Research | Open Access | Volume 9 (Suppl 12): Article 6 | Published: 28 May 2026

Views: 884
Menu, Tables and Figures
| Variables | STUDY COMMUNITIES | ||||
|---|---|---|---|---|---|
| EHINOGBE | IDASEN | IFON | IJAGBA | IJEBU | |
| Sex | |||||
| Female | 68 (53.5%) | 13 (54.2%) | 67 (54.9%) | 51 (44.7%) | 73 (60.3%) |
| Male | 59 (46.5%) | 11 (45.8%) | 55 (45.1%) | 63 (55.3%) | 48 (39.7%) |
| Age (years) | |||||
| 2 to 5 | 10 (9.9%) | 0 (0.0%) | 5 (4.1%) | 10 (8.8%) | 10 (8.3%) |
| 6 to 10 | 14 (11.0%) | 5 (20.8%) | 4 (3.3%) | 23 (20.2%) | 16 (13.2%) |
| 11 to 17 | 24 (18.9%) | 1 (4.2%) | 21 (17.2%) | 25 (21.9%) | 32 (26.4%) |
| 18 to 50 | 62 (48.8%) | 11 (45.8%) | 59 (48.4%) | 44 (38.6%) | 50 (41.3%) |
| Above 50 | 17 (13.4%) | 7 (29.2%) | 33 (27.0%) | 12 (10.5%) | 13 (10.7%) |
| Total | 127 | 24 | 122 | 114 | 121 |
| Variables | ILALE | IPELE | ISUADA | IYERE | OGBESE |
| Sex | |||||
| Female | 42 (50.6%) | 28 (51.9%) | 17 (51.5%) | 44 (54.3%) | 153 (61.4%) |
| Male | 41 (49.4%) | 26 (48.1%) | 16 (48.5%) | 37 (45.7%) | 96 (38.6%) |
| Age (years) | |||||
| 2 to 5 | 9 (10.8%) | 3 (5.6%) | 2 (6.1%) | 4 (4.9%) | 18 (7.2%) |
| 6 to 10 | 11 (13.3%) | 13 (24.1%) | 6 (18.2%) | 6 (7.4%) | 41 (16.5%) |
| 11 to 17 | 18 (21.7%) | 10 (18.5%) | 8 (24.2%) | 8 (9.9%) | 59 (23.7%) |
| 18 to 50 | 37 (44.6%) | 19 (35.2%) | 13 (39.4%) | 37 (45.7%) | 114 (45.8%) |
| Above 50 | 8 (9.6%) | 9 (16.7%) | 4 (12.1%) | 26 (32.1%) | 17 (6.8%) |
| Total | 83 | 54 | 33 | 81 | 249 |
Table 1: Gender and Age Groups of Participants across the Study Communities
| Age (years) | Number of participant | Anti-LASV IgG result | Baseline | 6 months | 12 months | 18 months | 24 months |
|---|---|---|---|---|---|---|---|
| 2 to 5 | 71 | Negative | 57 | 2 | 46 | 42 | 40 |
| Positive | 14 | 53 | 21 | 23 | 23 | ||
| Indeterminate | 0 | 16 | 4 | 6 | 8 | ||
| 6 to 10 | 139 | Negative | 89 | 83 | 77 | 73 | 69 |
| Positive | 48 | 50 | 53 | 55 | 53 | ||
| Indeterminate | 2 | 6 | 9 | 11 | 17 | ||
| 11 to 17 | 206 | Negative | 128 | 121 | 120 | 103 | 104 |
| Positive | 75 | 69 | 79 | 85 | 75 | ||
| Indeterminate | 3 | 16 | 7 | 18 | 27 | ||
| 18 to 50 | 446 | Negative | 251 | 222 | 222 | 201 | 202 |
| Positive | 187 | 178 | 190 | 193 | 172 | ||
| Indeterminate | 8 | 46 | 34 | 52 | 72 | ||
| Above 50 | 146 | Negative | 81 | 71 | 69 | 68 | 63 |
| Positive | 63 | 63 | 62 | 62 | 58 | ||
| Indeterminate | 2 | 12 | 15 | 16 | 25 | ||
| Statistical significance | LR=19.743 P=0.011 | LR=25.469 P=0.001 | LR=15.233 P=0.055 | LR=7.766 P=0.457 | LR=6.336 P=0.610 | ||
Table 2: Anti-LASV IgG Results at baseline and follow-up periods across different age groups of the cohort
Adetumi Adetunji Subulade1,2,&, Oladele Oluwafemi Ayodeji1, Chukwuyem Abejegah1, Austine Osagbaekhoe1, Akinola Nelson Adedosu3, Isaac Ihinmikhaye1, Gloria Abimbola Awe1, Olufunke Gbenga-Ayeni3, Johnson Etafo3, Ronke Irene3, Winifred Ingbian3, MacDonald Onyechi3, Grace Temitope Olubayo1, Adesola Omowumi Kareem1, Olufunmilayo Yetunde Adesida1, Liasu Adeagbo Ahmed4, Adebola Olayinka5, Jan Kamji5, Henshaw Mandi6
1Infectious Disease & Research Unit, Community Health Department, Federal Medical Centre, Owo, Ondo State, Nigeria, 2Department of Public Health, Achievers University, Owo, Ondo State, Nigeria, 3Infectious Disease and Research Centre Molecular Laboratory, Federal Medical Centre, Owo, Ondo State, Nigeria, 4Family Medicine Department, Federal Medical Centre, Owo, Ondo State, Nigeria, 5Nigeria Centre for Disease Control and Prevention (NCDC), Abuja, Nigeria, 6Coalition for Epidemic Preparedness Innovation (CEPI)
&Corresponding author: Adetumi Adetunji Subulade, Infectious Disease & Research Unit, Community Health Department, Federal Medical Centre, Owo, Ondo State, Nigeria, Email: tunjigold2@gmail.com ORCID: https://orcid.org/0000-0001-7019-4814
Received: 16 Oct 2025, Accepted: 27 May 2026, Published: 28 May 2026
Domain: Infectious Disease Epidemiology
Keywords: Lassa fever, Age-Specific, Seroprevalence, Anti-Lassa virus IgG
©Adetumi Adetunji Subulade et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Adetumi Adetunji Subulade et al., Age-specific seroprevalence trend of anti-Lassa virus antibodies: A prospective cohort study in Ondo State, Nigeria. Journal of Interventional Epidemiology and Public Health. 2026; 9(Suppl 12):6. https://doi.org/10.37432/jieph-d-25-00239
Introduction: Lassa fever infection is endemic in West Africa, and it commonly occurs in humans when there is exposure to infected excreta, urine or remains of infected Mastomys natalensis. Pattern of Lassa fever virus (LASV) epidemiological behaviour is essential for the development of appropriate targeted intervention through a vaccine; hence, this study determined the age-specific serological prevalence among a prospective cohort in Ondo State, Nigeria.
