therefore, no formal ethical clearance and informed consent was required. However, permission was obtained from the Savannah Regional Health Directorate for the extraction and use of the institutional data for this study. The data extracted was stored on a computer protected with a password and used specifically for the study. Only authorized personnel had access to the data. Additionally, we ensured that our analysis adhered to the ethical principles outlined in the World Medical Association Declaration of Helsinki and relevant data protection regulations.
Characteristics of snakebite cases
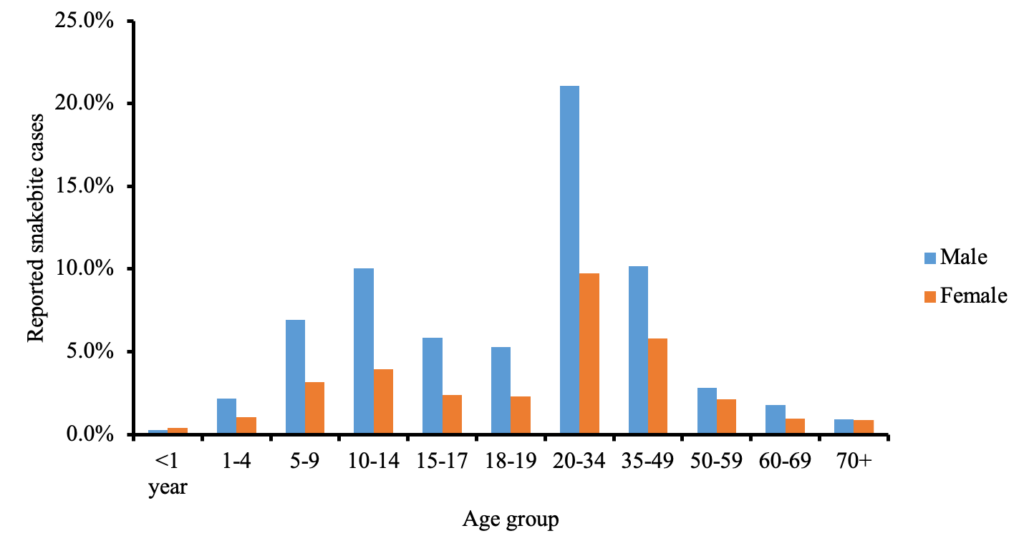
A total of 3,013 snakebite cases were recorded in the Savannah Region from 2018 to 2022. The majority of the cases were males, 67.3% (2,028/3,013). The highest proportion of snakebites occurred among persons aged 20-34 years, 30.8% (928/3,013), whilst children aged less than one year were the least affected, 0.7% (20/3,013). The majority of snakebites occurred in the rainy season, 54.8% (1,651/3,013) (Table 1). The distribution of snakebite cases was higher among males across the various age groups except for children less than one year old. Males among persons aged 20-34 years were more affected, 21.1% (635/3,013) and males less than one-year-old were the least affected by snakebites, 0.3% (8/3,013) (Figure 1).
Snakebite incidence
The regional average snakebite incidence was 101 [95% CI: 92.7 – 108.9] cases per 100,000 population. The highest incidence occurred in 2019 with 118 [95% CI: 108.6 – 127.4] cases per 100,000 population and the lowest in 2022, 84 [95% CI: 77.6 – 91.7] cases per 100,000 population. However, the incidence declined over the study period (Table 2).
