Research | Open Access | Volume 9 (2): Article 95 | Published: 08 Jun 2026

Views: 554
Menu, Tables and Figures
Table 1: Demographic characteristics and knowledge of healthcare workers on the measles case-based surveillance system in Insiza District, Zimbabwe, 2023
| Characteristic | Frequency N= 40 (%) |
|---|---|
| Designation | |
| Medical Doctor | 1 (2.5) |
| General Nurse | 13 (32.5) |
| Primary Care Nurse | 10 (25) |
| Midwife | 1 (2.5) |
| Environmental Health Officer | 8 (20) |
| Health Information Officer | 1 (2.5) |
| Village Health Worker | 6 (15) |
| Sex | |
| Male | 10 (25%) |
| Female | 30 (75%) |
| Median age | 37.5 Years (Q1=28.5; Q3=47.0) |
| Median years in service | 11.5 Years (Q1=5.5; Q3=17.5) |
| Participants who knew | |
| Measles case definition | 38 (95) |
| Time limit to investigate suspected measles case | 20 (50) |
| Number of investigation form copies to be filled | 28 (70) |
| Phase in which Zimbabwe is on measles surveillance | 36 (90) |
| Type of sample collected for investigation | 34 (85) |
| Participant knowledge assessment | |
| Good | 11 (27.5) |
| Fair | 21 (52.5) |
| Poor | 8 (20) |
Table 1: Demographic characteristics and knowledge of healthcare workers on the measles case-based surveillance system in Insiza District, Zimbabwe, 2023
Table 2: Usefulness and attributes of the measles case-based surveillance system in Insiza District, Zimbabwe, 2023
| Variable | Frequency n= 40 Percentage (%) |
|---|---|
| Usefulness | |
| Perceived the system to be useful | 37 (92.5) |
| Conduct surveillance meetings | 36 (90%) |
| Planning for resource requirement and distribution | 22 (55%) |
| Policy making | 0 |
| Plan for training of healthcare workers | 3 (7.5%) |
| Awareness and Vaccination campaigns | 11 (27.5%) |
| Conduct research | 1 (2.5%) |
| Detect Outbreaks | 25 (62.5%) |
| Stability | |
| Received training in EPI surveillance including measles | 8 (20%) |
| Knew measles case definition available | 34 (80%) |
| Case definition displayed | 10/10 |
| Measles case investigation forms available | 34 (80%) |
| EPI Guidelines available | 34 (80%) |
| Cell phone or landline available | 10/10 |
| Transport available | 10/10 |
| Specimen collection tubes available | 10/10 |
| Simplicity | |
| Ever completed a measles investigation form | 24 (30%) |
| Reported time to complete in minutes | |
| Less than 10 | 6 (25%) |
| Between 10-20 | 12 (50%) |
| More than 20 | 6 (25%) |
| Data Quality | |
| Any difficulties in completing the form (No) | 24 (100%) |
| Forms correctly filled in all sections | 0/10 |
| Areas incompletely filled in | |
| Case identification | 5/10 |
| History of vaccination | 8/10 |
| Blood specimen information | 2/10 |
| Final classification | 10/10 |
Table 2: Usefulness and attributes of the measles case-based surveillance system in Insiza District, Zimbabwe, 2023
Table 3: Timeliness of measles case-based surveillance system in Insiza District, Zimbabwe, 2023
| Timeliness | ||||||
|---|---|---|---|---|---|---|
| Year | Suspected cases detected | Reported within 7 days of rash onset | Investigated within 48 hours | Reaching the lab within 3 days | Results received within 7 days | |
| 2020 | 2 | 1 | 1 | 0 | 0 | |
| 2021 | 3 | 3 | 2 | 0 | 0 | |
| 2022 | 10 | 7 | 6 | 0 | 0 | |
| 2023 | 9 | 7 | 3 | 1 | 0 | |
| Sensitivity | ||||||
| Year | Total population target | Cases Expected | Cases detected | Cases investigated | Results confirmed | Calculate sensitivity |
| 2020 | 132323 | 3 | 0 | 0 | 0 | 0 |
| 2021 | 133794 | 3 | 0 | 0 | 0 | 0 |
| 2022 | 135282 | 3 | 10 | 10 | 0 | 0 |
| 2023 | 136191 | 3 | 9 | 7 | 1 | 14.3% |
Table 3: Timeliness of measles case-based surveillance system in Insiza District, Zimbabwe, 2023
Hwacha Kudzai1, Muza Andrew2, Chadambuka Addmore3,4, Juru Tsitsi4, Gombe Notion3, Mandozana Gibson1, Shambira Gerald1, Tshimanga Mufuta1
1University of Zimbabwe, Department of Global Public Health and Family Medicine, Harare, Zimbabwe, 2Provincial Medical Directorate Matabeleland South, Bulawayo, Zimbabwe, 3African Field Epidemiology Network, Harare, Zimbabwe, 4Zimbabwe Field Epidemiology Training Program, Harare, Zimbabwe
&Corresponding author: Addmore Chadambuka, Zimbabwe Field Epidemiology Training Program, Harare, Zimbabwe, Email: achadambuka1@yahoo.co.uk ORCID: https://orcid.org/0000-0003-2407-1172
Received: 11 Dec 2024, Accepted: 04 Jun 2026, Published: 08 Jun 2026
Domain: Infectious Disease Epidemiology
Keywords: measles, case-based surveillance, knowledge
