Research | Open Access | Volume 9 (2): Article 107 | Published: 29 Jun 2026
Views: 460
Menu, Tables and Figures
| Kidney Diseases | Frequency (n=885) | Percentage (%) |
|---|---|---|
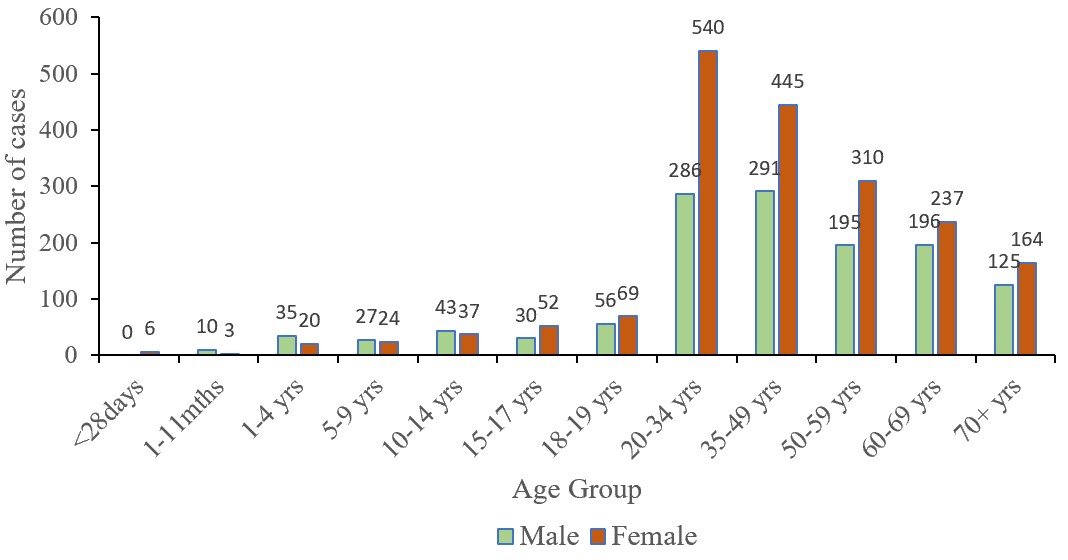
| Diabetic kidney disease | 328 | 37.1 |
| Pyelonephritis | 103 | 11.6 |
| Hypertensive renal diseases | 97 | 11.0 |
| Nephrotic syndrome | 61 | 6.9 |
| Chronic kidney disease, unspecified | 49 | 5.5 |
| Nonobstructive reflux-associated chronic pyelonephritis | 33 | 3.7 |
| Unspecified renal colic | 29 | 3.3 |
| Calculus of the kidney | 27 | 3.1 |
| Acute Renal Failure | 24 | 2.7 |
| Acute tubulointerstitial nephritis | 23 | 2.6 |
| Chronic kidney disease, stage 5 | 21 | 2.4 |
| End-stage renal disease | 14 | 1.6 |
| Chronic kidney disease, stage 4 | 13 | 1.5 |
| Unspecified hydronephrosis | 13 | 1.5 |
| Chronic kidney disease, stage 2 | 11 | 1.2 |
| Chronic obstructive pyelonephritis | 9 | 1.0 |
| Polycystic kidney | 8 | 0.9 |
| Chronic kidney disease, stage 3 | 6 | 0.7 |
| Hydronephrosis with ureteropelvic junction obstruction | 6 | 0.7 |
| Chronic kidney disease, stage 1 | 4 | 0.5 |
| Cyst of the kidney | 3 | 0.3 |
| Hydronephrosis with renal and ureteral calculous obstruction | 3 | 0.3 |
Bakalilu Kijera1,&, Abdul Nasir Alhasan2, Sarja Jarjusey1, Mary Bobb1, Lamin Manjang1, Delia Bandoh1, Donne Ameme1, Charles Lwanga Noora1, Ernest Kenu1
1Ghana Field Epidemiology and Laboratory Training Programme, School of Public Health, University of Ghana, Legon, Ghana, 2Ghana Health Services, Accra, Ghana
&Corresponding author: Bakalilu Kijera, Ghana Field Epidemiology and Laboratory Training Programme, School of Public Health, University of Ghana, Legon, Ghana, Email: bkkijera@gmail.com, ORCID: https://orcid.org/0009-0006-0055-147X
Received: 20 Apr 2025, Accepted: 25 Jun 2026, Published: 29 Jun 2026
Domain: Non-communicable Disease Epidemiology
Keywords: Kidney diseases, spatial analysis, outpatient, Ho Municipality
©Bakalilu Kijera et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Bakalilu Kijera et al., Epidemiology of acute and chronic kidney diseases among outpatients in Ho Municipality, Ghana, 2022. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):107. https://doi.org/10.37432/jieph-d-25-00096
Introduction: Kidney diseases are a major public health concern in Africa. Due to a paucity of epidemiologic data from different African countries, the issue remains underestimated on the entire continent. We determine the epidemiological distribution by person, trend, and clinical spectrum of outpatient kidney disease data in Ho Municipality.
