Research | Open Access | Volume 9 (2): Article 97 | Published: 10 Jun 2026

Views: 1,194
Menu, Tables and Figures
| Characteristic | Number (%) |
|---|---|
| Gender | |
| Male | 23 (76.7) |
| Female | 7 (23.3) |
| Median Age in Years (IQR) | 30 (28 – 32) |
| Work Experience | |
| Median Years of Work Experience (IQR) | 2 (1 – 4) |
| Employer | |
| MoH – Tanzania Mainland | 25 (83.3) |
| MoH – Zanzibar | 5 (16.7) |
| Pre-test Mean Knowledge Score (SD) | Post-test Mean Knowledge Score (SD) | Difference in Mean Knowledge Scores (95% CI) | Percentage (%) Improvement | P values | |
|---|---|---|---|---|---|
| Workshop 1 | 54.23 (10.02) | 71.63 (11.03) | 17.40 (12.72, 22.08) | 32.08 | <0.001 |
| Workshop 2 | 54.05 (9.16) | 69.30 (8.59) | 15.25 (11.03, 19.47) | 28.21 | <0.001 |
| Workshop | Skill | Before Training Mean Skill Level (SD) | After Training Mean Skill Level (SD) | Difference in Mean Skill Level (95% CI) | Percentage (%) Improvement | P values |
|---|---|---|---|---|---|---|
| Workshop 1 | Collecting surveillance data | 2.06 (0.57) | 2.87 (0.43) | 0.81 (0.55, 1.07) | 39.32 | <0.001 |
| Applying case definitions | 2.30 (0.64) | 2.90 (0.30) | 0.60 (0.34, 0.85) | 26.08 | <0.001 | |
| Creating a line list | 2.16 (0.64) | 2.90 (0.30) | 0.74 (0.48, 0.99) | 34.26 | <0.001 | |
| Data cleaning | 1.93 (0.62) | 2.83 (0.37) | 0.90 (0.63, 1.16) | 46.63 | <0.001 | |
| Summarising data | 1.83 (0.68) | 2.90 (0.30) | 1.07 (0.79, 1.34) | 58.47 | <0.001 | |
| Displaying data | 1.56 (0.56) | 2.80 (0.40) | 1.24 (0.98, 1.49) | 79.48 | <0.001 | |
| Interpreting data | 1.56 (0.56) | 2.73 (0.51) | 1.17 (0.89, 1.44) | 75.00 | <0.001 | |
| Communicating information | 1.56 (0.56) | 2.83 (0.45) | 1.27 (1.00, 1.53) | 81.41 | <0.001 | |
| Case investigation | 1.60 (0.66) | 2.80 (0.47) | 1.20 (0.90, 1.49) | 75.00 | <0.001 | |
| Excel | 1.46 (0.56) | 2.76 (0.49) | 1.30 (1.02, 1.57) | 89.04 | <0.001 | |
| PoPCAB | 1.50 (0.56) | 2.76 (0.49) | 1.26 (0.98, 1.53) | 84.00 | <0.001 | |
| Workshop 2 | Identifying an outbreak | 1.83 (0.52) | 2.93 (0.25) | 1.10 (0.89, 1.31) | 60.11 | <0.001 |
| Descriptive steps of an OI | 1.40 (0.61) | 2.86 (0.34) | 1.46 (1.20, 1.72) | 104.29 | <0.001 | |
| Analytical steps of an OI | 1.23 (0.49) | 2.63 (0.60) | 1.40 (1.11, 1.68) | 113.82 | <0.001 | |
| Response steps of an OI | 1.53 (0.80) | 2.80 (0.40) | 1.27 (0.94, 1.59) | 83.00 | <0.001 | |
| Problem analysis | 1.26 (0.51) | 2.86 (0.34) | 1.60 (1.37, 1.82) | 126.98 | <0.001 | |
| Linking with laboratory | 1.96 (0.65) | 2.80 (0.40) | 0.84 (0.56, 1.11) | 42.86 | <0.001 | |
| Developing a presentation | 2.06 (0.57) | 2.76 (0.42) | 0.70 (0.44, 0.96) | 33.98 | <0.001 | |
| PowerPoint | 2.30 (0.52) | 2.90 (0.30) | 0.60 (0.38, 0.82) | 26.09 | <0.001 | |
| IHR Core Capacities Assessment | 1.96 (0.55) | 2.80 (0.40) | 0.84 (0.59, 1.08) | 42.86 | <0.001 | |
| Contingency Plan | 1.87 (0.61) | 2.86 (0.34) | 0.99 (0.73, 1.24) | 52.94 | <0.001 | |
| Workshop 3 | Developing a presentation | 2.00 (0.36) | 2.96 (0.18) | 0.96 (0.81, 1.11) | 48.00 | <0.001 |
| Giving a presentation | 1.86 (0.43) | 2.93 (0.25) | 1.07 (0.89, 1.25) | 57.53 | <0.001 | |
| Creating Maps using QGIS | 1.40 (0.75) | 2.90 (0.30) | 1.50 (1.20, 1.79) | 107.14 | <0.001 |
Ally Kassim Hussein1,2,3,4,&, Nsiande Andrew Lema1,2,4, Devotha Leonard1,5, Loveness John Urio1,2,4, Nelson Edwin Malugu1,4,5, Rogath Saika Kishimba1,3,4,6, Azma Ayoub Simba1,4, Vida Makundi Mmbaga1,4,6, Nisalile Mwangoka4,6, Remidius Kakulu4,6, Elias Bukundi3,4, Ruth Jonathan4,7, Mucho Mizinduko3, Mohamed Ally Mohamed4,8
1Tanzania Field Epidemiology and Laboratory Training Program, Dar es Salaam, United Republic of Tanzania, 2African Field Epidemiology Network, Dar es Salaam, United Republic of Tanzania, 3Muhimbili University of Health and Allied Sciences, Dar es Salaam, United Republic of Tanzania, 4Tanzania Field and Laboratory Epidemiologists Association, Dar es Salaam, United Republic of Tanzania, 5Centre of Excellence in Health Monitoring & Evaluation, Mzumbe University, Morogoro, United Republic of Tanzania, 6Ministry of Health, Dodoma, United Republic of Tanzania, 7Lugalo Military Hospital, Dar es Salaam, United Republic of Tanzania, 8East, Central and Southern Africa Health Community, Arusha, United Republic of Tanzania
&Corresponding author: Ally Kassim Hussein, Tanzania Field Epidemiology and Laboratory Training Program, Dar es Salaam, United Republic of Tanzania, Email: allykhussein@gmail.com, ORCID: https://orcid.org/0000-0002-6674-7487
Received: 18 Jun 2025, Accepted: 10 Jun 2026, Published: 10 Jun 2026
Domain: Field Epidemiology
Keywords: Health workforce development, point of entry, field epidemiology, global health security
©Ally Kassim Hussein et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Ally Kassim Hussein et al., Strengthening public health surveillance at points of entry: A Tanzanian case study of FETP-Frontline adaptation. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):97. https://doi.org/10.37432/jieph-d-25-00143
Introduction: In an increasingly interconnected world with rising global health risks, the competence of Point of Entry (PoE) staff in epidemiology is essential for timely detection and response to public health threats. This study describes the adaptation of the Field Epidemiology Training Program (FETP)-Frontline curriculum for PoE staff in Tanzania and assesses the performance of the first cohort that completed the training.
