Research | Open Access | Volume 9 (3): Article 117 | Published: 17 Jul 2026

Views: 46
Menu, Tables and Figures
| Table 1: Selected health facilities in the study on KAP among healthcare workers in Uganda, August-September, 2024 (n=17) | ||
| Name | Location/District | Level |
|---|---|---|
| Bwera General Hospital | Kasese | Hospital |
| Mount. Saint. Mary Hospital | Kasese | Hospital |
| Saint. Paul Hospital | Kasese | Hospital |
| Kagando Hospital | Kasese | Hospital |
| Rukooki Health Centre | Kasese | HC IV |
| Nyabirongo Health Centre | Kasese | HC III |
| Nyabugando Health Centre | Kasese | HC III |
| Kasese Municipal Health Centre | Kasese | HC III |
| Railway Health Centre | Kasese | HC III |
| Bukangara Health Centre | Kasese | HC III |
| Buluba Hospital | Mayuge | Hospital |
| Mayuge Health Centre | Mayuge | HC IV |
| Kityerera Health Centre | Mayuge | HC IV |
| Kigandalo Health Centre | Mayuge | HC IV |
| Busaala Health Centre | Mayuge | HC III |
| Bwondha Health Centre | Mayuge | HC II |
| Wandegeya Health Centre | Mayuge | HC II |
Table 1: Selected health facilities in the study on KAP among healthcare workers in Uganda, August-September, 2024 (n=17)
| Characteristics | Frequency (n) | Percentage (%) |
|---|---|---|
| Age (years) | ||
| 18-35 | 253 | 75 |
| ≥36 | 86 | 25 |
| Sex | ||
| Female | 215 | 63 |
| Male | 124 | 37 |
| Marital status | ||
| Married | 149 | 44 |
| Un-married | 190 | 56 |
| Level of education | ||
| Masters | 10 | 2.9 |
| Bachelors | 25 | 7.4 |
| Diploma | 92 | 27 |
| Certificate | 196 | 58 |
| Missing | 16 | 4.7 |
| Years of experience | ||
| <5 | 184 | 60 |
| 5-10 | 62 | 20 |
| >10 | 61 | 20 |
| Cadre | ||
| Clinicians | 69 | 21 |
| Nurses/midwives | 210 | 62 |
| Laboratory technicians | 52 | 15 |
| Others* | 8 | 2 |
| Health facility level | ||
| Hospital | 116 | 34 |
| HC IV | 169 | 50 |
| HC III | 44 | 13 |
| HC II | 10 | 3 |
| Source of information | ||
| Social media platforms | 232 | 71 |
| Health facilities | 2 | 0.6 |
| People* | 94 | 29 |
Table 2: Socio-demographic characteristics of healthcare workers, Uganda, August-September, 2024 (n=339)
| Table 3: Assessment of knowledge towards mpox among healthcare workers’, Uganda, August–September, 2024 | ||
| Variable | Frequency | Percentage |
|---|---|---|
| Accessed to mpox information | ||
| Yes | 295 | 87 |
| No | 44 | 13 |
| Received training on mpox | ||
| Yes | 39 | 12 |
| No | 300 | 88 |
| Aware of the causative agent for mpox | ||
| Yes | 268 | 79 |
| No | 71 | 21 |
| Aware of ongoing mpox outbreak | ||
| Yes | 211 | 62 |
| No | 128 | 38 |
| Aware of clinical manifestations for mpox | ||
| Yes | 43 | 13 |
| No | 296 | 87 |
| Aware of availability of mpox vaccine | ||
| Yes | 100 | 29 |
| No | 239 | 71 |
Table 3: Assessment of knowledge towards mpox among healthcare workers, Uganda, August–September, 2024
| Table 4: Source of health information among healthcare workers’, Uganda, August-September, 2024 | ||
| Source of information | Frequency | Percentage (%) |
|---|---|---|
| Media outlets* | 319 | 93 |
| Health platforms* | 273 | 81 |
| Colleagues* | 167 | 49 |
| Social media* | 178 | 43 |
| Community* | 87 | 26 |
| Media outlets=Radios, Television, Newspaper, Health platforms=Ministry of Health, Health facility, Colleagues=Healthcare workers, Friends and family, Social media=WhatsApp, Facebook, X, Google, Instagram, Community=Voluntary health teams, Church leaders, Community leaders | ||
Table 4: Source of health information among healthcare workers, Uganda, August-September, 2024
| Table 5: Assessment of attitude towards mpox among healthcare workers, Uganda, August–September, 2024 (n=339) | ||||||
| Characteristics | Agree (n) | (%) | Disagree (n) | (%) | Don’t know (n) | (%) |
|---|---|---|---|---|---|---|
| One should go to hospital if they present mpox clinical features | 313 | 92 | 4 | 1.2 | 22 | 6.5 |
| Mpox transmission can increase by direct contact | 288 | 85 | 4 | 1.2 | 47 | 14 |