Methods: Outpatient kidney disease data from January 1, 2017, to December 31, 2021, were extracted from electronic records of the District Health Information Management System 2 and the Lightwave Health Information Management database. Patients’ aggregated age group, sex, reporting health facility, and clinical condition of kidney diseases were collected. Spatial analysis and descriptive statistics, including frequencies, percentages, and rates per 100,000 population, were performed to describe the distribution of the data.
Results: A total of 3,201 cases of kidney disease were extracted, with a rate of 306 per 100,000 population. Of the cases, 59.6% (1907/3201) were female, and the 20-34 and 70+ age groups accounted for 25.8% (826/3201) and 9% (289/3201), respectively. The rate of kidney diseases per 100,000 population increased from 246 in 2018 to 486 in 2021. In all, 83% (2659/3201) of the cases were reported at Ho Teaching Hospital. Among the clinical spectrum, diabetes mellitus renal disease accounted for 37.1% (328/885). Pyelonephritis and hypertensive renal disease contributed 11.6% (103/885) and 11.0% (97/885) of kidney diseases, respectively.
Conclusion: Kidney diseases are increasing rapidly in the Ho municipality. Diabetic kidney disease, Pyelonephritis, and hypertensive renal disease are key clinical conditions related to kidney disease, and young adults are highly affected. The Director of Public Health should raise awareness of the alarming rate of kidney-related diseases in the population, especially among young adults, and strategise mechanisms to reduce the burden.
Kidney diseases are a major public health issue and can occur in people at any age and at any time [1]. The kidney plays an important role in maintaining water and electrolyte balance and regulating homeostasis. Kidney diseases, including renal cell carcinoma (RCC), acute kidney injury (AKI), and chronic kidney disease (CKD), are major causes of kidney failure, which leads to poor quality of life for patients and causes excessive burden and loss to society [2]. Kidney disease affects approximately 10% of the world’s adult population; it is one of the top 20 causes of death worldwide [3, 4]. Kidney diseases are mostly linked to high-risk diseases like hypertension and diabetes.
Sub-Saharan Africa has a higher prevalence of CKD than North Africa, and high-risk populations have a roughly twofold higher prevalence of CKD than the general population [5]. Kidney diseases are frequent, but they develop unnoticed in most instances. This paucity of symptoms may lead to late diagnosis and serious consequences [5, 6]. Kidney disease symptoms include life-threatening complications of uremia, such as pericarditis, pulmonary oedema, neurologic problems, and/or metabolic abnormalities, as kidney function becomes marginal [7]. Patients without comorbidities usually remain asymptomatic until eGFRs (estimated Glomerular Filtration Rate) are below 10 ml/min per 1.73 m2 [8].
Literature has reported that 50% of end-stage renal disease (ESRD) patients receive renal replacement therapy, and even less, in low and middle-income countries, and in Sub-Saharan Africa, less than 2% have access to ESRD. Kidney diseases and disorders that do not meet the diagnostic criteria for AKI, AKD, or CKD are classified as no known kidney disease (NKD)[9]. Examples of NKD include decreased kidney perfusion (volume depletion, heart failure, cirrhosis, segmental arterial, or venous infarction), parenchymal diseases (acute glomerulonephritis, new-onset nephrotic syndrome, pyelonephritis, interstitial nephritis, papillary necrosis, thrombotic microangiopathy, mild acute tubular necrosis, and mild transplant rejection), and obstruction of the urinary tract (stone or tumor, especially if unilateral) [9].
Due to a paucity of epidemiologic data from different African countries, kidney diseases remain underestimated in the entire continent [10-12]. Most people are unaware of kidney diseases or even where their kidneys are found. Healthcare providers are required to support individuals in preventing themselves and seeking care [13]. There are many “questions unanswered and answers unquestioned”[13]. We determined the epidemiological distribution by person, trend, and clinical spectrum of outpatient kidney disease data in Ho Municipality, Volta Region.
Study design and settings
A secondary data analysis of kidney diseases (acute or chronic) reported to the Outpatient Departments (OPD) of all the health facilities in Ho Municipality from January 2017 through December 2021. Data from electronic records of the District Health Information Management System (DHIMS2), Hospital Administration and Management System (HAMS), and Lightwave Health Information Management System (LHIM) databases were extracted on the 22nd November 2022. We showed the epidemiological distribution of kidney diseases in the district.