©Hwacha Kudzai et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Hwacha Kudzai et al. Evaluation of the measles case-based surveillance system in Insiza District, Zimbabwe, 2023. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):95. https://doi.org/10.37432/jieph-d-24-02031
Introduction: The WHO recommends case-based surveillance with laboratory investigation for every measles-suspected case. Insiza District failed to investigate all the suspected measles cases in 2022. Failure to detect and investigate measles cases contributes to the spread of the disease. This can result in death or other sequelae requiring admission, or a cost to the state and family. The district detected an outbreak of measles 14 days after 10 community deaths had occurred. We evaluated the measles case-based surveillance system in Insiza District to determine reasons for failure to investigate all cases, knowledge of the surveillance system, and system attributes.
Methods: A descriptive cross-sectional study using the updated CDC guidelines for surveillance system evaluation was conducted. Structured pretested interviewer-administered questionnaires were used to collect data on reasons for failure to investigate all cases, knowledge of the surveillance system, and system attributes. A key informant interview guide was used to assess reasons for not investigating all cases. Epi Info 7 was used to generate frequencies and proportions.
Results: Most participants were nurses, 26 (65%). The median years in service was 11.5 years (IQR:6-16). The majority, 21 (52.5%), had fair knowledge of the surveillance system. Eight (20%) of participants had ever received training on measles surveillance, and the system was simple, as 18 (75%) required less than 20 minutes to complete a measles case investigation form. Most facilities (8/10) had adequate resources, making the system stable. The system was acceptable as all participants expressed willingness to participate. The system was not sensitive, as only ten out of 24 cases identified as meeting the case definition on records review were investigated in 2023. The major reasons for failure to investigate all cases were a lack of training and poor health worker knowledge of the system. A poor-performing event-based surveillance system was the major cited reason for the late detection of the outbreak in 2022.
Conclusion: The measles surveillance system was simple, somewhat stable and acceptable, but neither sensitive nor timely. Lack of health worker training and poor community case finding threatened the performance of the surveillance system. Refresher training for all healthcare workers and intensified community event-based surveillance are needed.
In Africa, 30 million cases of measles and 900 000 deaths are recorded annually [1]. An estimated 13 million cases and 650 000 deaths have been recorded from 2000 to 2020 in Africa. The sub-Saharan region has the highest morbidity and mortality. The World Health Organisation (WHO) African region recommended that countries implement measles case-based surveillance with laboratory confirmation as one of the main strategies for measles control [2]. World Health Organization (WHO) African region adopted measles control activities in 2001, aiming to reduce measles deaths by 2005. The strategies implemented included improving vaccination coverage, supplementary immunization activities (SIAs), improving measles case-based management, and establishing case-based measles surveillance [3]. In September 2011, the 47 World Health Organization (WHO) African Region (AFR) member states adopted goals of measles elimination by 2020, by achieving 95% or greater coverage of their target populations with the first dose of measles containing vaccine (MCV1) at national and district levels, 95% or greater coverage with measles containing vaccine (MCV) per district during SIAs and confirmed measles incidence of less than 1 case per 1 million population in all countries [4–6].
Two key surveillance performance indicator targets include investigating 2 or more cases of non-measles febrile rash illness per 100,000 population annually and obtaining a blood specimen from 1 or more suspected measles cases in 80% or more of districts annually [5]. Zimbabwe, a member state of WHO Afro-Region, has recorded a single case each year from 2016 to 2017. However, in 2019 and 2020 four and three cases were detected respectively [7]. In 2022 Zimbabwe recorded nearly 7701 cases and 747 deaths by 30 September 2022 during the measles outbreak, and Matabeleland South Province was not spared, with more than 10 epidemiologically linked deaths being recorded in Insiza District.
