Research | Open Access | Volume 8 (3): Article 51 | Published: 11 Jul 2025
Views: 2,329
Menu, Tables and Figures
| Variable | Frequency | Percentage (%) |
|---|---|---|
| Age of Students | ||
| 16–25 | 297 | 80.9 |
| 26–35 | 66 | 17.9 |
| 36 above | 4 | 1.1 |
| Gender | ||
| Male | 131 | 35.6 |
| Female | 236 | 64.3 |
| Level of Study | ||
| 2nd year | 46 | 12.5 |
| 3rd year | 134 | 36.5 |
| 4th year | 187 | 50.9 |
| Parents’ Occupation | ||
| Business | 151 | 41.1 |
| Civil servants | 93 | 25.3 |
| Farmers | 60 | 16.3 |
| Professionals (Lawyers, Doctors, Lecturers etc) | 31 | 8.4 |
| Petty traders | 32 | 8.7 |
Table 1: Socio-demographic Characteristics of the Respondents (N=367)
| Variable | Wald | Df | P-Value | Adjusted Odd Ratio | 95% Confidence Interval |
|---|---|---|---|---|---|
| Lack of Parental influence or motivation | 4.167 | 1 | 0.041 | 0.778 | 0.612 – 0.990 |
| Social media | 0.000 | 1 | 0.992 | 1.003 | 0.765 – 1.413 |
| Peer group influence | 0.028 | 1 | 0.731 | 1.035 | 0.832 – 1.264 |
| Financial hardship | 5.404 | 1 | 0.020 | 0.727 | 0.556 – 0.951 |
| Self-Satisfaction | 0.004 | 1 | 0.848 | 1.099 | 0.834 – 1.338 |
Table 2: Multivariate Analysis of Factors Promoting Risky Sexual Behaviours of Respondents (N=367)
| Variable | Frequency | Percentage (%) |
|---|---|---|
| I perceive the risk of contracting sexually transmitted infections (STIs) as high when engaging in risky sexual behavior | ||
| Strongly Agree | 182 | 59.2 |
| Agree | 82 | 26.7 |
| I Don’t Know | 60 | 16.3 |
| Strongly Disagree | 27 | 8.8 |
| Disagree | 16 | 5.2 |
| I believe that engaging in risky sexual behavior significantly increases the likelihood of unintended pregnancy | ||
| Strongly Agree | 155 | 50.4 |
| Agree | 108 | 35.2 |
| Neither | 60 | 16.3 |
| I Don’t Know | 32 | 10.4 |
| Strongly Disagree | 12 | 3.9 |
| My experiences with risky sexual behavior have led me to adopt safer sexual practice | ||
| Strongly Agree | 84 | 27.3 |
| Agree | 48 | 15.6 |
| I Don’t Know | 60 | 16.3 |
| Strongly Disagree | 97 | 31.6 |
| Disagree | 78 | 25.4 |
| I think social norms and peer pressure have influenced my past engagement in risky sexual behavior | ||
| Strongly Agree | 102 | 33.2 |
| Agree | 52 | 16.9 |
| I Don’t Know | 60 | 16.3 |
| Strongly Disagree | 111 | 36.1 |
| Disagree | 42 | 13.7 |
| I perceive that the long-term consequences of risky sexual behavior can be severe | ||
| Strongly Agree | 179 | 58.3 |
| Agree | 97 | 31.6 |
| I Don’t Know | 60 | 16.3 |
| Strongly Disagree | 21 | 6.8 |
| Disagree | 10 | 3.2 |
Table 3: Perceived Health Effects of Risky Sexual Behavior on Respondents (N=367)
Browne Okonkwo1, Richard Akinola Aduloju2, Christabel Nneka Ogbolu3,&, Justice Iyawa3, Otovwe Agofure4, Loveth Onuwa Okololise3
1School of Medicine and Surgery, Novena University, Ogume, Delta State, Nigeria, 2School of Dentistry, Novena University, Ogume, Delta State, Nigeria, 3Department of Public and Community Health, College of Medical and Health Sciences, Novena University, Ogume, Delta State, Nigeria, 4Department of Public Health, Faculty of Health Sciences, Achievers University, Owo, Ondo State, Nigeria
&Corresponding author: Christabel Nneka Ogbolu, Department of Public and Community Health, College of Medical and Health Sciences, Novena University, Ogume, Delta State, Nigeria, Email: christabelnnekaogbolu@gmail.com
Received: 10 Dec 2024, Accepted: 09 Jul 2025, Published: 11 Jul 2025
Domain: Adolescent Health, Sexual and Reproductive Health
Keywords: Risky Sexual Behavior, Behavior Patterns, Health Outcomes, Sexual Health, Youth Health, Perceived Effect, Tertiary Institution, Sexual Risk Factors, Public Health, Predictors
©Browne Okonkwo et al Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Browne Okonkwo et al Risky sexual behaviours: Predictors and perceived effect on the health of undergraduate students in a tertiary institution in Delta State, Nigeria. Journal of Interventional Epidemiology and Public Health. 2025;8:51. https://doi.org/10.37432/jieph-d-24-02026
Background: There are serious public health concerns associated with risky sexual conduct among undergraduate students, such as the spread of sexually transmitted diseases (STDs) and unwanted pregnancies. The prevalence of these practices, perceived health hazards, and contributing variables are investigated in this research of students at a tertiary institution in Delta State, Nigeria.