Methods: We conducted a workshop to review and adapt FETP-Frontline training materials for relevance to port health functions. A total of 30 PoE staff were recruited and trained from April to August 2023. Participants underwent knowledge assessments before and after the first two workshops. We used paired sample t-tests to compare changes in mean knowledge scores. Self-assessed skill levels were also collected after each workshop to evaluate perceived improvements in competencies.
Results: The adapted curriculum retained the standard three-workshop FETP-Frontline structure, with contextualised enhancements for PoE operations. Workshop 1 included a session on Population Connectivity Across Borders (PoPCAB). Workshop 2 incorporated International Health Regulations Core Capacities assessments at PoEs, Risk Assessments, and Contingency Planning. Workshop 3 included training on geographic information system (QGIS) mapping. Of the 30 trained PoE staff from 25 different PoEs across Tanzania, 76.7% (n=23) were male, with a median age of 30 years (interquartile range: 28-32). There were significant increases in the mean knowledge scores after both Workshops 1 and 2. Mean knowledge scores increased by 17.4 (95% confidence interval (CI): 12.72 – 22.08) and 15.25 (95%CI: 11.03 – 19.47) points after Workshops 1 and 2, respectively. There were significant increases in all trainee self-assessed skills after all three workshops.
Conclusion: The adapted FETP-Frontline curriculum was associated with improved knowledge and self-reported skills among PoE surveillance officers in Tanzania. This context-specific adaptation demonstrates the feasibility of strengthening surveillance capacity at Points of Entry. Scaling up the training to include all PoE personnel may further enhance national preparedness for cross-border public health threats.
Global health security is of paramount concern in today’s interconnected society. International collaboration and steadfast adherence to the International Health Regulations (IHR) are essential for the management of public health concerns and the prevention of infectious diseases [1]. Efficient operation of Points of Entry (PoEs) is crucial to maintaining global health security, as they are the front lines in our defence against potential health crises [2]. The cornerstone of these efforts is vigilant and comprehensive surveillance, meticulous screening procedures, and seamless international cooperation [1,3].
An essential element of this endeavour involves enhancing the capacities of surveillance officers stationed at these PoEs [4,5]. These dedicated professionals play a pivotal role in early detection, rapid response, and effective management of health threats. Their training and expertise are the cornerstone in ensuring that PoEs function as robust barriers against the international spread of diseases [5,6]. Thus, investing in the knowledge and skills of surveillance officers is not only essential but also represents a pivotal obligation in strengthening global health security.
The Field Epidemiology Training Program-Frontline (FETP-Frontline) course is a three-month mentored workforce development initiative designed to enhance the epidemiological knowledge, skills, and competencies of Ministry of Health (MoH) workers in the country. This program effectively blends training and practical service, aiming to strengthen the MoH’s ability to tackle public health priorities and improve overall public health capacities. Specifically, it bolsters epidemiological capabilities at the district level within the healthcare system, equipping staff with the essential skills to detect, investigate, and respond to diseases and other public health events of international significance [7].
In Tanzania, the FETP-Frontline commenced in 2015, providing training to individuals in all districts, primarily focusing on Integrated Disease Surveillance and Response (IDSR) focal persons and vaccination focal persons [8]. Given the increasing global health risks and emerging diseases, it has become crucial for PoE staff to possess epidemiological knowledge and skills [6].
Despite the demonstrated effectiveness of the standard FETP-Frontline curriculum in strengthening surveillance capacity at district and facility levels, it is not specifically tailored to the operational context of PoE. Surveillance officers at PoEs operate in a unique environment characterized by cross-border population movement, international travel regulations, and the need for rapid coordination across sectors. Key competencies such as risk assessment at borders, assessment of IHR core capacities at designated PoEs, and analysis of population mobility patterns are not explicitly emphasized in the standard curriculum.
To our knowledge, no published study has documented the systematic adaptation and implementation of the FETP-Frontline curriculum specifically for PoE staff. This gap underscores the need for context-specific training approaches to strengthen surveillance at these critical points. This article describes the adaptation of the FETP-Frontline curriculum to align with the specific requirements of surveillance officers stationed at PoEs in Tanzania. Furthermore, we present an overview of the performance of the first cohort comprising 30 trainees who completed this adapted training program.
Adaptation of the FETP-Frontline Curriculum
Since 2021, Muhimbili University of Health and Allied Sciences (MUHAS) has been the host for the FETP-Frontline. This program is conducted in collaboration with the Ministry of Health (MoH) and the U.S. Centres for Disease Control and Prevention (CDC). Upon successful completion of the training, trainees are awarded a short course certificate, which is equivalent to 144 continuous professional development points (CPD).
We conducted a workshop from 21st to 26th March 2023 at MUHAS in Dar es Salaam to review and enhance the existing FETP-Frontline curriculum by integrating PoE-specific concepts. The workshop brought together a diverse group of participants, including technical staff from the East, Central, and Southern Africa Health Community (ECSA-HC), the Ministry of Health’s Port Health Section and Department of Human Resource Development, Tanzania FELTP staff under the African Field Epidemiology Network (AFENET), Mzumbe University (MU), and MUHAS faculty who are engaged in facilitating the three tiers of FETP training (Advanced, Intermediate and Frontline).
We reviewed various FETP-Frontline training materials, including curricula, timetables, slides, field assignments, pre/post-tests and case studies. In addition to these resources, several other documents were presented and discussed. These included IHR core capacities assessment tools [9], a risk assessment presentation developed by WHO, a presentation by the MoH-PoE section, contingency plans, and the Population Connectivity Across Borders (PoPCAB) toolkit [10].
The adaptation process focused on aligning the standard FETP-Frontline competencies with the functional roles of PoE surveillance officers. Key gaps identified in the standard curriculum included limited emphasis on cross-border surveillance, population mobility analysis, PoE-specific risk assessment, and assessment of IHR core capacities at designated entry points.
To address these gaps, selected modules were refined and contextualized to reflect PoE-specific functions, while additional content was incorporated into the training. To accommodate the new material without compromising the depth of existing content, the duration of each of the three workshops was extended by one day. This approach ensured that the core structure and learning objectives of the standard FETP-Frontline curriculum were maintained while allowing for the inclusion of PoE-relevant competencies.
Design, population and setting
We utilised a quasi-experimental design, specifically a pre-post study, to assess and compare the trainees’ knowledge before and after completing the training. The recruitment of trainees occurred in collaboration with the MoH Port Health Section two weeks prior to the training’s commencement. Port Health Staff are environmental health officers who are responsible for the screening of travellers, the collection and review of surveillance information, and the provision of public health emergency response measures in collaboration with other relevant agencies. Effective communication with District and Regional Medical Officers, together with the MoH, for timely notification of any emergency situation is a key function. Additionally, PoE staff are tasked with inspecting and clearing conveyances, verifying certificates, and tracking and reporting the status of travellers to local medical institutions, particularly in cases involving isolation or other health facility arrangements. They also play a crucial role in inspecting and certifying the import and export of human remains, as well as inspecting deceased bodies.
