Outbreak Investigation | Open Access | Volume 9 (2): Article 101 | Published: 18 Jun 2026
Views: 45
Menu, Tables and Figures
| Table 1: Sociodemographic characteristics of chickenpox cases, Old Ayoma, Jasikan Municipality, Ghana, October 2021 | ||
| Variable | Frequency (N=10) | Per cent (%) |
|---|---|---|
| Median age in years | 9.5 (IQR: 5.5, 15.5) | |
| Age group (years) | ||
| Below 15 | 7 | 70.0 |
| 15 and above | 3 | 30.0 |
| Sex | ||
| Male | 9 | 90.0 |
| Female | 1 | 10.0 |
| Community of residence | ||
| Dzolu | 3 | 30.0 |
| Old Ayoma | 7 | 70.0 |
| Median household size | 8 (IQR: 3.5, 10) | |
| Main occupation | ||
| Pupil | 6 | 60.0 |
| Preschool child | 2 | 20.0 |
| Farmer | 1 | 10.0 |
| Health worker | 1 | 10.0 |
Table 1: Sociodemographic characteristics of chickenpox cases, Old Ayoma, Jasikan Municipality, Ghana, October 2021
| Table 2: Clinical presentations of suspected chickenpox cases in Old Ayoma, Jasikan Municipality, Ghana, October 2021 | ||
| Variable | Frequency (N=10) | Per cent (%) |
|---|---|---|
| Surveillance type | ||
| Active | 5 | 50.0 |
| Passive | 5 | 50.0 |
| Signs and symptoms* | ||
| Rash | 10 | 100.0 |
| Fever | 8 | 80.0 |
| Loss of appetite | 7 | 70.0 |
| Muscle pains | 6 | 60.0 |
| Headache | 5 | 50.0 |
| Abdominal pains | 4 | 40.0 |
| Joint pains | 4 | 40.0 |
| Tiredness | 4 | 40.0 |
| Discomfort | 2 | 20.0 |
| Runny nose | 0 | 0.0 |
| Duration of rash | ||
| Mean ± S.D (range) days | 4.2 ± 1.31 (3,7) | |
| Location of rash* | ||
| Head and face | 9 | 90.0 |
| Arms | 9 | 90.0 |
| Trunk | 6 | 60.0 |
| Legs | 6 | 60.0 |
| Inside mouth | 2 | 20.0 |
| Severity of rash | ||
| Mild | 2 | 20.0 |
| Average | 3 | 30.0 |
| Moderate | 4 | 40.0 |
| Severe | 1 | 10.0 |
| Case management location | ||
| Managed within health facility (under observation) | 4 | 40.0 |
| Managed at home | 6 | 60.0 |
| Case observation period among facility-managed cases (n=4) | ||
| Mean ± S.D (range) days | 2 ± 1.42 (1,4) | |
| * Multiple responses; S.D = Standard deviation | ||
Table 2: Clinical presentations of suspected chickenpox cases in Old Ayoma, Jasikan Municipality, Ghana, October 2021
| Table 3: Exposure history and adherence to infection prevention measures among suspected chickenpox cases in Old Ayoma, Jasikan Municipality, Ghana, October 2021 | ||
| Variable | Frequency (N=10) | Per cent (%) |
|---|---|---|
| Events attended prior to rash onset | ||
| School | 6 | 60.0 |
| Family Gathering | 8 | 80.0 |
| Travel history | ||
| Yes | 1 | 10.0 |
| No | 9 | 90.0 |
| Previous experience of chickenpox | ||
| No | 10 | 100.0 |
| Face mask ownership | ||
| Yes | 2 | 20.0 |
| No | 8 | 80.0 |
| Face mask use | ||
| Yes | 2 | 20.0 |
| No | 8 | 80.0 |
| Access to toilet facility | ||
| Yes | 10 | 100.0 |
| Sharing of toilet facility | ||
| Yes | 8 | 80.0 |
| No | 2 | 20.0 |
| Access to bathhouse | ||
| Yes | 10 | 100.0 |
| Sharing of bathhouse | ||
| Yes | 9 | 90.0 |
| No | 1 | 10.0 |
| Handwashing facility | ||
| Yes | 5 | 50.0 |
| No | 5 | 50.0 |
| Handwashing facility usage | ||
| Yes | 4 | 40.0 |
| No | 6 | 60.0 |
Table 3: Exposure history and adherence to infection prevention measures among suspected chickenpox cases in Old Ayoma, Jasikan Municipality, Ghana, October 2021
Mawuli Gohoho1,2,3,&, Mavis Pearl Kwabla3, Isaac Annobil2, Gabriel Ofori2, Simon Klu2, Emmanuel Osei2, Joyce Berkumwin Der1,3, Anthony Zunuo Dongdem1,3, Gideon Kye-Duodu1,3, Fortress Yayra Aku1,3, Ernest Kenu1
1Ghana Field Epidemiology and Laboratory Training Programme, School of Public Health, University of Ghana, Legon- Accra, Ghana, 2Jasikan Municipal Health Directorate, Ghana Health Service, Jasikan, Ghana, 3Fred N Binka School of Public Health, University of Health and Allied Sciences, Hohoe, Ghana
&Corresponding author: Mawuli Gohoho, Disease Control and Surveillance Unit, Jasikan Municipal Health Directorate, Ghana Health Service, Jasikan, Ghana. Email: mawulikgohoho@gmail.com ORCID: https://orcid.org/0009-0001-4357-3509
Received: 11 Oct 2025, Accepted: 16 Jun 2026, Published: 18 Jun 2026
Domain: Infectious Disease Epidemiology
Keywords: Chickenpox, Disease outbreaks, Surveillance, Field epidemiology, Ghana
©Mawuli Gohoho et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Mawuli Gohoho et al., Chickenpox outbreak investigation in the Old Ayoma community, Jasikan Municipality, Ghana, 2021. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):101. https://doi.org/10.37432/jieph-d-25-00230
Introduction: Chickenpox is a vaccine-preventable disease caused by varicella-zoster virus. Vaccination against chickenpox has yet to be introduced into the routine immunization program in Ghana. On 26 October 2021, the Jasikan Municipal Health Directorate was notified by the Old Ayoma Health Centre of individuals presenting with blister-like rash and fever in the Old Ayoma community. We investigated to determine the magnitude and implement control and prevention measures.