Methods: 367 undergraduate students participated in a cross-sectional survey. A structured questionnaire was used to gather data on sociodemographic traits, hazardous sexual activity categories, perceived health risks, and contributing variables. To find important determinants of hazardous sexual activity, the research used descriptive statistics and multivariate logistic regression.
Results: Most of the respondents (80.9%) were aged 16-25 years, with an average age of 22.3 years (standard deviation of 2.74). Females represented 64.3% of the sample. Prevalence of Risky Behaviors: Hook-ups/multiple sexual partners (67.6%), abortion (56.1%), phone sex (49.6%), oral sex (59.1%), use of strong drugs for sex (48.0%), and masturbation (46.0%) were the most common risky behaviors. Perceived Risks: Most respondents recognized the high risks of contracting sexually transmitted infections, unplanned pregnancy and perceived severe long-term consequences from hazardous sexual conduct. Influencing Elements: lack of parental influence or motivation (aOR=0.778, 95% CI=0.612-0.990), and financial hardship (aOR=0.727, 95% CI=0.556-0.951) significantly predicted their behavior.
Conclusion: A high prevalence of risky sexual behaviors among undergraduate students was revealed in this study, calling for better access to comprehensive sexual health education and reproductive health care. Financial hardship and a lack of parental influence were important protective factors, but require further investigations to understand their actual role and to guide targeted interventions to promote safer sexual practices among students and reduce associated health consequences.
A heterogeneous population of people with a range of sexual orientations and behaviors makes up undergraduate students. Most college students engage in sexual activity, according to a study [1], and the average age of sexual initiation is between 17 and 19 years old. Generalizing sexual conduct of undergraduate students might not be appropriate as each individual is unique and may have different experiences and preferences however, we can infer using a general sample. Hookup culture is prevalent on college campuses, with many students engaging in casual sexual encounters [2]. Hookups are typically defined as sexual encounters without the anticipation of a dedicated partnership, and they can range from kissing to sexual intercourse. Research has indicated that hookup culture is more common among university attendees than among other age groups, although not all students participate in hookups [3-5].
Throughout the previous few decades, it has been observed that there has been a substantial increase in the percentage of undergraduate students who report sexual activity while at school [6], with Kenku et al, hypothetically stating that hazardous sexual behavior is greatly influenced by religion among Northern Nigerian undergraduate students [7]. Tekletsadik et al. [8] reported risky sexual behaviors to include sexual activity without condom usage, substance and alcohol use. There are consequences connected with this behavior that places the students at risk. Among these include the rise in HIV and other sexually transmitted diseases (STDs), gynecological issues, a significant gap in the risk of unintended pregnancies and non-marital pregnancies, and an increase in the prevalence of abandoned babies [6,9].
In Nigeria, problems associated with adolescent sexual behaviors include a high rate of teenage pregnancy, increased rates of sexual offenses, child abandonment, school dropout, increased prevalence of STDs, and the acquisition of venereal illnesses [10,11]. Hence the study’s goal was to discuss the frequency of risky sexual behavior and its effects on undergraduate students’ health, which is essential for improving campus health services, developing supportive campus environments, influencing policy formation, and increasing student well-being and academic performance.