Method: This was a 24-month prospective cohort study conducted in ten communities in three Local Government Areas of Ondo State. Samples were collected from 1008 enrolled participants at 6 monthly intervals of 0 (baseline), 6, 12, 18 and 24 months following informed consent. The samples were analysed for anti-Lassa virus (anti-LASV) IgG using ELISA.
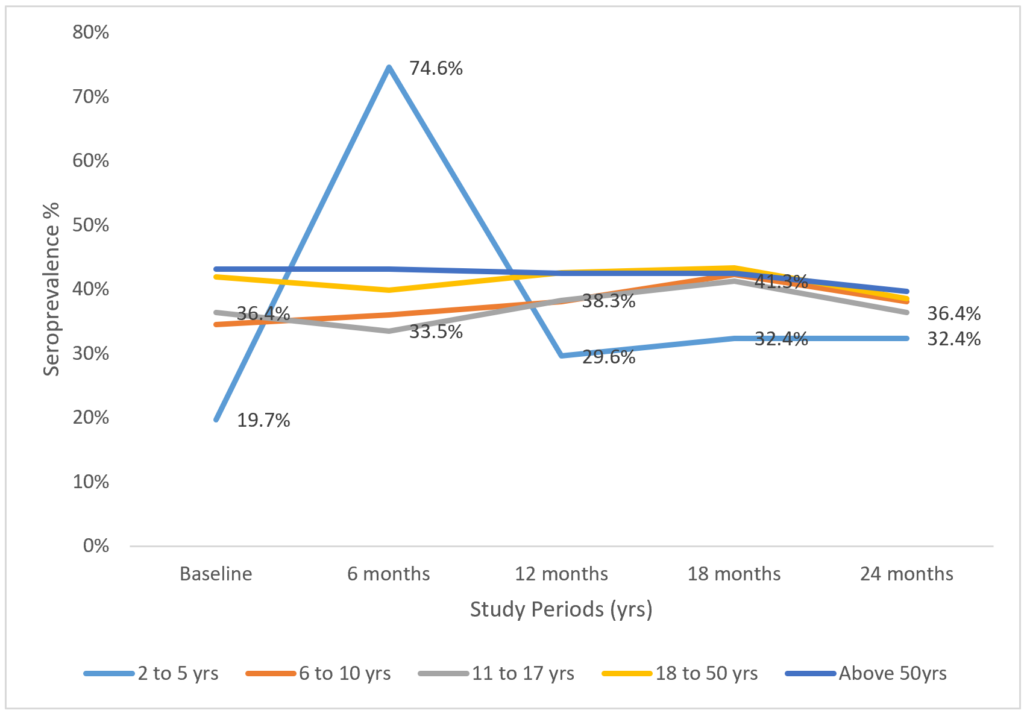
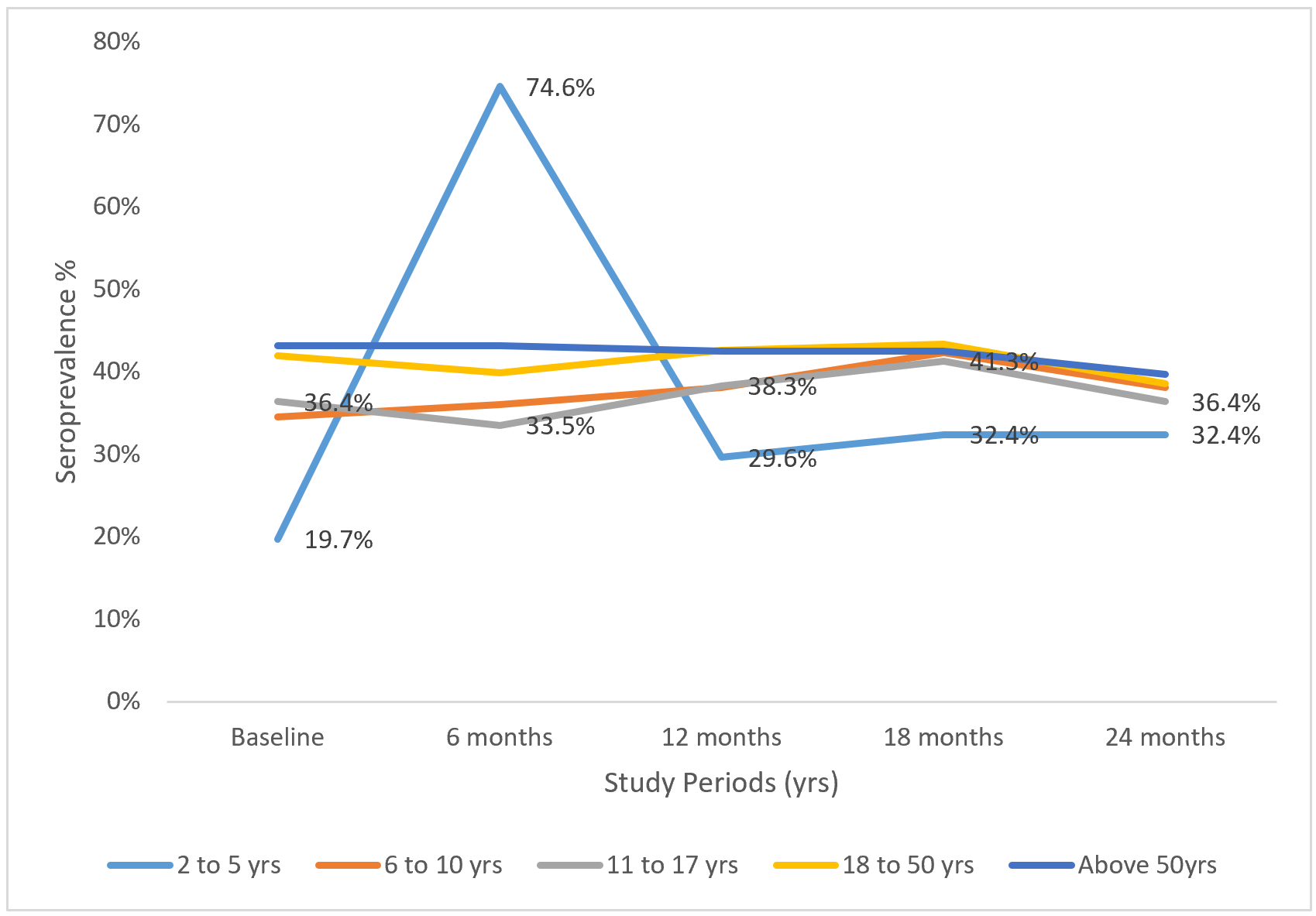
Results: The seroprevalence of anti-LASV IgG of the participants showed an upward trend with 35.1% at baseline, which slightly increased to 37.0% at the 24th month. In the age-specific trend, the lowest baseline seroprevalence of 19.7% was observed among children of 2 to 5years, followed by 34.5% for 6 to 10years and 36.4% for adolescents. The seroprevalence among children aged 2 to 5 years steadily increased to the highest among other age groups to 74.6% at 6 months, after which it dropped to 29.6% at 12 months, below other age groups and minimally increased but remained below other age groups to 32.4% at 24 months. Age 50 years and above had the highest seroprevalence (43.2%) at baseline and remained fairly constant till month 24, when it decreased to 39.7%. The seroprevalence of other age groups was almost constant throughout the study. The seroconversion risk from the baseline was 10.1%.
Conclusion: The age-specific seroprevalence trend of anti-LASV IgG has significant importance in Lassa fever prevention and control. The low prevalence among adolescents and children shows a large population of vulnerable age-groups who are still at risk of contracting the disease later in life, and their vaccination before substantial exposure is likely to have a long-term benefit. The gradual increase in seroprevalence with older age indicates a cumulative exposure pattern and sustained transmission in an endemic environment with recurrent outbreaks. Vaccination coverage of adults may reduce overall transmission.
The Lassa virus belongs to Arenaviridae family and causes Lassa fever, which is an acute viral hemorrhagic illness that continues to pose a serious threat to public health in West Africa region, especially in Nigeria, where the disease is endemic [1,2]. Although human-to-human transmission of the virus does occur, particularly in healthcare settings, the main method of infection is exposure to the urine or feces of infected multimammate rat, the Mastomys natalensis [3]. Lassa fever outbreaks occur annually in the endemic region, and have been consistently concentrated in Ondo State, Nigeria, especially in Owo town. It also affects other states in the country, including Edo, Bauchi, Ebonyi, and Taraba states. The disease is a major contributor to the national disease burden [4,5].
Serology of Lassa fever involves the detection of antibodies to the virus that show previous exposure to the Lassa virus infection [6]. The human immune system produces immunoglobulin M (IgM) and immunoglobulin G (IgG) antibodies after infection. The IgM appears early in the blood within the first week of exposure to the viral infection, which is referred to as an acute or recent infection, while IgG develops later, beyond the first week, and persists for months and for years in some instances [7,8]. This serves as the marker of previous exposure, which can confer immunity on individuals with the antibodies [7]. The mainstay of laboratory diagnosis of these antibodies involves enzyme-linked immunosorbent assays (ELISA) in the Nigerian setting, which detects the antibodies in serum samples [9].
