Outbreak Investigation | Open Access | Volume 9 (2): Article 84 | Published: 26 May 2026

Views: 586
Menu, Tables and Figures
| Name of Kebele | Cases per Kebele | The total population in each Kebele | Attack rate per 10,000 |
|---|---|---|---|
| Yali | 123 | 6470 | 190.1 |
| Tebeja yaze | 84 | 3965 | 211.8 |
| kasha | 31 | 6093 | 50.9 |
| Boseka | 31 | 3223 | 96.2 |
| Utsikin | 27 | 6269 | 43.1 |
| Walla | 25 | 8579 | 29.1 |
| Dakin | 17 | 6008 | 28.3 |
| Sarity | 15 | 4836 | 31.0 |
| Tishu | 12 | 4427 | 27.1 |
| Yekir Demoze | 10 | 6879 | 14.5 |
| Oka | 10 | 4675 | 21.4 |
| Genja | 8 | 4663 | 17.2 |
| Endekel | 7 | 6960 | 10.1 |
| Golla | 5 | 9691 | 5.2 |
| Gayizikin | 2 | 3810 | 5.2 |
| koskole | 2 | 3955 | 5.1 |
| Muya | 2 | 5750 | 3.5 |
| Go/mag | 1 | 7185 | 1.4 |
| fakatin | 1 | 6710 | 1.5 |
| woshkene | 1 | 4757 | 2.1 |
| kayekene | 1 | 4161 | 2.4 |
| Total | 415 | 119,066 | 34.8 |
Table 1: Rubella case distribution per kebele with attack rate in North Bench District, Southwest Ethiopia, 2024
| Variable | Cases n=143(%) | Controls n=143(%) |
|---|---|---|
| Gender | ||
| Male | 74(51.7) | 66(46.2) |
| Female | 69(48.3) | 77(53.8) |
| Age | ||
| <5 | 114(79.7) | 98(68.5) |
| 5-9 | 23(16.1) | 32(22.4) |
| 10-14 | 3(2.1) | 10(7.0) |
| 15-49 | 3(2.1) | 3(2.1) |
| Caregiver’s Marital Status | ||
| Single | 9(6.3) | 7(4.9) |
| Married | 119(84.3) | 126(88.1) |
| Divorced | 9(6.3) | 5(3.5) |
| Widowed | 6(4.2) | 5(3.5) |
| Family size | ||
| <5 | 89(62.2) | 108(75.5) |
| ≥5 | 54(37.8) | 35(24.5) |
| Caregiver’s occupation | ||
| Farmer | 72(50.3) | 43(30.1) |
| Housewife | 31(21.7) | 65(45.5) |
| Student | 9(6.3) | 7(4.9) |
| Unemployed | 8(5.6) | 7(4.9) |
| Daily laborer | 9(6.3) | 8(5.6) |
| Merchant | 9(6.3) | 5(3.5) |
| Gov’t employed | 5(3.5) | 8(5.6) |
| Religion | ||
| Orthodox | 35(43.8) | 45(56.3) |
| Protestant | 91(53.8) | 78(46.2) |
| Muslim | 10(40.0) | 15(60.0) |
| Catholic | 7(58.3) | 5(41.7) |
| Ethnicity | ||
| Bench | 102(71.3) | 107(74.8) |
| Sheko | 7(4.9) | 6(4.2) |
| Meinit | 8(5.6) | 6(4.2) |
| Kaffa | 12(8.4) | 9(6.3) |
| Amhara | 7(4.9) | 9(6.3) |
| Tigre | 7(4.9) | 6(4.2) |
| Caregiver’s Age | ||
| 20-29 | 66(46.2) | 51(35.7) |
| 30-39 | 58(40.6) | 60(42) |
| >40 | 19(13.3) | 32(22.4) |
| Caregiver education | ||
| No formal education | 89(62.2) | 80(55.9) |
| Elementary | 30(21) | 32(22.4) |
| Secondary | 15(10.5) | 18(12.6) |
| Diploma and above | 9(6.3) | 13(9.1) |
Table 2: Socio-demographic-related factors of participants, North Bench District, Southwest Ethiopia, 2024
| Table 3: Bivariable logistic regression for multivariate analysis, North Bench District, Southwest Ethiopia, 2024. | ||||
|---|---|---|---|---|
| Variables | Cases n=143 (%) | Controls n=143 (%) | P value | COR (95% CI) |
| Age Participants | ||||
| <5 | 114 (79.7) | 98 (68.5) | 0.30 | 1.2 (0.3-4.1) |
| 5-9 | 23 (16.1) | 32 (22.4) | 0.20 | 1.7 (0.2-3.9) |
| 10-14 | 3 (2.1) | 10 (7.0) | 0.70 | 0.3 (0.07-1.3) |
| 15+ | 3 (2.1) | 3 (2.1) | ||
| Family size | ||||
| <5 | 89 (62.2) | 108 (75.5) | 1 | |
| ≥5 | 54 (37.8) | 35 (24.5) | 0.02 | 1.9 (1.1-3.1) |
| Age of caregivers | ||||
| 22-31 | 66 (46.2) | 51 (35.7) | 1 | |
| 32-41 | 58 (40.6) | 60 (42) | 0.54 | 0.9 (0.5-1.4) |
| >41 | 19 (13.3) | 32 (22.4) | 0.04 | 0.5 (0.3-1.0) |
| Measles Vaccination Status | ||||
| Vaccinated | 74 (51.7) | 88 (61.5) | 1 | |
| Not vaccinated | 69 (48.3) | 55 (38.5) | 0.10 | 1.5 (0.9-2.4) |
| History of diarrhea | ||||
| Yes | 91 (63.6) | 54 (37.8) | 0.01 | 2.9 (1.8-4.7) |
| No | 52 (36.4) | 89 (62.2) | 1 | |
| Vitamin A supplementation | ||||
| Supplemented | 65 (45.5) | 91 (63.6) | 1 | |
| Not supplemented | 78 (54.5) | 52 (36.4) | 0.02 | 2.1 (1.3-3.4) |
| Travel history | ||||
| Yes | 48 (33.6) | 35 (24.5) | 0.09 | 1.6 (0.9-2.6) |
| No | 95 (66.4) | 108 (75.5) | 1 | |
| Contact history | ||||
| Yes | 88 (61.5) | 39 (27.3) | 0.01 | 4.3 (2.6-7.0) |
| No | 55 (38.5) | 104 (72.7) | 1 | |
| House condition | ||||
| Well Ventilated | 64 (44.8) | 86 (60.1) | 1 | |
| Poorly ventilated | 79 (55.2) | 57 (39.9) | 0.01 | 1.9 (1.2-3.0) |
Table 3: Bivariable logistic regression for multivariate analysis, North Bench District, Southwest Ethiopia, 2024
| Table 4: Variables independently associated with rubella infection in multivariable logistic regression, North Bench District, Southwest Ethiopia, 2024. | |
|---|---|
| Variables | AOR (95% CI) |