| Mpox is a serious disease | 286 | 84 | 9 | 2.7 | 44 | 13 |
| Mpox infection could increase by overcrowding | 279 | 82 | 11 | 3.2 | 49 | 14.5 |
| Hand washing could protect someone from mpox | 251 | 74 | 40 | 11.8 | 48 | 14.2 |
| Wearing PPE* does not protect one from mpox | 35 | 10 | 269 | 79.4 | 35 | 10 |
| Mpox disease does not lead to death | 27 | 7.9 | 276 | 81 | 36 | 11 |
| PPE=Personal protective equipment | ||||||
Table 5: Assessment of attitude towards mpox among healthcare workers, Uganda, August–September, 2024 (n=339)
| Table 6: Factors associated with knowledge towards mpox among healthcare workers’, Uganda, August–September, 2024 | ||||
| Characteristics | Knowledge level | uPR 95% CI | aPR 95% CI | |
|---|---|---|---|---|
| Adequate n (%) | Inadequate n (%) | |||
| Age (years) | ||||
| 18-35 | 214 (75) | 39 (74) | Ref | |
| ≥36 | 72 (25) | 14 (26) | 1.1 (0.57-1.9) | – |
| Sex | ||||
| Female | 181 (63) | 34 (64) | Ref | |
| Male | 105 (37) | 19 (36) | 0.97 (0.55-1.7) | – |
| Marital status | ||||
| Married | 128 (45) | 21 (40) | Ref | |
| Un-married | 158 (55) | 32 (60) | 1.2 (0.69-2.1) | – |
| Level of education | ||||
| Masters | 8 (2.8) | 2 (3.8) | 2.5 (0.35-18) | – |
| Bachelors | 23 (8.0) | 2 (3.8) | Ref | |
| Diploma | 75 (26) | 17 (32) | 2.3 (0.53-10) | – |
| Certificate | 169 (59) | 27 (51) | 1.7 (0.41-7.3) | – |
| Years of experience | ||||
| <5 | 140 (54) | 23 (48) | Ref | |
| ≥5 | 119 (46) | 25 (52) | 1.2 (0.69-2.2) | – |
| Designation | ||||
| Clinicians | 63 (22) | 6 (11) | Ref | |
| Nurses/midwives | 178 (62) | 32 (60) | 1.8 (0.73-4.2) | 1.7 (0.69-3.9) |
| Laboratory technicians | 39 (14) | 13 (25) | 2.9 (1.1-7.6) | 2.7 (1.0-7.2) |
| Others* | 6 (2.0) | 2 (3.8) | 2.9 (.58-14) | 2.9 (0.59-15) |
| Health facility level** | ||||
| Lower level | 40 (14) | 14 (26) | Ref | |
| Higher level | 246 (86) | 39 (74) | 2.6 (1.7-3.8) | – |
| Access to mpox information | ||||
| No | 42 (15) | 2 (3.8) | Ref | |
| Yes | 244 (85) | 51 (96) | 3.8 (0.93-15) | 3.4 (0.85-14) |
| Previous mpox-specific training | ||||
| No | 52 (2.6) | 248 (97) | Ref | |
| Yes | 38 (83) | 1 (17) | 0.15 (0.02-1.1) | 0.17 (0.02-1.2) |
| Others*=Radiographers and pharmacists, Lower level**= Health centre (HC) III and II and Higher level**= Hospitals and HC IV | ||||
Table 6: Factors associated with knowledge towards mpox among healthcare workers’, Uganda, August–September, 2024

Joyce Owens Kobusingye1,&, Richard Migisha1, Emmanuel Mfitundinda1, Hannington Katumba1, Joanita Nalwanga1, Daniel Wenani1, Lilian Bulage1, Stella Lunkuse2, Michael Mwanga2, Benon Kwesiga1, Alex Riolexus Ario1
1Uganda Public Health Fellowship Program, Uganda National Institute of Public Health, Kampala, Uganda, 2Integrated Epidemiology, Surveillance and Public Health Emergencies, Ministry of Health, Kampala, Uganda
&Corresponding author: Joyce Owens Kobusingye, Uganda Public Health Fellowship Program, Uganda National Institute of Public Health, Kampala, Uganda, Email: jokobusingye@uniph.go.ug, ORCiD: https://orcid.org/0000-0002-7172-2938
Received: 27 Oct 2025, Accepted: 11 Jul 2026, Published: 16 Jul 2026
Domain: Infectious Disease Epidemiology
Keywords: Mpox, Knowledge, Attitude, Practice, Kasese, Mayuge, Uganda
©Joyce Owens Kobusingye et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Joyce Owens Kobusingye et al., Healthcare workers’ knowledge, attitudes, and practices regarding mpox in two affected districts of Uganda, 2024. Journal of Interventional Epidemiology and Public Health. 2026; 9(3):117. https://doi.org/10.37432/jieph-d-25-00252
Introduction: The Ministry of Health reported the first mpox cases in Uganda on July 24, 2024, in Kasese and Mayuge. Initial case investigations revealed low clinical suspicion among healthcare workers. To inform targeted interventions, we assessed the knowledge, attitude, and practices (KAP) toward mpox among HCWs and determined factors associated with mpox KAP in Kasese and Mayuge districts, Uganda.