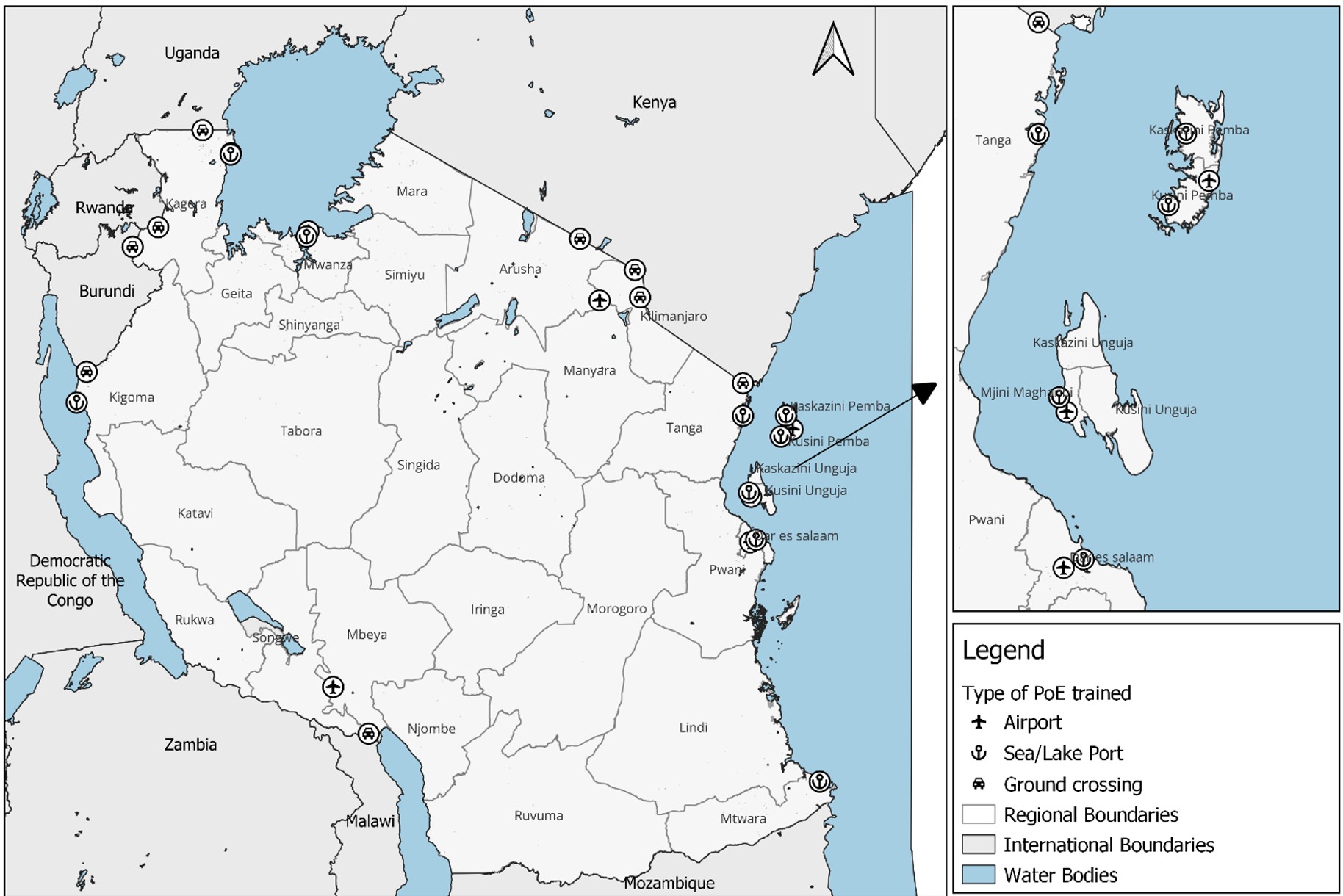
Tanzania shares its borders with Kenya and Uganda to the north, Rwanda, Burundi and the Democratic Republic of the Congo to the west, and Zambia, Malawi and Mozambique to the south. Tanzania has a total of sixty-two PoEs, with fifty-four located in Tanzania Mainland and eight in Zanzibar. Among these, thirteen PoEs are designated, with eleven in Tanzania Mainland and two in Zanzibar. The total number of Port Health Staff was four hundred and seventy, with three hundred and forty-three in Tanzania Mainland and one hundred and twenty-seven in Zanzibar. We purposively recruited 30 trainees from high risk/high volume PoEs, specifically targeting port health staff responsible for surveillance and data management. Trainees were selected from different types of PoEs, including airports, sea/lake ports and ground crossings, to ensure representation of diverse operational contexts.
Data collection
To assess knowledge gained in alignment with Level 2 of the Kirkpatrick Evaluation Model, we administered structured knowledge tests before and after course completion during workshops 1 and 2. The tests included questions that aligned with the course learning objectives, and trainees were given 30 minutes to complete each test. In addition, trainees conducted a self-assessment of their surveillance and data analysis skills before and after the FETP-Frontline training, using a three-point scale (1 = not skilled, 2 = somewhat skilled, 3 = capable). Workshops 1, 2, and 3 were conducted on 12th -19th April, 5th -11th June, and 15th -19th August 2023, respectively.
Data analysis
We summarised data using means and proportions and assessed changes in mean scores in the pre-tests and post-tests from workshops 1 and 2 using a paired sample t-test (significance level set at P< 0.05). We also assessed mean changes in self -assessed levels of skills pre and post the training using a t-test. Maps showing Tanzania’s PoEs and locations where trainees were recruited from were drawn using QGIS Desktop 3.28.7 (QGIS Development Team, Switzerland). Information on the points of entry were obtained from the Tanzania Ministry of Home Affairs – Immigration Services Department (Tanzania Ministry of Home Affairs Immigration), and geographic coordinates were sourced from Google Maps (https://www.google.com/maps/). All shapefiles used are from openly available sources (Tanzania Shape Files) and (Africa Metadata).
Ethical consideration
The study was considered exempt from requiring IRB approval because it involved the analysis of routine programmatic data and scores from individuals participating in a government training program in their official roles. No personal identifiers were utilised or disclosed.