| Family size | |
| ≥5 | 2.2(1.2, 3.9) |
| <5 | 1 |
| History of diarrhea | |
| Yes | 2.7(1.5, 4.6) |
| No | 1 |
| Vitamin A supplementation | |
| Not supplemented | 1.8(1.1, 3.1) |
| Supplemented | 1 |
| Contact history | |
| Yes | 3.8(2.2, 6.6) |
| No | 1 |
| House condition | |
| Poorly ventilated | 1.8(1.0, 3.2) |
| Well Ventilated | 1 |
Table 4: Variables independently associated with rubella infection in multivariable logistic regression, North Bench District, Southwest Ethiopia, 2024
Desalew Mulu Gebey1,&, Guta Kune2, Gemechu Chemeda1
1Ethiopia Field Epidemiology and Laboratory Training Program (EFELTP), Jimma University, Jimma, Ethiopia, 2Department of Epidemiology, Faculty of Public Health, Jimma University, Jimma, Ethiopia
&Corresponding author: Desalew Mulu Gebey, Ethiopia Field Epidemiology and Laboratory Training Program (EFELTP), Jimma University, Jimma, Ethiopia, Email: mdessye12@gmail.com ORCID: https://orcid.org/0009-0009-8612-4736
Received: 14 Sep 2025, Accepted: 22 May 2026, Published: 26 May 2026
Domain: Infectious Disease Epidemiology
Keywords: Rubella, Outbreak investigation, North Bench District, Southwest Ethiopia
©Desalew Mulu Gebey et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Desalew Mulu Gebey et al. Rubella outbreak investigation in North Bench District, Southwest Ethiopia, 2024. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):84. https://doi.org/10.37432/jieph-d-25-00191
Introduction: Rubella poses severe risks to pregnant women due to the potential for Congenital Rubella Syndrome. In Ethiopia, rubella remains an overlooked public health concern. The disease is not a priority in national surveillance, and its vaccine has yet to be included in the infant immunisation program. On January 8, 2024, a rumour of a suspected rubella outbreak in Southwest Ethiopia was reported, with rising cases, prompting a study to confirm the existence of the outbreak, describe cases epidemiologically, and assess risk factors.
Methods: A descriptive cross-sectional study combined with a 1:1 unmatched case-control investigation was conducted in the North Bench district, Ethiopia, from July 10 to 30, 2024. The descriptive analysis included all 415 cases from the outbreak line list. The case-control study enrolled 143 cases and 143 controls. Cases were defined as individuals with laboratory-confirmed rubella IgM, epidemiologically linked to confirmed cases, or presenting with fever and maculopapular rash in the affected kebeles from January 8 to May 26, 2024; randomly selected from the line list. Controls were selected from rash- and fever-free neighbours. Variables with P<0.25 in bivariable analysis entered multivariable logistic regression; those with P<0.05 were deemed significant predictors of rubella infection. The adjusted odds ratios and 95% confidence intervals were reported.
Results: Rubella outbreak was confirmed in the district, and it had an overall attack rate of 34.8 per 10,000 population. Having a history of contact with an active case (aOR: 3.8, 95%CI: 2.2- 6.6), having a history of diarrhea before two weeks (aOR: 2.7, 95%CI: 1.5-4.6), families with a size of more than 5 per household (aOR: 2.2, 95%CI: 1.2-3.9), lacking vitamin A supplementation in the past six months (aOR: 1.8, 95%CI: 1.1 – 3.1), and living in a poorly ventilated house (aOR: 1.8, 95%CI: 1.0- 3.2) were found to be associated with rubella infection.
Conclusion: Rubella outbreak was confirmed in the district, and was associated with contact with cases, recent diarrhoea, large households, poor ventilation, and lack of vitamin A. Improving vitamin A coverage, early case detection, and community awareness on ventilation and infection prevention are essential to prevent future outbreaks
Rubella, caused by the rubella virus, is an acute and contagious viral infection. It is a leading cause of vaccine-preventable birth defects, contributing to 1.5 million child deaths globally[1,2]. It spreads through respiratory droplets from coughs, sneezes, or direct contact with an infected person. The incubation period lasts 14 to 18 days, and rubella symptoms include a maculopapular rash, often accompanied by fever and lymphadenopathy (occipital or cervical). The virus can be transmitted up to seven days before or after a rash appears, with the highest transmission rate occurring during the rash phase.