Study Setting and Design
The study employed a descriptive cross-sectional study design that explored the risky sexual behaviour of university students in Novena University, Ogume in addition to the health consequences of these behaviours on them. The institution is the first private university in Delta State located in Amai, Ukwuani Local Government Area. As at the time of the study the university had four colleges and 19 departments, with a total student population of 3435.
Study Population
Both male and female undergraduate students in their second through fifth years at the university comprised the study’s population.
Sample size and Sample Technique
The Taro Yamane algorithm [12] was utilised to determine the size of the sample.
$$
n = \frac{N}{1 + N(e)^2}
$$
Three key elements were used in the formula:
N: The total number of students enrolled in the most recent academic session, which was 3,435 pupils.
e: The acceptable amount of inaccuracy in the estimate, expressed as the intended margin of error or degree of precision, which is set at 5% (0.05).
n: The estimated sample size
Following the computation of n, a 10% predicted non-response rate was taken into consideration. About 398 people made up the final estimated sample size. A multi-stage sampling approach was used to select respondents across the 19 department within the institution.
$$ \frac{\text{Total Population in a Department} \times \text{No. of Questionnaires to be Distributed in the College}}{\text{Total Population in the 2 Selected Departments}} $$
Distribution: CMHS: 164 (Nursing: 136; PCH: 28), CMSS: 129 (ISS: 53; Political Science: 76), CNAS: 103 (EPS: 78; Biological Sciences: 25) and CL: 3 (Law: 3)
Respondents were distributed evenly among four student academic years within each department. Using a random number generator, eligible students were chosen at random from departmental registers. After lectures, recruitment took place in person, and informed consent was acquired.
398 questionnaires were distributed and 367 were obtained, yielding a 92% response rate.
Method and Instrument of Data Collection
A questionnaire was the primary instrument used to collect data from the respondents. Respondents were given the questionnaire under careful observation and direction. The questionnaire was broken down into three sections: a part on sociodemographic characteristics that asked about age, gender, parents’ employment and level of education, and a piece on students’ study level. Additional parts included details on the prevalent hazardous sexual activity among students as well as the perceived health consequences of these activities.
Study Variables
Dependent: Engagement in Risky Sexual Behaviour
Independent: Socio-demographics, lack of parental Influence, financial hardship, social media, peer influence, self-satisfaction.
Data Management
Structured paper-based questionnaires were used to gather data. Statistical Product and Service Solution version 22.0 (IBM Corp SPSS, Armonk, NY, USA) was used to manually input the responses. To guarantee correctness, data were thoroughly examined and validated during entry. Prior to statistical analysis, which included descriptive statistics and logistic regression, the dataset was cleaned in SPSS by looking for duplicates, missing values, and inconsistent replies. Both descriptive statistics (frequencies & percentages) and tabular presentations were used to describe the variables. Only variables significant in the bivariate analysis were included in the logistic regression to identify independent predictors of risky sexual behaviors.
Ethical approval
The Helsinki Declaration was followed in the conduct of the research. After receiving a thorough explanation of the study, participants gave their informed consent. The Ministry of Health in Delta State provided ethical authorisation as well, with reference number HM/596/T2/85.
Socio-demographic characteristics of respondents
A total of 367 respondents were recruited. Most respondents 297 (80.9%) fell within the 16–25 age range, 66 (17.9%) within 26-35 and 4 (1.1%) within the 36 and above age range. The respondents were 22.3 years old on average, with a standard deviation of 3.74. Majority were females 236 (64.3%) and in their fourth year of university study187 (50.9%). In addition, most of the respondents’ parents 151(41.1%) were businesspeople, followed by civil servants 93 (25.3%) and the least were petty traders 31(8.4%).