FETP-Frontline curriculum specific for PoE staff
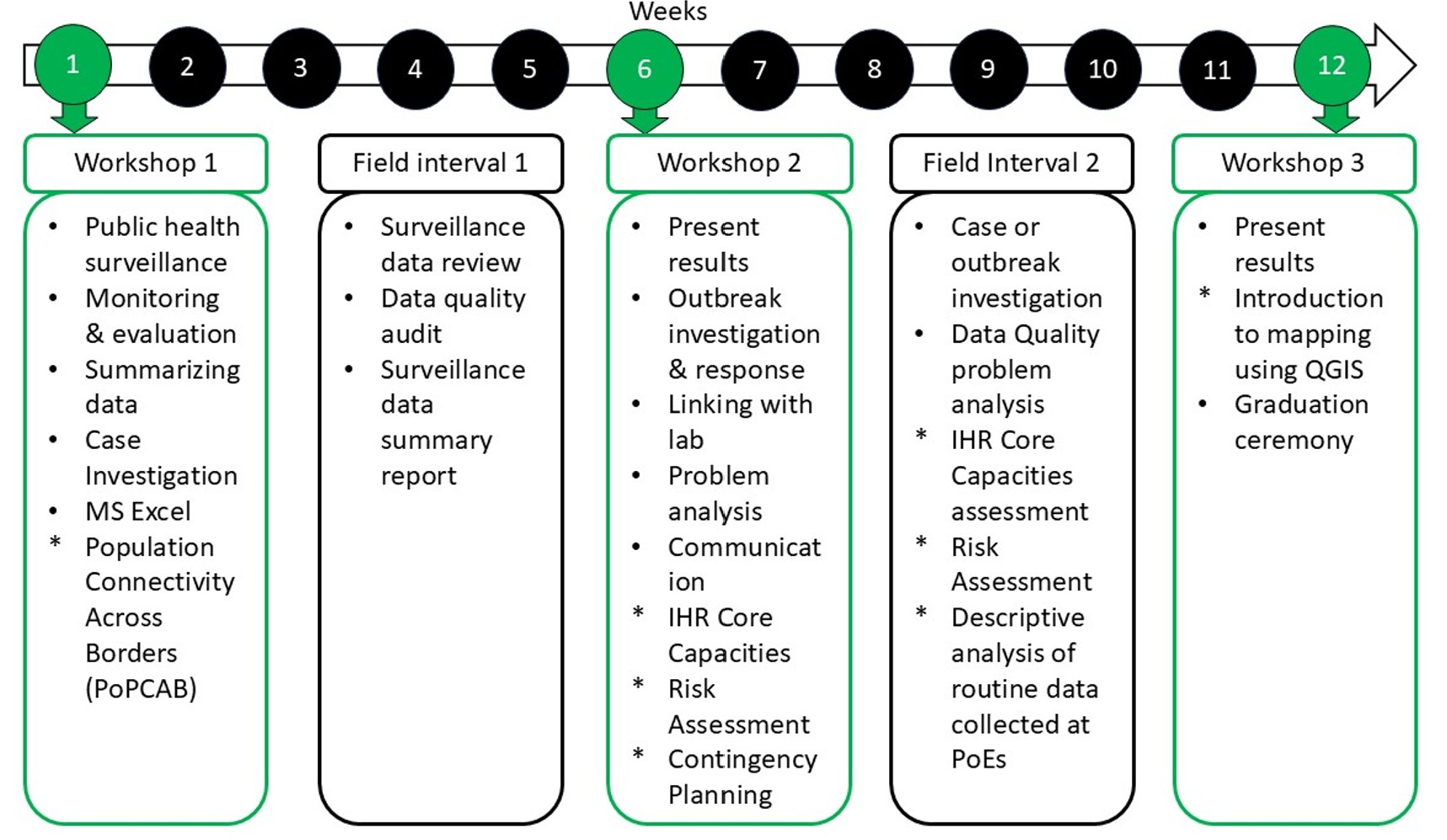
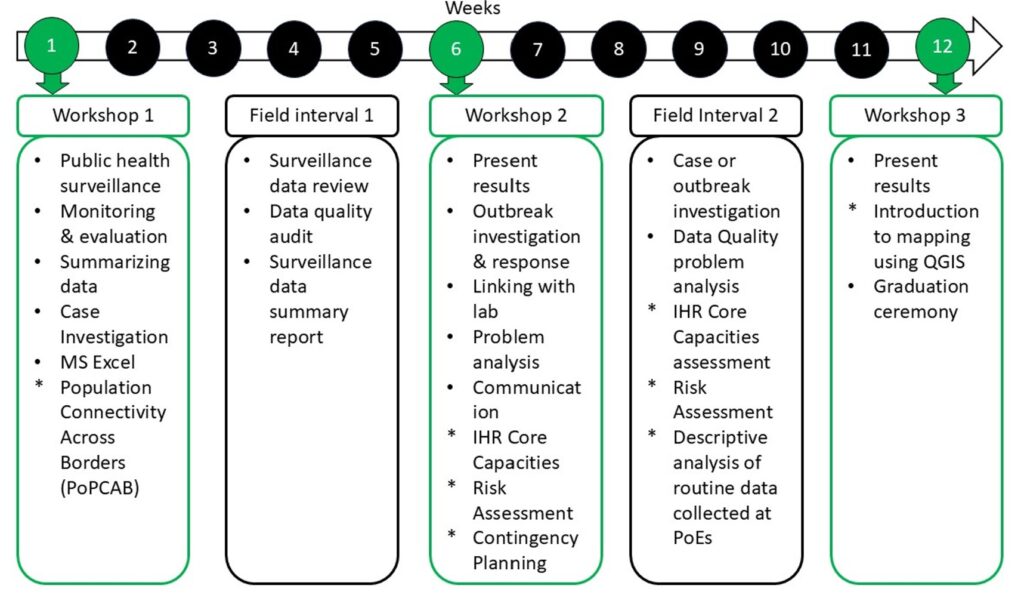
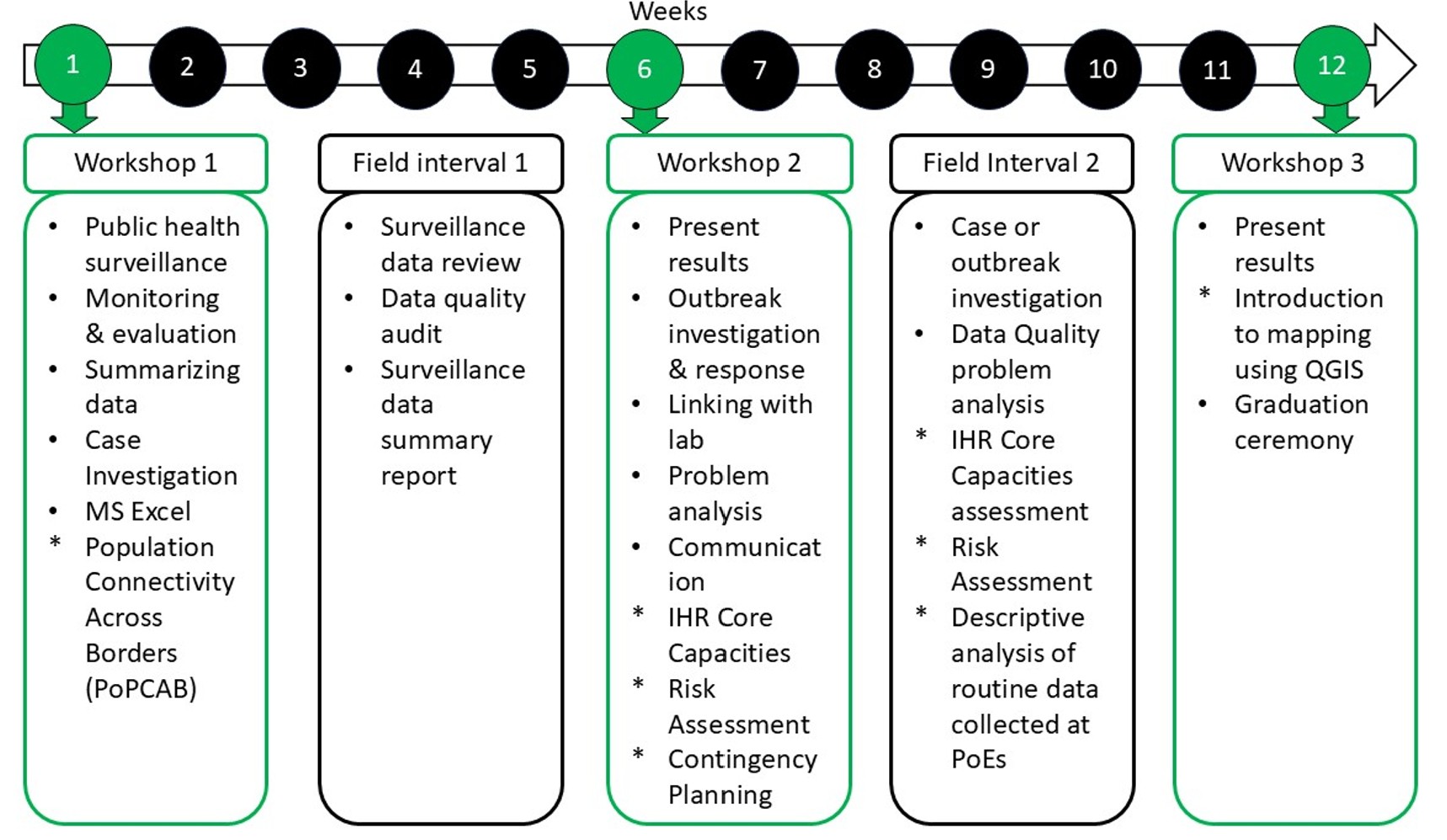
The adapted FETP-Frontline program for PoE Staff spans approximately three months, comprising three one-week classroom sessions (workshops) and around nine weeks of field assignments. Each of the three workshops was extended by one additional day to accommodate the integration of PoE-specific content while maintaining the structure and core learning objectives of the standard FETP-Frontline curriculum. In the final workshop, trainees are required to demonstrate their acquired skills by presenting outputs from their field assignments.