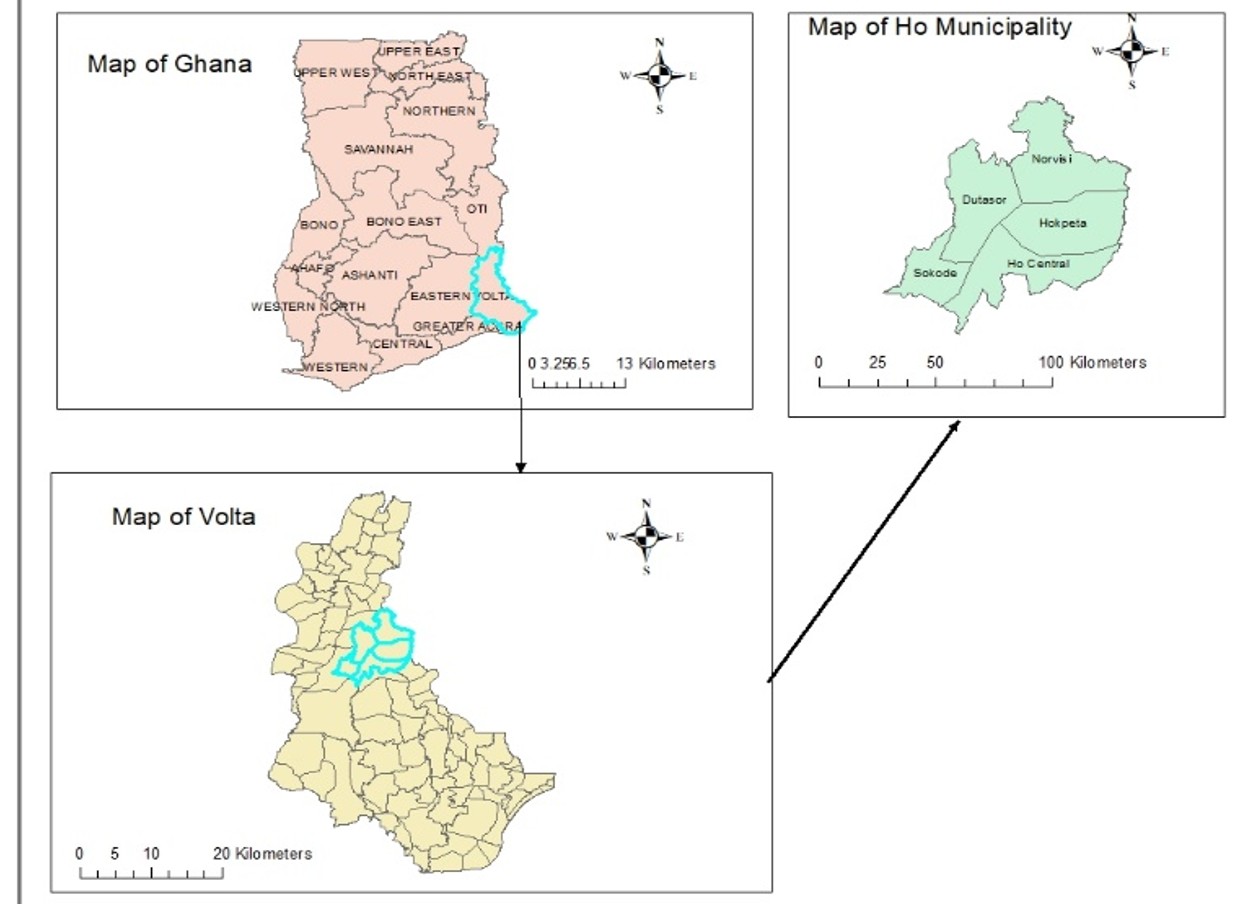
The study was conducted at the Ho Municipality, Volta Region. Ho Municipality is one of the 18 districts in the Volta Region. The district has five sub-districts (Hokpeta, Norvisi, Dutasor, Sokode / Akrofu, and Ho Central) (Figure 1), housing 61 health facilities (public and private), and two hospitals (Ho Municipal Hospital and Ho Teaching Hospital). Ho Municipality Teaching Hospital is the only hospital in the district with a dialysis machine. The district is bordered northwest by the Ho West district, east and southeast by the Adaklu-Anyigba district, and southwest by Togo. Ho Municipality has a total population of 184,209 and an under- 15 population of 96,266. In 2022, Hokpeta had a population size of 16,570, Norvisi 18,073, Dutasor 22,105, Sokode/Akrofu 20, 263, and Ho central 106,289.