Methods: A cross-sectional study was conducted from August–September, 2024 among healthcare workers’ (HCWs) on a day-time shift at health facilities that had either registered a confirmed, probable, or suspected mpox case in Kasese and Mayuge districts. Data related to HCWs KAP and socio-demographic characteristics were collected using a pre-tested self-administered tool. Knowledge was assessed using 15 items, attitude 7, and practices 6. Using Bloom’s cut‐off criteria ≥80% cut off was used to determine good knowledge and positive attitude, and a cut-off of ≥75% for good practices toward mpox. Modified Poisson regression was used to identify factors associated with adequate mpox knowledge at 95% confidence interval.
Results: Overall, 339 HCWs participated in the study with an 80% response rate. Of these, 253 (75%) were aged 18-35 years, 215 (63%) were female, and 62% were nurses or midwives. The majority (84%; n=286) had adequate knowledge, 297 (88%) had a bad attitude, and 326 (96%) demonstrated poor mpox practices. Being a laboratory technician (aPR=2.7, 95% CI:1.0-7.2) was associated with adequate knowledge of mpox.
Conclusion: Surveyed HCWs demonstrated adequate knowledge; however, their attitude and practices toward mpox were suboptimal. There is a need for targeted training and mentorship, including simulation exercises, to translate knowledge into actionable and effective outbreak management practices and a positive attitude during similar outbreaks.
Mpox is an infectious disease caused by the monkeypox virus (MPXV) that primarily affects the skin and mucous membranes with a case-fatality rate (CFR) less than 10%, varying by clade type and route of exposure [1]. Globally, the CFR across all ages is about 0.2%, and cases have been reported in more than 122 countries [1,2]. Anyone can acquire mpox, including children, pregnant women, sex workers, immunosuppressed individuals, and men who have sex with men; however, healthcare workers (HCWs) face heightened risk because they are often the first point of contact for patients seeking care [3,4].
World Health Organization (WHO) declared mpox as a Public Health Emergency of International Concern (PHEIC) on August 14, 2024, as a result of an upsurge of mpox cases globally [5]. Despite mpox being a re-emerging disease, knowledge among HCWs, the first point of contact and care, remained limited. Lessons from the COVID-19 response highlighted critical gaps: inadequate disease knowledge and clinical management, wastage of medical supplies, and delayed actions that contributed to secondary community transmission [6].
In Africa, studies assessing HCWs’ knowledge, attitude and practice (KAP) towards mpox have highlighted mixed results. In Nigeria, a study revealed a fair (45%) knowledge level of mpox and positive attitudes, while another highlighted adequate knowledge (71%) among most HCWs [7]. In Burundi, related work documented <50% knowledge and very poor mpox-related practices, with many HCWs lacking confidence to diagnose and prevent mpox in their workplaces [8]. Together, these findings highlight the need for early KAP assessments among HCWs to respond effectively to contact-transmissible infections such as mpox.
On July 24, 2024, the Ministry of Health (MoH) Uganda reported two confirmed cases of mpox in Kasese District [9]. On August 19, 2024, a third mpox case was confirmed in Mayuge District and as of September 30, 2024, Uganda had reported a cumulative of 10 confirmed mpox cases across five districts, with no deaths recorded. Laboratory testing indicated circulation of clade 1b [10]. Before the outbreak in Uganda, the degree of cross-border transmission and epidemiological linkage between the outbreaks in DRC and Uganda was not fully quantified. It only became clearer by September 2024 that cases, especially in the West near the DRC border, were likely part of a larger regional crisis rather than isolated events, highlighting transnational spread [11]. Similarly, the full extent of Clade I’s circulation and its specific epidemiological profile in the context of the post-2022 global mpox landscape was not fully known [10–12]. Confirmation that Clade I was the dominant and essentially exclusive strain causing human illness in Uganda and detailed data on its case fatality rate in the current outbreak were solidified around September 2024 [4]. The potential for sustained and efficient human-to-human transmission, particularly through sexual contact, was a major question. Before late 2024, sexual transmission was considered a hallmark of the global Clade IIb outbreak, but not typical for Clade I. It was unknown whether the mpox case demographics had shifted to mirror the pattern seen in the 2022 global outbreak (affecting men who had sex with men or MSM), including in DRC [13]. Given the novelty of this outbreak in Uganda and the need to rapidly interrupt transmission, an early assessment of HCWs’ KAP was warranted. We assessed the KAP and factors associated with knowledge toward mpox among HCWs in Kasese and Mayuge districts, August–September, 2024, to inform the ongoing response.