The antibody testing of the serological status of Lassa fever endemic communities is crucial in the understanding of the epidemiology of Lassa fever and the provision of adequate public health control of transmission and interventions [8,10,11]. The population-based anti-LASV antibody serology assessment in a Lassa fever infection endemic setting can assist in determining the level of exposure to the transmission of the virus and identification of risk factors of transmission as related to different age groups, environment, occupation, and other sociodemographic factors [5,12,13]. The identification of high anti-LASV IgG antibody prevalence in communities indicates a long-term transmission of the virus and shows the potential for transmission from asymptomatic or mildly infected individuals, which is common in an endemic setting [10]. Serological studies are essential in the research and development of vaccines, as these provide an understanding of the immune responses of the population to an infection and the immunity trend over time. In the interpretation of serology results, there is however, a possibility of cross-reactivity with other arenaviruses and variability in immune response of different individuals based on various factors [7,10]. These could be a limitation to serological interpretation and surveillance efforts.
Determining the seroprevalence of anti-Lassa virus antibodies in various age groups is essential for identifying exposure trends and guiding public health initiatives, especially in the development of a Lassa fever vaccine. Previous serological surveys reported that seroprevalence rates differed by age, occupation, and environmental exposure [14,15]. Nevertheless, the information on age-specific seroprevalence patterns in high-burden areas, such as Ondo State, is still limited and often derived from cross-sectional studies that only provide a snapshot of exposure and fail to reflect the temporal dynamics of Lassa fever infection incidence. This prospective cohort study aimed to bridge this gap by examining the age-specific seroprevalence trend of anti-Lassa virus antibodies among residents of Ondo State.
The objective of this study was to determine the age-specific serological prevalence of anti-LASV IgG among a prospective cohort in Ondo State, Nigeria. This will improve the knowledge of exposure risks to LASV and its transmission pattern and guide focused surveillance and preventive measures in vaccine development.
The study was conducted across three Local Government Areas (LGAs), Ose, Owo and Akure North in Ondo State, Nigeria. The state is in southwestern Nigeria, bounded by Edo State on the east, Kwara and Kogi States on the north, Delta on the southeast, and Osun and Ogun States on the west, and by the Bight of Benin of the Atlantic Ocean on the south. The town is located at longitude 7.19890N and latitude 5.59320E. The state is one of the oil-producing states, and the major occupations are civil service and farming. Ondo State has two primary weather seasons determined by the tropical pattern, which are rain season from April to October and the dry season from November to March annually. The dry season has been reported as the period of consistent annual outbreaks for Lassa fever [5].