The WHO recommends that preparation for measles elimination should be integrated with active case-based surveillance confirmed by laboratory investigations [8]. Every suspected case should have blood samples collected for measles-specific antibody. The serum samples adequate for detecting measles immunoglobulin M (IgM) are collected in at least 80% of suspected measles cases (excluding from the denominator cases that are epidemiologically linked to the laboratory-confirmed cases). There is viral isolation obtained from every confirmed chain of transmission (for genotyping to help identify the source of the virus).
Countries in elimination zones should collect case-based data. Disease incidence and performance indicators for countries collecting case-based data are annual incidences of measles cases (laboratory confirmed and epidemiologically linked), deaths, annual national incidences of non-measles, and suspected measles cases (target more than 2 per 100,000 population). Eighty percent of the districts should report at least one non-measles suspected case per 100,000 population annually. Every suspected case of measles should be investigated within 72 hours. In measles surveillance, 80% of identified cases should be investigated within 72 hours [9].
Measles case-based surveillance in Zimbabwe
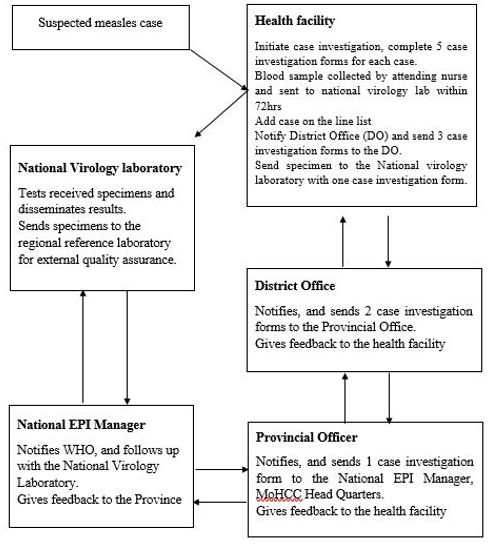
Measles surveillance begins at the health facility level. Suspected measles cases data is collected routinely by health workers at all levels of the health delivery system, and the measles case-based surveillance form is used. Data from the primary facilities is sent through the district, province, and onto the national level (MOHCC Head Office), where it is entered into the measles case-based surveillance system database. The data is consolidated, cleaned, analyzed and disseminated for action. This data is also shared with the World Health Organisation (Figure 1).
Measles surveillance in Insiza District
Between 2019 and 2021, Insiza District failed to meet the target of investigating all identified suspected measles cases, investigating only 2 out of the identified 6 in 2019, 2 out of the identified 8 in 2020 and one out of the identified 7 in 2021. Furthermore, in 2022, the district only detected a measles outbreak after 14 days, and after a total of 10 community deaths of measles had occurred. The measles-rubella 1 (MR1) and measles-rubella 2 (MR2) coverage for Insiza is 72% and 69%, respectively. Despite support and supervision being provided in the province and training of healthcare workers to strengthen active surveillance and case detection of measles, not all cases were investigated.
Continued failure to investigate all cases may result in unnoticed spreading of the disease, leading to the burden of morbidity and mortality, outbreaks and failure to achieve elimination. We therefore evaluated the measles case-based surveillance system for Insiza District to determine reasons for failure to meet targets set for detection and investigation of measles cases.
Study design
This study used a mixed-methods approach. A descriptive cross-sectional study using the updated Centres for Disease Control (CDC) guidelines for evaluation of a surveillance system was done to collect quantitative data, and in-depth interviews to collect qualitative data. The study was conducted from 15 January 2024 to 15 February 2024.
Study setting
The study was conducted in Insiza District, in Matabeleland South Province, the south-western part of Zimbabwe. Insiza District has 19 health facilities that all provide routine immunisation, including rural district council clinics, one private facility and one district hospital (Filabusi District Hospital). The health facilities collect blood samples and submit them to the National Virology Laboratory, where measles diagnosis is done.
Study population
The study population were healthcare workers in Insiza District. Records reviewed included outpatient records (patient-held), outpatient register/Tally 12 (T12), Integrated management of childhood illness (IMCI) registers, and measles case notification forms. The study participants were nurses and environmental health technicians involved in measles surveillance.
Sample size calculation
Sample size was calculated using the Dobson formula [10]
$$n = \frac{z^2 p (1-p)}{d^2}$$
based on a study by Makova et al, 2017-2020, where good knowledge of health workers on the measles surveillance system was found to be 87.7% at 95% confidence level, z=1.96 and d = 0.1, and a non-response rate of 10%. The minimum sample size for health workers calculated was 46 [11]. All the case notification forms from the years 2021-2023 were reviewed for completeness and data quality. The IMCI register for 2023 was actively searched for cases meeting the standard case definition of measles.