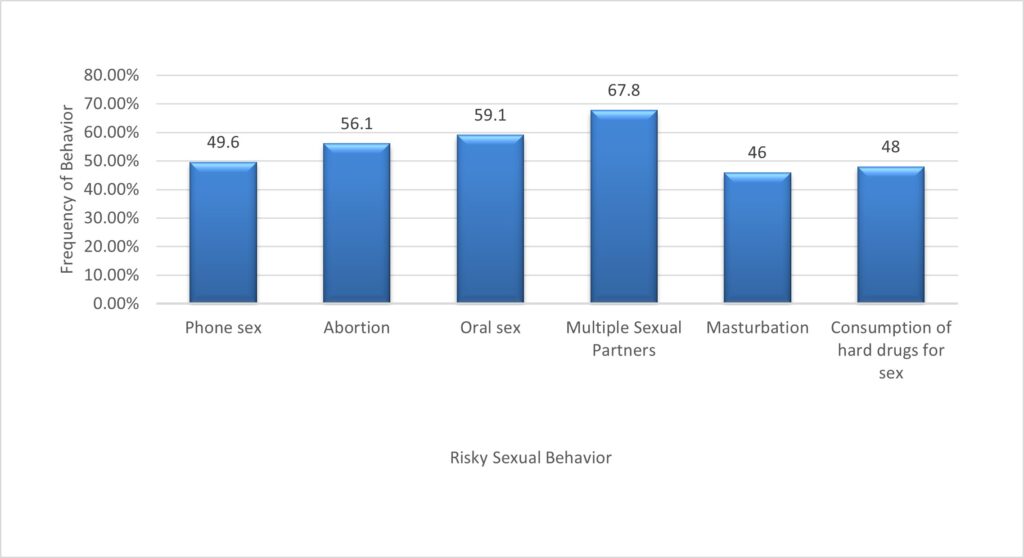
Respondents’ Dangerous Sexual Practices
Out of 367 respondents, at least 248 students (67.6%) reported engaging in one or more forms of risky sexual behavior, with the most common being having multiple sexual partners (248, 67.6%). Abortion was also widely reported, with 206 students (56.1%) indicating they had either experienced or been involved in one. Other notable behaviors included viewing pornography (228, 62.1%), oral sex (217, 59.1%), phone sex (182, 49.6%), use of strong drugs for sex (176, 48.0%), and masturbation (169, 46.0%). Additionally, 169 students (46.0%) reported inconsistent or no condom use during sexual activity. These findings reflect a high prevalence of risky sexual practices among undergraduates, highlighting the need for targeted interventions. (Figure 1).
Factors Promoting Risky Sexual Behaviour of Respondents
To investigate the relationship between a few independent factors and hazardous sexual activity, bivariate analysis was used. Financial difficulty and a lack of parental influence or motivation were two variables that showed strong connections. The multivariate logistic regression model was then fitted with these important factors from the bivariate analysis.
Multivariate analysis revealed that both lack of parental influence or motivation (Adjusted Odds Ratio [AOR] = 0.778, 95% Confidence Interval [CI] = 0.612–0.990) and financial hardship (AOR = 0.727, 95% CI = 0.556–0.951) were statistically significant predictors of risky sexual behavior. However, the odds ratios were less than 1 suggesting that these factors, while significant, were associated with reduced likelihood of engaging in risky sexual behavior when adjusted for other variables in the model. (Table 2).
Respondents’ Perceived Health Effects of Dangerous Sexual Behaviour
The majority of respondents, 264/367 (85.9%), believe that there is a high risk of STDs when participating in unsafe sexual conduct. The vast majority of 263/367 people (85.6%), think that having unsafe sexual relations greatly raises the possibility of becoming pregnant unintentionally. 132/367 people (42.9%) who had previously engaged in hazardous activity have switched to safer sexual practices. 50.1% (154/367) of the participants admitted that peer pressure and societal norms had an impact on their decision to participate in hazardous sexual conduct. The majority, 276/367 (89.9%), believe that hazardous sexual conduct has serious long-term effects (Table 3).
The majority of respondents were young individuals aged 16–25, with females outnumbering males. This aligns with findings by Jahanfar et al. and Perera et al., who reported similar gender distributions, but contrasts with Osuala et al. and Chi et al., who observed a male majority [13, 14, 15, 16]. Across various studies, cohort medians indicate that 38% to 63% of HIV infections in women occur among those aged 15-24 years, while 30% to 63% of infections in men are found in the 20-29 age group [17]. Given these trends, it is not surprising that UNAIDS reported the highest rates of newly acquired HIV infections among individuals aged 15-25 years, who account for 60% of the global HIV-positive population [17,18]. It may be necessary to modify programs designed to discourage hazardous sexual activity differently for men and women [19–21]. Most respondents’ parents were engaged in business or civil service roles—occupations associated with better access to education and health resources. This socioeconomic background may shape attitudes toward public health and academic performance. Public health activities can also be influenced by the employment of the parents; families in the civil service tend to be more stable and supportive [22, 23]. The relatively narrow age range and consistent background allow for targeted, age-specific public health and educational interventions.