Study design
A prospective cohort study design was used to enrol and successfully follow up the cohort of 1008 participants for 24 months from November 2020 to November 2022.
Study population
The study population were the people resident in ten communities with a relatively high risk of LASV infection across three LGAs in Ondo state. These communities have similar sociocultural characteristics but are geographically separated. They were selected based on available data on confirmation of LASV in the state and the communities included Ehinogbe, Idasen, Iyere, Ipele Isuada, Ijebu and Ilale from Owo LGA; Ifon and Ijagba/Imoru from Ose LGA; and Ogbese from Akure North LGA.
Inclusion criteria
Exclusion criteria
Sample size
The sample size was calculated by using the Wilson score interval method table [16]. Sample size for different precision levels was calculated considering the seroprevalence level between 1% and 50%. The seroprevalence proportion of LASV infection was estimated at 52%, with a 95% confidence interval (CI) of 46.9 – 53.1 for seroprevalence proportion of 1/100 person-years [16]. A sample size of 1,000 subjects was hence determined and distributed among the selected communities with a probability proportional to their respective population sizes. In consideration of possible baseline seropositivity because of the endemicity of LASV infection, and attrition of participants during the follow-up study, 1100 were recruited. However,1008 participants successfully completed the study, which was about a 92% retention rate.
Sampling technique
A two-stage cluster sampling method was used for random selection of communities and households for the study in three LGAs, namely Owo, Akure North, and Ose. These were the LGAs with high prevalence of Lassa fever confirmation PCR test results in Ondo State, and based on the prevalent spread of the PCR results, one community was selected in Akure North, seven communities in Owo LGA, and two communities in Ose LGA. The first cluster was the selection of communities with the LGAs using the positive LASV PCR prevalence, and the second cluster was the selection of households within the selected communities by convenience sampling from the randomly selected starting point within the community. A household was defined as persons living in the same dwelling, sharing meals and sleeping quarters. In the first cluster stage, Ogbese community was selected in Akure North, Ehinogbe, Idasen, Iyere, Ipele, Isuada, Ijebu, and Ilale communities in Owo LGA, and Ifon and Ijagba-Imoru communities in Ose LGA.
In the second cluster stage, the list of all households was obtained from the LGAs using the most recent census conducted in 2020 for the National Program on Immunisation (NPI) in the state. The number of households was proportionally allocated to the ten selected communities. In selecting households in each community, a central point within the community was used to randomly select the direction of the starting point. This was done by spinning a pen, and the direction of the tip of the pen was used as the starting point. All the dwellings in each community were numbered in a clockwise direction from the dwelling at the starting point to the last house in the community. One household was then selected from each house. In every house with more than one household, simple random sampling was used to select a household. The individuals within each selected household who fulfilled the study eligibility criteria and gave consent were selected for the study enrollment. This process was continued until the total sample size was achieved for each selected community.
Data collection procedure
The pre-study activities conducted included key stakeholders’ engagement in the communities, community sensitisation, mapping of selected communities, selection of community liaison officers (CLOs), and recruitment and training of study personnel. A structured questionnaire in an electronic data collection tool was used to collect baseline data at enrollment. A 5ml blood sample was taken from each participant at baseline and follow-up periods of 6, 12, 18 and 24 months. The samples were processed to obtain aliquots of serum specimens, which were used to evaluate LASV serostatus (IgG) by Enzyme-linked Immunosorbent Assay (ELISA). Serum was separated and stored at -80 degrees Celsius until screening for LASV IgG antibodies was performed at the National Reference Laboratory (NRL), Abuja, in Nigeria.
ELISA Procedure
All serum samples were screened for LASV IgG antibodies using a commercially available ELISA assay, ReLASV® Pan-Lassa Combo nucleoprotein (NP)/Prefusion glycoprotein (GP) IgG ELISA kit, Zal-gen Labs, Frederick, Maryland, USA, with sensitivity of above 90% and specificity of less than 95%(17). To detect a wider range of Lassa virus infections, the assay targets both prefusion glycoprotein (GP) and nucleoprotein (NP) antigens specific to Lassa virus lineages II (Nigeria), and IV (Guinea, Liberia, and Sierra Leone) (18). Four lineages (I-III and VI/Kako strain) have been identified in Nigeria (19). IgG is considered a marker of prior exposure to Lassa virus and can persist in healthy populations for months to years after infection (20). Assays were performed according to the manufacturer’s guidance and methods used previously for assay evaluation for laboratory diagnostics for a vaccine development program (17,18). Following established methodology from a prior Nigerian study, cutoffs were determined based on the sample data set’s optical density (OD) values (18). Consistent with the reference, the negative cutoff was set at the 95th percentile (OD < 0.250), and the positive cutoff was set at twice the negative cutoff (OD ≥ 0.500). Presence of Lassa virus-specific IgG shows positive results, while absence shows negative results. Samples with OD values between these cutoffs were considered indeterminate. A follow-up test was not conducted for the indeterminate results.
Statistical analysis
The collected data was analysed using International Business Machine Statistical Package for Social Sciences (IBM SPSS version 27) (IBM Corporation, Armonk, NY, USA). Data was presented in tables and a line graph showing the frequencies, proportions and trends of LASV infection seroprevalence across different age groups. Based on epidemiological relevance, biological vulnerability, exposure patterns, and clinical outcomes from the literature, the age grouping of 0–5, 6–10, 11–17, 18–50, and >50 years was used in the analysis [5,12,13]. The seroprevalence was calculated by dividing the number of positive results by the total tested within the age groups and within the periods, multiplied by 100. Seroconversion was observed in participants within the same age group from the serum of the samples collected from one period to the other, as previously anti-LASV IgG negative results became positive in the subsequent period; likewise, seroreversion occurred when the previously anti-LASV IgG positive results became negative in the subsequent serum collection.
