Outbreak investigation | Open Access | Volume 9 (Suppl 13): Article 05 | Published: 16 Jul 2026

Views: 30
Menu, Tables and Figures
Table 1: Age distribution of confirmed cholera cases, Kasensero Landing Site, April-May 2024
| Age group (years) | Frequency | Percentage (%) |
|---|---|---|
| 0-20 | 1 | 7.1 |
| 21-40 | 6 | 42.9 |
| 41-60 | 5 | 35.7 |
| 61-80 | 2 | 14.3 |
| Total | 14 | 100 |
Table 2: Response assessment using the WHO Five Pillars framework, Kasensero Landing Site, April-May 2024
| Pillar | Strengths | Gaps |
|---|---|---|
| Surveillance | Rapid alert, case finding, contact tracing | Limited diagnostics, confirmation delays |
| Risk communication & engagement | VHT mobilization, UNICEF materials, campaigns | Sustaining behavior change |
| Laboratory | RDT availability, culture & sensitivity testing | Initial capacity constraints, transport delays |
| Case management | Designated unit, supply mobilization | Stock-outs, limited isolation space, delivery delays |
| WASH/IPC | Water tablets, hygiene promotion | Untreated lake water, poor sanitation, open defecation, no waste disposal or handwashing |
Ibrahim Mutebi1,&, Twesigye Belinda1, Nakidde Florence1, Wilson Tusiime1, Connie Nait1, Alex Mulyowa1, Bernard Lubwama2, Ben Masiira3, Suzanne Namusoke Kiwanuka1
1Department of Health Policy Planning and Management, College of Health Sciences, Makerere University School of Public Health, Kampala, Uganda, 2Division of Integrated Epidemiology and Surveillance, Ministry of Health, Uganda, 3African Field Epidemiology Network, Kampala
&Corresponding author: Ibrahim Sseddangira, Department of Health Policy Planning and Management, College of Health Sciences, Makerere University School of Public Health, Kampala, Uganda, Email: ibrahimsseddangira@gmail.com, ORCID: https://orcid.org/0009-0009-2974-3231
Received: 17 Oct 2025, Accepted: 15 Jul 2026, Published: 16 Jul 2026
Domain: Field Epidemiology
Keywords: Cholera, outbreak, fishing community, WASH, Uganda
©Ibrahim Sseddangira et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Ibrahim Sseddangira et al., Cholera outbreak in a fishing community with inadequate water, sanitation, and hygiene infrastructure: A descriptive investigation at Kasensero Landing Site, Uganda. Journal of Interventional Epidemiology and Public Health. 2026; 9(Suppl 13):05. https://doi.org/10.37432/jieph-d-25-00242
Introduction: On 26 April 2024, Kyotera District health officials reported suspected cholera cases at Kasensero Landing Site, a fishing community along Lake Victoria with known water, sanitation and hygiene (WASH) vulnerabilities. We investigated the outbreak to confirm its existence, characterize cases by person, place and time, assess WASH conditions, and evaluate the response.
Methods: We conducted a descriptive outbreak investigation reviewing outpatient records at Kasensero Health Center II from 1 April to 14 May 2024. Standard case definitions were applied where suspected (acute watery diarrhoea ± vomiting in persons ≥2 years, or acute watery diarrhoea with some or severe dehydration in children <2 years); confirmed (Vibrio cholerae O1/O139 isolated by culture or detected by rapid diagnostic test). Data were analyzed descriptively using Microsoft Excel. Field observations assessed WASH infrastructure and response efforts using the WHO Five Pillars framework.
Results: We identified 52 suspected cases, of which 14 (26.9%) were laboratory-confirmed. The epidemic curve was consistent with common-source exposure. Confirmed cases were geographically clustered in Kimwanyi Cell 5 (92.9%; 95% CI: 66.1% – 99.8%) and predominantly working-age adults (78.6% aged 21-60 years) with equal sex distribution. Field observations revealed heavy reliance on untreated lake water, inadequate latrine coverage, open defecation, and absent handwashing facilities.
Conclusion: This outbreak was consistent with common-source exposure in a high-risk WASH setting. Preventing future outbreaks requires sustained investment in safe water supply, sanitation facilities, hygiene promotion, oral cholera vaccination, and strengthened laboratory diagnostics for fishing communities along Lake Victoria.
Cholera, caused by Vibrio cholerae, is an acute diarrheal disease transmitted primarily through contaminated water or food. It remains a major public health threat in resource-limited settings, causing an estimated 1.3-4.0 million cases and 21,000 -143,000 deaths annually worldwide [1-3].