According to multivariate analysis, respondents’ hazardous sexual conduct was statistically significantly predicted by financial difficulty (AOR = 0.727, 95% CI = 0.556–0.951) and a lack of parental influence or drive (AOR = 0.778, 95% CI = 0.612–0.990). Nonetheless, the fact that the odds ratios were less than one suggests that these characteristics may have had a protective impact in our study since they were linked to a decreased chance of participating in hazardous sexual conduct. Existing literature have highlighted the role of parental monitoring and communication in adolescent sexual decision-making. For example, Wang et al. and Ross-Gray reported that improved parent-child communication and supervision correlate with reduced adolescent risk behaviors [24, 25]. Similarly, Grey et al. emphasized that warmth and openness in parenting foster positive youth outcomes, while Ryan et al. demonstrated that monitoring delayed risky behaviors, including early sexual initiation [26, 27]. However, Okigbo et al. noted gender differences in the influence of paternal communication, suggesting that maternal involvement may be more impactful in shaping adolescents’ sexual behaviors [28]. These studies collectively affirm that enhancing parental engagement—especially through open, supportive communication—can serve as a key strategy for mitigating youth involvement in high-risk sexual activities. In addition, Reed et al. reported that females without financial support engaged in inconsistent condom use, while Duncan et al. found that individuals facing high financial hardship were more likely to engage in condomless anal sex and transactional sex [29, 30]. Similarly, Freedman et al. noted that many young women engaged in transactional sex out of necessity—to pay for food, healthcare, housing, or education. Morris and Rushwan added that economic pressures often restrict access to reproductive health services, increasing susceptibility to coercion and reducing the ability to practice safe sex [31,32]. Collectively, these studies affirm that financial stability is a crucial determinant of young people’s ability to make safe and informed sexual decisions.
According to the research, the majority of respondents are aware of the significant long-term implications and the high risks involved in participating in hazardous sexual conduct, such as getting an STD or becoming pregnant unintentionally. However, not all hazardous behavior experiences result in the adoption of safer habits; over 50% of respondents saw peer pressure and social norms as major impacts. This finding contrasts with the findings of Desmenu et al, and Balán et al. which indicated that despite engaging in risky behaviors, the majority of respondents had low perceptions of risk of contracting STIs [33, 34]. People who do not perceive risk may take fewer precautions, which can increase the spread of STIs [35,36]. Targeted sexual health education aims to dispel misconceptions and increase knowledge of risks [37]. Behavior changes interventions, which make use of visual aids, statistical data, and personal testimonials, can raise risk perception and promote safer behaviors.
The present study revealed that a significant proportion of respondents engaged in various high-risk sexual behaviors. Among these, having multiple sexual partners was the most commonly reported behavior, followed by oral sex, abortion, phone sex, the use of substances to enhance sexual activity, and masturbation. These findings align with previous research indicating high rates of multiple sexual partnerships among university students in Nigeria, which increases vulnerability to sexually transmitted diseases and intimate partner violence [38, 39, 40, 41]. However, the present findings slightly contrast with studies carried out in Northen Nigeria which may be related to regional differences [42,43].Abortion was notably the most commonly reported behavior in this study, with more than half (56.1%) of respondents indicating they had undergone an abortion. This percentage, which is higher than those found in other studies within the same country [44, 45], highlights increasing concerns about reproductive health risks among female students, particularly in areas with limited access to safe reproductive services. The high rate of abortion also points to deeper emotional and psychological consequences. Consistent with previous studies, abortion has been associated with increased risk of depression, anxiety, and reduced academic performance, particularly among female medical students in the same region [41, 46]. Such outcomes may contribute to long-term psychological distress, including trauma, guilt, and diminished self-confidence, which can negatively affect interpersonal relationships and academic success.
Additionally, substance use for sexual performance enhancement was reported among the respondents, a behavior strongly linked in literature to psychological dependence, depression and long-term health risks [47,48]. Drug and alcohol use among students has been shown to impair academic performance and increase the likelihood of risky sexual decisions, unplanned pregnancies, and sexually transmitted infections [49, 50]. This pattern is further supported by [51], who found that alcohol consumption heightens the probability of unsafe sexual encounters.
Collectively, these findings suggest that high-risk sexual behaviors among university students are shaped by complex socio-emotional and economic factors. Interventions should not only target sexual health education but also address mental health support, access to contraception, and substance abuse prevention.