Ethical consideration
Ethical approval was obtained from the ethics committee of Federal Medical Owo, Ondo State, and the National Health Research Ethics Committee (NHREC). Informed consent and assent (where required) were appropriately obtained from the participants after they had been properly informed about the study and the option of withdrawing their consent at any point if they didn’t feel like continuing the study.
Table 1 shows the distribution of the gender and age groups of the participants across the study communities, with more females in each community except in Ijagba where 55.5% of the participants were males. Majority (44.2%) of the participants were within the age group 18 to 50 years. Table 2 shows the Anti-LASV IgG results for the participants during the study periods, with the highest number of 172 seropositive individuals among 18 to 50 years individuals and the lowest number of 23 seropositive individuals among 2 to 5 years individuals at 24 months of follow-up period.
Figure 1 shows the serological prevalence trend of anti-Lassa virus immunoglobulin G in different age groups among participants, and the seroprevalence was lowest for the age group 2 to 5 years with 19.1% at baseline. It steadily increased to the highest above other age groups to 74.6% at 6 months, after which it dropped to 29.6% at 12 months, below other age groups. This minimally increased but remained below other age groups to 32.4% at 24 months. Age 50 years and above had the highest seroprevalence (43.2%) at baseline, and remained fairly constant till month 24, when it decreased to 39.7%. The seroprevalence of other age groups was almost constant throughout the study.
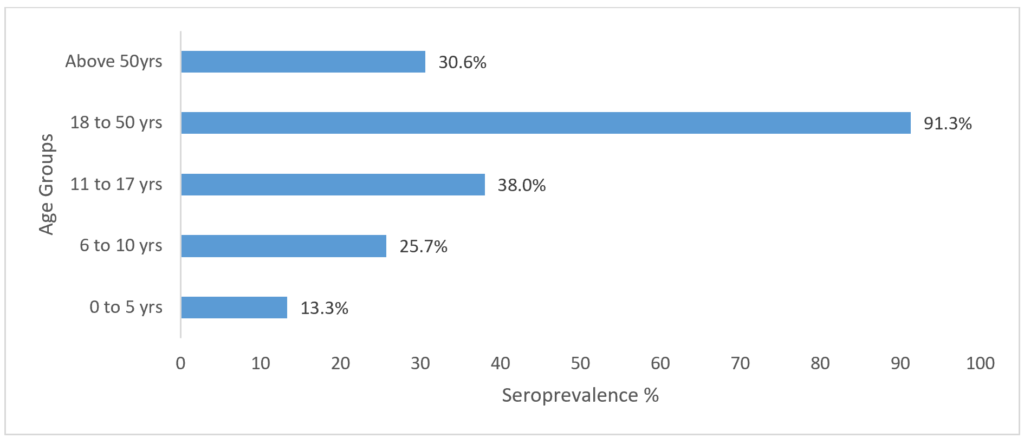
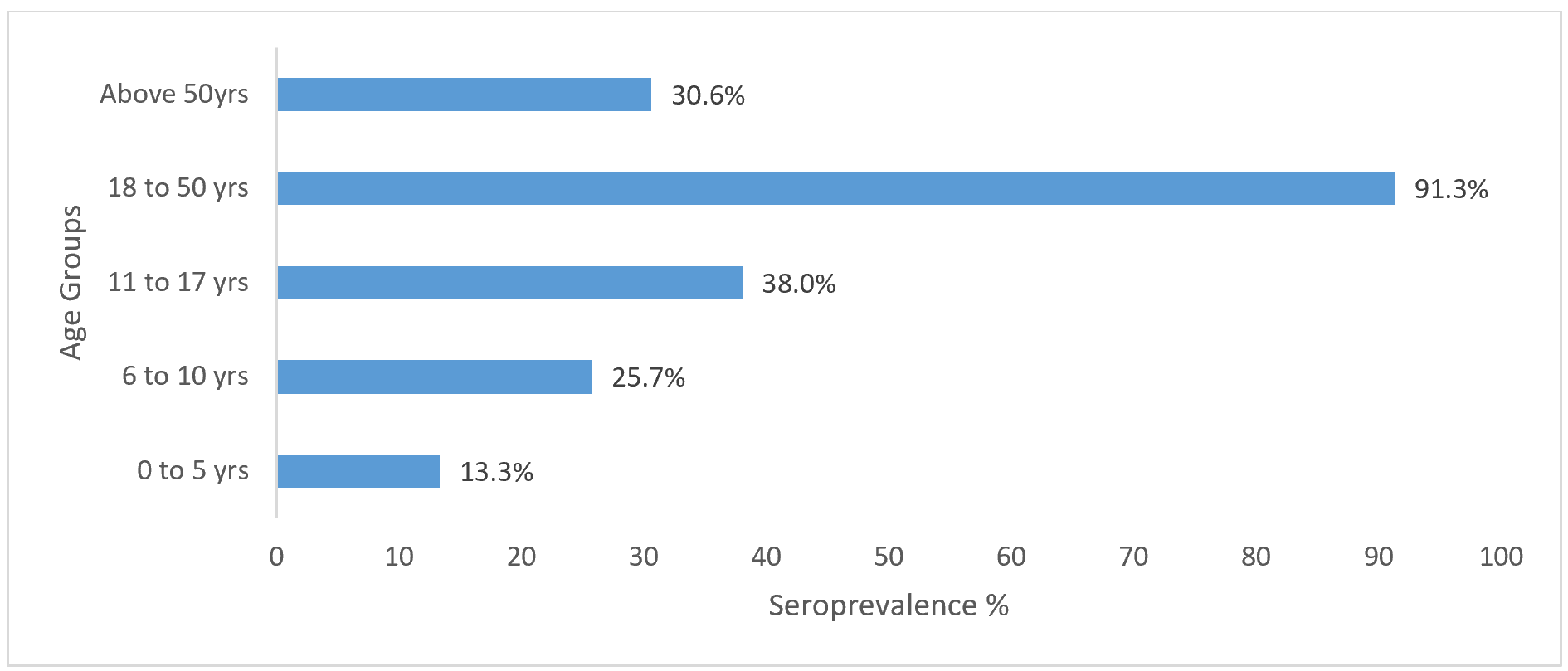
The overall serological prevalence of LASV IgG antibody for the different age groups is shown in Figure 2. There is an increasing pattern of the seroprevalence from the lowest value of 13.3% in the childhood 2 to 5 years age group to the peak of 91.3% in adulthood 18 to 50 years age group, with a decrease in the prevalence to 30.6% in the age group 50 years and above.