In sub-Saharan Africa, including Uganda, cholera is endemic in areas near water bodies, with recurrent outbreaks linked to poor WASH infrastructure, overcrowding, and environmental factors [4-6]. Uganda experiences near-annual outbreaks that disproportionately affect fishing communities along Lake Victoria, which despite comprising only 5-10% of the population have historically contributed over half of national cases due to reliance on untreated lake water and inadequate sanitation [7, 8].
Kasensero Landing Site in Kyotera District is a densely populated fishing hub on Lake Victoria. On 26 April 2024, Kasensero Health Center II reported a suspected cholera death and rising cases of acute watery diarrhea, vomiting and dehydration, triggering an outbreak investigation. We conducted this investigation to confirm the outbreak, characterize cases by person, place and time, assess WASH conditions, and evaluate response effectiveness using the WHO Five Pillars framework.
Study setting
The investigation took place at Kasensero Landing Site, a major fishing port on the northern shores of Lake Victoria in Kyotera District, Central Uganda, approximately 15 kilometers from the Tanzania border. The landing site has an estimated population of 12,000 residents, predominantly engaged in fishing and fish-related commercial activities [9]. Most residents rely on lake water for domestic use and have inadequate toilet facilities. The primary health facility is Kasensero Health Center II, a government facility providing outpatient care, basic laboratory services, and maternal health services.
Investigation design
We conducted a descriptive outbreak investigation characterizing cases by person, place and time, assessing WASH conditions, and evaluating the response. The investigation included retrospective review of outpatient department (OPD) records, laboratory registers, and daily surveillance reports. All activities followed WHO and Uganda Ministry of Health guidelines for cholera outbreak investigation and response [3,10,11]. The investigation was conducted by a multidisciplinary team comprising Field Epidemiology Training Programme (FETP) trainees and graduates from Makerere University School of Public Health, deployed in response to a formal request from Kyotera District Health Office (DHO). The team was supervised by experienced field epidemiologists affiliated with the Africa Field Epidemiology Network (AFENET) and operated under the mandate of the district health authorities in support of the routine public health surveillance and response system. Team members had training in applied epidemiology, laboratory sciences, and public health, and worked in close collaboration with the Kyotera District Health Team throughout the investigation.
Case definitions
Suspected case: Any resident or visitor of Kyotera District aged two years or above presenting with acute watery diarrhea (three or more loose stools within 24 hours), with or without vomiting, at Kasensero Landing Site between 1 April and 14 May 2024. For children under two years, a suspected case was defined as any child presenting with acute watery diarrhoea with some or severe dehydration within the same parameters.
Confirmed case: A suspected case with laboratory confirmation of Vibrio cholerae O1 or O139 by stool culture or positive rapid diagnostic test (RDT).
Contact: Any person who shared food, water, or living quarters with a confirmed or suspected case during the five days before and after the onset of illness in the index case.
Data collection
Data were obtained from OPD registers (1 April-14 May 2024), stool culture results from the National Health Laboratory Services, RDT results at the facility, and daily District Health Team surveillance reports. Records from 1 to 25 April 2024 served as a look-back period to identify any cases predating the formal outbreak alert of 26 April 2024; no cases meeting the suspected case definition were identified during this look-back period. Additionally, response effectiveness was assessed qualitatively using the WHO Five Pillars framework through document review and field observations. District task force meeting minutes and surveillance reports were reviewed for each pillar domain, and field observation findings were thematically summarised against pillar-specific indicators to identify strengths and gaps in the outbreak response.
Data management and analysis
Data were entered and cleaned in Microsoft Excel 2019 using pre-designed templates with validation rules. Descriptive analysis characterized the outbreak by person, place and time. An epidemic curve was generated to visualize the temporal distribution of cases.
Ethical considerations
Ethical approval was granted by the Makerere University School of Public Health Higher Degrees Research and Ethics Committee (REC No: SPH-2024-591, 26 April 2024). This investigation was conducted as part of routine public health surveillance; individual participant consent was therefore waived and all data were anonymized prior to analysis.