The curriculum largely adhered to the structure and content of the standard FETP-Frontline curriculum version 2.0 [11]. However, targeted adaptations were introduced to reflect PoE-specific functions. In Workshop 1, we introduced a session on Population Connectivity Across Borders (PoPCAB). Workshop 2 integrated IHR Core Capacities assessments at PoEs, Risk Assessments, and Contingency Planning. Workshop 3 included training on geographic information system (QGIS) mapping. Figure 1 shows the FETP-Frontline (PoE Specific) structure/timeline by weeks.
Following the completion of Workshops 1 and 2, there is a Field Interval that spans 4 to 6 weeks. During this period, trainees return to their regular full-time job responsibilities. Despite the demands of their everyday work, trainees are expected to make time for essential field activities. To facilitate this, each participant is paired with a mentor who provides guidance and support as needed, ensuring the successful completion of the assignments.
Trainee recruitment and completion
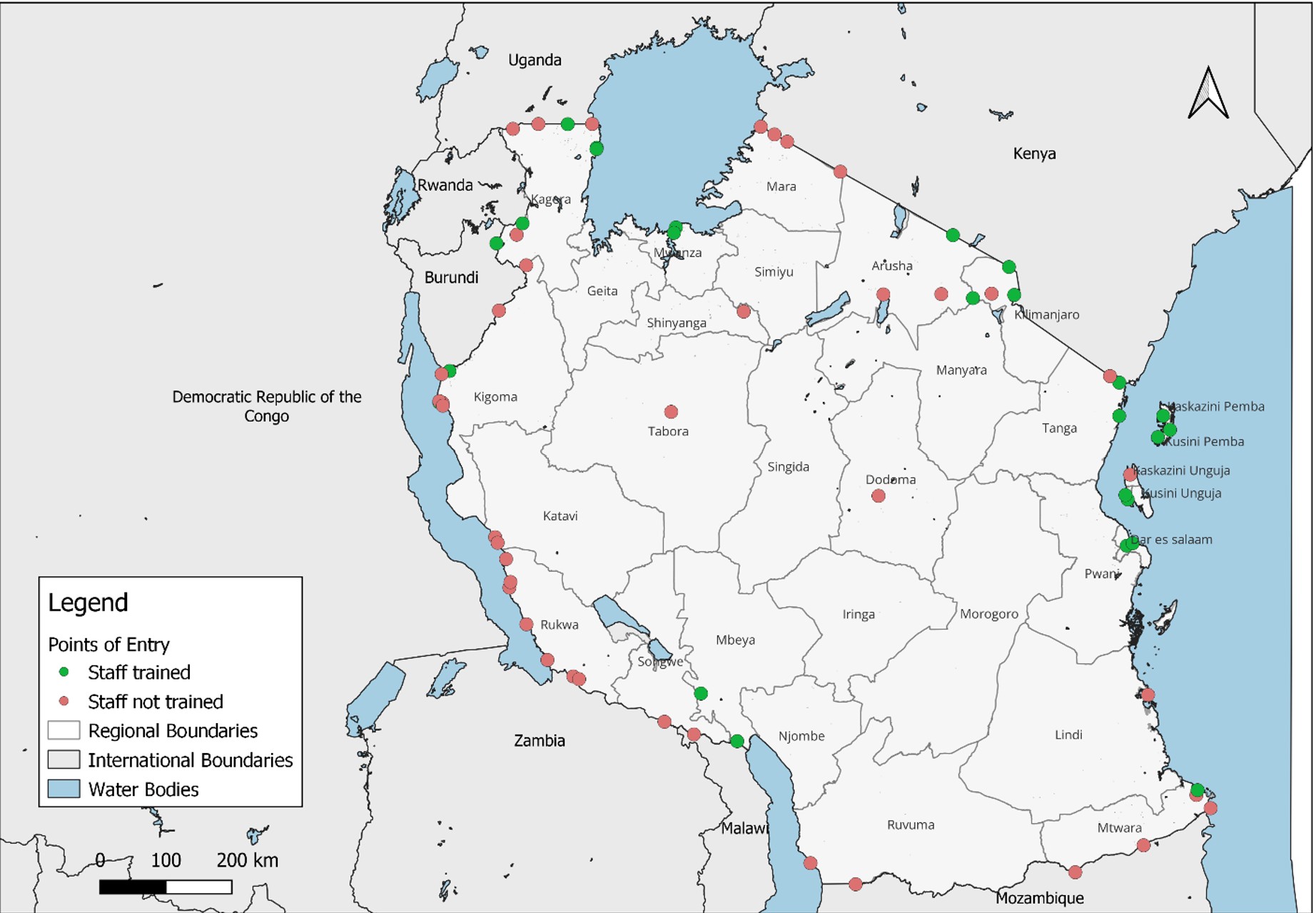
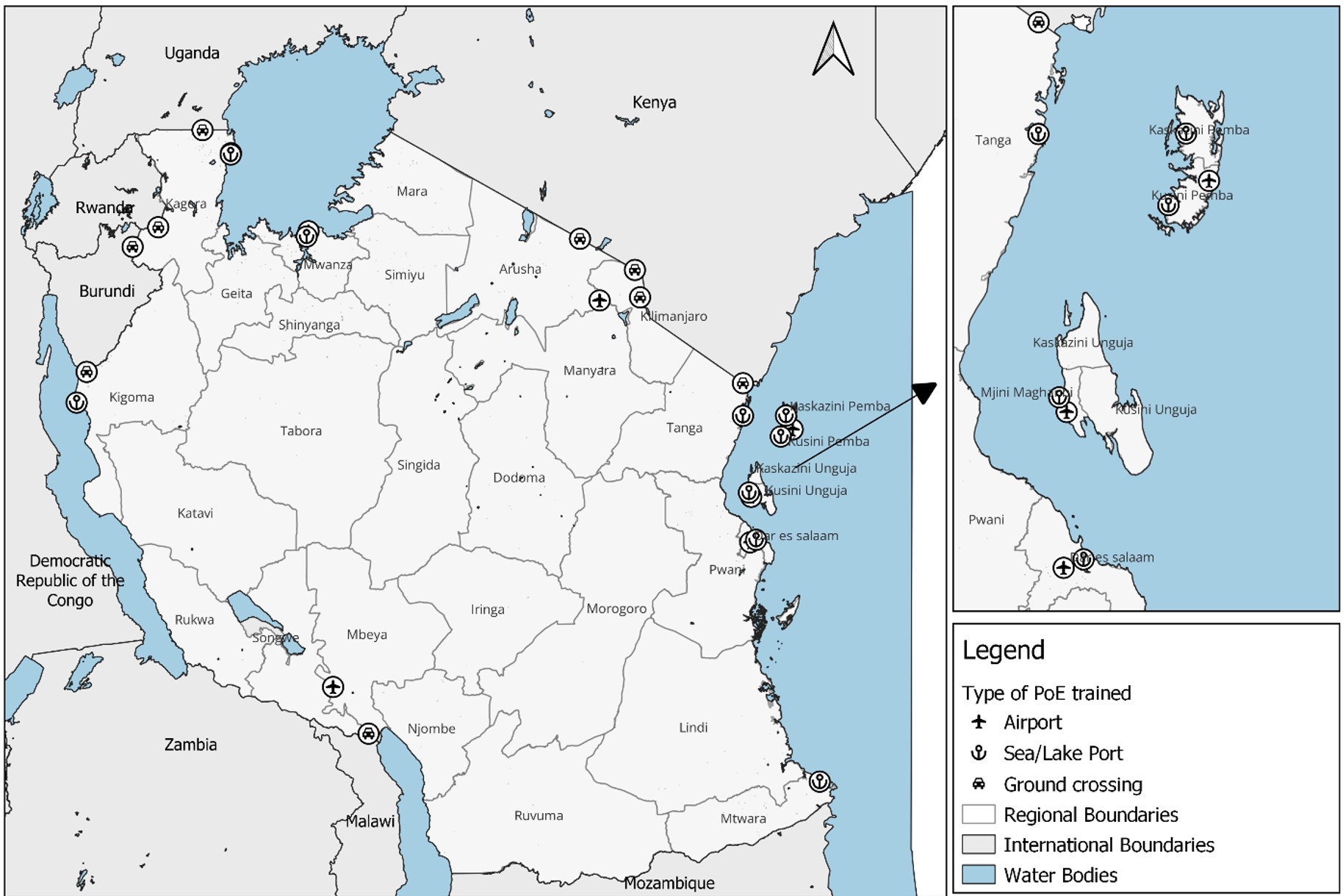
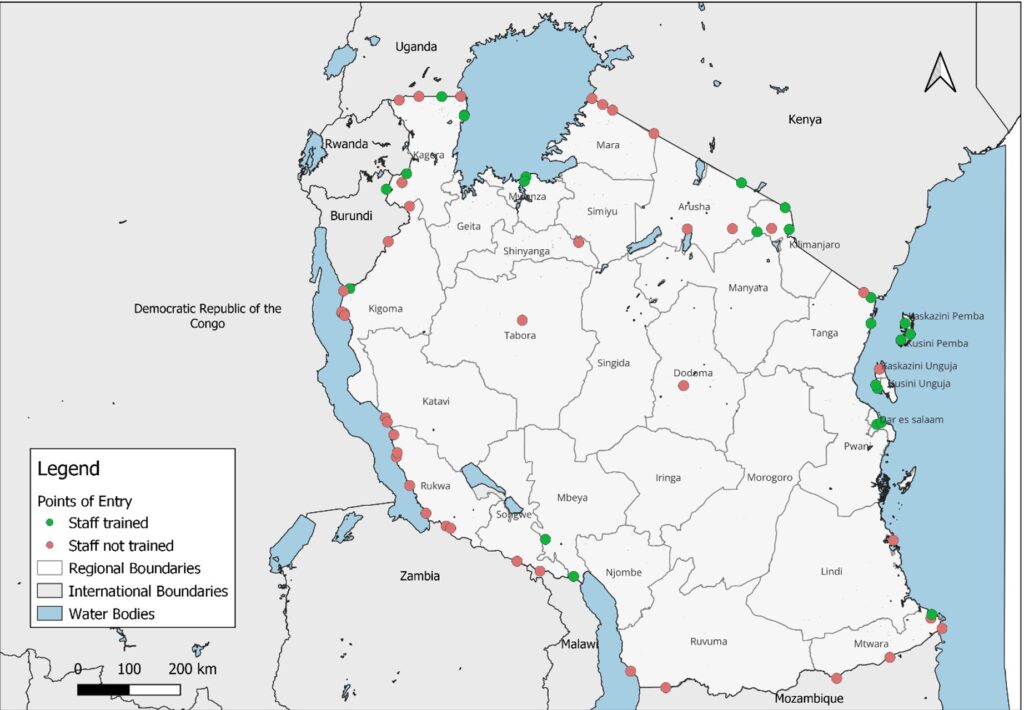
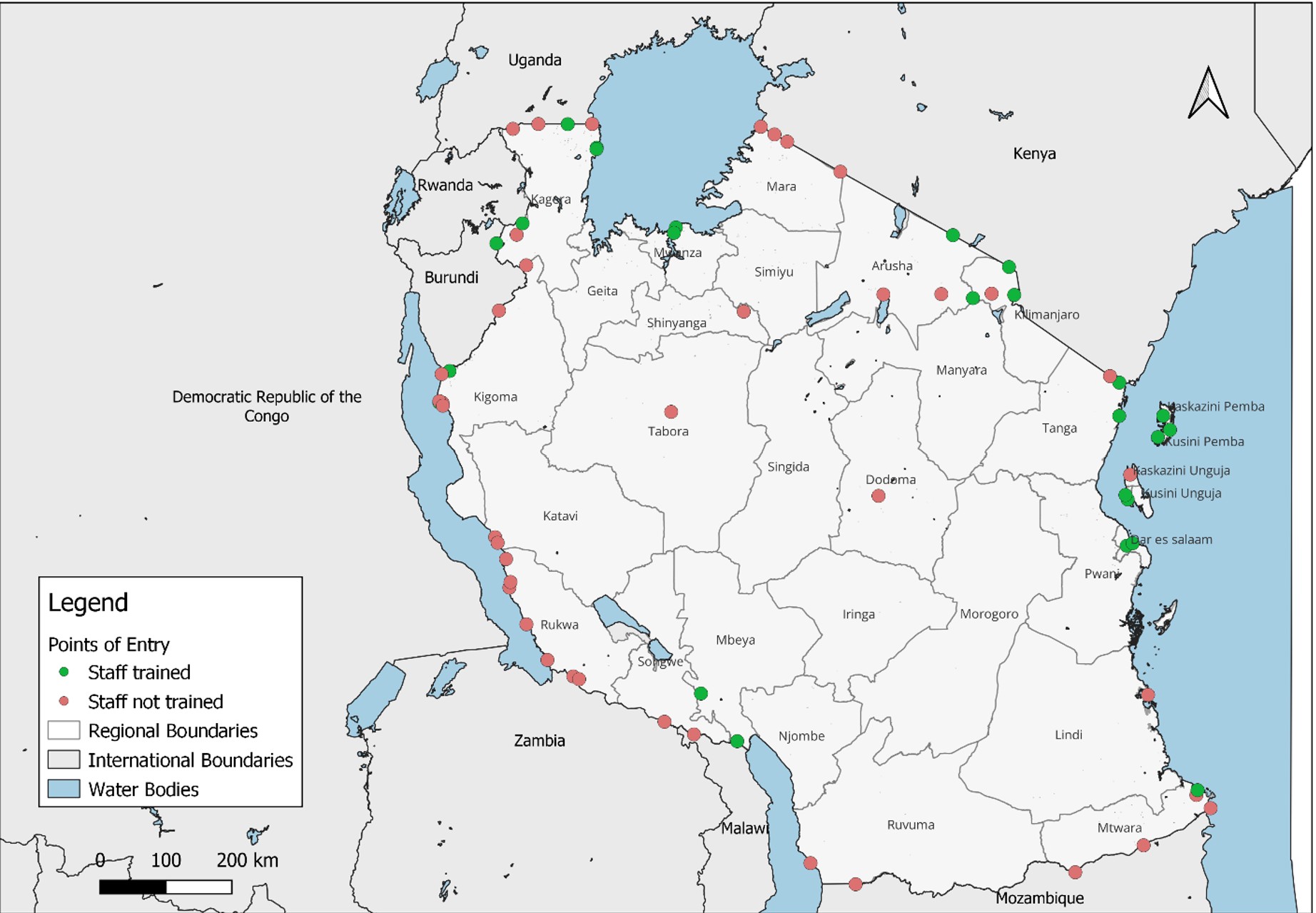
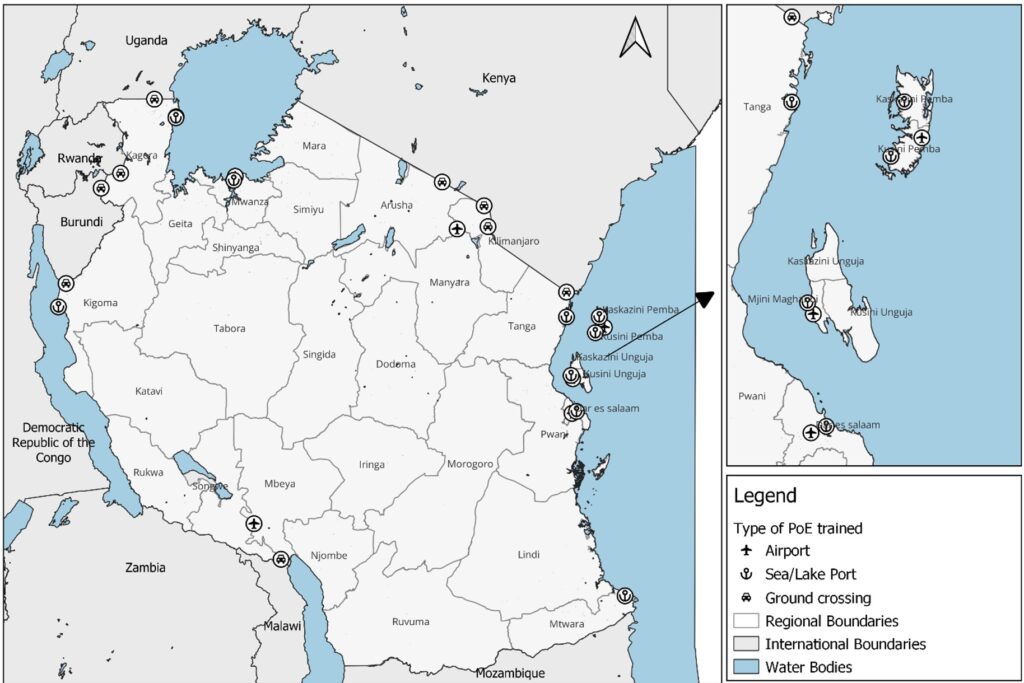
Thirty Port Health Staff were recruited from 25 PoEs for the training (Table 1). The trainees were selected from 9 airports, 9 sea/lake ports and 7 ground crossings. Most of the trainees were male (n=23, 76.7%). All trainees were environmental health officers (n=30, 100.0%). Workshops 1, 2, and 3 were conducted on 12th -19th April, 5th -11th June, and 15th -19th August, respectively. All 30 trainees attended all sessions and completed all required assignments. Figure 2 shows the distribution of Tanzania’s PoEs categorised by their training status. Figure 3 shows the distribution of PoEs selected for FETP-Frontline training categorised by type.
Changes in trainees’ knowledge
There were significant increases in trainees’ mean knowledge test scores after both Workshops 1 and 2. Mean knowledge test scores increased by 17.4 (95% Confidence Interval (CI): 12.72 – 22.08) and 15.25 (95%CI: 11.03 – 19.47) points after Workshops 1 and 2, respectively (Table 2).
Changes in trainees’ self-assessed skills