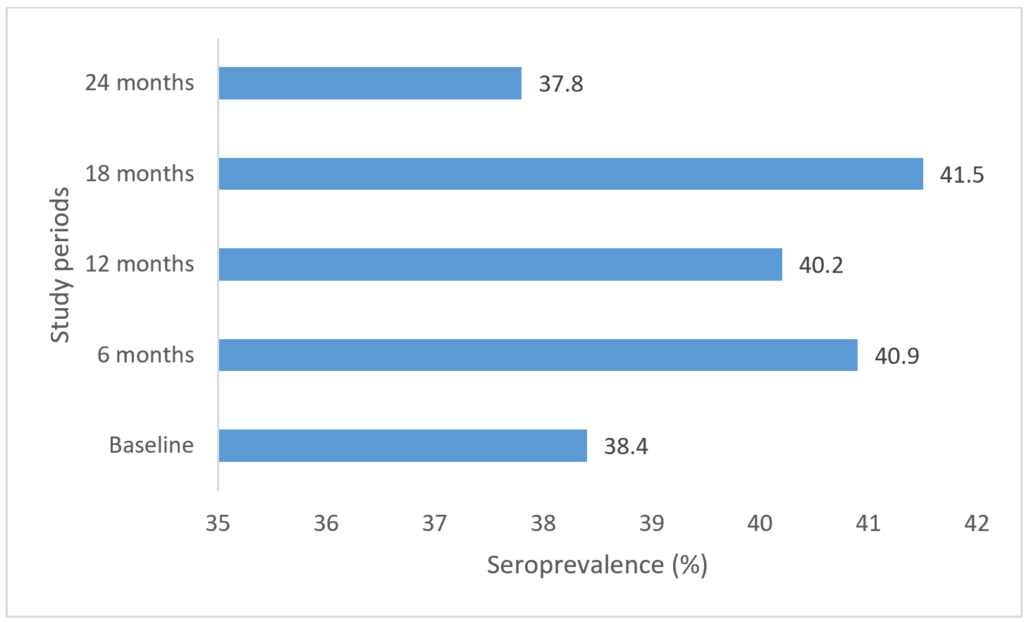
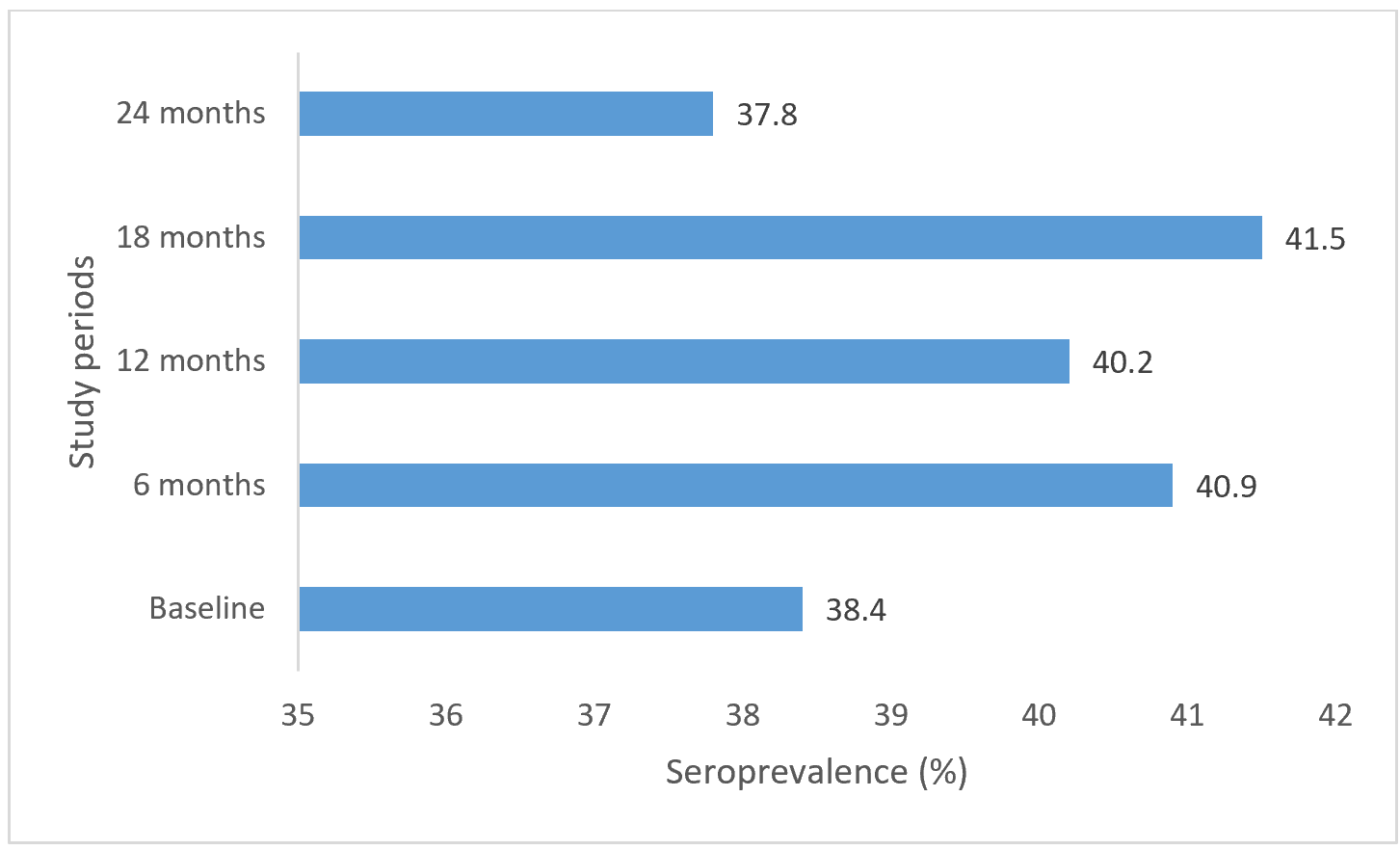
Figure 3 shows the anti-LASV serology prevalence of participants at baseline and follow-up periods. The seroprevalence pattern has a wavy pattern all-through the study period, with 38.4% at baseline, and a moderate increase at the 6-month follow-up period to 40.9%, a subsequent decrease at 12 months to 40.2%, a marginal increase again to 41.5% at 18 months and a final slight decrease to 37.8% at the 24th month. The seroconversion risk from the baseline was 2.5%, which was the probability of developing anti-LASV IgG antibodies from the baseline.