Methods: We carried out a descriptive outbreak investigation to collect data on suspected chickenpox cases. We defined a suspected case as any person reporting with acute onset of blister-like rash, with or without fever, from 16 September to 9 December 2021 in the Old Ayoma community. We reviewed medical records and interviewed patients for active case searching. Using a questionnaire, we collected demographic, clinical and exposure variables of cases. Data were described by person, place and time.
Results: We identified 10 clinically diagnosed chickenpox cases; 5 (50%) through passive surveillance and 5 (50%) through active case search. The index case was seen on 7 October 2021. A non-resident who visited the community for a funeral on 18 September 2021 was identified as the likely source of infection. The overall attack rate was 1.1% (10/879). The most affected were males (90%), children under 15 years (70%) and pupils (60%). Seven (70%) of them resided within the community. All cases presented with maculopapulovesicular rash, and 80% reported fever. None had a history of chickenpox. On average, there were two household members per room and 19 pupils per class. All cases were managed and recovered without complications. Health education was provided to the community members. No new cases were reported within six weeks after the last reported case on 28 October 2021.
Conclusion: Males, children below 15 years, and pupils were the most affected. The outbreak was managed by isolation, treatment, and health education. We recommend intensified surveillance among pupils, children < 15 years, and males for a timely response.
Chickenpox (also known as Varicella) is an acute infectious disease primarily caused by the highly contagious varicella zoster virus, also known as human herpesvirus 3 (HHV-3) [1,2]. The virus is propagated from person-to-person primarily by direct contact with vesicular fluid or aerosolized virus-containing particles from skin lesions, and possibly by infected respiratory tract secretions [2]. Individuals are infectious from one to two days before rash onset until the lesions have crusted [3].
The disease typically presents with fever, fatigue, headache, or runny nose, followed by a red, spotty rash that develops into vesicles [4]. Although infection typically results in lifelong immunity and is self-limiting in most cases, it can lead to complications, especially in infants, pregnant women, adults, and immunocompromised individuals [4]. Because of its highly contagious nature, the attack rate among susceptible household contacts can exceed 85%. The case fatality rate in developed settings is 2–4 per 100,000, and hospitalization rates range from 2 to 6 per 100,000 population [2,5].
The incidence of varicella has decreased significantly in many parts of the world due to widespread vaccination programs [6]. A single dose provides around 76% to 85% protection, reaching up to 100% with two doses, with immunity lasting over a decade [7]. Despite this, chickenpox outbreaks continue to occur, particularly in communities with low vaccination coverage or among vulnerable groups [6]. For instance, routine childhood vaccination against chickenpox is not part of the Expanded Programme on Immunization in Ghana [8], leading to persistent risks and outbreaks in unvaccinated and susceptible communities. In tropical regions, chickenpox tends to occur more frequently in adults, where severity and risk of complications are higher [4].
On 26 October 2021, a registered general nurse at the Old Ayoma Health Centre notified the district of an increasing number of suspected chickenpox cases seen at the facility. Based on this notification, a team was constituted to confirm, characterize, identify the possible source, and respond to the suspected outbreak in the Old Ayoma community in the Jasikan Municipality of Ghana.