There were significant increases in all trainee self-assessed skills after all three workshops (Table 3). Trainees’ self-assessed skill levels in the descriptive and analytical steps of outbreak investigation, problem analysis, and creating maps using QGIS more than doubled.
Application of skills during field assignments
During the field intervals, trainees applied the skills acquired during the workshops in their respective PoEs. These activities included conducting PoE assessments using IHR core capacity tools, performing basic risk assessments for public health events, and mapping PoE locations, nearby health facilities and surrounding catchment areas using QGIS. In addition, trainees utilised concepts from the PoPCAB toolkit to better understand movement patterns and identify potential cross-border disease transmission risk.
We introduced targeted modifications to the FETP-Frontline curriculum to better align it with the roles and responsibilities of surveillance officers stationed at Points of Entry (PoEs) in Tanzania. We then described the implementation of the revised curriculum by presenting an overview of the trained cohort, including their professional background, the extent of PoE coverage achieved, and their knowledge levels before and after the training. The results demonstrated a notable improvement in trainees’ knowledge and self-reported skills, suggesting that the adapted curriculum addressed important gaps in the training of PoE staff.
These modifications are particularly relevant given the distinct operational context of PoE surveillance. Unlike district and health facility-based surveillance systems, PoEs require competencies related to cross-border population movement, international travel regulations, and rapid multi-sectoral coordination. Since the initiation of FETP-Frontline in Tanzania in 2015, the MoH has used a standardised curriculum for all frontline surveillance personnel. The revised curriculum builds on this foundation by incorporating content tailored to the specific functions and challenges of PoE surveillance.
The FETP-Frontline curriculum developed by the U.S. Centres for Disease Control and Prevention (CDC) is intentionally flexible, allowing programs to adapt it to their national contexts [11]. Several countries have leveraged this flexibility to address local priorities; for example, Kenya has adapted the program for malaria-specific surveillance officers [12], countries