Sampling
We applied stratified sampling for health facilities, i.e. hospitals and clinics were the strata. There are 4 hospitals and 15 clinics. We randomly selected two hospitals (Filabusi District Hospital and Shangani Rural Hospital) and seven clinics to represent either strata. At each clinic, there are two nurses and one environmental health technician. All health workers found on duty at the clinic on the day of the survey were included in the study. Several hospital departments that attend to children (outpatients, family and child health, children’s ward, male and female wards) participated in measles surveillance. We included all nurses on duty from the different departments on the day of the survey, and the two environmental health technicians stationed at the hospital. It was important to stratify by hospital and clinics to allow for the selection of participants by department at the hospital level. The District Health Executive, sisters in charge and health information officers were our key informants. All measles case-based surveillance forms for the period 2021– 2023 were reviewed.
Data collection tools and techniques
A pretested interviewer-administered questionnaire developed by the researchers was used to collect data from health workers on knowledge of the measles case-based surveillance system and the attributes of the system, which include simplicity, data quality, acceptability, representativeness, timeliness, and stability.
The researchers developed the interviewer-administered questionnaire and pretested it. Knowledge was assessed by a set of 15 questions, and a Likert scale classified the knowledge into poor, fair and good. A key informant guide was used to collect data from key informants who were members of the district health executive and the health information officer. The researchers conducted interviews in private at the key informant’s workplace to understand the reasons for failure to meet targets and not investigate cases.
Checklists were used to assess the availability of the resources needed for running the measles case-based surveillance system to measure the stability of the system, to review measles case-based surveillance data quality, and to review the timeliness and completeness of the measles case-based surveillance data. Reports and minutes from surveillance meetings, spot maps, and line lists were used to assess the usefulness of the system. We directly observed healthcare workers completing the measles case investigation form.
Data analysis
Data were analysed using Epi Info version 7 to generate frequencies, means, and proportions. Knowledge level was assessed by asking fifteen questions on measles case-based surveillance system and analysed using a three-point Likert scale (good knowledge = 11-15 correct answers, fair knowledge = 8-10 correct answers and poor knowledge = 0-7 correct answers). Participants who scored twelve and above were categorised as good knowledge, seven to eleven were catergorised as fair knowledge and below seven as poor knowledge. We read through qualitative transcripts, coded the data and grouped the coded data under themes.
Sensitivity was measured by calculating the proportion of cases in the population that were detected by the surveillance system in a given year or period. Transport cost was measured by distance covered and the cost of fuel per litre. The cost of notifying measles suspected cases using a paper-based system and the use of an electronic-based system was also calculated. The costs were calculated per month/year using prevailing market prices. We calculated the cost of paper used for collection and compiling data, the call charges to verify information and notify the district, assuming an average call cost of 8.3 cents, time spent completing measles surveillance forms as a proportion of the nurse’s salary and transport charges for sending forms from facilities to the district.
Permission and ethical considerations
The Provincial Institutional Ethics Committee approved the study (MS/EC/203/24). Permission to carry out the study was obtained from the Provincial Medical Director (PMD) of Matabeleland South and the District Medical Officer (DMO) of Insiza District, and the Health Studies Office. Informed written consent was obtained from all the interviewees and they were assured of confidentiality. Participants were advised that they will be no monetary benefits for participating, and participation was voluntary, and they could withdraw from the study at any time during the study. Any information obtained in connection with this study was not linked to the participants. The data was handled as confidential and was only shared with the University of Zimbabwe and Matabeleland South Province. Participants’ identities were be kept confidential and participants were not required to put their names on the questionnaire. Records of the data and the consent form were kept under lock and key. The data was only accessed by the investigators.
The response rate was 87.0% (40/46) with a total of 40 health workers interviewed. They comprised 26 (65%) nurses, one (2.5%) doctor, 8 (20%) environmental health technicians and one (2.5%) health information officer. Majority of the participants were females, 30 (75%), and males were 10 (25%). Median age was 37.5 (IQR: 28.5 – 47)years, and the median years in service was 11.5 (IQR: 6-16) years (Table 1).
Most of the participants, 21 (52.5%), had fair knowledge of the measles case-based surveillance system, 11 (27%) had good knowledge, and 8 (20%) had poor knowledge. The majority of participants, 38 (95%), knew the case definition of measles. The majority of the participants, 36 (90%), knew the phase Zimbabwe is on measles surveillance.