Globally, the World Health Organization (WHO) reported nearly 42,403 cases of rubella and 1,332 cases of congenital rubella syndrome in 2023 [3]. The global efforts to eliminate rubella bounced back remarkably. According to the 2024 WHO/UNICEF Estimates of National Immunization Coverage (WUENIC) report, regions like the Americas and Western Pacific have maintained the vital 95% coverage mark for infants. This strong community immunity is the main reason rubella and CRS cases have fallen, keeping transmission rates at or below the target of one case per 100,000 live births[4]. However, for countries in the African region, Rubella is a major factor for neurological and developmental complications and has long-term health effects[5].
In 2023, the WHO reported that 8% and 13% of children with CRS later developed neurological and developmental complications, respectively. Notably, in sub-Saharan Africa, 95% of reported rubella infections involved children under 14 years of age. Moreover, studies in Africa, like in Zimbabwe[4], showed that the rubella outbreak affected 1–29% of adults and 6–21% of women aged 15–49 years in 2022[6,7].
The rubella outbreak investigation in Kenya revealed that the occurrence of the rubella outbreak was associated with being unvaccinated, as well as with crowded working and living conditions, and children aged 5-14 years were predominantly affected[8]. Moreover, studies in Ethiopia also show that living in an unventilated household, having a history of contact with rubella cases, lacking adequate information, having a family size of more than five, and not receiving vitamin A supplements in the last six months are all major risk factors for contracting the disease[9].
Rubella is preventable through immunization, as WHO reports show that over 95% of children who receive RCV after 12 months of age develop protective immunity, and over 90% of those vaccinated remain protected for at least 15 years, with immunity often persisting lifelong[6].
In Ethiopia, the Expanded Program on Immunization (EPI) began in 1980[10], yet rubella vaccination remains absent from the infant schedule. Rubella is endemic, with a prevalence of 19.5% and an incidence rate of 2.3 cases per 100,000 population. The highest immunoglobulin M (IgM) positivity (20.7%) and cases (1,103) occur in children aged 5-9 years [1]. A lack of dedicated surveillance for CRS hampers understanding of rubella’s public health impact[11].
On January 8, 2024, seven suspected rubella cases were reported from Bear Health Center in the North Bench District. A multidisciplinary rapid response team was deployed to investigate and respond to the outbreak. This study is crucial to inform the potential introduction of the rubella vaccine nationally and strengthen surveillance systems to prevent future outbreaks. With limited evidence on rubella’s epidemiology and associated factors in Ethiopia, particularly in this district, the study sought to confirm the outbreak, describe cases epidemiologically, and identify key associated factors driving rubella transmission in North Bench District.
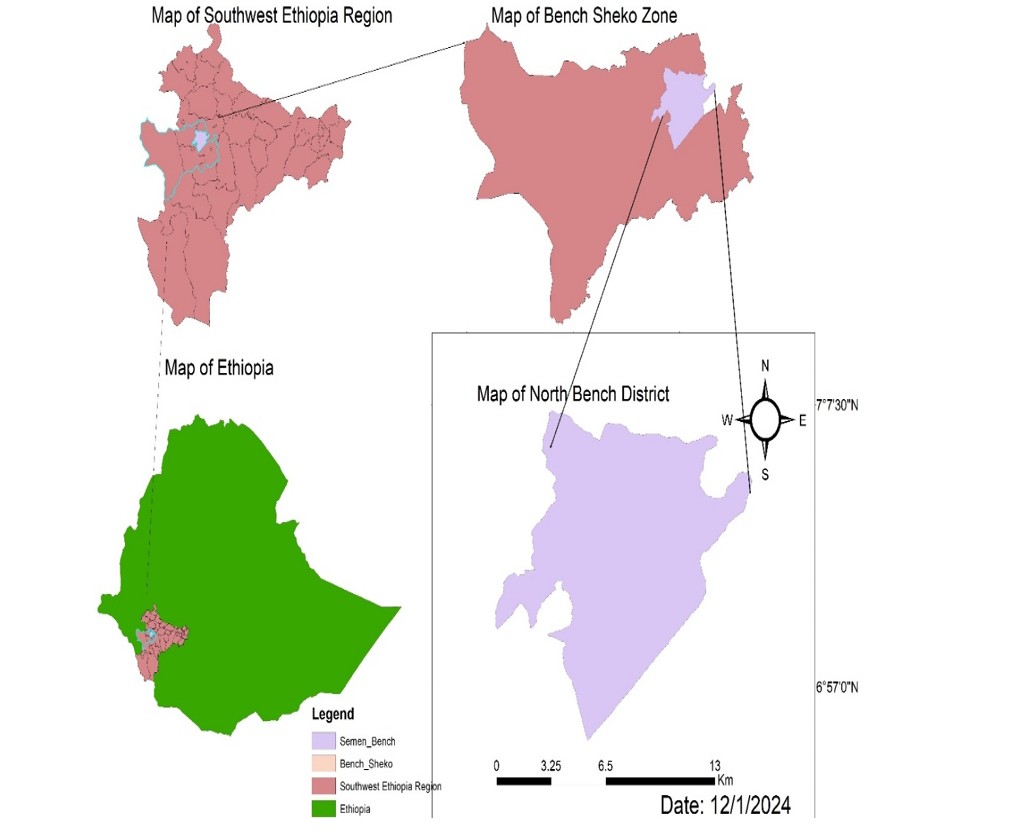
Study area, design, and period
A descriptive cross-sectional study, followed by a community-based unmatched case-control design, was conducted in the North Bench District between July 10 and 30, 2024. The district lies approximately 550 kilometres southwest of Addis Ababa, the capital of Ethiopia, and is predominantly rural in character. According to the 2023/24 population projection, the district is home to 119,066 inhabitants, of whom 58,343 are men, and 18,587 are children under the age of five. Administratively, North Bench (Figure 1) is divided into 21 kebeles (the smallest governmental units in Ethiopia). Health services in the district are delivered through three health centres and 21 health posts, which provide primary health care to the community.