Data source
Data were obtained from three health systems: DHIS2, HAMS, and LHIMS. Two levels of data were used. Individual-level data for 2021 were extracted from HAMS and LHIMS, including patient demographics and clinical information. For 2017–2020, only aggregated monthly data were available from DHIMS2, comprising reported case counts by facility and period. Data managers routinely enter patient data into HAMS/LHIMS and submit aggregated reports to DHIMS2. Facility-level data quality teams ensure accuracy, completeness, and timeliness.
Study variables
The study variables include: an aggregated patient’s age group, sex, reporting health facility, and population. The clinical condition of kidney diseases in 2021 was also collected.
Data collection and procedures
Datasets were cleaned and harmonised before analysis. Datasets on kidney diseases for the Ho Municipality were extracted from DHIMS2. In 2021, the Ho Municipal Teaching Hospital began using LHIMS, from which its data were extracted. Data for Ho Municipal Hospital and other health facilities for 2021 were extracted from the HAMS. Discrepancies were observed in the 2021 data, as all three databases were utilized during this period. Since HAMS and LHIMS contained individual-level data, these sources were prioritised over the aggregated DHIMS2 data.
Data analysis
The Ghana health services’ age-grouping of kidney diseases in DHIS2 was adopted, and a composite graph was developed by sex. The data collected were presented in frequencies, percentages, and proportions. Spatial analysis was performed using ArcGIS software to map the distribution of kidney-related disease cases across health facilities and hospitals. Annual kidney disease case counts were standardised by calculating rates per 100,000 population for each year. We also analyzed the clinical spectrum of kidney diseases in frequency and percentage for 2021.
Ethical Considerations:
The Head of the Diseases Surveillance Department of the Ghana Health Service permitted the data analysis to be conducted as part of surveillance activities to strengthen the surveillance system in the country. The individual-level datasets from LHIMS and HAMS were given unique identifiers and were anonymised to ensure confidentiality.
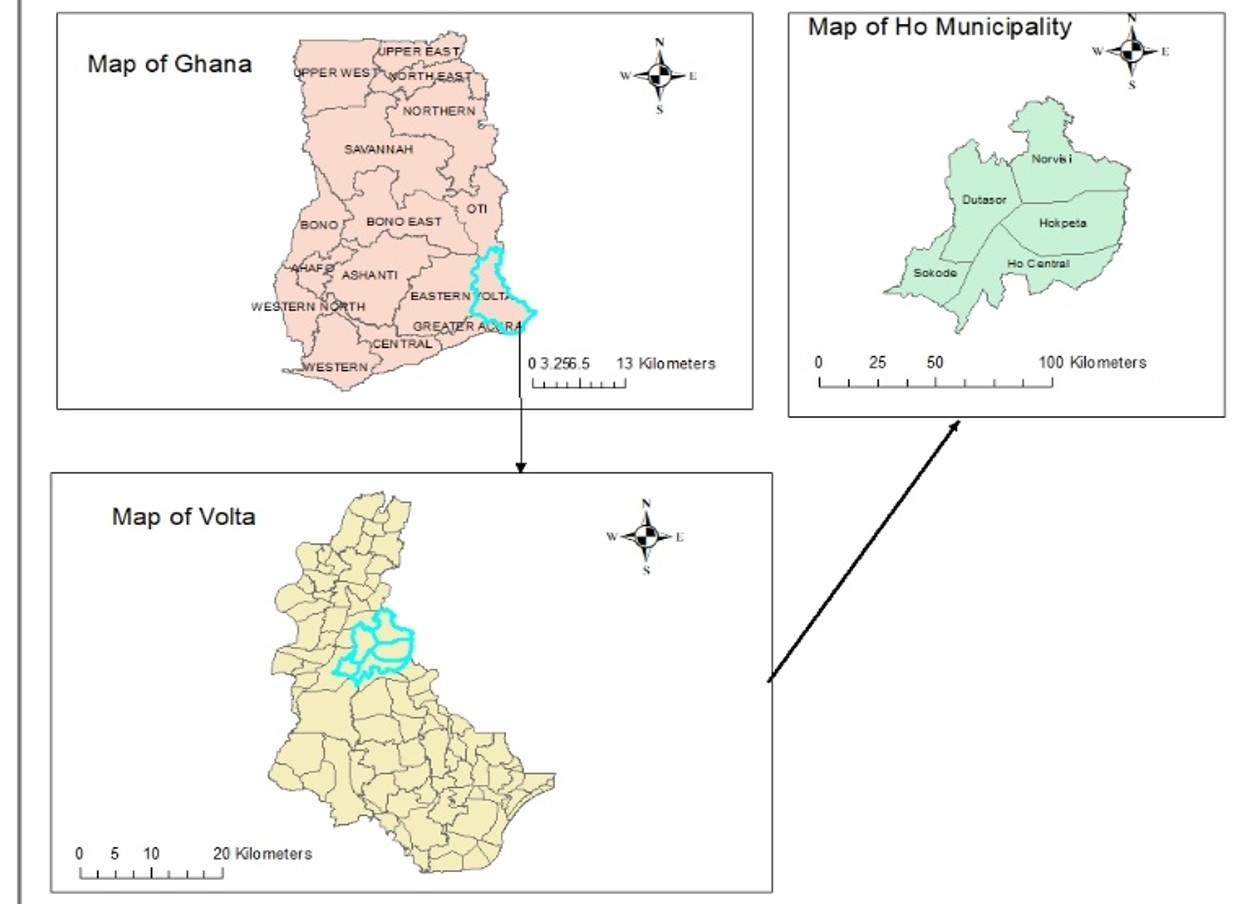
As shown in the spatial analysis of cases by health facility, more than three-quarters of the cases, 83% (2659/3201), were reported at Ho Teaching Hospital. Ho Municipal Hospital reported 13.6% (434/3201) cases, and Emmanuel Medical Hospital reported 0.2% (51/3201). However, cases were reported at some health facilities, including Ho Polyclinic, Nyive Health Centre, Miracle Life Health Centre, Matse Health Centre, Forsight Medical Centre, and Kiefe Health Centre. Hodzo and Ho Wusu were the two CHPS Compounds that reported at least one case of kidney disease during the five years (Figure 2).