Geographical distribution of snakebites
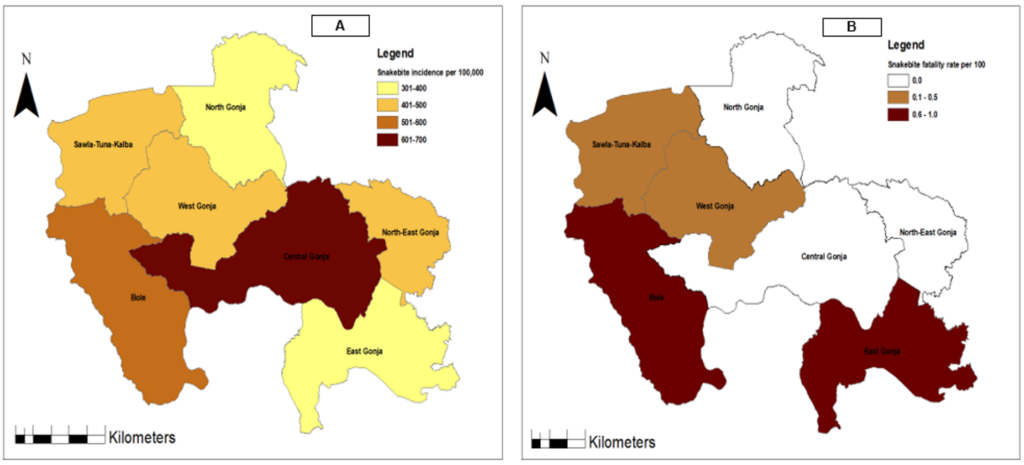
Snakebite cases occurred in all the seven districts of the Savannah Region, with district level cumulative incidence ranging from 312 to 626 per 100,000 population. Central Gonja District recorded the highest cumulative incidence, 626 cases per 100,000 population. The lowest incidence was reported in East Gonja District, 312 cases per 100,000 population (Figure 2A).
Snakebite mortality
A total of 11 snakebite deaths were reported in the Savannah Region over the five-year study period, with a case fatality rate of 0.4% (11/3,013). The years 2018 and 2019 recorded five and four snakebite deaths, respectively, whilst no snakebite-related mortality occurred in 2022. The highest case fatality rate, one per cent (3/312), was recorded in East Gonja District, with no death recorded in North, Central and North-East Gonja Districts (Figure 2B).
The five-year average of snakebite incidence was 101 per 100,000 persons. This is higher compared to results from studies in the Western, Volta and Oti Regions of Ghana which reported the incidence of snakebites between 24 and 82.8 cases per 100,000 respectively [10,11]. Studies in some Sub-Saharan African countries also showed lower snakebite incidence [27–29]. Our finding is similar to a study in the Bole District that reported an incidence of 110 per 100,000 population [13]. However, other studies in Nepal and Africa have reported varying high snakebite incidence between 262 and 650 cases per 100,000 populations [30,31]. The high incidence recorded in the region may be due to its rural setting where majority of the population are farmers and also the high prevalence of the activities of nomadic herdsmen. Furthermore, the vast unused land and Mole National Park are potential habitats for various species of snakes in the region which may be accountable for the high chances of snakebite cases in the region. This finding indicates that snakebite remains a pertinent public health issue in the Savannah Region which will require continuous sensitization of community members to mitigate the occurrence.
The study also showed that both males and females were affected with the majority of cases being males. This corroborates with other studies in Ghana which revealed similar findings where most snakebite victims are males [10–13,32]. Additionally, studies in India and Sudan had similar findings of snakebite being common among males [29,33]. However, some studies in Cameroun and Nepal showed that females were more affected by snakebites (61.6%-64%) because the major risk factor of snakebite was shown to be farming which is largely the occupation of women [27,31]. The economic activities such as farming, fishing and hunting engaged by men living in rural communities in the Savannah Region may be the possible reasons for the high proportion of snakebites among males. Thus, strategies and interventions designed to prevent snakebites should focus more on males.
All age groups were victims of snakebite in the region. However, persons between 20-34 years were the most affected. This is similar to other studies in Ghana which revealed that snakebite is common among young adults [10,11]. Persons in this age group are economically active and are engaged in farming, hunting, animal herding, wood logging and fishing. Additionally, other studies showed snakebite affects adult populations [12,31–33]. However, some studies showed that children and young adults were the majority of snakebite victims. These persons are mostly engaged in farming activities and animal herding in certain communities which expose them to accidental contact with snakes [13,29].
Snakebite cases were heterogeneously distributed across the region. This corroborates with other studies which showed that all districts in the Western, Oti and Volta Regions of Ghana recorded snakebite cases with spatial variations [10,11]. Additionally, studies in Sudan, Sri Lanka and Nepal revealed that all districts in the study regions recorded snakebites with widespread variation of hot and cold spots [17,29,31]. Central Gonja District recorded the highest snakebite incidence over the period. The district is occupied by large forest land with both the White and Black Volta rivers interlocking it. These provide favourable environmental conditions for farming activities, animal herding and fishing throughout the year which may have contributed to the high incidence of snakebite cases in the district. This corroborates with other studies which revealed that most snakebite victims are farmers with human-snake encounters occurring in forest areas and near waterbodies during agricultural activities such as farming and hunting [13,16,21,32].