Participants 34 (85%) also demonstrated knowledge of the type of sample that is collected for measles investigation. A total of 20 (50%) participants knew the correct time limit to investigate a suspected measles case. Only 28 (70%) of the participants interviewed knew the number of case investigation forms to be filled for measles investigation (Table 2).
Usefulness
The majority, 37 (92.5%), perceived the system to be useful. The majority of the participants, 36 (90%), reported that they conducted surveillance meetings at the local level; however, only 3 facilities out of the 10 facilities visited produced minutes of weekly surveillance meetings. Although participants reported using the surveillance system to detect outbreaks, only 3/10 had charts to monitor measles incidence. Line lists for suspected cases were kept in 5/10 facilities. Spot maps were not available in all 10 health facilities. Reports of vaccination campaigns and awareness campaigns were available at 2 out of the 10 facilities (Table 2).
Stability
Only 8 (20%) of the participants had ever received training on measles surveillance. Eight out of the ten health facilities visited had case investigation forms and Expanded Program on Immunisation (EPI) guidelines available. Case definitions were available at 10/10 of the health facilities. Specimen collection tubes and specimen carrier boxes were available at all of the health facilities. The results showed that the surveillance system was somewhat stable (Table 2).
Simplicity
The majority, 24 (60%), of the participants reported that they had ever completed measles case investigation forms. Simplicity was assessed for the 24 participants who had prior experience with the system. Only 6 (25%) required more than 20 minutes to complete the case investigation forms. The majority, 18 (75%), required 10-20 minutes and less than 10 minutes to complete the case investigation forms. Two healthcare workers were asked to fill in the case investigation form whilst the investigator observed. Both healthcare workers took between 10 and 20 minutes to complete the forms. The system was deemed simple.
Data quality
All of the 10 forms evaluated for the year 2022 were not filled in some sections. Information on the date the sample was received at the virology laboratory and the results of the sample were missing on all 10/10 the case investigation forms. All 9 forms evaluated for the year 2023 were not completely filled in some sections. Three out of 9 forms had the date specimen received in the laboratory and date specimen examined documented. None of the 9 forms had date results received. Data quality was deemed poor.
Timeliness
The majority (18/24) of the suspected measles cases evaluated on the case investigation forms were reported within seven days of the onset of rash. Investigation of some of the cases (12/24) was conducted within 48 hours. The time of reaching the virology laboratory was not documented, except for one specimen and the period during which the results were received. The surveillance system was not timely (Table 3).
Sensitivity
The set annual target of 3 suspected measles investigations was not met by the district from 2020 to 2021. This is despite a review of six IMCI registers showing 12 cases meeting the case definitions of measles at 3 facilities reviewed. A total of 1 209 records were reviewed from the six registers. In 2022, 10 suspected cases were identified, and all 10 were investigated. None of the 10 cases investigated were confirmed as measles. However, on review of the records, 24 cases met the case definition. Fourteen suspected measles cases were missed. In 2023, 9 suspected cases were identified, and 7 suspected cases were investigated, with one confirmed case. However, on records review, 11 cases met the case definition. Two suspected measles cases were missed. The surveillance system was deemed not sensitive (Table 3).
Cost of operating the measles case-based surveillance system
The estimated cost for reporting one suspected measles case in US dollars included stationery USD1, completion of surveillance forms USD10, call charges USD2, and transport charges USD10, and the total cost was USD 23 per month.
Reasons for failure to investigate all cases
The majority of the participants (36/40) 90% cited lack of training on the measles case-based surveillance as the main reason for failure of the surveillance system. The second most cited reason was poor healthcare worker knowledge of the surveillance system (30/40), 75%. Six out of the forty participants (15%) reported that the unavailability of resources was a reason for failure to investigate all cases, and the resources cited were mainly fuel for contact tracing and a shortage of case investigation forms.
Reasons why the 2022 suspected measles outbreak was detected late
All of the participants (40/40) 100% mentioned the behaviour of people who do not accept modern medicine based on their religion (religious objectors) of hiding illness amongst themselves and not reporting to the health system as the main reason why the suspected outbreak in 2022 was detected late. Additionally, a weak event-based surveillance system was mentioned by 57% (23/40) of the participants. Poor community participation was mentioned as another reason for why the outbreak was detected late, 80% (32/40).
Key informant interviews
Four main themes emerged during key informant interviews, that is, healthcare worker motivation, staff attrition/staff shortage, lack of feedback and religious objection.