in Central America have implemented regional customisations [13], and Guinea-Bissau has integrated Geographic Information System training into its workshops [14]. However, to our knowledge, no other country has documented the development and implementation of a curriculum specifically tailored for point-of-entry staff. Tanzania’s experience, therefore, provides a valuable model that other countries and programs can reference when seeking to strengthen capacity at PoEs through context-specific training interventions.
The evaluation of the PoE training applied Level 2 of the Kirkpatrick Evaluation Model, which focuses on measuring the extent of knowledge and skill acquisition following a learning intervention. This model has been widely used in evaluating FETP-Frontline and similar training programs globally [15,16]. The observed improvements in both knowledge test scores and self-reported skills are consistent with findings from other program evaluations [17,18]. These results further support the value of adapting training content to reflect the operational needs of specific public health roles.
In addition to improvements in knowledge and perceived competencies, trainees reported applying newly acquired skills during field assignments. These included conducting PoE assessments using IHR core capacity tools, performing basic risk assessments, and utilising population movement concepts to identify potential cross-border risks. These findings suggest that the adapted curriculum was relevant to the operational needs of PoE staff. However, this study did not assess whether these skills translated into sustained changes in surveillance practices or measurable improvements in system performance.
The demographic profile of the cohort revealed a notable gender disparity, with females comprising less than a quarter of the participants. This likely reflects broader gender disparities within the health workforce in Tanzania [19]. Similar patterns have been observed in other countries implementing FETP, where male trainees have also predominated in training cohorts [15,17,18]. Addressing this issue would require deliberate and sustained efforts, including gender sensitive recruitment policies and strategies aimed at encouraging and supporting more women to take on surveillance roles and in public health more broadly [20].