The findings of this study revealed an excellent insight into the temporal and age-specific seroprevalence of anti-Lassa virus (LASV) immunoglobulin G (IgG) antibodies in Ondo State, Nigeria, an endemic region for LASV infection. This study in Figure 1 revealed rapid seroconversion and Sero reversion rates among the age group 2 to 5 years, with constant rates among older age groups. This shows that early exposure to LASV in childhood leads to quick transmission, mostly due to the naïve immunity in this age group and reduced activity engagement with the infectious environment. The rapid seroconversion could imply the effectiveness of vaccination against LASV if introduced early in life, and the seroreversion, a need for booster dosages. The serology pattern also shows that transmission is both continuous over time and increases with age, supporting the typical pattern of transmission of the virus in an endemic setting. The age-dependent growth in LASV IgG seroprevalence also shows the cumulative nature of exposure in the study cohort, and this demonstrates the understanding of LASV ecology in endemic regions.
Seropositivity was most prevalent among the 18 to 50 years of age group in Figure 2, and lowest among children and young adults. These findings are similar to the findings in previous studies from Guinea, Mali, and Sierra Leone demonstrating increases in LASV seroprevalence with age over time [13,21,18]. The pattern of transmission of LASV across the different age groups in this study shows continuous contact with Mastomys natalensis, the main LASV reservoir, and indicates that cumulative exposures to the hazards of LASV transmission at work and home increase with age [5]. The finding of LASV antibodies in children is significant because it emphasises the importance of early-life exposure in endemic populations. This is crucial when taking into account the possibility of lifetime reinfections in this age group and the potential damage that such exposures could cause to the development and health of children in the future. The variation in the pattern of LASV seroprevalence in the age groups from children, adolescents, to the adult population could be explained by the likelihood of LASV transmission across the age groups due to increased exposure resulting from an increase in activities, mobility, and contacts with the infected environment among these individuals as they grow in age, with the adult population being the most active. The downward trend in LASV seroprevalence among those aged 51 and above was further corroborated by the gradual decline in activities and mobility in this age group due to advanced age. As revealed in the overall pattern, LASV is widely spread throughout the study communities, as seen by the low prevalence in children at baseline and the nearly universal presence of antibodies in individuals in other age groups.
The increase in IgG antibody seroprevalence between the baseline and the first follow-up visit at 6 and 18 months in Figure 3, illustrates the recurring exposure to LASV infection among the study population and the decrease at 12 and 24 months shows antibody reversion, which implies that LASV immunity is sustained by continuous transmission from repeated exposures to the infection. Agricultural practices and rodent ecology are linked to seasonal outbreak differences, and this discovery is in line with previous reports that LASV transmission can occur year-round [22,23]. In high-burdened communities like those in Ondo State, the emergence of new infections despite the implementation of awareness campaigns and improved surveillance systems highlights the shortcomings of the current intervention program. Ondo State is frequently listed as one of the epicentres of Lassa fever outbreaks in Nigeria in recent national reports, which underscores persistent community transmission in the state [4]. This implies that all age groups are at high risk of LASV transmission, and the virus is well-established in the communities under study within Ondo State’s ecological and sociological environment.
In addressing the cumulative and sustained patterns of exposure that define LASV transmission in endemic settings, a dual-faceted public health preventive strategy would be effective. Primary preventive measures must be employed to target households with children in the age group with an emphasis on rodent control, safe and secure food storage, and good environmental hygiene, in order to protect the children from early exposure to the risk of LASV transmission [20]. Secondly, high-risk adults, including health workers and caregivers of Lassa fever cases, food handlers and farmers, need targeted interventions, particularly workplace infection prevention and control (IPC) measures. Additionally, structural interventions, such as waste management, rodent-proof housing, and environmental sanitation, are essential. These measures have been demonstrated to lower the risk of transmission in other zoonotic diseases, which can also be adopted for LASV prevention [24,25]. Establishing Infection prevention and control measures in the hospital settings is essential because it prevents possible nosocomial infection outbreaks.
The findings of this cohort study have a direct bearing on LASV vaccine design. As shown in previous studies, some of the vaccines being actively explored for clinical testing include live attenuated and viral vector platforms [26]. The results of this study show that a vaccination campaign should target both the adult and child age groups because LASV exposure begins early in life and builds up over time, which is similar to a suggestion in a previous study [27]. The baseline seropositivity rate assessment in this study is critical for the design of studies used in evaluating LASV vaccines, which include consideration of age-stratification pattern and prior exposure. Older adults with pre-existing immunity may benefit from immunisation to evaluate the vaccine’s potential for enhancing immunity, and younger individuals with lower antibody levels may serve as sentinel populations to assess the effectiveness of the vaccine. Ondo State, with a high intensity of transmission as an endemic state, is suitable for this kind of research.
Study limitations
Long-term seroconversion rates may have been miscalculated because of the short duration of follow-up. There is also a limitation in the calculation of the overall seroprevalence of the age groups due to the difficulty in calculating the period prevalence for each age group in the study, because of the seroconversions and seroreversions that occur within each age group across the study periods. Considering the very high point prevalence of the 2 to 5 years age group at 6 months, the positive results could possibly be an outlier, which could be from possible issues around the laboratory testing, though appropriate measures were put in place to ensure quality. The only detection of IgG serology is the previous exposure to LASV infection, and it could not distinguish between the symptomatic and non-symptomatic ones, which are both prevalent in the infection. The number of indeterminate results across the study periods could have affected the eventual outcome of the study. In addition, the relationship between the observed seroprevalence and the behavioural and ecological risk factors could not be established, as these risk factors were not involved in the present work. Therefore, additional studies should combine the serological socio-behavioural assay with the ecological monitoring system of rodents to elucidate the modes of transmission.