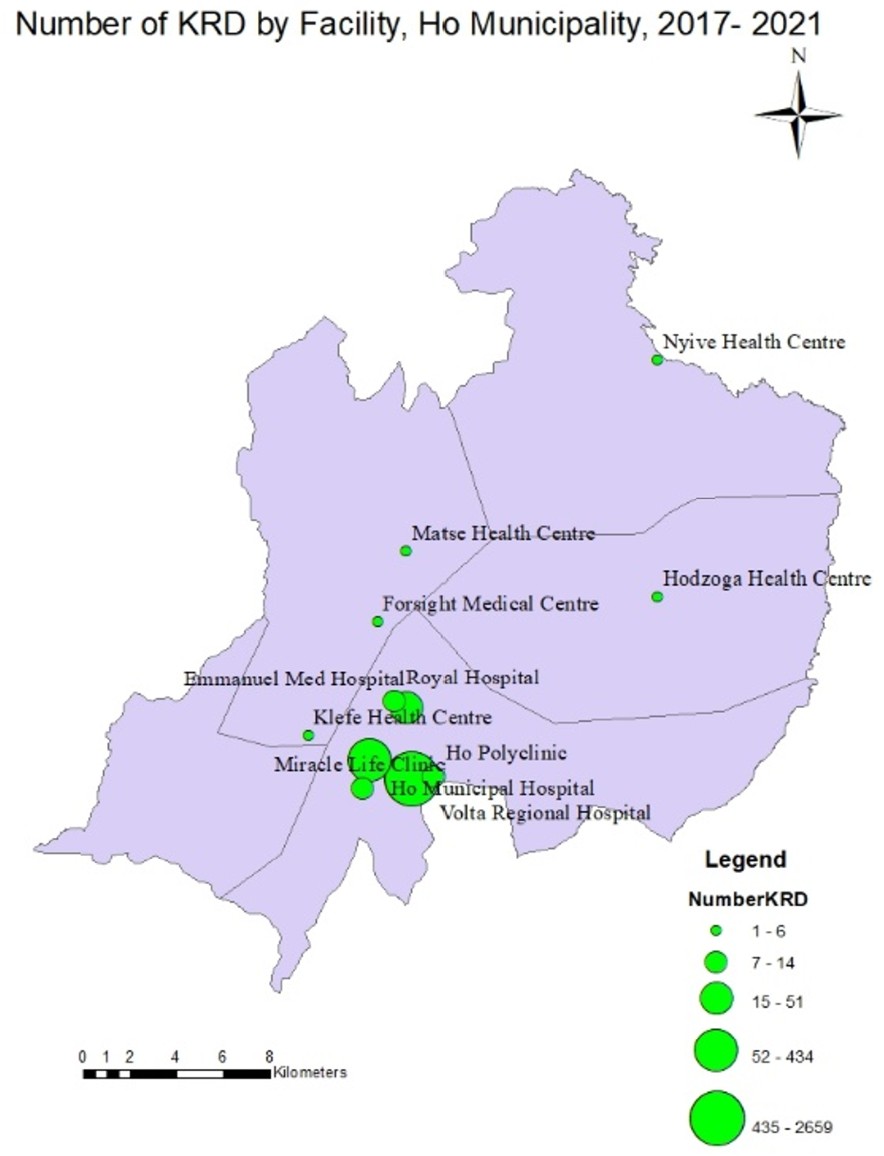
More than half, 59.6% (1907/3201), of the cases were female. The number of females aged 15 to 70+ with kidney diseases was higher compared to males. There were six cases among neonates, and the age group 20-34 reported the highest number of cases, 25.8% (826/3201). Patients aged 70+ years represent 9% (289/3201), and those <20 years constitute 12.9% (412/3201) of the total number of cases (Figure 3).