Overview of the outbreak
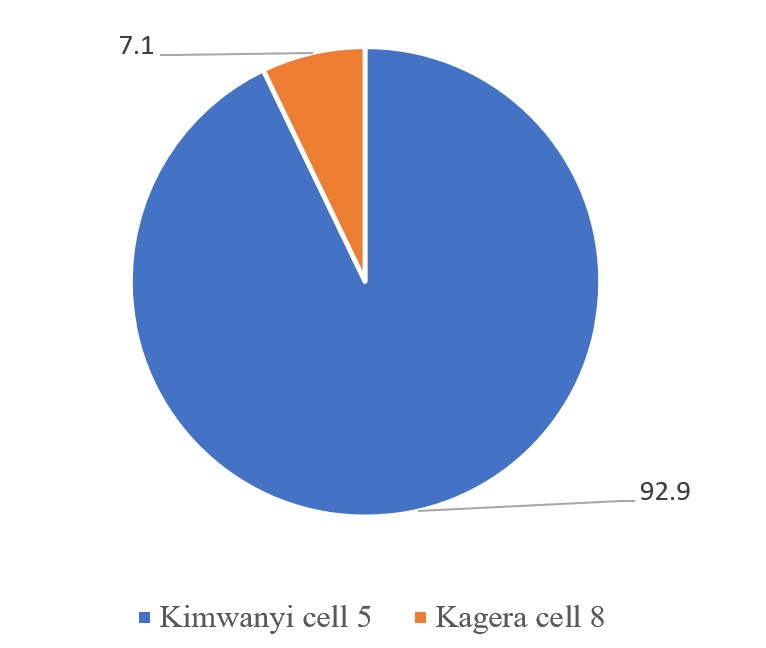
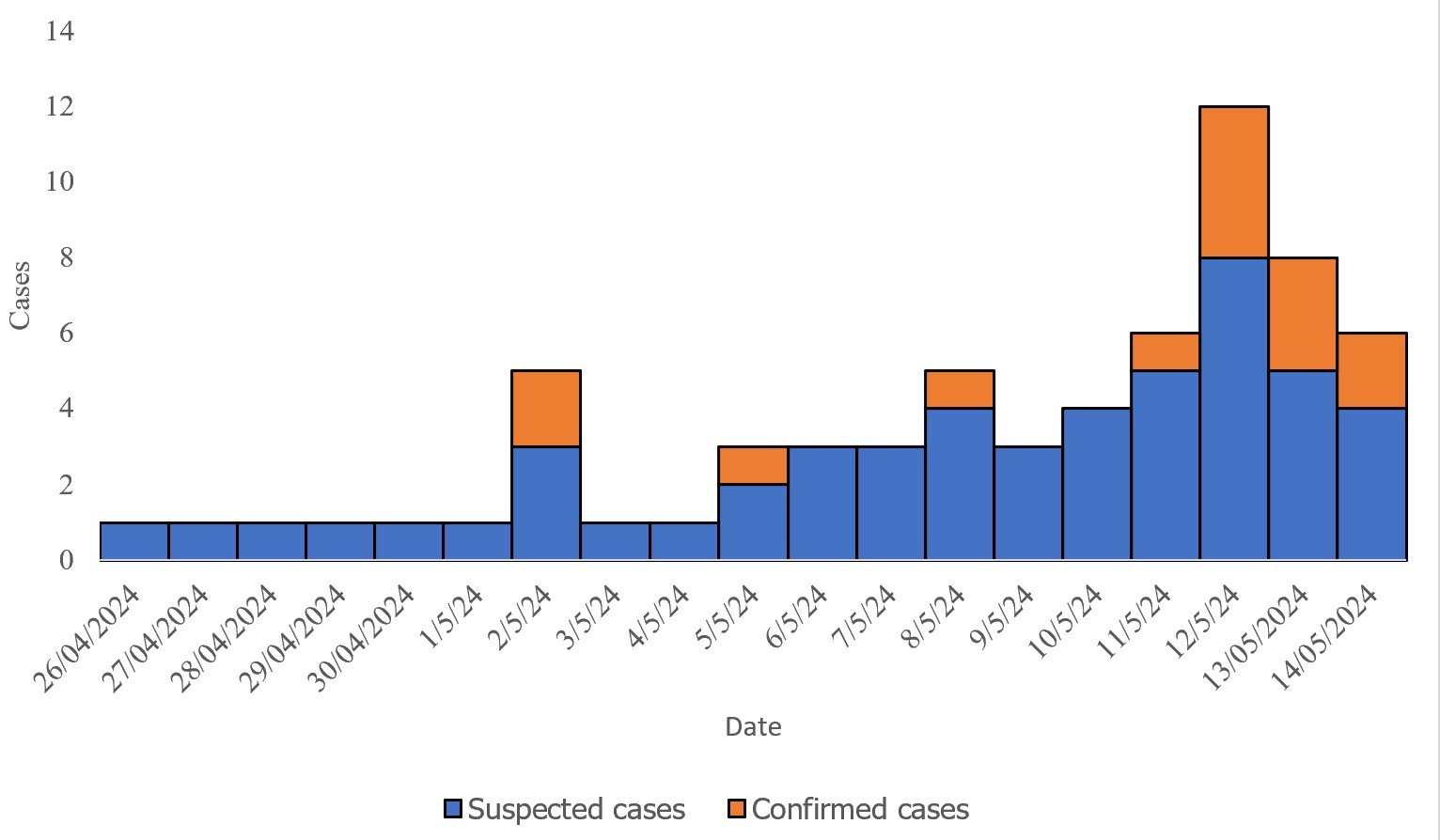
Between 26 April and 14 May 2024, 52 suspected cholera cases were identified at Kasensero Landing Site. Of these, 14 (26.9%) were laboratory-confirmed for Vibrio cholerae: 10 (71.4%) by RDT and four (28.6%) by stool culture. The suspected cholera death reported at the time of the initial alert could not be laboratory-confirmed; on review of available records, no confirmed deaths were attributable to this outbreak, and no case fatality rate could be calculated. The median age was 40 years (range: 11 months to 74 years). Among confirmed cases, 42.9% were aged 21-40 years, 35.7% were aged 41-60 years, 14.3% were aged 61-80 years, and 7.1% were aged 0-20 years (Table 1). Confirmed cases were predominantly working-age adults (78.6% aged 21–60 years) with equal sex distribution (7 male, 7 female). Cholera cases were significantly clustered within Kasensero Landing Site. Of the 14 confirmed cases, 13 (92.9%; 95% CI: 66.1%–99.8%) were residents of Kimwanyi Cell 5 (Figure 1). The epidemic curve demonstrated a pattern consistent with common-source exposure, with a sharp rise, peak, and gradual decline over a 19-day period. The first suspected case was reported on 26 April 2024, and the first confirmed case on 2 May 2024 (Figure 2).
WASH conditions
Field observations revealed major deficiencies in WASH infrastructure. The majority of residents relied on untreated lake water for drinking and domestic purposes. Latrine coverage was inadequate and existing latrines were in poor condition. Open defecation was widespread, particularly along the lakeshore. No waste disposal facilities were available. Handwashing facilities with soap were absent from public places.
Response assessment: Five Pillars framework
Pillar 1: Surveillance. The rapid alert system enabled quick case identification and contact tracing. However, limited diagnostic capacity and delays in laboratory confirmation slowed the response. Overall, 52 suspected and 14 confirmed cases were identified.
Pillar 2: Risk communication and community engagement. Village Health Teams (VHTs) were mobilized, UNICEF distributed information and education materials, and radio announcements were used to raise community awareness. Sustaining behavior change remained a challenge.