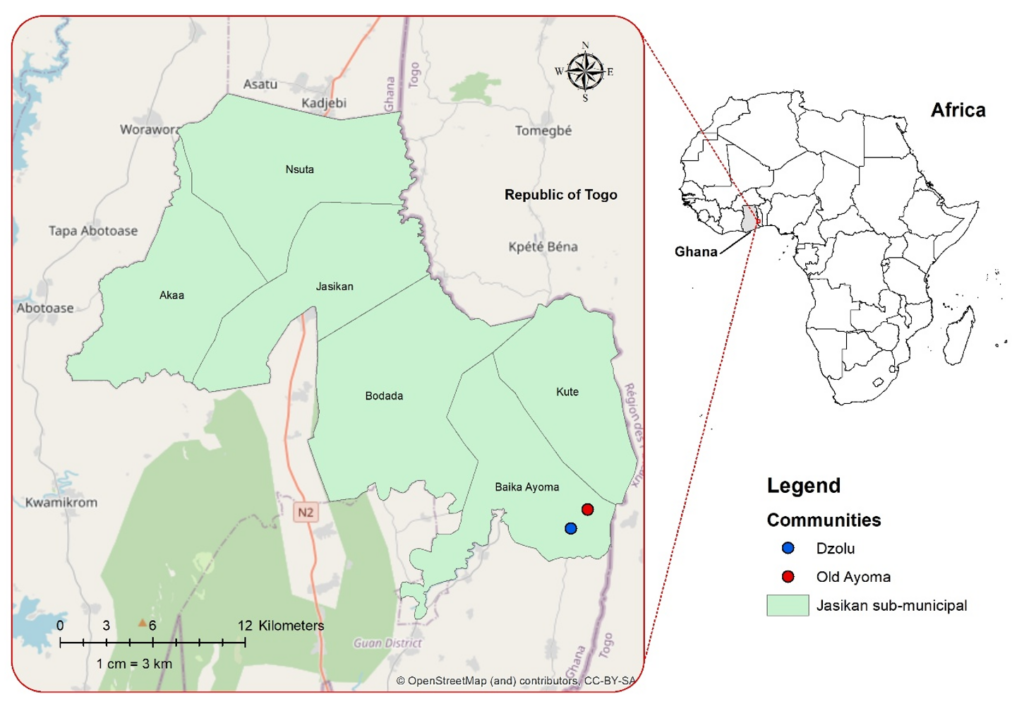
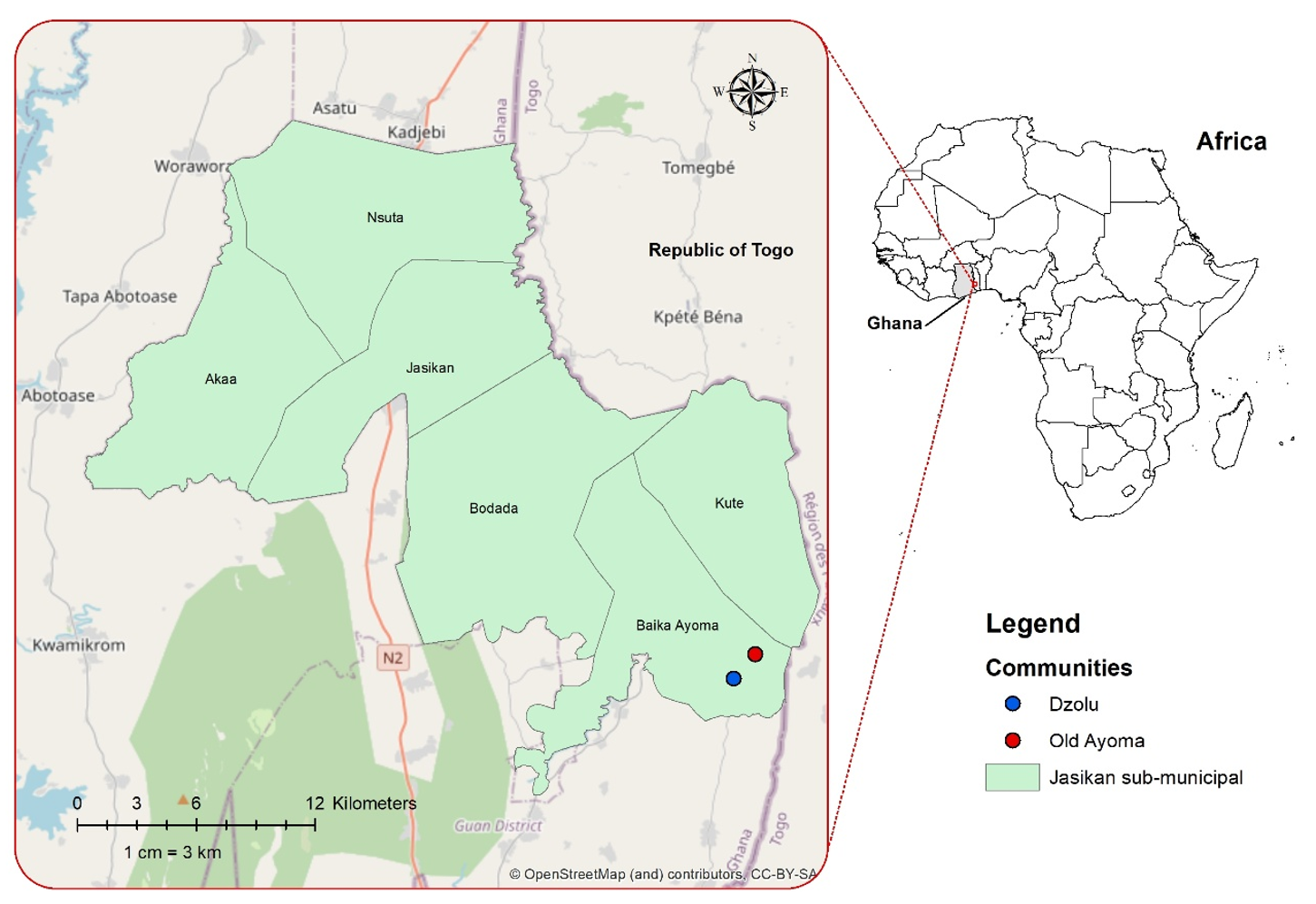
Outbreak investigation design and setting
We carried out a descriptive outbreak investigation in the Old Ayoma community where the outbreak occurred (Figure 1). The Old Ayoma community is part of the Baika Ayoma sub-municipality, one of six sub-municipalities in the Jasikan Municipality of Ghana. Of the 101 communities in the municipality, 18 are located within the Baika Ayoma sub-municipality. Old Ayoma has an estimated population of 879, comprising 429 males and 396 children aged below 15 years, with the remainder aged 15 years and above. The community has one basic school, which is supported by a School Health Education Programme (SHEP) coordinator who liaises with the nearby health facility to promote school health activities, health education, and early detection and reporting of health conditions among pupils. There is a health centre that provides primary healthcare needs and supports in public health surveillance activities as well.