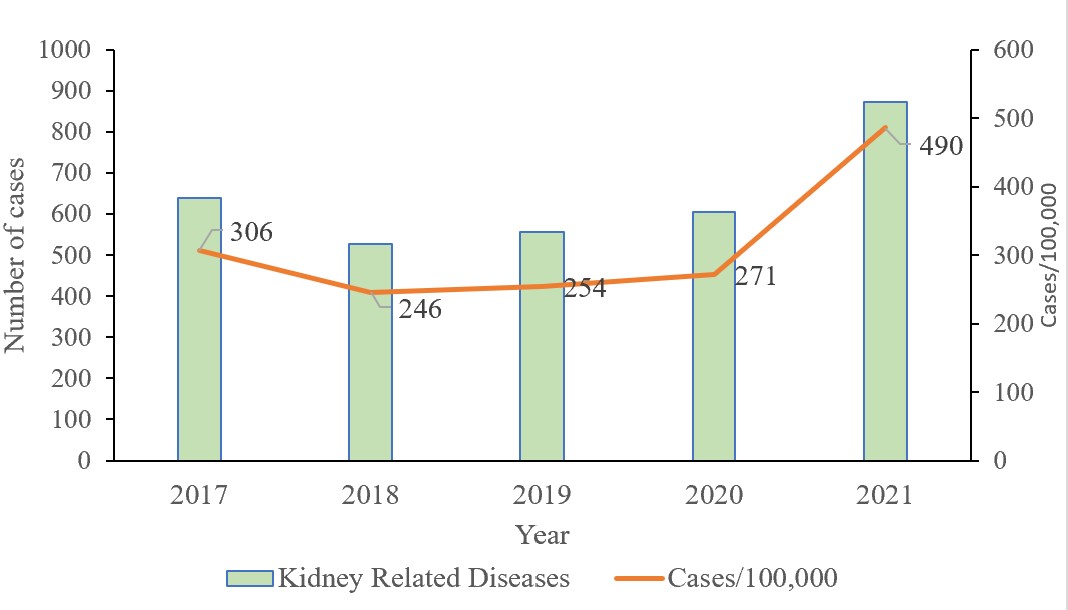
The number of kidney diseases reported has increased steadily from 2018 to 2021. In 2020, a proportion of 271/100,000 (606/223,947) of the kidney disease population was reported, which increased to 490/100,000 (872/180,420) population in 2021 (Figure 4).
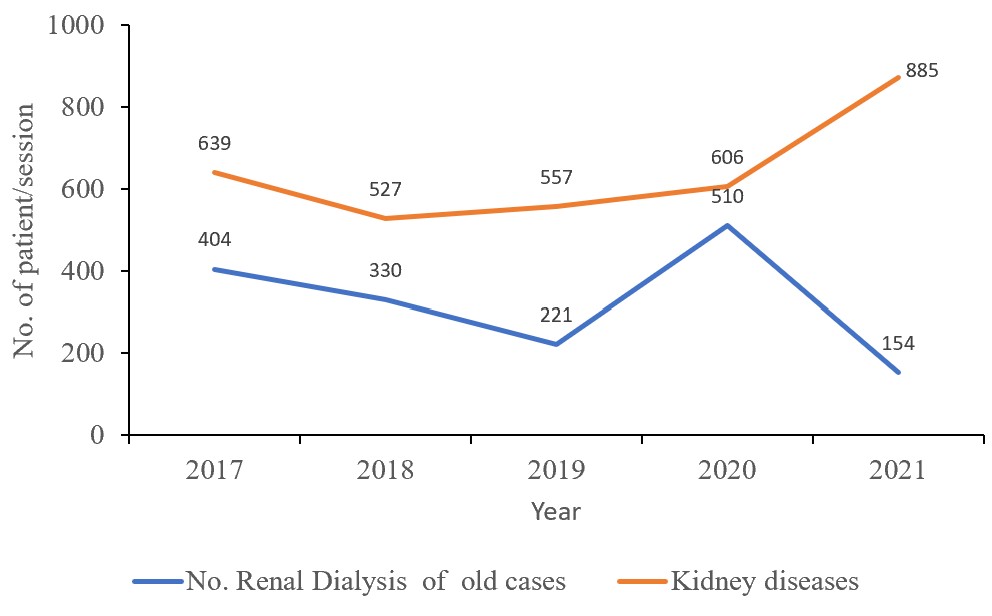
The number of kidney dialysis services was lower than the number of kidney diseases reported during the year in review. From 2020 to 2021, the number of dialyses conducted in the district reduced from 510 to 154 (Figure 5). Diabetic nephropathy constituted 37.1% (328/885) of all kidney disease cases reported in Ho Municipality in 2021. Pyelonephritis contributed 11.6% (103/885) of kidney disease cases. Hypertensive renal disease was ranked third with 11.0% (97/885). There were 5.5% (49/885) who were diagnosed with chronic kidney disease, unspecified (Table 2).