Study population
The source population comprised all individuals residing in the North Bench District during the investigation period. The study units were therefore individual cases and controls residing in selected households of the affected kebeles. Cases were included if they had laboratory confirmation of rubella IgM antibody or were epidemiologically linked to a confirmed rubella case or presented with fever and maculopapular rash in the selected kebele of North Bench District from January 8 to May 26, 2024. Controls were eligible if they were neighbours of cases from the same kebeles and did not meet the rubella case definition. Individuals who did not meet the rubella case definition and declined participation were excluded from the case and control groups, respectively.
Sample size determination
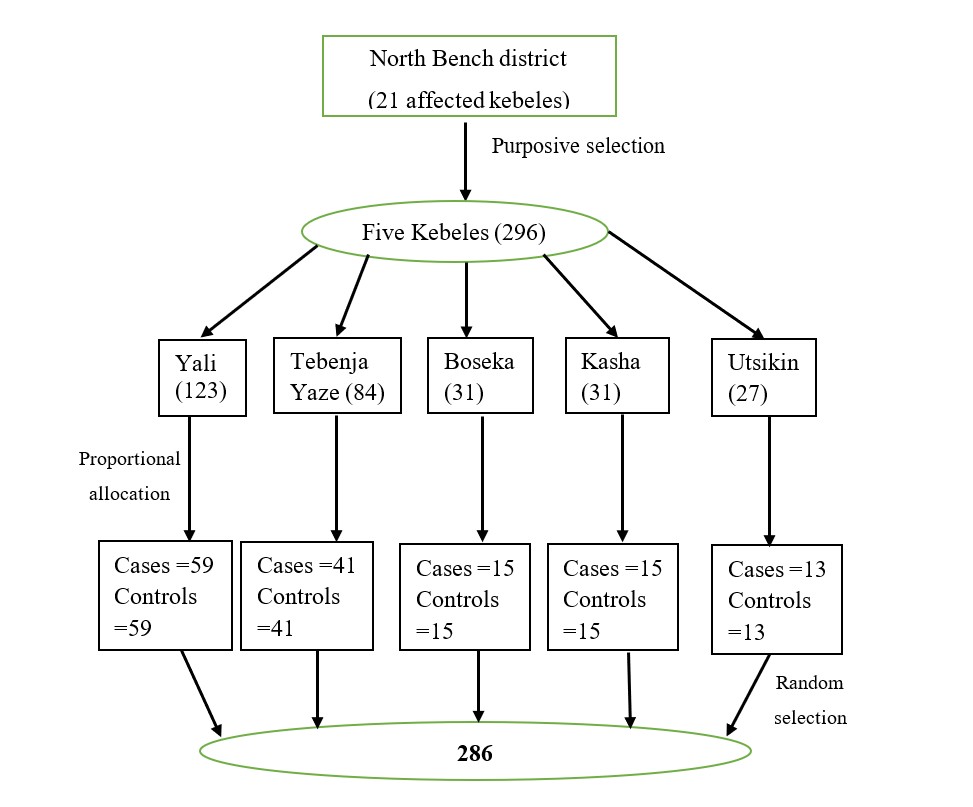
The required sample size was calculated using the double population proportion formula in Epi Info version 7.2.5.0. Parameters included a control exposure proportion of 24%, an aOR of 2.2[7], a 95%CI, 80% power, and a 1:1 case-to-control ratio. The largest estimated sample size was 260, based on the variable “contact history with rubella cases.” To account for a possible 10% non-response rate, the final sample size was increased to 286 participants, comprising 143 cases and 143 controls.
Sampling procedures
For the descriptive component, data were extracted from a line list covering the period between January 8 and May 20, 2024. This list, which contained 415 confirmed and epidemiologically linked rubella cases, was compiled through house-to-house active surveillance. For the case-control component, five kebeles with the highest reported caseloads were selected. Within these kebeles, cases were randomly chosen, and home-to-home visits were conducted for recruitment. For each case, one neighbourhood control was identified using purposive sampling. To ensure epidemiological validity, recruitment took place 42 days after the outbreak was declared (after May 26, 2024), which accounted for the incubation period of rubella. In households with more than one eligible participant, the lottery method was applied to select the study participants (Figure 2).
Operational definitions
A suspected case was any individual with a generalised maculopapular rash, fever, and at least one of the following symptoms: arthralgia or arthritis, lymphadenopathy, or conjunctivitis, in the absence of epidemiologic linkage or laboratory confirmation. Probable case was a suspected patient of rubella that has not had a specimen taken for serologic confirmation, but is connected (by time, place, and person) to a case that has tested positive for rubella IgM by a laboratory and resides in the same or a nearby district where there is a chance of transmission. A confirmed case was defined as a suspected case with laboratory evidence, including virus isolation, detection of rubella-specific nucleic acid by polymerase chain reaction, a significant rise in rubella immunoglobulin G (IgG) antibody titers, or a positive IgM serologic test[12].
A total of 10 questions, demonstrating a reliability test with a Cronbach’s alpha value of 0.72, were used to assess participants’ knowledge regarding exposure status, modes of transmission, signs and symptoms, treatment options, and prevention methods. Participants were given a score of 1 for each correct answer and zero otherwise. All correct answers were added together, and the mean score was calculated to be 4.3. Finally, participants who scored above the mean score were declared as having good knowledge, and those who scored the mean or below the mean as having poor knowledge of rubella[13].
Study variables
The dependent variable in this study was rubella infection status, categorised as case or control. Independent variables included sociodemographic factors, including gender, age, caregiver’s marital status, family size, caregiver’s occupation, religion, ethnicity, caregiver’s age, caregiver’s education, risk-related factors including recent contact history with confirmed rubella cases, measles vaccination status, housing conditions, vitamin A supplementation in the last 6 months, history of diarrhea within two weeks, travel history outside the kebele in the incubation period (12–23 days pre-rash) and knowledge-scores.