Case definition and case finding
A suspected case of chickenpox was defined as any person with acute onset of a generalised maculopapulovesicular rash without other apparent causes [15], residing in the Old Ayoma community, with symptom onset between 16 September and 9 December 2021. As laboratory confirmation was not conducted, all suspected cases were assessed by healthcare professionals and counted as clinically diagnosed cases. A clinically diagnosed case was defined as a suspected case assessed and confirmed by a healthcare professional based on characteristic rash, presence of fever, epidemiologic links to other cases, and exclusion of other common vesicular illnesses such as measles or scabies. To confirm the outbreak and identify all suspected cases, we reviewed records from the Old Ayoma Health Centre, specifically the consulting room register and patient medical records. The team further visited households to search for additional suspected cases within the community.
Data collection and variables
We collected data primarily through questionnaires administered to suspected cases and key informant interviews, using KoboCollect for electronic data collection. Variables gathered included sociodemographic characteristics such as age, sex, household size, community of residence, and main occupation. Clinical presentations were documented, including signs and symptoms experienced. Disease severity was assessed based on the number of lesions and categorized as mild (<50), average (50–249), moderate (250–499), and severe (≥500) [9]. Exposure history covered attendance at events prior to rash onset and any recent travel. A previous history of chickenpox was also recorded. Information on adherence to infection prevention measures included ownership and use of face masks, availability and sharing of toilet and bathhouse facilities, and access to and usage of handwashing facilities. Only households with suspected cases were visited to identify additional suspected cases and gather detailed case-level information.
We conducted in-person key informant interviews using a semi-structured interview guide. The participants included two healthcare workers at the Old Ayoma Health Centre, the SHEP coordinator, and a community based surveillance volunteer. These individuals were purposively selected to provide information in relation to the suspected cases relevant to the outbreak. Findings from these interviews were used to verify case details and support the description of outbreak dynamics.
Data analysis
Data collected using the KoboCollect tool were exported, cleaned, and analysed using Microsoft Excel and STATA version 16 (StataCorp LLC, College Station, Texas, USA). Descriptive analysis was conducted to characterize the outbreak by person, place, and time. Categorical variables were summarized using frequencies and percentages, while continuous variables were summarized using means, standard deviations (SD), range, median, and interquartile range (IQR). Findings were presented in tables and graphs, including an epidemic curve to visualize the distribution of cases over time. The source of the outbreak was further assessed by interpreting the epidemic curve alongside responses from questionnaires and key informant interviews to identify the exposure period and potential index cases.
Ethical considerations
This investigation was conducted as part of a public health response to a suspected chickenpox outbreak and did not require ethical clearance from an institutional review board. However, administrative approval was obtained from the Jasikan Municipal Health Directorate. Verbal consent was obtained from each participant with a clear explanation of the investigation’s purpose, the type of questions to be asked, and the voluntary nature of participation. All data collected were stored on a password-protected computer and accessed only by the investigation team to maintain confidentiality.
Descriptive epidemiology
Ten suspected chickenpox cases were recorded in Old Ayoma, Jasikan Municipality of Ghana. These cases were identified through both passive 5 (50%) and active 5 (50%) surveillance. Of the 10 suspected cases, 9 (90%) were males, and 7 (70%) were children under 15 years, with a median age of 9.5 years (IQR: 5.5–15.5 years). Seven (70%) resided in Old Ayoma, while the remaining were from the neighbouring community called Dzolu. Apart from one farmer and one health worker, two cases were preschool children, and six (60%) were pupils. These cases lived in households with a median size of eight persons per household (IQR: 3.5–10) (Table 1). The overall attack rate was 1.1% (10/879, 95% CI: 0.5–2.1%). Sex-specific attack rates were 2.1% (9/429, 95% CI: 1.0–3.9%) for males and 0.2% (1/450, 95%CI: 0.006–1.2%) for females. Age-specific attack rates were 1.8% (7/396, 95% CI: 0.7–3.6%) for those below 15 years and 0.5% (3/483, 95% CI: 0.1–1.8%) for those 15 years and above. All cases presented with generalized rash, while eight (80%) had fever. Other reported symptoms included loss of appetite (70%), muscle pains (60%), headache (50%), abdominal pains (40%), joint pains (40%), tiredness (40%), and discomfort (20%). None of the cases reported runny nose. The mean rash duration was 4.2 (± 1.31) days (Table 2). Rash locations included the head and face (90%), arms (90%), and inside the mouth (20%). The severity of the rash was moderate in 4(40%), average in 3(30%), mild in 2 (20%), and severe in one (10%) (Table 2).