Healthcare worker motivation
Key informant interviews revealed that sometimes healthcare workers were not motivated to fully participate in the surveillance system, hence the failure to investigate all cases.
“Healthcare workers are working under poor conditions, and this is coupled with a heavy workload. There are no incentives for doing better, and they will do the minimum they can and end there. I also find it difficult to push them further under these circumstances”. Key informant 1
When the expected target of investigating 2 per 100 000 cases is reached, no further investigations are done for those who meet the case definition.
Staff attrition/shortage
They also cited high staff attrition and staff shortages as some of the contributing factors for failure to investigate all cases as available.
“With the prevailing economic climate and poor remuneration for staff, our staff are resigning as they either move to better-paying jobs or emigrate in search of opportunities elsewhere. This leaves us most of the time with inexperienced staff with little or no knowledge of surveillance to run the facilities. They are overwhelmed with work, compromising surveillance activities” Key informant 2
Staff are overwhelmed with work, and as the experienced, trained healthcare workers leave, the inexperienced remain and have limited knowledge on measles surveillance.
Lack of feedback
It was also noted that the selected healthcare workers who attend training workshops may not come back and give feedback or teach the remaining cadres at the facility. This is evidenced in this quote:
“We have a challenge with staff participating in training or refresher workshops giving adequate feedback to staff who did not attend due to a variety of reasons. Summarising a day’s or week’s training in a morning session before work begins is not enough exposure for those who did not attend”. Key Informant 1
Lack of active case finding in registers was also mentioned as a contributing factor to not investigating all cases as they appear in the registers.
Religious objectors
Concerning why the measles outbreak in 2022 was detected late, one of the key informants said, and I quote:
“Religious objectors pose a great challenge in measles elimination in Insiza as they do not report illness to health authorities, refuse vaccinations and investigation. Additionally, the population is highly mobile, crossing over to neighbouring districts, and most cases are missed in the community, and we only discover them late, as in the previous outbreak”. Key Informant 3
This group of people is highly mobile between districts and secretive about their operations and burials, which affects our surveillance activities. A poor event-based surveillance system was mentioned by one of the key informants as a reason why the measles outbreak in Insiza District was detected late.
The study found that the main reasons for failure to investigate all cases were a lack of training and poor knowledge of measles case-based surveillance. Most healthcare workers had a fair knowledge of the surveillance system. The healthcare workers perceived the system to be simple, acceptable, somewhat stable and useful.
The most common reasons cited by healthcare workers for failure to investigate all cases were lack of training and poor knowledge of measles case-based surveillance. Refresher training has been reported to improve knowledge and enable healthcare workers to identify patients meeting the case definition of measles early, have a high index of suspicion and be able to respond appropriately to suspected cases according to the guideline. Those who receive training outside the health facility should be able to give feedback to the remaining cadres and conduct in-house training [6,12,13].
A majority of the participants had fair knowledge of the measles case-based surveillance system. This could be attributed to the selective training of healthcare workers per facility. As noted by the key informant interviews, when others attend training workshops, they may not come back and provide feedback to the rest of the team at the facility.
Despite the median years in service being 11.5 years, less than half of the participants had good knowledge. Our findings were similar to Makova et al (2022) in Kwekwe, who noted that despite the high years in service, knowledge of the measles case-based surveillance system was mostly fair [11]. The fair and poor knowledge could be attributed to a lack of training on the measles case-based surveillance system.
Good knowledge of the measles case-based surveillance system is of importance in the performance of the system and early detection of outbreaks [3,14–18]. The findings were contrary to the findings in Masvingo District, where the majority of the participants had excellent knowledge of the system [19].
A poor-performing event-based surveillance system was indicated as a major issue in why the measles outbreak was detected late. Event-based surveillance is meant to complement routine case-based surveillance in detecting cases in the community.
In a setting where there are religious objectors and hard-to-reach areas, a functional event-based surveillance system would greatly improve measles elimination in the district. Our findings are similar to Makoni et al (2015) in Gokwe North, who mentioned that cases were not being reported from the community, and this threatened the performance of the surveillance system and led to late detection of outbreaks. The author mentioned the importance of involving village health workers in the surveillance as well as improving the community involvement in the surveillance system [15,20,21].