Data collection procedures
For the descriptive component, information was obtained from line lists and patient medical records maintained at local health facilities. For the analytical component, a structured, interviewer-administered questionnaire adapted from previous literature [1,12], [14–16]was employed. Adult participants were interviewed directly, while for children, data were obtained from parents or guardians. Data collection was carried out electronically using Kobo Toolbox software on Android devices by two field epidemiology residents and one environmental technician, under the close supervision of the zonal Public Health Emergency Management Directorate.
Laboratory methods
At Bear Health Centre of the North Bench District, a laboratory technician collected 5 mL serum samples from five suspected rubella patients. Using sterile protocols, each sample was labelled and linked to case-based reporting forms. These were transported to the Ethiopian Public Health Institute national laboratory for IgM antibody testing.
Data analysis
Data collected via Kobo Toolbox were exported to Excel for cleaning and subsequently imported into SPSS version 26 for analysis. Descriptive statistics, including frequencies, proportions, and means, were generated, and epidemic curves were plotted to illustrate temporal trends. Bivariate logistic regression was initially performed, and variables with p-values less than 0.25 were entered into multivariable logistic regression models. Statistical significance was declared at p < 0.05, and associations were reported using adjusted odds ratios with 95% confidence intervals. Model fitness was assessed using the Hosmer-Lemeshow test (p = 0.58), while multicollinearity was evaluated using the variance inflation factor (VIF = 1.03), which indicated no significant collinearity.
Data quality management
To ensure data quality, data collectors received a half-day training covering study objectives, interviewing techniques, and the use of Kobo Collect software. The questionnaire was pretested in non-study kebeles, using 5% of the total sample, to improve the instrument’s clarity and consistency. Field supervisors closely monitored data collection to ensure adherence to study protocols. Both cases and controls were recruited from the same communities to minimise selection bias. Data entry verification, range/logic checks, identification of outliers, and missing data assessment were performed.
Ethical consideration
The study received approval from the Bench Sheko Zone Health Department’s Public Health Emergency Management Ethical Committee, with reference number 4359/54/2024, dated 13/04/2024. We obtained an official permission letter from the North Bench District Health Office to conduct the outbreak investigations. After providing participants with a brief explanation of the study’s objectives and ensuring they understood their voluntary choice to participate, we obtained written informed consent from those aged over 18 years, as well as from their legal guardians for participants under 18. To protect participant confidentiality, all data were anonymised by removing personal identifiers during data collection. Access to the data was restricted to the research team and authorised personnel only.
Descriptive epidemiology by place, person, and time
Between January 8 and May 20, 2024, 415 cases of rubella were reported. The outbreak’s index case was a 2-year-old boy who travelled with his sister to the South Bench District on December 20, 2023, where similar symptoms were noted. On January 8, the Bear Health Centre alerted the North Bench District Health Office, which notified higher authorities. A multidisciplinary rapid response team was dispatched for investigation and response. Two weeks after samples were transported to the Ethiopian Public Health Institute, results confirmed rubella in four of the five patients through IgM antibody testing. This precise diagnostic process ensured the outbreak was accurately identified and documented according to standard national health protocols.
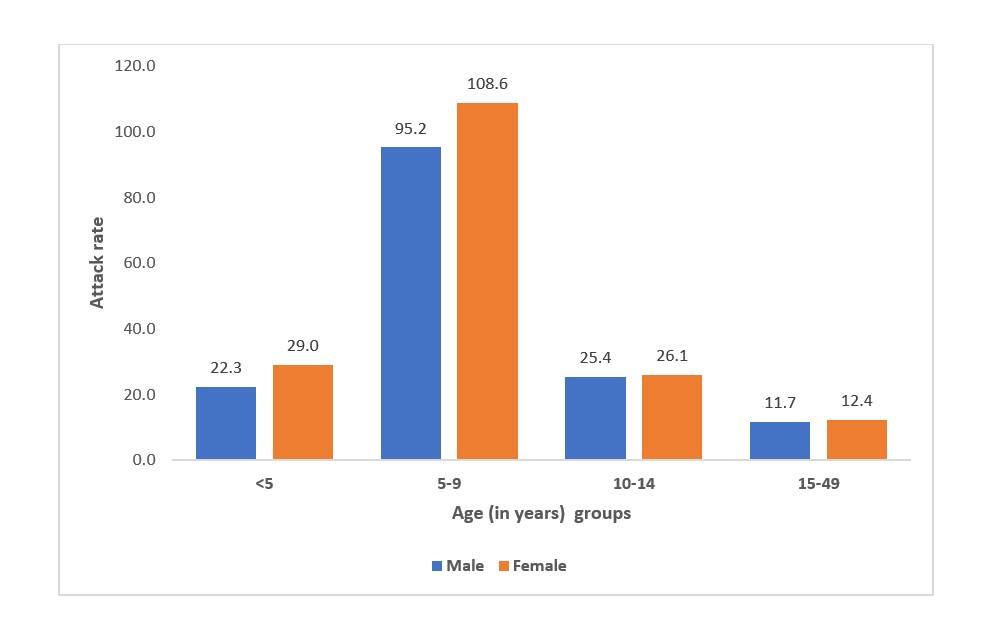
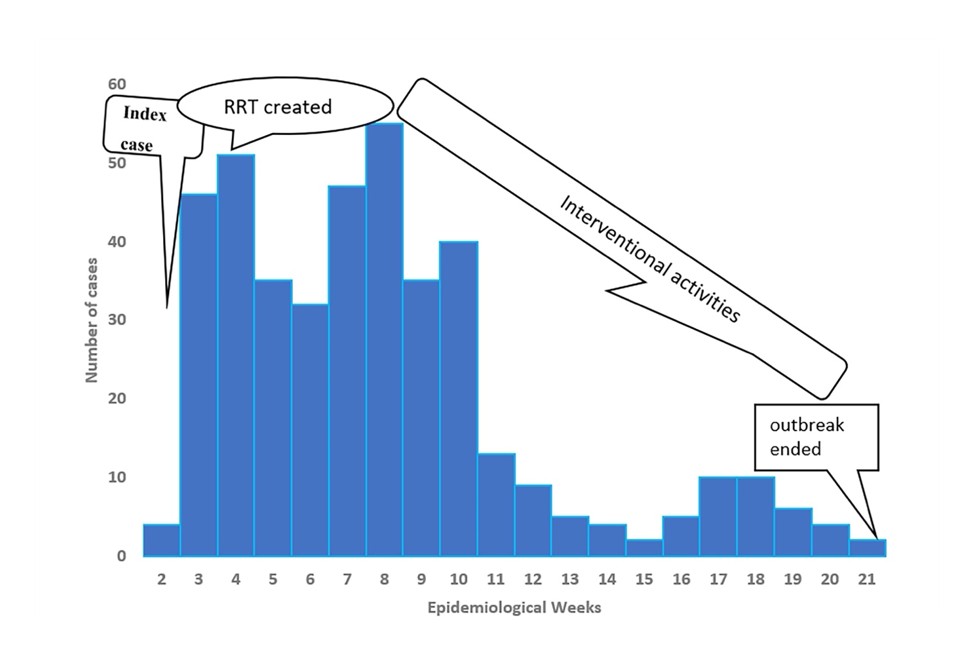