Study design, setting and study population
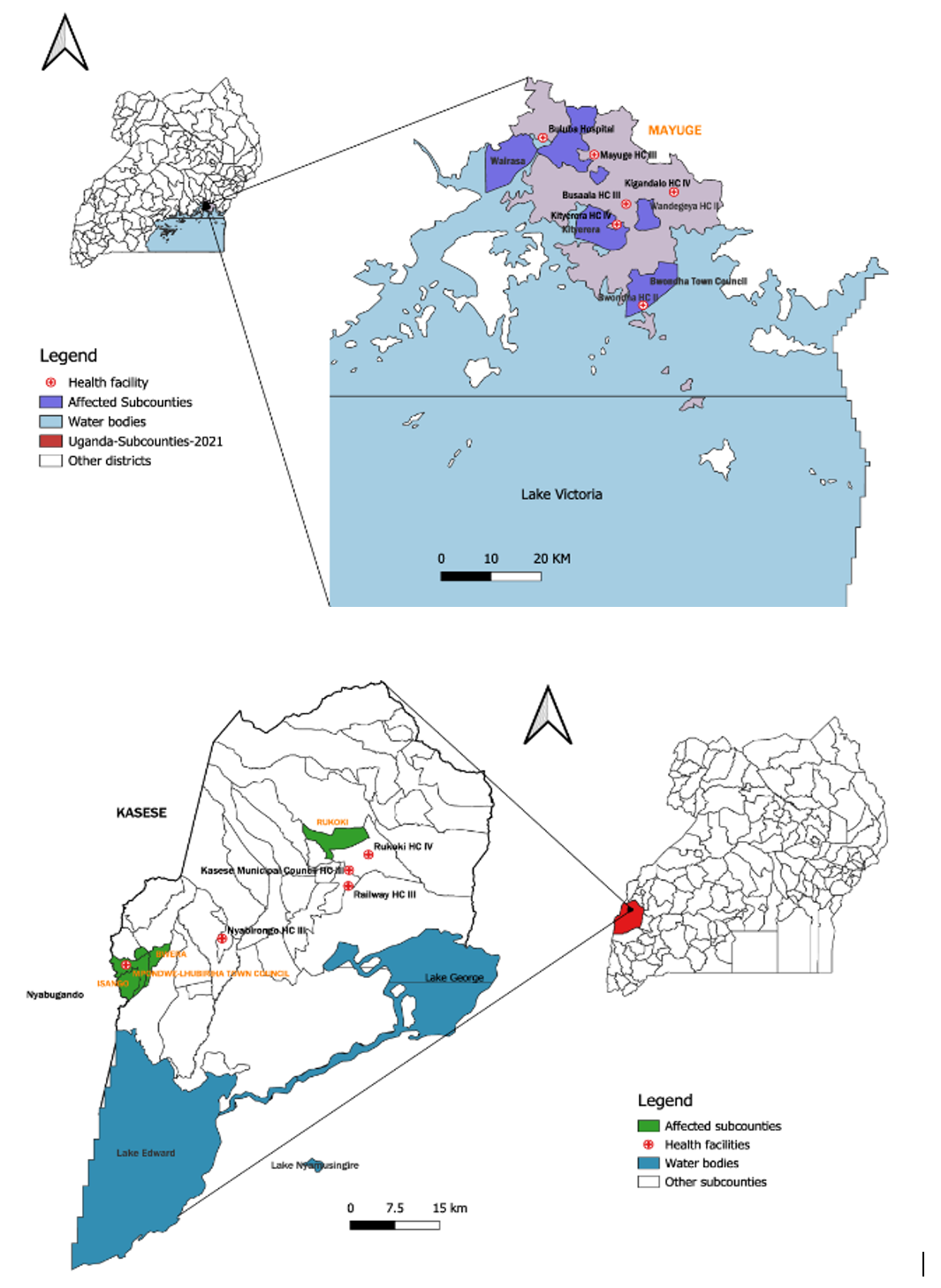
A cross-sectional study was conducted among HCWs working at selected health facilities in Kasese and Mayuge districts, August 1–September 30, 2024 (Table 1). Kasese is a border district bordering the North Kivu Province of the Democratic Republic of Congo (DRC) to the West, where an active mpox outbreak was ongoing at the time (Figure 1). Mayuge District is located in the Eastern region of Uganda. Both districts had registered five confirmed mpox cases at the time of the study (Figure 1). Eligible HCWs adults (≥18 years) who consented to participate in the study: medical doctors, nurses, midwives, intern doctors, laboratory assistants, laboratory technologist, and pharmacists were included.
Sample size and sampling procedure
We calculated the sample size using a single population proportion formula, considering a 50% prevalence of KAP from previous studies, a 5% margin of error at a 95% confidence level, i.e. N=(1.96)2 *0.5*0.5/(0.05)2 =384. The adjusted sample size was 426 after allowing for a non-response rate of 10%. We obtained a list of health workers at each randomly selected health facility, and using simple random sampling in Microsoft Excel, we selected the participants, ensuring that each HCW had an equal chance of being included in the study.
Data collection and study variables
A pre-tested self-administered questionnaire was adapted from previous studies on infectious disease outbreaks: COVID-19 and Ebola, and WHO guidance on prevention and control of mpox [4,11]. The questionnaire included questions on socio-demographic characteristics: age, sex, marital status, cadre, years of experience in health service and level of education, adapted from previous studies. KAP was assessed based on the following aspects of mpox, adapted from: mpox clinical features, transmission dynamics, prevention measures, mpox virulence and threat of transmission, treatment, patient care, training, involvement in mpox-related activities and associated knowledge factors [2,7,12]. There were 15 questions assessing participant understanding of mpox: clinical manifestations, causative agent, mode of transmission, treatment, information on mpox, source of information and incubation period of mpox. The six practice items included HCWs mpox suspicion index, screening, treatment and care of mpox patients, infection prevention and control practices, training and mentorship during mpox.