Chronology of events, transmission dynamics, and source of outbreak
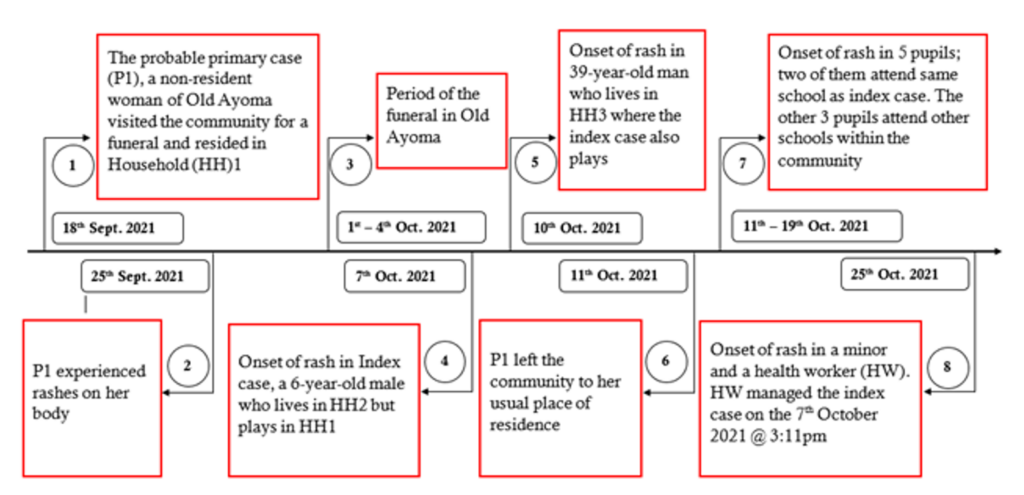
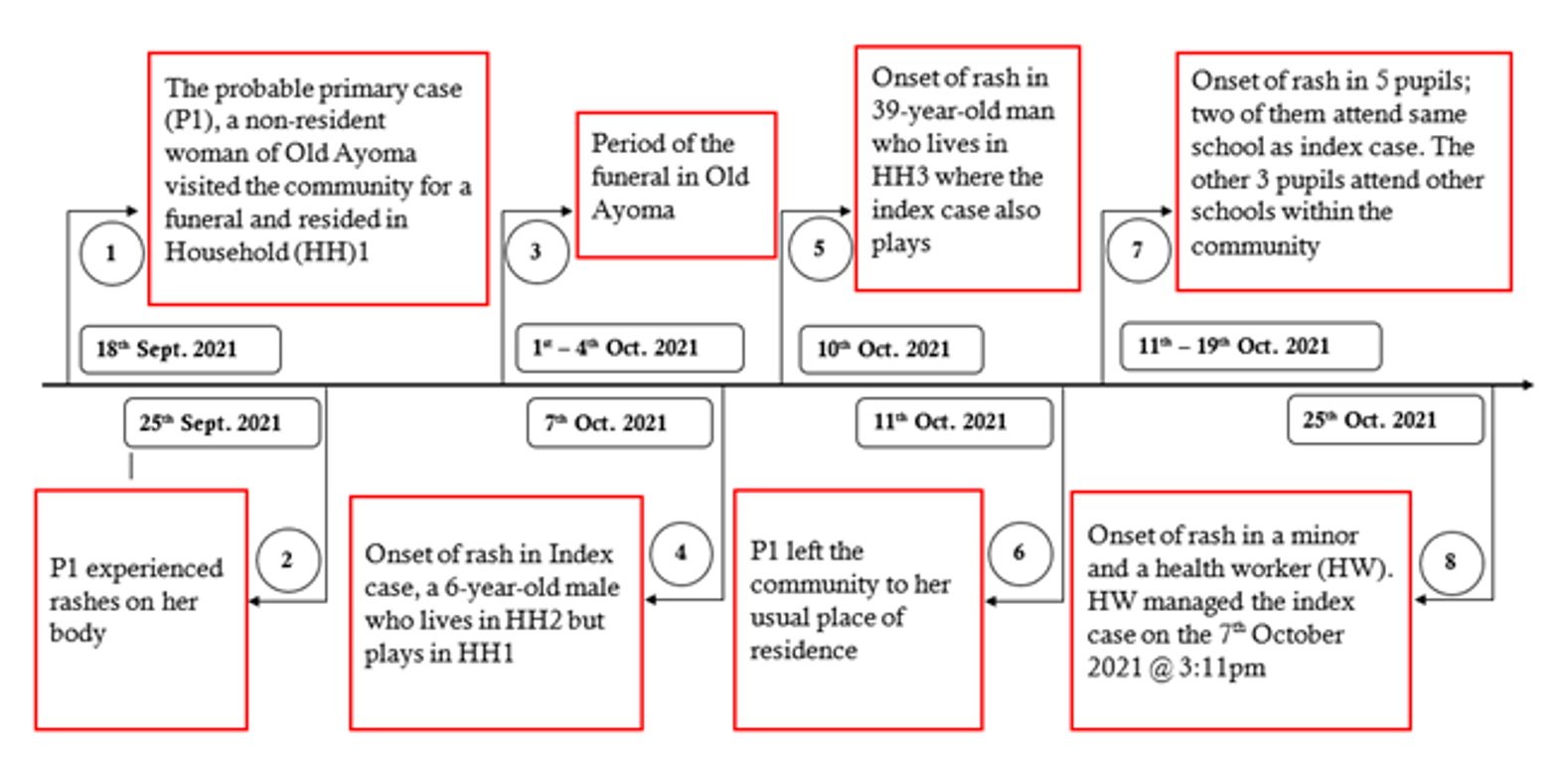
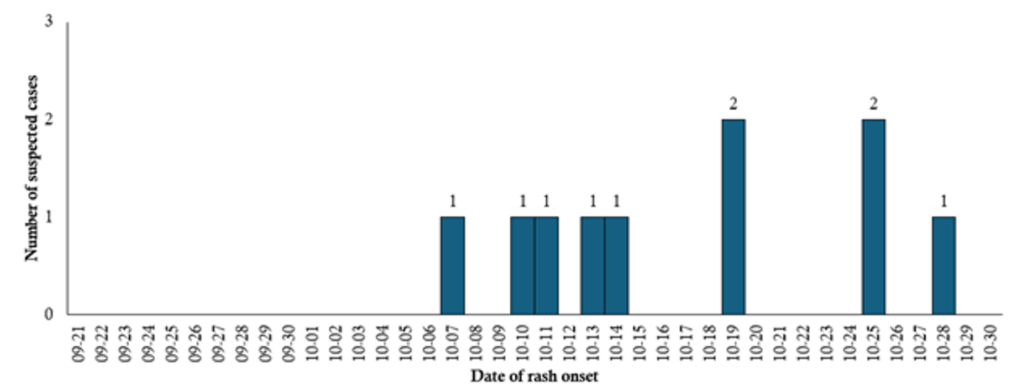
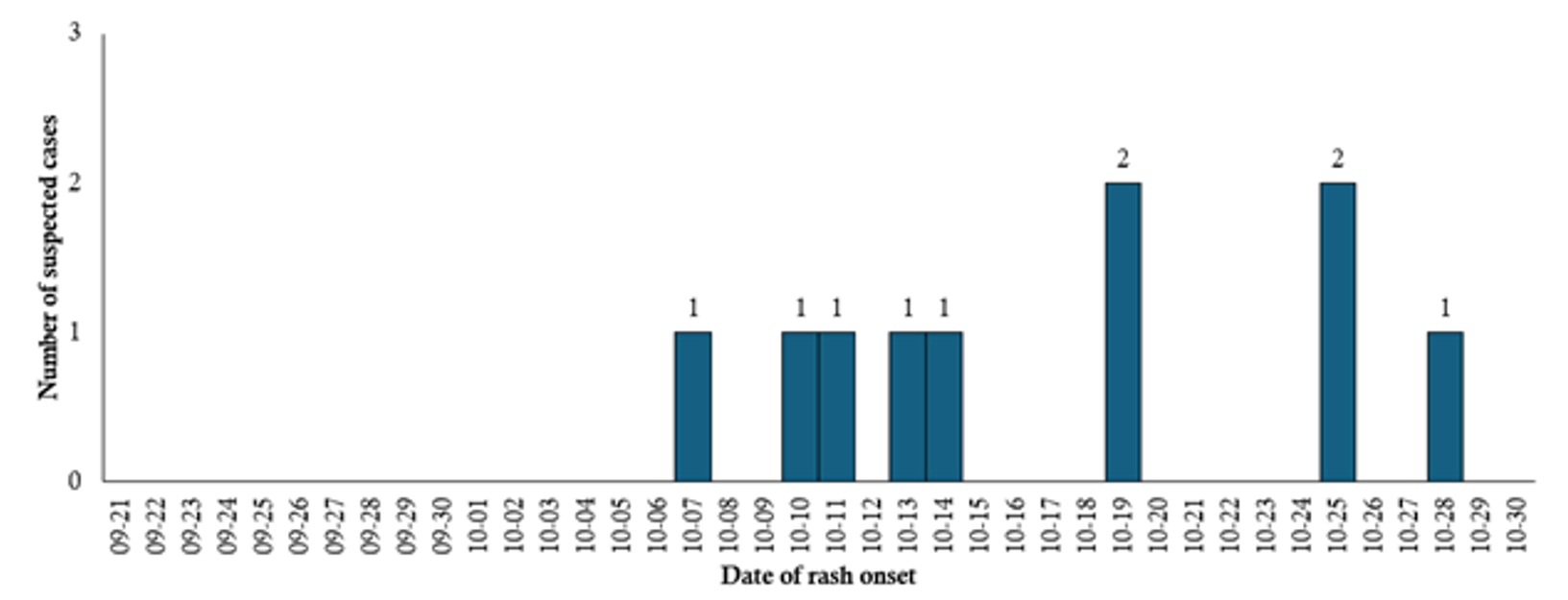
A non-resident woman identified as the probable primary case (P1) arrived in Old Ayoma on 18 September 2021 to attend a funeral and resided in household (HH) 1 (Figure 2). On 25 September 2021, P1 experienced rashes on her body. Between 1 and 4 October 2021, the funeral was held in Old Ayoma. On 7 October 2021, the index case, a 6-year-old boy who lives in HH two but frequently plays in HH 1, developed a rash (Figure 3). The average number of persons per room in affected households was two. P1 left the community to return to her usual place of residence on 11 October 2021. Based on the timeline and exposure history, P1 was identified as the likely source of the outbreak.