The overall attack rate was 34.8 per 10,000 population. Most rubella cases occurred in the age groups of 5-9 years, accounting for an AR of 95.2 per 10,000 in the male population and 108.6 per 10,000 in the female population (Figure 3). The distribution of rubella cases across the 21 Kebeles demonstrated geographic variation, with an overall attack rate of 34.8 per 10,000 population, with 119,066 total population. Tebeja Yaze has the highest attack rate (211.8 per 10,000), followed by Yali (190.1 per 10,000) (Table 1). The epidemic curve, plotted with date of symptom onset grouped by epidemiological week, showed the index case on January 8, 2024, peaking in week 8, followed by intermittent declines, showing a propagated pattern that rises to peak in week 8, then declines intermittently to end week 21(Figure 4).
All rubella cases presented with fever and maculopapular rash. Nearly half, 225 (54%), also experienced cough, while 7 (1.7%) developed severe pneumonia requiring hospital referral. In addition, 3 (1.2%) had severe acute malnutrition alongside their rubella infection.
Public health action
Following the announcement of a Rubella outbreak on January 8, 2024, in the North Bench District, we took immediate action by organising an emergency meeting to address the crisis. We provided on-site orientation to ensure that all team members, following training of focal persons and health extension workers in each kebele, were informed about the situation. The rapid response team was assigned to support the primary health facility in assessing the status of the outbreak and enhancing the active case search within affected communities, including schools, religious institutions, and private clinics, to identify and contain the outbreak swiftly. We distributed a standardised format for documenting cases of rubella, known as the rubella line-list. We also undertook a thorough review of the resources currently available, evaluating whether additional supplies or personnel were necessary to effectively manage the outbreak. Alert letters were disseminated throughout the district, and the reporting kebele was instructed to supply more detailed information to assist the rapid response team. Isolation treatment areas were prepared, and supportive treatments like fluids and analgesics were given as needed.
Analytical epidemiology
A total of 286 individuals participated in this study, consisting of 143 cases and 143 controls, with response rates of 100% for both cases and controls. The median age of the case participants was 3 years interquartile range (IQR:1-4), while the median age of the control participants was also 3 years (IQR: 2-6) (Table 2).
Regarding knowledge, 74 (51.7%) participants in the case group were categorised as having poor knowledge. Similarly, 81(56.6%) participants in the control group also displayed poor knowledge.
In the bivariate binary logistic regression analysis, the age of the participants, family size, age of the caregivers, educational level of the caregivers, vaccination status for measles, history of diarrhea within two weeks before rubella illness, history of vitamin A supplementation, travel to areas with active cases, and contact with individuals who had active cases were found to be significant factors for rubella infection, with a statistically significant p-value <0.25(Table 3).
After adjusting for potential confounding effects, five multivariate logistic variables were found to be significantly associated with rubella infection. Individuals who had contact with an active case had higher odds (aOR: 3.8, 95%CI: 2.2-6.6) of infection compared to those who did not. The. The odds of contracting rubella were 2.7 times greater (aOR: 2.7, 95%CI: 1.5-4.6) for individuals who had a history of diarrhoea within two weeks before the rubella infection than for those without a history of diarrhoea. Families with a size of more than 5 per household had 2.2 (aOR: 2.2, 95%CI: 1.2-3.9) higher odds of having rubella infection than households with fewer than five persons. Individuals who did not receive vitamin A supplementation had higher odds (aOR: 1.8, 95%CI: 1.1-3.1) of rubella infection than those who received vitamin A supplementation. Compared with living in well-ventilated houses, living in a poorly ventilated house increased the odds of contracting rubella infection by 1.8 times (aOR: 1.8, 95% CI: 1.0-3.2(Table 4).
In this study, the overall rubella AR was 34.8 per 10,000 people. This result is greater than the results of studies conducted in Gonder Town, Northern Ethiopia[15]. This discrepancy may be attributed to differences in healthcare access and quality, as these factors can significantly influence the detection and reporting of rubella cases. In areas with limited healthcare access, many infections may go unreported, while regions with higher quality healthcare are likely to identify and document more cases, thereby affecting the overall reported attack rates.