Validity and reliability of study instrument
The content validity of the questionnaire was reviewed by four public health professionals, including epidemiologists. They reviewed the variables in the tools for context, scope, clarity, appropriateness of language, relevance, and comprehensiveness and adjustments were made accordingly. The evaluation process involved multiple rounds of review to ensure alignment with the intended constructs. Recommendations were adjusted into the final questionnaire, which enhanced its quality to collect the intended data. The questionnaire was also pre-tested among 20 HCWs in Kampala district, and minor changes were made to the questionnaire before we deployed it for the study. Reliability was assessed using the Cronbach’s alpha test, which yielded a score of at least 0.68 (~0.7) for all sections in the questionnaire, indicating good reliability.
Data management and analysis
Data were extracted from the electronic Kobo Collect tool, cleaned in Microsoft Excel, and analysed using STATA version 14 (StataCorp, College Station, Texas, USA). We used frequencies, means, and percentages to summarise categorical and numerical data for the presentation of descriptive statistics. Bloom’s modified cut-off point was used to determine adequate knowledge and positive attitude (≥80%), and good practice toward mpox (≥75%) [14].
There were 15 items assessing knowledge. For the first 7 questions, “yes” was indicated as a correct answer and scored 1, and “no or don’t know” answers were scored 0. The score was added to give a total knowledge score that ranges from 0 to 7. The rest of the 8 questions depended on the number of choices correctly chosen. Multiple responses were allowed, where three or more correct options chosen had a value of 1, and “don’t know or non-response” choices had a value of 0. Knowledge was assessed on a 15-point scale. Based on Bloom’s cut-off criteria, scores of ≥80% (≥12 points) were classified as “adequate knowledge” while scores <80% (<12 points) were classified as “inadequate knowledge”. The reason for using an ≥80% point cut off value for knowledge was by considering that the majority of HCWs receive health-related information from the Ministry of Health on the status of health for the country and neighbouring countries where outbreaks are ongoing, attend training courses with respect to infection prevention and control and generally infectious disease prevention and control mechanisms [15].
Regarding attitude, 7 items on attitude-related aspects were assessed. The items were scored on a 3-point Likert scale (disagree, agree and don’t know). The responses were scored 1 for disagree, 2 for agree and 0 for don’t know or non-response. The cumulative score for all 7 questions was 0–14 points per participant. HCWs who had a score ≥80% (11-14 points) were categorised as having a positive attitude and a bad attitude if they scored <80%. The reason for using a ≥80% point cut off for attitude was by considering the uncontrolled nature of the mpox epidemic: cross-border transmission and HCWs concerns and fears of getting infected during care, given the low suspicion index, inadequate screening and shortage of personal protective equipment at the time [16–18]
Regarding mpox practices, a six-item scale assessed as “yes”, “no”, “don’t know”, and non-response was used. “Yes” was indicated as a correct answer and scored 1, while “no, don’t know and non-response” answers were scored 0. Multiple responses were allowed. The cumulative score for all 6 questions ranged from 0-6 points for each participant. Scores ≥75% (≥5 out of 6) to determine good practice and poor mpox practices if the score was <75%. The reason for using this cut-off value for practice was by considering the contagiousness of the mpox disease, HCWs to whom the prevention practices for any infectious disease are mandatory to protect themselves, the patients in their care and the rest of the community [15,17].
We used Modified Poisson regression analysis with robust standard errors to determine factors associated with having adequate mpox knowledge. Bivariate analysis was conducted to determine factors independently associated with knowledge toward mpox at a p-value of < 0.2. In multivariable analysis, a p-value of <0.05 at 95% confidence interval using prevalence ratios (PR) was used to determine factors significantly associated with adequate knowledge after checking for collinearity of variables. We controlled for clustering at the health facility level with robust standard errors.
Ethical consideration
This outbreak investigation was in response to a public health emergency and was therefore determined to be non-research. The Ministry of Health gave permission to investigate this outbreak. In agreement with the International Guidelines for Ethical Review of Epidemiological Studies by the Council for International Organizations of Medical Sciences (1991) and the Office of the Associate Director for Science, US CDC/Uganda, it was determined that this activity was not human subject research and that its primary intent was public health practice or disease control activity (specifically, epidemic or endemic disease control activity). This activity was reviewed by the US CDC and was conducted consistent with applicable federal law and CDC policy. §§See, e.g.,45 C.F.R. part 46, 21 C.F.R. part 56; 42 U.S.C. §241(d); 5 U.S.C. §552a; 44 U.S.C. §3501 et seq. We sought permission to conduct the investigation from the District health authorities of Kasese and Mayuge Districts. We obtained written consent from the HCWs who participated in the study. We also informed them that their participation was voluntary and their refusal to participate would not have any negative consequences in line with their work. No participant identifiers were kept in the dataset.