On 10 October 2021, a 39-year-old man who lives in HH 3, where the index case also plays, developed a rash (Figure 3). Between 11 and 19 October 2021, five pupils developed the rash. Two of them attended the same school as the index case, while the other three were from different schools within the community and indicated participation in a family gathering before the rash developed. In the schools attended by affected children, the average class size was 19 pupils. On 25 October 2021, two additional cases developed rashes: one was a preschool-aged child, and the other was a health worker who had managed the index case at 3:11 pm on 7 October 2021 (Figure 2).
Exposure history and adherence to infection prevention measures
Prior to rash onset, 6 (60%) of the cases had attended school, and 8 (80%) had attended a family gathering. One case (10%) had a history of travel outside the municipality. None of the cases reported any previous history of chickenpox (Table 3). Among the 10 cases, only 2 (20%) owned face masks, and the same number reported using them. All cases had access to toilet and bathhouse facilities, though 8 (80%) and 9 (90%) shared these, respectively. Half (50%) had access to handwashing facilities. Overall, four (40%) reported using them (Table 3).
Case management and outcomes
Among all cases identified, four (40%) were managed within the health facility under observation, while the rest were managed at home (Table 2). Treatment given was focused on symptomatic relief and supportive care. No complications were recorded among the cases. All 10 cases fully recovered without sequelae, and no deaths were reported.
Public health actions and outbreak control measures
Following the investigation, we implemented targeted public health interventions to prevent further spread. The team provided education to health workers and the community based surveillance volunteer in the community on the signs, symptoms, transmission, and reporting process for suspected chickenpox cases. Household visits were conducted to sensitize residents verbally on the disease and encourage prompt reporting of symptoms. As most of the cases were linked to a school, the team had a face-to-face engagement with the SHEP coordinator on the importance of school-based surveillance and early case identification. Additionally, the Municipal Health Directorate provided the health facility with essential drugs and non-drug consumables to support effective case management. No new cases were reported within 6 weeks after the last reported case on 28 October 2021.
This outbreak investigation identified 10 clinically diagnosed chickenpox cases in the Old Ayoma community of the Jasikan Municipality of Ghana. The low overall attack rate observed suggests limited spread within the community. Although household attack rates for chickenpox can exceed 85%, such high transmission was not observed in this outbreak, likely due to the small number of susceptible individuals. The index case was linked to a non-resident visitor, with subsequent cases arising in schools and households. The outbreak predominantly affected males and children under 15 years, consistent with findings from Nepal [10] and India [11] where the majority of cases were school-aged children. Other outbreaks have involved adults, such as in a psychiatric facility in Riyadh [12] and among asylum seekers in Italy [13]. In Ghana, varicella vaccination is not included in the routine childhood immunization schedule [8]. This predisposes many individuals, especially children and young adults to infection due to a lack of prior immunization or exposure.
All suspected cases presented with generalized rash, and four-fifths had fever. Other symptoms such as loss of appetite, muscle pains, and headache were commonly reported. The location and duration of the rash observed were consistent with reports from other countries [2,10], which described a generalized maculopapulovesicular rash with lesions often appearing on the scalp, trunk, and oropharynx. The outbreak began after a non-resident woman, the probable primary case, developed a rash during a funeral visit to the community. A 6-year-old boy who played frequently in her household developed a rash two weeks later, followed by additional cases among pupils and a health worker. Similar transmission through close contact and school exposure was noted in Nepal [10], India [11], and Canada [2], where school environments and shared living spaces contribute substantially to facilitating transmission. The observation that the probable primary case was a non-resident individual attending a communal event such as a funeral suggests the potential for imported cases to initiate outbreaks in susceptible populations, similar to the imported cases identified in the Italy asylum seeker outbreak [13].
We found that only one fifth of cases had face masks, and half of them had access to handwashing facilities, while most shared toilets and bathhouse facilities. Although the small number of cases limits the ability to directly link these conditions to transmission in this outbreak, such factors are known to increase the risk of household and community spread [2,10]. All 10 cases recovered without complications, and no deaths were recorded. This is consistent with reports from Nepal [10] and Italy [13], where an uncomplicated disease course was observed. The absence of complications is typical in healthy children but not in adults or immunocompromised individuals, as emphasized in CDC and Maryland outbreak guidelines [4]. Public health interventions included health education for community based surveillance volunteers, sensitization visits to households, and collaboration with SHEP coordinator. These measures supported case isolation and timely reporting. This approach aligns with established infectious disease outbreak control guidelines, which recommend early case identification, public awareness, and exclusion of infectious cases from school or work until lesions crust [4]. Although formal exclusion from school or work was not implemented, cases were verbally encouraged to stay home until lesions crusted to minimize further transmission.
The outbreak was identified and managed solely through clinical diagnosis. No laboratory confirmation was conducted. This limits the definitive classification of cases. Previous studies used Polymerase Chain Reaction for case confirmation [2,14], and the lack of such diagnostic testing in the present study constitutes a notable limitation. Nonetheless, the case definition used is congruent with standard clinical definitions for chickenpox, and the epidemiologic links support the diagnosis [15]. Differential diagnoses were also considered and excluded based on clinical features and epidemiologic links. However, the small number of suspected cases limits statistical power, rendering inferential analyses inappropriate and restricting meaningful comparisons between subgroups.