The study revealed that most snakebites occurred during the rainy season (i.e., from May to October). This is similar to a surveillance data review in the Volta and Oti Regions of Ghana where the majority of snakebite cases were recorded in the rainy seasons between March to July and August to November [10]. Additionally, other studies in Ghana found the highest proportion of snakebite cases in the months of March, April, June, October and November [12,13,32]. This is corroborated by a study in northern Mozambique that showed the majority of snakebites occurred in the rainy season [16]. The higher snakebite cases in these months invariably coincide with key agricultural activities such as farmland preparations, harvesting of shea fruits, planting and harvesting in the region. The majority of inhabitants in the Savannah Region are subsistence farmers living in rural communities. Farming activities intensify during the rainy season, increasing human-snake interaction. This may explain why most snakebite cases are reported in the rainy season compared to the dry season. A study in Ghana showed a correlation between the high incidence of snakebite and the intensity of rainfall [12]. The study found that snakebite could result in mortality though the case fatality was low. A secondary data review of snakebites in the Western Region of Ghana reported a similar low-case fatality rate [11]. This low case fatality rate and the decline in the number of snakebite deaths may be due to bites by non-poisonous snakes. Also, the increasing availability of anti-snake venom at health facilities in rural areas, through improved drug supply management, may have contributed to the timely accessibility of these lifesaving medicines, thereby preventing snakebite-associated mortalities. However, a study using surveillance data in the Volta and Oti Regions and facility-based studies at the Tamale Teaching Hospital, Bole and Kintampo District Hospitals in Ghana revealed no mortality related to snakebites [10,13,32]. Early seeking of medical care and timely access to effective treatment may have been key to the survival of the snakebite victims [15]. Thus, this finding highlights the need to institute strategies to ensure that anti-snake venom and other essential medicines are readily available in primary hospitals and polyclinics across the Savannah Region. Also, Health Centers and lower health facilities should be provided with anti-snake venom to enable them to provide effective pre-referral emergency care to victims of snakebites.
Strengths and limitations
The study provides substantial information on snakebite burden in the Savannah Region, which will help health authorities and community stakeholders in planning preventive and control measures. However, the restricted data characteristics about snakebite cases in DHIMS 2, is a limitation of this study. The snake species, site of the bite, occupation of the cases reported and mode of clinical management were not recorded in the DHMIS-2. Also, tissue necrosis, organ damage, amputations and disability associated with snakebites are not reported in the DHIMS 2 database. Thus this study could not highlight most morbidity outcomes of snakebite. Furthermore, only individuals bitten by snakes who reported to health facilities were taken into account, hence, the results of this study may not accurately reflect the incidence of snakebites in the region. This suggests the possibility of an underestimation of snakebite incidence in our study, potentially due to under-reporting, since cases of snakebite seeking care from traditional healers are not captured in the DHIMS 2 database. Despite these limitations, the reported incidence of snakebite in this study is enormous and will be useful for local health authorities and community stakeholders.
The incidence of snakebite in the Savannah Region over the five year period was high. Snakebites were recorded among both males and females, with males being the more affected. All age groups were victims of snakebite and persons between the ages of 20-34 years were the most affected. All districts in the region recorded snakebite cases. The Central Gonja District recorded the highest incidence of snakebite cases. Snakebite cases were recorded all year round, with the majority occurring in the rainy season.
The Neglected Tropical Disease Program Focal Person in the Savannah Region should work with the Health Promotion Unit to organize health education and awareness campaigns on snakebites in health facilities and communities across the region, especially during the rainy season, to help reduce the morbidity of snakebites. Additionally, the population should be encouraged to wear wellington boots and other protective clothing whilst engaging in their activities on farmlands and herding of animals. The Regional Research Unit may conduct further studies to determine venomous snake species of medical importance and the factors that expose the population to snakebites. Community-based studies are imperative to estimate the true magnitude of snakebites in the Savannah Region. Furthermore, there is a need to review the DHIMS 2 database to collect snakebite-related information such as administration of anti-snake venom, type of snake, time of the bite and bite location. These variables are essential for public health planning and designing preventive interventions and strategies to help address the snakebite burden.