Socio-demographic characteristics of healthcare workers’
Four hundred twenty-six HCWs were approached. Of these, 339 completed the questionnaire, giving a response rate of 80%. Most (75%) were 18-35 years old; the mean age was 31 (SD± 9.3); 63% (n=215) were female; 62% were nurses and midwives, and 58% were certificate holders by education level (Table 2).
Knowledge towards mpox among healthcare workers’
The majority, 84% (n=286), demonstrated adequate knowledge. Additionally, 87% (n=295) had access to information on mpox, 62% (n=211) were aware of the ongoing mpox outbreak in Uganda, and 79% (n=268) knew that mpox is a viral infection (Table 3). The main sources of health information among HCWs were through media outlets: newspapers, radio stations, televisions (93% [n=319/339]) and health platforms: Ministry of Health sites and health facilities (81% [n=273/339]) (Table 4). However, 88% of the HCWs had not received any training in mpox.
Attitude toward mpox among healthcare workers’
Overall, 88% (n=297) of the participants demonstrated a bad attitude toward mpox. The majority (313 [92%]) of the HCWs reported that they would go to the health facility once they started presenting with mpox clinical features (Table 5). Most HCWs (84%) agreed that mpox is a serious disease that could cause death, and that infection can be transmitted through direct contact with an infected person (85%).
Practices towards mpox among healthcare workers
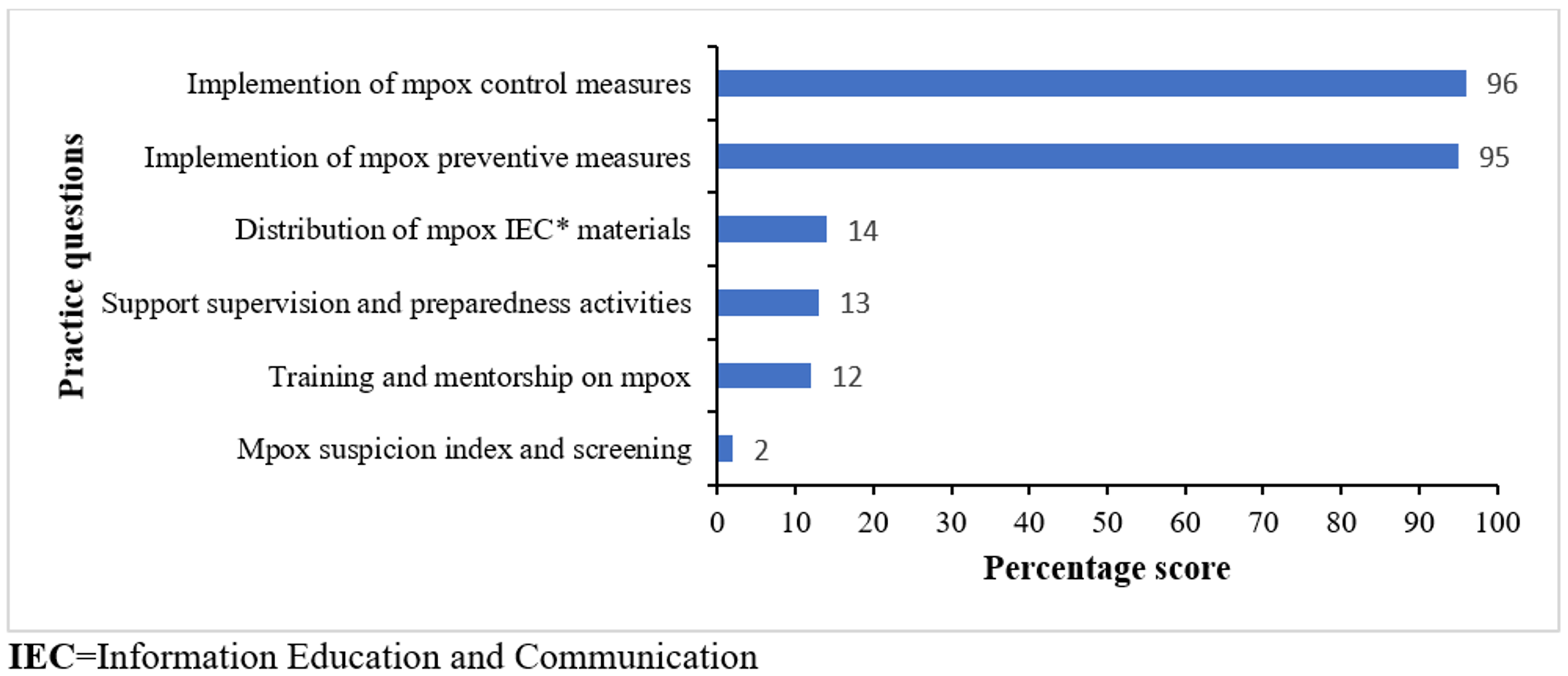
Overall, 96% (n=326) of the participants demonstrated poor mpox practices. The majority (95%, [n=321]) of the HCWs had not implemented mpox prevention measures (Figure 2). Only 39 (12%) had trained or mentored other people on different aspects of mpox, and 46 (14%) HCWs reported having participated in the distribution of mpox information and education materials, and only 7 (2%) had a good mpox suspicion index and screening practices.