Though the majority of healthcare workers perceived the surveillance system to be useful, most of the health facilities did not have minutes for surveillance meetings or reports for health education promotions and risk communication sessions conducted. The District Hospital, the Mission Hospital, and one other facility detected the outbreak in 2022. This could be attributed to poor documentation and prioritisation of other competing programs among health workers. These findings are contrary to Chimsimbe et al, (2020) in Chegutu, who noted that the surveillance system was useful to the healthcare workers and reports were generated from activities done as a result of analysis of the surveillance system data 2]. Data generated was used for public health actions, and the system detected and responded promptly to cases of measles. However, this was not consistent with findings by Mitiku et al. (2019), who reported that measles surveillance in Afar Region, Ethiopia, was not useful and no action had been taken as a result of data analysis and interpretation [23].
Our results revealed that the system was simple, acceptable and somewhat stable. Simplicity of the surveillance system motivates health workers’ willingness to participate. Simplicity is crucial for effective implementation, as it allows health workers to easily understand and participate in the surveillance system without extensive training. This aligns with findings from Makova et al 2020 in Kwekwe, which emphasise that a simple surveillance system enhances reporting rates and data accuracy, ultimately contributing to better performance of the surveillance system [11]. Furthermore, the stability of the system indicates that it can consistently function over time, which is essential for maintaining ongoing surveillance and a timely response to measles cases. A stable system fosters trust among health workers, encouraging them to report suspected cases promptly, thereby improving the overall effectiveness of the surveillance efforts. The lower proportion of trained healthcare workers in Insiza affected the system’s stability, though resources like case investigation forms and case definitions were available.
Additionally, acceptability can lead to better compliance with reporting protocols and increased participation in surveillance activities, which are vital for early detection and response to measles outbreaks. The combination of simplicity, stability, and acceptability not only enhances the functionality of the surveillance system but also supports the broader goal of measles elimination in the region, as effective surveillance is a cornerstone of public health initiatives aimed at controlling vaccine-preventable diseases.
Despite the surveillance system being simple and stable, data quality was poor, and the system was neither timely nor sensitive. This can be attributed to the lack of training of healthcare workers on data quality, timelines for submission and active case finding at the facility. Moreover, the high staff attrition leading to the remaining healthcare workers being overwhelmed with competing programs may contribute to limited time being dedicated for active case finding in the registers and failure to meet deadlines. These findings concurred to Makoni at al, 2020 who found the system to be not sensitive attributed it to poor healthcare worker knowledge and being overwhelmed with competing programs [20,22].
Limitations
Most of the data was self-reported and has possible reporting bias. We, however, triangulated the data using other sources of data to minimise this bias. We did not manage to reach the calculated sample size, which might affect the power of the study. We, however, included all eligible participants in the district. The number of interviewed health workers did not reach the calculated sample size of 46. These should be taken into consideration while interpreting the results of our work.
The system failed to identify cases on time because health workers had limited knowledge, were not fully motivated to participate and staff shortages. The measles case-based surveillance system in Insiza District was simple, somewhat stable and acceptable but neither sensitive nor timely and data quality was poor. Healthcare workers’ knowledge was fair. Lack of health worker training and poor community case finding threatened the performance of the surveillance system. Refresher training for all healthcare workers and intensified community event-based surveillance are needed.
Recommendations
We recommended periodic refresher training for all healthcare workers on the measles case-based surveillance system and feedback sessions at the facility level. Additionally, quarterly mentorship and supportive supervision in the measles case-based surveillance system, as well as monthly active search in registers for cases meeting the measles case definition. Identification and training of more village health workers manning border and hard-to-reach villages on measles event-based surveillance and cross-border collaboration meetings between Insiza and Zvishavane districts. Community awareness programme on measles involving community leaders, church leaders and women.
Public health actions
The following public health actions were undertaken: Training of 12 health workers on the measles case-based surveillance system, distribution of rumour log books drafts to facilities, development of community case definition in Ndebele with community nursing and health promotion departments and distribution of case investigation forms to the private health facility in Insiza.
What is already known about the topic
What this study adds
Addmore Chadambuka is an Associate Editor at the Journal of Interventional Epidemiology and Public Health (JIEPH) and a co-author of this manuscript. In line with the journal’s conflict-of-interest policy, he was fully recused from the peer-review process and had no involvement in the editorial handling or decision-making for this submission. An independent editor oversaw the review and decision-making process. All other authors declare that they have no competing interests.