Pillar 3: Laboratory. RDTs and confirmatory culture testing with antimicrobial sensitivity profiling were available. Initial diagnostic capacity was constrained and sample transport delays affected timeliness.
Pillar 4: Case management. A treatment facility was designated, and medical supplies were mobilised. Drug stock-outs, limited isolation capacity (one bed in one small isolation room), and supply delivery delays were significant barriers.
Pillar 5: WASH/IPC. Water treatment tablets and hygiene promotion campaigns were provided by UNICEF Uganda. These short-term measures were undermined by persistent structural deficiencies in sanitation and ongoing environmental contamination. Strengths and gaps for each pillar are summarised in Table 2.
This descriptive investigation identified 52 suspected and 14 confirmed cholera cases at Kasensero Landing Site between April and May 2024. The confirmation rate of 26.9% aligns with experiences in other resource-limited outbreaks, where rates typically range from 20-40% due to constraints in diagnostic capacity and specimen transport [7].
Confirmed cases predominantly involved working-age adults (78.6% aged 21-60 years), contrasting with the more common pattern in sub-Saharan Africa, where young children and elderly adults bear the highest burden [12]. This age distribution is consistent with occupational exposure risks in fishing communities, where adults engage in activities involving direct contact with lake water [13,14]. Equal sex distribution among confirmed cases, differing from national surveillance data showing slight female predominance [15], suggests shared household or community-level exposure rather than gender-specific occupational risk.
Marked spatial clustering (92.9% of confirmed cases in Kimwanyi Cell 5; 95% CI: 66.1%-99.8%) and an epidemic curve consistent with common-source exposure suggest prolonged exposure to a localised environmental reservoir, most likely contaminated lake water, though no environmental microbiological testing was conducted to confirm this. Similar clustered patterns have been documented in Ugandan fishing villages, including Kaiso (2015) and Kasese (2015), where transmission was linked to specific lakeshore water collection points [16,17].