Factors associated with knowledge of mpox among healthcare workers’
The majority of socio-demographic characteristics were not associated with knowledge at bivariate analysis. In multivariable analysis, cadres who were laboratory technicians had a 2.7 times higher prevalence of knowledge compared to the clinicians (aPR = 2.7; 95% CI: 1.0–7.2) (Table 6).
This study evaluated HCWs’ KAP toward mpox and identified factors associated with knowledge in the first two districts to register mpox cases in Uganda. Most HCWs demonstrated adequate knowledge of mpox, obtaining information from social media, mass media, colleagues, and Ministry of Health sources. Healthcare workers had bad attitudes towards mpox although many recognized that mpox is a serious and were willing to seek care once they suspected having it. Practices were very low demonstrated in: low clinical suspicion, misdiagnosis, limited screening, and minimal participation in preparedness or surveillance activities. Adequate knowledge was higher among medical laboratory technologists compared to other cadres. Overall, our findings highlight the need for strategies that translate knowledge into evidence-based practices to strengthen preparedness, response and creating a positive attitude expected of frontline health workers, who are the first point of contact during similar infectious diseases outbreaks.
In this study most of the HCWs had adequate knowledge toward mpox, which could have been attributed to more robust risk communication on social media platforms, situation reports and health sites by Ministry of Health and implementing partners focused on the mpox outbreak. These findings are consistent with reports from Saudi Arabia and Lebanon, where 55% and 34% of physicians, had adequate knowledge of mpox [19,20]. Conversely, some studies have documented lower knowledge levels, 48% in Saudi Arabia among the general population and 53% in Nepal among physicians, reflecting contexts where outbreaks were new or no cases had been reported, and public education was limited [21,22].
Being a medical laboratory technologist (MLT) was associated with adequate mpox knowledge in this study. In the early phase of the mpox outbreak in Uganda, MLTs were at the forefront of the response with many involved in sample collection, rapid expansion of testing capabilities in the districts, employing various diagnostic modalities: polymerase chain reaction testing, antigen testing, and serological testing, and adapting to the evolving mpox guidelines and protocols. Similar studies in Lebanon and Nigeria highlighted, being a nurse and a physician was associated with having adequate knowledge [7,20]. While this expertise highlights knowledge gaps among other healthcare workers, it also presents an opportunity to leverage MLTs in training and supporting clinicians, nurses, and midwives to strengthen outbreak preparedness and response.
Only 12% of HCWs demonstrated positive attitude in our study possibly due to differences in healthcare education and training before the mpox outbreak although this was expected given the level of knowledge that the majority of them had. These findings resonate with the low positive attitudes reported in Saudi Arabia (15.2%) and (30%) among the general public in Lebanon [19,20]. These findings highlight the critical role of timely information in shaping HCWs’ perceptions during outbreak response. Another study among Nepalese reported found that the majority of HCWs who had studied mpox in medical school had a negative attitude, possibly after being aware of its potential consequences [21]. Similar to our findings, there’s need for training at all levels to emphasize emerging and re-emerging diseases as they could potentially transform into epidemics.
Despite having adequate knowledge, the majority of HCWs demonstrated suboptimal mpox practices including low suspicion index, screening: limited recognition of basic clinical features, minimal experience in managing mpox patients (care and treatment), and less mentorship of peers on transmission, prevention, and control measures. In contrast, a study in Vietnam reported that 52% of HCWs had good mpox practices, with the majority adhering to preventive measures, following Ministry of Health guidelines, and implementing infection prevention and control strategies to protect themselves [23].
Translating knowledge into practice requires moving beyond one-time training to a holistic approach that addresses all the barriers before and during outbreak response. Bridging this gap among HCWs is essential for effective outbreak control, patient safety and continuity of healthcare service delivery [24]. Strategies like interactive and scenario-based learning using realistic case simulations, role-playing, and table-top exercises allow HCWs to practice donning and doffing PPE and making clinical decisions in a safe environment [24]. Other practical measures that can bridge this gap include experimental learning that develops and reinforces skills like Just-In-Time Training (JITT); providing short, immediate, accessible, and actionable information at the point of care for use [25,26]. Adoption of implementation science frameworks like the consolidated framework for implementation research (CFIR) and practical, robust implementation and sustainability model (PRISM) which aim to assess and diagnose implementation of current and failed strategies to address challenges [27,28].
Overall, our study findings have some public health and policy implications for outbreak preparedness and response. Despite adequate knowledge reported among HCWs, gaps exist in mpox-related practices and attitudes, highlighting the need for structured mentorship, training and continuous professional development. Policymakers and health administrators could prioritize targeted capacity-building programs, including simulation-based exercises and JIIT, to translate knowledge into effective infection prevention, case detection, and patient management practices. Additionally, leveraging digital platforms, official guidelines, and routine situation updates could ensure the timely dissemination of outbreak information.