All authors contributed equally to the development of this article
Kudzai Hwacha contributed to conceptualization, formal analysis, investigation, methodology, writing – original draft, and writing – review & editing. Andrew Muza contributed to conceptualization, formal analysis, methodology, supervision, writing – original draft, and writing – review & editing. Tsitsi Patience Juru contributed to conceptualization, formal analysis, methodology, supervision, writing – original draft, and writing – review & editing. Notion Tafara Gombe contributed to conceptualization, formal analysis, investigation, methodology, supervision, writing – original draft, and writing – review & editing. Gibson Mandozana contributed to conceptualization, formal analysis, supervision, writing – original draft, and writing – review & editing. Gerald Shambira contributed to conceptualization, formal analysis, methodology, software, writing – original draft, and writing – review & editing. Mufuta Tshimanga contributed to conceptualization, formal analysis, methodology, supervision, writing – original draft, and writing – review & editing. Addmore Chadambuka contributed to conceptualization, formal analysis, supervision, writing – original draft, and writing – review & editing.
Table 1: Demographic characteristics and knowledge of healthcare workers on the measles case-based surveillance system in Insiza District, Zimbabwe, 2023
| Characteristic | Frequency N= 40 (%) |
|---|---|
| Designation | |
| Medical Doctor | 1 (2.5) |
| General Nurse | 13 (32.5) |
| Primary Care Nurse | 10 (25) |
| Midwife | 1 (2.5) |
| Environmental Health Officer | 8 (20) |
| Health Information Officer | 1 (2.5) |
| Village Health Worker | 6 (15) |
| Sex | |
| Male | 10 (25%) |
| Female | 30 (75%) |
| Median age | 37.5 Years (Q1=28.5; Q3=47.0) |
| Median years in service | 11.5 Years (Q1=5.5; Q3=17.5) |
| Participants who knew | |
| Measles case definition | 38 (95) |
| Time limit to investigate suspected measles case | 20 (50) |
| Number of investigation form copies to be filled | 28 (70) |
| Phase in which Zimbabwe is on measles surveillance | 36 (90) |
| Type of sample collected for investigation | 34 (85) |
| Participant knowledge assessment | |
| Good | 11 (27.5) |
| Fair | 21 (52.5) |
| Poor | 8 (20) |
Table 2: Usefulness and attributes of the measles case-based surveillance system in Insiza District, Zimbabwe, 2023
| Variable | Frequency n= 40 Percentage (%) |
|---|---|
| Usefulness | |
| Perceived the system to be useful | 37 (92.5) |
| Conduct surveillance meetings | 36 (90%) |
| Planning for resource requirement and distribution | 22 (55%) |
| Policy making | 0 |
| Plan for training of healthcare workers | 3 (7.5%) |
| Awareness and Vaccination campaigns | 11 (27.5%) |
| Conduct research | 1 (2.5%) |
| Detect Outbreaks | 25 (62.5%) |
| Stability | |
| Received training in EPI surveillance including measles | 8 (20%) |
| Knew measles case definition available | 34 (80%) |
| Case definition displayed | 10/10 |
| Measles case investigation forms available | 34 (80%) |
| EPI Guidelines available | 34 (80%) |
| Cell phone or landline available | 10/10 |
| Transport available | 10/10 |
| Specimen collection tubes available | 10/10 |
| Simplicity | |
| Ever completed a measles investigation form | 24 (30%) |
| Reported time to complete in minutes | |
| Less than 10 | 6 (25%) |
| Between 10-20 | 12 (50%) |
| More than 20 | 6 (25%) |
| Data Quality | |
| Any difficulties in completing the form (No) | 24 (100%) |
| Forms correctly filled in all sections | 0/10 |
| Areas incompletely filled in | |
| Case identification | 5/10 |
| History of vaccination | 8/10 |
| Blood specimen information | 2/10 |
| Final classification | 10/10 |
Table 3: Timeliness of measles case-based surveillance system in Insiza District, Zimbabwe, 2023
| Timeliness | ||||||
|---|---|---|---|---|---|---|
| Year | Suspected cases detected | Reported within 7 days of rash onset | Investigated within 48 hours | Reaching the lab within 3 days | Results received within 7 days | |
| 2020 | 2 | 1 | 1 | 0 | 0 | |
| 2021 | 3 | 3 | 2 | 0 | 0 | |
| 2022 | 10 | 7 | 6 | 0 | 0 | |
| 2023 | 9 | 7 | 3 | 1 | 0 | |
| Sensitivity | ||||||
| Year | Total population target | Cases Expected | Cases detected | Cases investigated | Results confirmed | Calculate sensitivity |
| 2020 | 132323 | 3 | 0 | 0 | 0 | 0 |
| 2021 | 133794 | 3 | 0 | 0 | 0 | 0 |
| 2022 | 135282 | 3 | 10 | 10 | 0 | 0 |
| 2023 | 136191 | 3 | 9 | 7 | 1 | 14.3% |