Field observations revealed major WASH deficiencies, widespread reliance on untreated lake water, inadequate and poorly maintained latrines, open defecation along the lakeshore, and absence of handwashing facilities and waste disposal systems. These observations are consistent with prior evidence identifying poor WASH as the key driver of recurrent cholera in Ugandan fishing communities [8, 17]. These communities, representing only 5-10% of the population, have historically contributed over half of national cases and deaths [8].
Evaluation using the Five Pillars framework revealed operational strengths alongside significant gaps. Rapid surveillance alerts, community engagement through VHTs, and emergency supply mobilization were commendable. However, delays in laboratory confirmation, drug stock-outs, and limited isolation capacity reflect deeper system-level challenges. These challenges are compounded by chronic under-resourcing of peripheral health facilities, logistical barriers inherent in remote lakeshore settings, fragmented supply chains, and over-reliance on short-term emergency funding rather than sustained programmatic investment in outbreak preparedness.
Limitations
Attack rates could not be estimated because verified population denominators for the landing site were unavailable. The case fatality rate could not be calculated because the single suspected death at the time of the outbreak alert could not be laboratory-confirmed, and no additional deaths were recorded during the investigation period. Health facility-based case ascertainment likely introduced selection bias toward more severe cases, with probable under-ascertainment of mild or community-managed cases. The predominant use of RDTs, while pragmatic, carries moderate specificity and may have resulted in some false-positive confirmed cases; the limited number of culture confirmations (n=4) restricts the strength of microbiological conclusions. Environmental microbiological testing of water sources was not conducted due to resource constraints, preventing direct confirmation of the implicated source. WASH conditions were assessed through direct field observation rather than structured household surveys; no quantitative indicators were systematically collected. The descriptive-only design precludes causal inference; all interpretations regarding transmission dynamics and risk factors should be understood as hypothesis-generating.
This descriptive investigation confirmed a cholera outbreak at Kasensero Landing Site associated with common-source exposure in a high-risk WASH setting, highlighting both strengths and operational gaps in the district-level response. To prevent future outbreaks in fishing communities, we recommend sustained investment in community-specific WASH infrastructure (protected water points, improved latrine coverage, solid waste management); strengthening peripheral laboratory capacity through consistent stocking of RDTs, culture media, and reliable cold-chain transport; conducting analytical epidemiological studies to quantify specific transmission risk factors; and prioritizing oral cholera vaccination campaigns targeting fishing communities along Lake Victoria given the persistence of environmental risk factors and the time required for WASH improvements to take effect.
What is already known about the topic
What this study adds
We acknowledge the support of the Ministry of Health, district health officials, and facility administration of Kasensero Health Center II. We also appreciate all field participants in this investigation. We acknowledge Angela N. Kisakye for reviewing the different versions of this manuscript.
List of abbreviations
AWD: Acute Watery Diarrhoea
DHO: District Health Officer
DHT: District Health Team
DTF: District Task Force
IPC: Infection Prevention and Control
MoH: Ministry of Health
OCV: Oral Cholera Vaccine
OPD: Outpatient Department
RDT: Rapid Diagnostic Test
UNICEF: United Nations Children’s Fund
VHT: Village Health Team
WASH: Water, Sanitation, and Hygiene
WHO: World Health Organization
IS wrote the initial draft, participated in the investigation and performed formal analysis. TB and NF participated in the investigation. WT and BL supervised the investigation team and edited the manuscript. CN and AM contributed to editing. BM and SNK reviewed and edited the manuscript for substantial intellectual content. All authors read and approved the final version for submission.
Table 1: Age distribution of confirmed cholera cases, Kasensero Landing Site, April-May 2024
| Age group (years) | Frequency | Percentage (%) |
|---|---|---|
| 0-20 | 1 | 7.1 |
| 21-40 | 6 | 42.9 |
| 41-60 | 5 | 35.7 |
| 61-80 | 2 | 14.3 |
| Total | 14 | 100 |
Table 2: Response assessment using the WHO Five Pillars framework, Kasensero Landing Site, April-May 2024
| Pillar | Strengths | Gaps |
|---|---|---|
| Surveillance | Rapid alert, case finding, contact tracing | Limited diagnostics, confirmation delays |
| Risk communication & engagement | VHT mobilization, UNICEF materials, campaigns | Sustaining behavior change |
| Laboratory | RDT availability, culture & sensitivity testing | Initial capacity constraints, transport delays |
| Case management | Designated unit, supply mobilization | Stock-outs, limited isolation space, delivery delays |
| WASH/IPC | Water tablets, hygiene promotion | Untreated lake water, poor sanitation, open defecation, no waste disposal or handwashing |