The chickenpox outbreak in Old Ayoma was confirmed based on clinical presentation and person-to-person spread following exposure to a probable imported case. The outbreak affected mainly males and children under 15 years, with transmission linked to schools, households, and community gatherings. The absence of prior immunity, either through vaccination or previous infection, likely contributed to the susceptibility of the affected population. All cases recovered without complications. The Ghana Health Service and Ghana Education Service should collaboratively intensify surveillance among pupils, children under 15 years, and males, and reinforce community and school-based education on chickenpox prevention and early reporting.
What is already known about the topic
What this study adds
We acknowledge the Jasikan Municipal Health Management Team, the staff of Old Ayoma Health Centre, and the Community-Based Surveillance Volunteers for their support during the investigation and response to the outbreak. Appreciation also goes to the Fred N Binka School of Public Health of the University of Health and Allied Sciences, the MPhil Applied Epidemiology Cohort 3, and the Ghana Field Epidemiology and Laboratory Training Programme for their guidance and contribution throughout the process.
Mawuli Gohoho led the investigation and response to the outbreak and drafted the manuscript. Gabriel Ofori, Simon Klu and Emmanuel Osei provided technical support during the outbreak investigation and edited the manuscript. Mavis Pearl Kwabla, Joyce Der, Anthony Zunuo Dongdem, Gideon Kye-Duodu and Fortress Yayra Aku provided technical guidance during the outbreak investigation, data analysis, edited and reviewed the manuscript. Isaac Annobil supervised the outbreak investigation and response and reviewed the manuscript. Ernest Kenu edited and reviewed the manuscript. All the authors read and approved the manuscript for publication.
| Table 1: Sociodemographic characteristics of chickenpox cases, Old Ayoma, Jasikan Municipality, Ghana, October 2021 | ||
| Variable | Frequency (N=10) | Per cent (%) |
|---|---|---|
| Median age in years | 9.5 (IQR: 5.5, 15.5) | |
| Age group (years) | ||
| Below 15 | 7 | 70.0 |
| 15 and above | 3 | 30.0 |
| Sex | ||
| Male | 9 | 90.0 |
| Female | 1 | 10.0 |
| Community of residence | ||
| Dzolu | 3 | 30.0 |
| Old Ayoma | 7 | 70.0 |
| Median household size | 8 (IQR: 3.5, 10) | |
| Main occupation | ||
| Pupil | 6 | 60.0 |
| Preschool child | 2 | 20.0 |
| Farmer | 1 | 10.0 |
| Health worker | 1 | 10.0 |
| Table 2: Clinical presentations of suspected chickenpox cases in Old Ayoma, Jasikan Municipality, Ghana, October 2021 | ||
| Variable | Frequency (N=10) | Per cent (%) |
|---|---|---|
| Surveillance type | ||
| Active | 5 | 50.0 |
| Passive | 5 | 50.0 |
| Signs and symptoms* | ||
| Rash | 10 | 100.0 |
| Fever | 8 | 80.0 |
| Loss of appetite | 7 | 70.0 |
| Muscle pains | 6 | 60.0 |
| Headache | 5 | 50.0 |
| Abdominal pains | 4 | 40.0 |
| Joint pains | 4 | 40.0 |
| Tiredness | 4 | 40.0 |
| Discomfort | 2 | 20.0 |
| Runny nose | 0 | 0.0 |
| Duration of rash | ||
| Mean ± S.D (range) days | 4.2 ± 1.31 (3,7) | |
| Location of rash* | ||
| Head and face | 9 | 90.0 |
| Arms | 9 | 90.0 |
| Trunk | 6 | 60.0 |
| Legs | 6 | 60.0 |
| Inside mouth | 2 | 20.0 |
| Severity of rash | ||
| Mild | 2 | 20.0 |
| Average | 3 | 30.0 |
| Moderate | 4 | 40.0 |
| Severe | 1 | 10.0 |
| Case management location | ||
| Managed within health facility (under observation) | 4 | 40.0 |
| Managed at home | 6 | 60.0 |
| Case observation period among facility-managed cases (n=4) | ||
| Mean ± S.D (range) days | 2 ± 1.42 (1,4) | |
| * Multiple responses; S.D = Standard deviation | ||
| Table 3: Exposure history and adherence to infection prevention measures among suspected chickenpox cases in Old Ayoma, Jasikan Municipality, Ghana, October 2021 | ||
| Variable | Frequency (N=10) | Per cent (%) |
|---|---|---|
| Events attended prior to rash onset | ||
| School | 6 | 60.0 |
| Family Gathering | 8 | 80.0 |
| Travel history | ||
| Yes | 1 | 10.0 |
| No | 9 | 90.0 |
| Previous experience of chickenpox | ||
| No | 10 | 100.0 |
| Face mask ownership | ||
| Yes | 2 | 20.0 |
| No | 8 | 80.0 |
| Face mask use | ||
| Yes | 2 | 20.0 |
| No | 8 | 80.0 |
| Access to toilet facility | ||
| Yes | 10 | 100.0 |
| Sharing of toilet facility | ||
| Yes | 8 | 80.0 |
| No | 2 | 20.0 |
| Access to bathhouse | ||
| Yes | 10 | 100.0 |
| Sharing of bathhouse | ||
| Yes | 9 | 90.0 |
| No | 1 | 10.0 |
| Handwashing facility | ||
| Yes | 5 | 50.0 |
| No | 5 | 50.0 |
| Handwashing facility usage | ||
| Yes | 4 | 40.0 |
| No | 6 | 60.0 |