The findings presented in this study reveal the cumulative and continuous exposure to LASV in Ondo State, with an increasing antibody seroprevalence as the population advances in age. These results show the pressing need for enhanced community-based preventive, focused health education, and better infection control strategies. Furthermore, age-specific serological profiles provide target indicators to direct vaccine development, distribution, and trial planning in endemic areas. A coordinated strategy combining biological advancements with behavioural and preventative measures at the community level is required to reduce the effects of Lassa fever.
What is already known about the topic
What this study adds
We acknowledge The Enable programmes, including BNITM, Epicentre, MMARCRO, and P95, for their support in study monitoring, data management and analysis, laboratory technical support and coordination, project management, and epidemiological technical support and coordination and the Coalition for Epidemic Preparedness Innovations (CEPI) for funding the Enable Lassa research programme.
Adetumi Adetunji Subulade: Original draft manuscript preparation, writing and editing, data curation, data analysis, visualization, and validation.
Oladele Oluwafemi Ayodeji: Writing – Original draft manuscript master review, project administration, resources, data curation, supervision, validation.
Chukwuyem Abejegah: Supervision, project support, resources.
Austine Osagbaekhoe: Project support, data collection
Akinola Nelson Adedosu: Project and laboratory support, resources.
Olufunke B. Gbenga-Ayeni: Project and laboratory support
Johnson Etafo: Project and laboratory support
Ireneh Ronke: Project and laboratory support
MacDonald Onyechi: Project and laboratory support
Isaac Ihinmikhaye: Project support
Grace Temitope Olubayo: Project support
Adesola Omowumi Kareem: Project support
Gloria Abimbola Awe: Project support
Adebola Olayinka: Project support
Kam Kanji: Project support
Winifred D.Ingbian: Project support
Liasu Adeagbo Ahmed: Project support
Henshaw Mandi: Project support
| Variables | STUDY COMMUNITIES | ||||
|---|---|---|---|---|---|
| EHINOGBE | IDASEN | IFON | IJAGBA | IJEBU | |
| Sex | |||||
| Female | 68 (53.5%) | 13 (54.2%) | 67 (54.9%) | 51 (44.7%) | 73 (60.3%) |
| Male | 59 (46.5%) | 11 (45.8%) | 55 (45.1%) | 63 (55.3%) | 48 (39.7%) |
| Age (years) | |||||
| 2 to 5 | 10 (9.9%) | 0 (0.0%) | 5 (4.1%) | 10 (8.8%) | 10 (8.3%) |
| 6 to 10 | 14 (11.0%) | 5 (20.8%) | 4 (3.3%) | 23 (20.2%) | 16 (13.2%) |
| 11 to 17 | 24 (18.9%) | 1 (4.2%) | 21 (17.2%) | 25 (21.9%) | 32 (26.4%) |
| 18 to 50 | 62 (48.8%) | 11 (45.8%) | 59 (48.4%) | 44 (38.6%) | 50 (41.3%) |
| Above 50 | 17 (13.4%) | 7 (29.2%) | 33 (27.0%) | 12 (10.5%) | 13 (10.7%) |
| Total | 127 | 24 | 122 | 114 | 121 |
| Variables | ILALE | IPELE | ISUADA | IYERE | OGBESE |
| Sex | |||||
| Female | 42 (50.6%) | 28 (51.9%) | 17 (51.5%) | 44 (54.3%) | 153 (61.4%) |
| Male | 41 (49.4%) | 26 (48.1%) | 16 (48.5%) | 37 (45.7%) | 96 (38.6%) |
| Age (years) | |||||
| 2 to 5 | 9 (10.8%) | 3 (5.6%) | 2 (6.1%) | 4 (4.9%) | 18 (7.2%) |
| 6 to 10 | 11 (13.3%) | 13 (24.1%) | 6 (18.2%) | 6 (7.4%) | 41 (16.5%) |
| 11 to 17 | 18 (21.7%) | 10 (18.5%) | 8 (24.2%) | 8 (9.9%) | 59 (23.7%) |
| 18 to 50 | 37 (44.6%) | 19 (35.2%) | 13 (39.4%) | 37 (45.7%) | 114 (45.8%) |
| Above 50 | 8 (9.6%) | 9 (16.7%) | 4 (12.1%) | 26 (32.1%) | 17 (6.8%) |
| Total | 83 | 54 | 33 | 81 | 249 |
| Age (years) | Number of participant | Anti-LASV IgG result | Baseline | 6 months | 12 months | 18 months | 24 months |
|---|---|---|---|---|---|---|---|
| 2 to 5 | 71 | Negative | 57 | 2 | 46 | 42 | 40 |
| Positive | 14 | 53 | 21 | 23 | 23 | ||
| Indeterminate | 0 | 16 | 4 | 6 | 8 | ||
| 6 to 10 | 139 | Negative | 89 | 83 | 77 | 73 | 69 |
| Positive | 48 | 50 | 53 | 55 | 53 | ||
| Indeterminate | 2 | 6 | 9 | 11 | 17 | ||
| 11 to 17 | 206 | Negative | 128 | 121 | 120 | 103 | 104 |
| Positive | 75 | 69 | 79 | 85 | 75 | ||
| Indeterminate | 3 | 16 | 7 | 18 | 27 | ||
| 18 to 50 | 446 | Negative | 251 | 222 | 222 | 201 | 202 |
| Positive | 187 | 178 | 190 | 193 | 172 | ||
| Indeterminate | 8 | 46 | 34 | 52 | 72 | ||
| Above 50 | 146 | Negative | 81 | 71 | 69 | 68 | 63 |
| Positive | 63 | 63 | 62 | 62 | 58 | ||
| Indeterminate | 2 | 12 | 15 | 16 | 25 | ||
| Statistical significance | LR=19.743 P=0.011 | LR=25.469 P=0.001 | LR=15.233 P=0.055 | LR=7.766 P=0.457 | LR=6.336 P=0.610 | ||