The study determined that the odds of rubella infection were higher for those who had contact with an active case than for those who did not. This finding aligns with the rubella outbreak findings in the Asossa zone, Benishangul Gumuz Region, Kuyu Oromia region, Miyo District-Borena zone, Oromia region[16,17]. It has already been proven that rubella-infected individuals are highly contagious from a week before the rash appears to a week after it has emerged [18]. This implies that the isolation and travel limitations of suspected cases should be increased during the contagious period. Public health surveillance systems should be enhanced in early rumour detection, management, and response to prevent widespread infection through contacts.
The odds of contracting rubella were higher for individuals who had a history of diarrhoea within two weeks before the rubella infection than for those without a history of diarrhoea, which aligns with studies in Kuyu District, Ethiopia, and Kenya[8,17]. This may be linked to diarrhoea, which is presumably common in this population and often forgotten; rubella symptoms could be a recall anchor for cases due to increased attention to symptoms, leading to potential recall bias. Diarrhoea is also most common in young children, which had higher attack rate. This calls for public health action to emphasise maintaining good personal and environmental health and seeking medical attention for diarrhoea.
We found that the odds of acquiring rubella infection in families with a size of more than 5 per household were higher than those in their counterparts. This is consistent with the study conducted in the Metekel Zone in Ethiopia, Oromia in Ethiopia, and Zimbabwe[17]. This finding may indicate that crowded living situations can facilitate transmission and underscores the importance of modifying public health strategies to address the specific associated factors with household size to effectively control rubella outbreaks.
The odds of having a rubella infection were higher for those who did not receive vitamin A supplementation in the past six months than for their counterparts. These findings align with study findings carried out in Poland and Oromia, Ethiopia[17,19]. This might be because vitamin A is essential for immune cell development and function; a deficiency can impair the body’s response to infections such as rubella. This underlines the need for monitoring systems to track vitamin A supplementation coverage and identify populations that lack recent supplementation.
Additionally, this study revealed that living in a poorly ventilated house increased the odds of rubella infection. Persons in such houses had 1.84 times higher odds of having a rubella infection than those in well-ventilated houses. This finding parallels the findings of the rubella outbreak conducted in the Asossa Zone in western Ethiopia[17]. This may be because inadequate ventilation can lead to various health issues, as it facilitates the spread of rubella through respiratory secretions, underscoring the importance of improving housing conditions.
Limitations
The results may not be broadly applicable, since neighbour-based controls might have similar socioeconomic or demographic traits to the cases. Since participants may not recall past events accurately, the use of self-reported data for exposures like vitamin A intake and diarrhoea history also increases the risk of recall bias. Additionally, correlated responses within the same household may result from the analysis’s incomplete adjustment for household clustering, which could overstate statistical significance.
Since up to 50% of rubella cases might be asymptomatic, we recognise that the case definition, which relies exclusively on symptomatic screening, could introduce misclassification bias, underestimating true incidence and skewing case-control comparisons. Controls were not tested for rubella due to resource limitations during the outbreak response; instead, rapid case confirmation and containment were prioritised over thorough control testing in accordance with national PHEM guidelines.
Despite those limitations, the inclusion of a diverse population enhances the findings’ applicability to various groups, and its large sample size boosts statistical power. Additionally, the use of thorough data collection techniques that incorporate a variety of exposure variables and outcomes improves the analysis’s overall quality. When considered collectively, these findings provide significant insights and provide important evidence for public health initiatives.
A rubella outbreak was confirmed in the North Bench District, with different factors associated with it, including contact with active cases, recent diarrheal illness, household size greater than five members, lack of vitamin A supplementation, and poor household ventilation. Therefore, introducing RCV, strengthening surveillance, improving vitamin A coverage, promoting early case detection, and enhancing community awareness on ventilation and infection prevention are essential to prevent future outbreaks.
What is already known about the topic
What this study adds
We would like to extend our heartfelt gratitude to Jimma University, the Institute of Health, the Faculty of Public Health, and the Department of Epidemiology for providing the essential academic training and resources vital for this study. We are also deeply appreciative of the Bench Sheko Zone health department PHEM officers, staff, and North Bench District public health emergency management officers and health extension workers for their invaluable guidance and information during the outbreak investigation.
DMG designed the study, analyzed the data, and drafted the manuscript. GK provided supervision and validation. GC was responsible for the conceptualization and methodology, contributed to the data software, carried out data curation, and oversaw the review and editing of the manuscript. All authors have drafted the original manuscript, reviewed it, and approved the final version of the manuscript.