The findings of the study have shown that more than half of the kidney disease cases were female, and six cases were reported as early as age less than 28 days. The 20-34 age group reported the highest number of cases. In 2021, the rate of kidney diseases per 100,000 population was the highest. More than three-quarters of the cases were reported from Ho Teaching Hospital, and two Community Health Post compounds reported at least one case of kidney disease during the five years. The number of kidney disease cases reported from 2018 to 2021 has increased steadily.
The higher proportion of cases among females in this study is consistent with a study that suggested that women may be more vulnerable to kidney disease due to lower income, higher unemployment, and a growing ageing female population[14]. In addition, women have additional risk factors for kidney disease, like autoimmune disease, pregnancy-related acute kidney injury AKI, and preeclampsia (PE), which may lead to subsequent CKD [13, 15]. The use of combined oestrogen–progesterone oral contraceptive pills by women can be associated with a significant increase in blood pressure and albuminuria, and a decline in kidney function [16, 17]. Compared with men, women have a higher body mass index and are more likely to be overweight or obese, a history of hypertension [18], and this increases the risk of kidney diseases.
In addition, females generally demonstrate better health-seeking behavior than males. In a study done in Limpopo Province in South Africa, several factors were identified that contribute to men’s poor health-seeking behaviour, and these include self-treating, fear of knowing one’s own health condition, use of traditional medicine, consulting influencers within the community, as well as sticking to cultural values [18]. However, in another study, they associated a high incidence of cases among males due to exposure to environmental risk factors such as environmental and agricultural chemicals, smoking, etc.
We found that in 2021, the rate per 100,000 almost doubled when compared to 2020. One key reason was that in 2021, Ghana conducted a census, and the population in the district decreased. We used the 2011 projected population to calculate the rate from 2017 to 2020. In addition, the teaching hospital that reported more than three-quarters of kidney disease cases has shifted from the traditional Hospital Administration Management System (HAMS) to the Lightwave Health Information Management System (LHIMS) in 2021. The LHIMS is more user-responsive and thus minimizes data entry errors. Due to staffing shortages, the challenge of accurately diagnosing and reporting diseases in African, it can affect the reliability of kidney disease data [12]
The occurrence of kidney diseases has no age boundary but shows an upward trend as age increases [19]. In this study, patients aged 20-34 years are mostly affected by kidney diseases. In another study conducted in Jigawa State, Nigeria [20], it was reported that patients aged 21-30 are mostly affected by CKD. This study’s findings also corroborate those of Ahmed et al. (2018), who reported that kidney diseases have no age boundaries [21]. Young adults are exposed to many environmental risks at work. The dietary intake of heavy metals through contaminated food can lead to various non-communicable diseases. There are water bodies around the Ho Municipality, and the residents, especially young adults, are likely involved in swimming, drinking, and irrigation activities [15]. A growing trend of non-communicable disease, prevalent use of nephrotoxic medicines, human immunodeficiency virus infection, and obesity among young adults [15]. This is a great concern as young people are the cream of any nation.
Ho Municipality Teaching Hospital is the only hospital in the district with a dialysis machine, and 50.6% of the kidney diseases reported benefited from the dialysis services. The reason could be that most of the patients had no indication of dialysis or could not afford the cost involved, and left the hospital against medical advice and opted to seek medication elsewhere, probably traditional medicine. Kidney disease care and management inequalities are aggravated by structural deficiencies in low-resource settings like Ho Municipality. Such as infrastructure and equipment gap, financial barrier, human resource deficiency, cultural and educational barriers [22]. In another study, it was found that renal replacement therapy is scarce or not available in low and middle-income countries, where resources are limited, and there are inadequately trained health personnel. The study further stated that the annual cost of dialysis can exceed the gross domestic product income per capita and become a burden for the local health authorities, patients, and their families [23].
Diabetes mellitus and hypertension, as joint secondary diagnoses, contributed to 45.6% of kidney disease cases. This is in line with the large-scale population-based cohort study among diabetics and non-diabetics [24]. It was reported that progression to CKD is faster among diabetic patients than among non-diabetics. In another study, it was reported that the probability of developing CKD is three times higher among hypertensive patients [25]. Emerging research on systemic factors has found that sleeping disorders may influence cardiovascular health, such as hypertensive renal disease [26]. We encourage future research in this area to support this claim further.