This study emphasizes how common hazardous sexual activities, such as masturbation, numerous sexual partners, phone sex, oral sex, hook-ups, and abortions, are among college students. Despite a general awareness of the associated health risks such as sexually transmitted diseases and unintended pregnancies, engagement in these behaviors remains high. This calls for better access to comprehensive sexual health education and reproductive health care. Lack of parental influence and financial difficulty were found to be important protective factors and require further investigation. These results highlight the pressing need for multi-level, focused interventions. To encourage safer sexual behaviors and protect the wellbeing of young people, academic institutions, parents, and legislators must work together to address behavioral patterns and the socioeconomic factors that underlie them.
What is already known about the topic
What this study adds
Conception and Study Design: Browne Okonkwo and Richard Akinola Aduloju. Data Collection, Entry and Clearing: Christabel Nneka Ogbolu. Data Analysis and Interpretation: Otovwe Agofure. Manuscript Drafting: Christabel Nneka Ogbolu. Manuscript Revision: Loveth Onuwa Okololise and Justice Iyawa. Christabel Nneka Ogbolu is accountable for the study’s general credibility. Before submitting the work, all writers gave their approval to its final draft.
| Variable | Frequency | Percentage (%) |
|---|---|---|
| Age of Students | ||
| 16–25 | 297 | 80.9 |
| 26–35 | 66 | 17.9 |
| 36 above | 4 | 1.1 |
| Gender | ||
| Male | 131 | 35.6 |
| Female | 236 | 64.3 |
| Level of Study | ||
| 2nd year | 46 | 12.5 |
| 3rd year | 134 | 36.5 |
| 4th year | 187 | 50.9 |
| Parents’ Occupation | ||
| Business | 151 | 41.1 |
| Civil servants | 93 | 25.3 |
| Farmers | 60 | 16.3 |
| Professionals (Lawyers, Doctors, Lecturers etc) | 31 | 8.4 |
| Petty traders | 32 | 8.7 |
| Variable | Wald | Df | P-Value | Adjusted Odd Ratio | 95% Confidence Interval |
|---|---|---|---|---|---|
| Lack of Parental influence or motivation | 4.167 | 1 | 0.041 | 0.778 | 0.612 – 0.990 |
| Social media | 0.000 | 1 | 0.992 | 1.003 | 0.765 – 1.413 |
| Peer group influence | 0.028 | 1 | 0.731 | 1.035 | 0.832 – 1.264 |
| Financial hardship | 5.404 | 1 | 0.020 | 0.727 | 0.556 – 0.951 |
| Self-Satisfaction | 0.004 | 1 | 0.848 | 1.099 | 0.834 – 1.338 |
| Variable | Frequency | Percentage (%) |
|---|---|---|
| I perceive the risk of contracting sexually transmitted infections (STIs) as high when engaging in risky sexual behavior | ||
| Strongly Agree | 182 | 59.2 |
| Agree | 82 | 26.7 |
| I Don’t Know | 60 | 16.3 |
| Strongly Disagree | 27 | 8.8 |
| Disagree | 16 | 5.2 |
| I believe that engaging in risky sexual behavior significantly increases the likelihood of unintended pregnancy | ||
| Strongly Agree | 155 | 50.4 |
| Agree | 108 | 35.2 |
| Neither | 60 | 16.3 |
| I Don’t Know | 32 | 10.4 |
| Strongly Disagree | 12 | 3.9 |
| My experiences with risky sexual behavior have led me to adopt safer sexual practice | ||
| Strongly Agree | 84 | 27.3 |
| Agree | 48 | 15.6 |
| I Don’t Know | 60 | 16.3 |
| Strongly Disagree | 97 | 31.6 |
| Disagree | 78 | 25.4 |
| I think social norms and peer pressure have influenced my past engagement in risky sexual behavior | ||
| Strongly Agree | 102 | 33.2 |
| Agree | 52 | 16.9 |
| I Don’t Know | 60 | 16.3 |
| Strongly Disagree | 111 | 36.1 |
| Disagree | 42 | 13.7 |
| I perceive that the long-term consequences of risky sexual behavior can be severe | ||
| Strongly Agree | 179 | 58.3 |
| Agree | 97 | 31.6 |
| I Don’t Know | 60 | 16.3 |
| Strongly Disagree | 21 | 6.8 |
| Disagree | 10 | 3.2 |