| Name of Kebele | Cases per Kebele | The total population in each Kebele | Attack rate per 10,000 |
|---|---|---|---|
| Yali | 123 | 6470 | 190.1 |
| Tebeja yaze | 84 | 3965 | 211.8 |
| kasha | 31 | 6093 | 50.9 |
| Boseka | 31 | 3223 | 96.2 |
| Utsikin | 27 | 6269 | 43.1 |
| Walla | 25 | 8579 | 29.1 |
| Dakin | 17 | 6008 | 28.3 |
| Sarity | 15 | 4836 | 31.0 |
| Tishu | 12 | 4427 | 27.1 |
| Yekir Demoze | 10 | 6879 | 14.5 |
| Oka | 10 | 4675 | 21.4 |
| Genja | 8 | 4663 | 17.2 |
| Endekel | 7 | 6960 | 10.1 |
| Golla | 5 | 9691 | 5.2 |
| Gayizikin | 2 | 3810 | 5.2 |
| koskole | 2 | 3955 | 5.1 |
| Muya | 2 | 5750 | 3.5 |
| Go/mag | 1 | 7185 | 1.4 |
| fakatin | 1 | 6710 | 1.5 |
| woshkene | 1 | 4757 | 2.1 |
| kayekene | 1 | 4161 | 2.4 |
| Total | 415 | 119,066 | 34.8 |
| Variable | Cases n=143(%) | Controls n=143(%) |
|---|---|---|
| Gender | ||
| Male | 74(51.7) | 66(46.2) |
| Female | 69(48.3) | 77(53.8) |
| Age | ||
| <5 | 114(79.7) | 98(68.5) |
| 5-9 | 23(16.1) | 32(22.4) |
| 10-14 | 3(2.1) | 10(7.0) |
| 15-49 | 3(2.1) | 3(2.1) |
| Caregiver’s Marital Status | ||
| Single | 9(6.3) | 7(4.9) |
| Married | 119(84.3) | 126(88.1) |
| Divorced | 9(6.3) | 5(3.5) |
| Widowed | 6(4.2) | 5(3.5) |
| Family size | ||
| <5 | 89(62.2) | 108(75.5) |
| ≥5 | 54(37.8) | 35(24.5) |
| Caregiver’s occupation | ||
| Farmer | 72(50.3) | 43(30.1) |
| Housewife | 31(21.7) | 65(45.5) |
| Student | 9(6.3) | 7(4.9) |
| Unemployed | 8(5.6) | 7(4.9) |
| Daily laborer | 9(6.3) | 8(5.6) |
| Merchant | 9(6.3) | 5(3.5) |
| Gov’t employed | 5(3.5) | 8(5.6) |
| Religion | ||
| Orthodox | 35(43.8) | 45(56.3) |
| Protestant | 91(53.8) | 78(46.2) |
| Muslim | 10(40.0) | 15(60.0) |
| Catholic | 7(58.3) | 5(41.7) |
| Ethnicity | ||
| Bench | 102(71.3) | 107(74.8) |
| Sheko | 7(4.9) | 6(4.2) |
| Meinit | 8(5.6) | 6(4.2) |
| Kaffa | 12(8.4) | 9(6.3) |
| Amhara | 7(4.9) | 9(6.3) |
| Tigre | 7(4.9) | 6(4.2) |
| Caregiver’s Age | ||
| 20-29 | 66(46.2) | 51(35.7) |
| 30-39 | 58(40.6) | 60(42) |
| >40 | 19(13.3) | 32(22.4) |
| Caregiver education | ||
| No formal education | 89(62.2) | 80(55.9) |
| Elementary | 30(21) | 32(22.4) |
| Secondary | 15(10.5) | 18(12.6) |
| Diploma and above | 9(6.3) | 13(9.1) |
| Table 3: Bivariable logistic regression for multivariate analysis, North Bench District, Southwest Ethiopia, 2024. | ||||
|---|---|---|---|---|
| Variables | Cases n=143 (%) | Controls n=143 (%) | P value | COR (95% CI) |
| Age Participants | ||||
| <5 | 114 (79.7) | 98 (68.5) | 0.30 | 1.2 (0.3-4.1) |
| 5-9 | 23 (16.1) | 32 (22.4) | 0.20 | 1.7 (0.2-3.9) |
| 10-14 | 3 (2.1) | 10 (7.0) | 0.70 | 0.3 (0.07-1.3) |
| 15+ | 3 (2.1) | 3 (2.1) | ||
| Family size | ||||
| <5 | 89 (62.2) | 108 (75.5) | 1 | |
| ≥5 | 54 (37.8) | 35 (24.5) | 0.02 | 1.9 (1.1-3.1) |
| Age of caregivers | ||||
| 22-31 | 66 (46.2) | 51 (35.7) | 1 | |
| 32-41 | 58 (40.6) | 60 (42) | 0.54 | 0.9 (0.5-1.4) |
| >41 | 19 (13.3) | 32 (22.4) | 0.04 | 0.5 (0.3-1.0) |
| Measles Vaccination Status | ||||
| Vaccinated | 74 (51.7) | 88 (61.5) | 1 | |
| Not vaccinated | 69 (48.3) | 55 (38.5) | 0.10 | 1.5 (0.9-2.4) |
| History of diarrhea | ||||
| Yes | 91 (63.6) | 54 (37.8) | 0.01 | 2.9 (1.8-4.7) |
| No | 52 (36.4) | 89 (62.2) | 1 | |
| Vitamin A supplementation | ||||
| Supplemented | 65 (45.5) | 91 (63.6) | 1 | |
| Not supplemented | 78 (54.5) | 52 (36.4) | 0.02 | 2.1 (1.3-3.4) |
| Travel history | ||||
| Yes | 48 (33.6) | 35 (24.5) | 0.09 | 1.6 (0.9-2.6) |
| No | 95 (66.4) | 108 (75.5) | 1 | |
| Contact history | ||||
| Yes | 88 (61.5) | 39 (27.3) | 0.01 | 4.3 (2.6-7.0) |
| No | 55 (38.5) | 104 (72.7) | 1 | |
| House condition | ||||
| Well Ventilated | 64 (44.8) | 86 (60.1) | 1 | |
| Poorly ventilated | 79 (55.2) | 57 (39.9) | 0.01 | 1.9 (1.2-3.0) |
| Table 4: Variables independently associated with rubella infection in multivariable logistic regression, North Bench District, Southwest Ethiopia, 2024. | |
|---|---|
| Variables | AOR (95% CI) |
| Family size | |
| ≥5 | 2.2(1.2, 3.9) |
| <5 | 1 |
| History of diarrhea | |
| Yes | 2.7(1.5, 4.6) |
| No | 1 |
| Vitamin A supplementation | |
| Not supplemented | 1.8(1.1, 3.1) |
| Supplemented | 1 |
| Contact history | |
| Yes | 3.8(2.2, 6.6) |
| No | 1 |
| House condition | |
| Poorly ventilated | 1.8(1.0, 3.2) |
| Well Ventilated | 1 |