Given the increased risk of kidney disease in people living with Diabetes mellitus and hypertension, it is important to employ comprehensive screening and monitoring strategies. The management of Non-Communicable Disease (NCD) can be influenced by many factors such as education level, residential location, and healthcare literacy. Thus, a multidisciplinary care approach can help with better management. This includes health education, nurse management, NCD clinics that provide integrated, comprehensive care, enhanced access to health insurance, and electronic medical record‐based strategies to target patients at high risk of complications [27]. The clinical conditions of kidney diseases from 2017 to 2020 were unavailable; therefore, only the cases reported in 2021 were classified and analyzed according to clinical circumstances. A five-year analysis of the clinical spectrum will give clearer insights than a one-year analysis. However, a one-year analysis can still offer an indication of the situation. There could be double-counting of the number of cases reported as per the patient’s visit. This could potentially misguide public health actions amid data quality issues. Despite these limitations, the study findings can guide the Ghana Health Services in developing policies and implementing public health measures to reduce the burden of kidney diseases. The increasing burden of kidney diseases will have huge implications on the health systems through increased budgets, demand for dialysis and specialised care, and could have a greater burden on health infrastructure.
Kidney diseases are higher among females than males. There is an increasing trend of kidney diseases in Ho Municipality from 2018 to 2021. Diabetic mellitus renal disease, pyelonephritis, and hypertensive renal disease are the three most common clinical conditions associated with kidney diseases in the district. The Ministry of Health should strengthen diabetes and hypertension prevention programs to reduce the burden of kidney diseases. Women should be supported during pregnancy to reduce pregnancy complications that might trigger kidney diseases. Understanding kidney disease and its health literacy, which was the theme of World Kidney Day 2022, can determine the outcomes for people affected by kidney disease. The Director of Public Health should raise awareness of the alarming rate of kidney-related diseases in the population, especially among young adults, and strategize mechanisms to reduce the burden.
What is already known about the topic
What this study adds
Delia Bandoh is an Associate Editor at the Journal of Interventional Epidemiology and Public Health (JIEPH) and a co-author of this manuscript. In line with the journal’s conflict of interest policy, she was fully recused from the peer review process and had no involvement in editorial handling or decision-making for this submission. An independent editor oversaw the review and decision-making process. The other authors declare that they have no competing interests.
We acknowledge the Ghana Field Epidemiology and Laboratory Training Program and the Ghana Health Services for their immense support during the data collection process. Special thanks go to the Regional Health Directorate, Volta Region, and the District Health Management of Ho Municipality, Ghana, for permitting us to conduct surveillance data analysis in Ho District.
Conceptualization: BK & AA
Data Collection: BK, SJ, MB, & LM
Methodology: BK & AA
Formal analysis: BK & AA
Resources: B. K, AA, SJ, MB, LM, DA, NL, DB & E. K
Supervision: AA, DA, NL, DB & EK
Writing – original draft: BK
Writing – review & editing: BK, AA, SJ, MB, LM, DA, NL, DB & EK
Manuscript writing: BK
| Kidney Diseases | Frequency (n=885) | Percentage (%) |
|---|---|---|
| Diabetic kidney disease | 328 | 37.1 |
| Pyelonephritis | 103 | 11.6 |
| Hypertensive renal diseases | 97 | 11.0 |
| Nephrotic syndrome | 61 | 6.9 |
| Chronic kidney disease, unspecified | 49 | 5.5 |
| Nonobstructive reflux-associated chronic pyelonephritis | 33 | 3.7 |
| Unspecified renal colic | 29 | 3.3 |
| Calculus of the kidney | 27 | 3.1 |
| Acute Renal Failure | 24 | 2.7 |
| Acute tubulointerstitial nephritis | 23 | 2.6 |
| Chronic kidney disease, stage 5 | 21 | 2.4 |
| End-stage renal disease | 14 | 1.6 |
| Chronic kidney disease, stage 4 | 13 | 1.5 |
| Unspecified hydronephrosis | 13 | 1.5 |
| Chronic kidney disease, stage 2 | 11 | 1.2 |
| Chronic obstructive pyelonephritis | 9 | 1.0 |
| Polycystic kidney | 8 | 0.9 |
| Chronic kidney disease, stage 3 | 6 | 0.7 |
| Hydronephrosis with ureteropelvic junction obstruction | 6 | 0.7 |
| Chronic kidney disease, stage 1 | 4 | 0.5 |
| Cyst of the kidney | 3 | 0.3 |
| Hydronephrosis with renal and ureteral calculous obstruction | 3 | 0.3 |