What is already known about the topic
What this study adds
| Variable | Frequency, N = 3,013 | Percent [95% CI] |
|---|---|---|
| Sex | ||
| Male | 2,028 | 67.3 [65.5 – 69.0] |
| Female | 985 | 32.7 [31.0 – 34.4] |
| Age group | ||
| <1 year | 20 | 0.7 [0.4 – 1.0] |
| 1–4 | 96 | 3.2 [2.6 – 3.9] |
| 5–9 | 304 | 10.1 [9.0 – 11.2] |
| 10–14 | 421 | 14.0 [12.8 – 15.3] |
| 15–17 | 248 | 8.2 [7.3 – 9.3] |
| 18–19 | 228 | 7.6 [6.6 – 8.6] |
| 20–34 | 928 | 30.8 [29.2 – 32.5] |
| 35–49 | 482 | 16.0 [14.7 – 17.4] |
| 50–59 | 149 | 4.9 [4.2 – 5.8] |
| 60–69 | 83 | 2.8 [2.2 – 3.4] |
| 70+ | 54 | 1.8 [1.3 – 2.3] |
| Season | ||
| Dry season | 1,362 | 45.2 [43.4 – 47.0] |
| Rainy season | 1,651 | 54.8 [53.0 – 56.6] |
| Year | Mid-year population | Number of cases N = 3,013 | Incidence per 100,000 [95% CI] |
|---|---|---|---|
| 2018 | 526,364 | 531 | 101 [92.5 – 109.8] |
| 2019 | 525,803 | 619 | 118 [108.6 – 127.4] |
| 2020 | 625,299 | 624 | 100 [92.1 – 107.9] |
| 2021 | 653,266 | 676 | 103 [95.8 – 111.6] |
| 2022 | 666,985 | 563 | 84 [77.6 – 91.7] |
| Average | 599,543.4 | 602.6 | 101 [92.7 – 108.9] |
Views: 4,917
Menu, Tables and Figures
| Variable | Frequency, N = 3,013 | Percent [95% CI] |
|---|---|---|
| Sex | ||
| Male | 2,028 | 67.3 [65.5 – 69.0] |
| Female | 985 | 32.7 [31.0 – 34.4] |
| Age group | ||
| <1 year | 20 | 0.7 [0.4 – 1.0] |
| 1–4 | 96 | 3.2 [2.6 – 3.9] |
| 5–9 | 304 | 10.1 [9.0 – 11.2] |
| 10–14 | 421 | 14.0 [12.8 – 15.3] |
| 15–17 | 248 | 8.2 [7.3 – 9.3] |
| 18–19 | 228 | 7.6 [6.6 – 8.6] |
| 20–34 | 928 | 30.8 [29.2 – 32.5] |
| 35–49 | 482 | 16.0 [14.7 – 17.4] |
| 50–59 | 149 | 4.9 [4.2 – 5.8] |
| 60–69 | 83 | 2.8 [2.2 – 3.4] |
| 70+ | 54 | 1.8 [1.3 – 2.3] |
| Season | ||
| Dry season | 1,362 | 45.2 [43.4 – 47.0] |
| Rainy season | 1,651 | 54.8 [53.0 – 56.6] |
Table 1: Characteristics of snakebite cases, Savannah Region, Ghana, 2018–2022
| Year | Mid-year population | Number of cases N = 3,013 | Incidence per 100,000 [95% CI] |
|---|---|---|---|
| 2018 | 526,364 | 531 | 101 [92.5 – 109.8] |
| 2019 | 525,803 | 619 | 118 [108.6 – 127.4] |
| 2020 | 625,299 | 624 | 100 [92.1 – 107.9] |
| 2021 | 653,266 | 676 | 103 [95.8 – 111.6] |
| 2022 | 666,985 | 563 | 84 [77.6 – 91.7] |
| Average | 599,543.4 | 602.6 | 101 [92.7 – 108.9] |
Table 2: Snakebite incidence, Savannah Region, Ghana 2018–2022