Recent public health events, including outbreaks of COVID-19, Mpox, Ebola, and Marburg virus disease, have underscored the critical role of PoEs in national and global disease surveillance systems. These events have tested the capacity of port health surveillance and highlighted the urgent need to strengthen frontline preparedness at borders. Enhancing the competencies of surveillance officers stationed at these strategic locations is vital for safeguarding global health security [6]. However, it is important to acknowledge that the training conducted as part of this initiative reached only a portion of the total PoE workforce. To achieve broader impact and ensure comprehensive preparedness, efforts must be made to scale up the training to include all remaining port health staff across the country.
This study has several limitations. First, the use of a pre-post study design without a comparison group limits the ability to attribute observed improvements solely to the training, as external factors or testing effects may have influenced the results. Second, the relatively short interval between assessments may have introduced recall bias and does not allow for evaluation of long-term knowledge retention. Third, the reliance on self-assessed skill measures introduces the possibility of social desirability bias and may not accurately reflect actual performance in field settings. Although knowledge assessments provided an objective measure of learning, they do not capture behavioural change or real-world application.
In addition, the sample size was relatively small and purposively selected from high-volume PoEs, which may limit the generalizability of the findings. The evaluation was also limited to Level 2 of the Kirkpatrick model and did not assess higher-level outcomes such as changes in workplace behaviour or the impact of training on surveillance system performance. Future evaluations should incorporate additional approaches, including mentor assessments, workplace supervisor evaluations, and objective performance indicators, to better understand the impact of training on surveillance practices at PoEs.
Despite these limitations, the findings demonstrate that adapting the FETP-Frontline curriculum to the PoE context is feasible and associated with improvements in key competencies among surveillance officers. Given the critical role of PoEs in the detection and control of cross-border health threats, strengthening workforce capacity at these locations remains a priority for national and global health security.
The adaptation of the FETP-Frontline curriculum to the PoE context in Tanzania was associated with significant improvements in trainees’ knowledge and self-reported skills. By addressing context-specific competencies such as cross-border risk assessment, population mobility analysis, and IHR core capacity assessments, this approach provides a practical model for strengthening surveillance at Points of Entry.
However, further evaluation is needed to assess the extent to which these improvements translate into sustained changes in surveillance prctices and improved public health outcomes. Scaling up this adapted training, alongside strengthened monitoring of field performance, will be essential to enhance national and global health security.
What is already known about the topic
What this study adds
AKH: conceptualization, data curation, formal analysis, methodology, visualization, writing original draft, review and editing; NAL: conceptualization, data curation, formal analysis, methodology, review and editing; DL: data curation, formal analysis, methodology, writing original draft, review and editing; LJU: data curation, formal analysis, review and editing; NEM: data curation, formal analysis, review and editing; AAS: conceptualization, data curation, supervision, review and editing; VMM: conceptualization, data curation, review and editing; NM: conceptualization, data curation, review and editing.
| Characteristic | Number (%) |
|---|---|
| Gender | |
| Male | 23 (76.7) |
| Female | 7 (23.3) |
| Median Age in Years (IQR) | 30 (28 – 32) |
| Work Experience | |
| Median Years of Work Experience (IQR) | 2 (1 – 4) |
| Employer | |
| MoH – Tanzania Mainland | 25 (83.3) |
| MoH – Zanzibar | 5 (16.7) |
| Pre-test Mean Knowledge Score (SD) | Post-test Mean Knowledge Score (SD) | Difference in Mean Knowledge Scores (95% CI) | Percentage (%) Improvement | P values | |
|---|---|---|---|---|---|
| Workshop 1 | 54.23 (10.02) | 71.63 (11.03) | 17.40 (12.72, 22.08) | 32.08 | <0.001 |
| Workshop 2 | 54.05 (9.16) | 69.30 (8.59) | 15.25 (11.03, 19.47) | 28.21 | <0.001 |
| Workshop | Skill | Before Training Mean Skill Level (SD) | After Training Mean Skill Level (SD) | Difference in Mean Skill Level (95% CI) | Percentage (%) Improvement | P values |
|---|---|---|---|---|---|---|
| Workshop 1 | Collecting surveillance data | 2.06 (0.57) | 2.87 (0.43) | 0.81 (0.55, 1.07) | 39.32 | <0.001 |
| Applying case definitions | 2.30 (0.64) | 2.90 (0.30) | 0.60 (0.34, 0.85) | 26.08 | <0.001 | |
| Creating a line list | 2.16 (0.64) | 2.90 (0.30) | 0.74 (0.48, 0.99) | 34.26 | <0.001 | |
| Data cleaning | 1.93 (0.62) | 2.83 (0.37) | 0.90 (0.63, 1.16) | 46.63 | <0.001 | |
| Summarising data | 1.83 (0.68) | 2.90 (0.30) | 1.07 (0.79, 1.34) | 58.47 | <0.001 | |
| Displaying data | 1.56 (0.56) | 2.80 (0.40) | 1.24 (0.98, 1.49) | 79.48 | <0.001 | |
| Interpreting data | 1.56 (0.56) | 2.73 (0.51) | 1.17 (0.89, 1.44) | 75.00 | <0.001 | |
| Communicating information | 1.56 (0.56) | 2.83 (0.45) | 1.27 (1.00, 1.53) | 81.41 | <0.001 | |
| Case investigation | 1.60 (0.66) | 2.80 (0.47) | 1.20 (0.90, 1.49) | 75.00 | <0.001 | |
| Excel | 1.46 (0.56) | 2.76 (0.49) | 1.30 (1.02, 1.57) | 89.04 | <0.001 | |
| PoPCAB | 1.50 (0.56) | 2.76 (0.49) | 1.26 (0.98, 1.53) | 84.00 | <0.001 | |
| Workshop 2 | Identifying an outbreak | 1.83 (0.52) | 2.93 (0.25) | 1.10 (0.89, 1.31) | 60.11 | <0.001 |
| Descriptive steps of an OI | 1.40 (0.61) | 2.86 (0.34) | 1.46 (1.20, 1.72) | 104.29 | <0.001 | |
| Analytical steps of an OI | 1.23 (0.49) | 2.63 (0.60) | 1.40 (1.11, 1.68) | 113.82 | <0.001 | |
| Response steps of an OI | 1.53 (0.80) | 2.80 (0.40) | 1.27 (0.94, 1.59) | 83.00 | <0.001 | |
| Problem analysis | 1.26 (0.51) | 2.86 (0.34) | 1.60 (1.37, 1.82) | 126.98 | <0.001 | |
| Linking with laboratory | 1.96 (0.65) | 2.80 (0.40) | 0.84 (0.56, 1.11) | 42.86 | <0.001 | |
| Developing a presentation | 2.06 (0.57) | 2.76 (0.42) | 0.70 (0.44, 0.96) | 33.98 | <0.001 | |
| PowerPoint | 2.30 (0.52) | 2.90 (0.30) | 0.60 (0.38, 0.82) | 26.09 | <0.001 | |
| IHR Core Capacities Assessment | 1.96 (0.55) | 2.80 (0.40) | 0.84 (0.59, 1.08) | 42.86 | <0.001 | |
| Contingency Plan | 1.87 (0.61) | 2.86 (0.34) | 0.99 (0.73, 1.24) | 52.94 | <0.001 | |
| Workshop 3 | Developing a presentation | 2.00 (0.36) | 2.96 (0.18) | 0.96 (0.81, 1.11) | 48.00 | <0.001 |
| Giving a presentation | 1.86 (0.43) | 2.93 (0.25) | 1.07 (0.89, 1.25) | 57.53 | <0.001 | |
| Creating Maps using QGIS | 1.40 (0.75) | 2.90 (0.30) | 1.50 (1.20, 1.79) | 107.14 | <0.001 |