Study limitations
Our study was subject to some limitations. First, data collection relied on self-administered questionnaires, introducing self-report and recall bias, especially when reporting mpox practices, a potential for social desirability that may have overestimated knowledge and attitudes or underestimated gaps in practice. Secondly, the cross-sectional design captures only a single point in time, restricting causal inference and failing to account for changes in knowledge and practices as the outbreak evolved or interventions were implemented. Finally, unmeasured contextual factors, such as workload, resource availability, training among a small group, and institutional policies, may have influenced mpox-related practices and attitudes, meaning the observed association may not have fully reflected the optimal determinants for adequate knowledge. Despite these limitations, our study provides valuable insights into HCWs’ preparedness and identifies areas for targeted training and mentorship to strengthen similar outbreak responses.
The HCWs surveyed demonstrated adequate knowledge; however, their attitudes and practices were suboptimal. There is a need for targeted training and on-the-job mentorship, including simulation exercises, to translate knowledge into actionable and effective outbreak management practices and a positive attitude during similar outbreaks.
What is already known about the topic
What this study adds
The authors declare no competing interests. Lilian Bulage is an Associate Editor at the Journal of Interventional Epidemiology and Public Health (JIEPH) and a co-author of this manuscript. In line with the journal’s conflict of interest policy, she was fully recused from the peer review process and had no involvement in editorial handling or decision-making for this submission. An independent editor oversaw the review and decision-making process.
Availability of data and materials
The datasets upon which our findings are based belong to the Uganda Public Health Fellowship Program. For confidentiality reasons, the datasets are not publicly available. However, the datasets can be availed upon reasonable request from the corresponding author with permission from the Uganda Public Health Fellowship Program (Ms Barbra Loyce Khoba works as the Information Technology and Learning Officer at the institute. Email: barbra@uniph.go.ug.).
This study was supported by the President’s Emergency Plan for AIDS Relief (PEPFAR) through the United States Centres for Disease Control and Prevention Cooperative Agreement number GH001353-01 through Makerere University School of Public Health to the Uganda Public Health Fellowship Program, Ministry of Health. The contents of this manuscript are solely the responsibility of the authors and do not necessarily represent the official views of the US Centres for Disease Control and Prevention and the Department of Health and Human Services, Makerere University School of Public Health, or the Uganda Ministry of Health.
We acknowledge the management of Kasese and Mayuge District Local Government for the stewardship, and the participating HCWs for their participation in the investigation. We also thank the Ministry of Health, Public Health Emergency Operations Centre, and the US CDC for funding this investigation.
JOK: Conceptualized, designed, data curated and analyzed, wrote the report and manuscript. RM reviewed the study instrument, reviewed the report and manuscript. EM participated in methodology design and data analysis. HK, JN and DW participated in data collection. LB, SL, MW, BK and ARA reviewed the manuscript to ensure scientific integrity and intellectual content.
| Name | Location/District | Level |
|---|---|---|
| Bwera General Hospital | Kasese | Hospital |
| Mount. Saint. Mary Hospital | Kasese | Hospital |
| Saint. Paul Hospital | Kasese | Hospital |
| Kagando Hospital | Kasese | Hospital |
| Rukooki Health Centre | Kasese | HC IV |
| Nyabirongo Health Centre | Kasese | HC III |
| Nyabugando Health Centre | Kasese | HC III |
| Kasese Municipal Health Centre | Kasese | HC III |
| Railway Health Centre | Kasese | HC III |
| Bukangara Health Centre | Kasese | HC III |
| Buluba Hospital | Mayuge | Hospital |
| Mayuge Health Centre | Mayuge | HC IV |
| Kityerera Health Centre | Mayuge | HC IV |
| Kigandalo Health Centre | Mayuge | HC IV |
| Busaala Health Centre | Mayuge | HC III |
| Bwondha Health Centre | Mayuge | HC II |
| Wandegeya Health Centre | Mayuge | HC II |
| Characteristics | Frequency (n) | Percentage (%) |
|---|---|---|
| Age (years) | ||
| 18-35 | 253 | 75 |
| ≥36 | 86 | 25 |
| Sex | ||
| Female | 215 | 63 |
| Male | 124 | 37 |
| Marital status | ||
| Married | 149 | 44 |
| Un-married | 190 | 56 |
| Level of education | ||
| Masters | 10 | 2.9 |
| Bachelors | 25 | 7.4 |
| Diploma | 92 | 27 |
| Certificate | 196 | 58 |
| Missing | 16 | 4.7 |
| Years of experience | ||
| <5 | 184 | 60 |
| 5-10 | 62 | 20 |
| >10 | 61 | 20 |
| Cadre | ||
| Clinicians | 69 | 21 |
| Nurses/midwives | 210 | 62 |
| Laboratory technicians | 52 | 15 |
| Others* | 8 | 2 |
| Health facility level | ||
| Hospital | 116 | 34 |
| HC IV | 169 | 50 |
| HC III | 44 | 13 |
| HC II | 10 | 3 |
| Source of information | ||
| Social media platforms | 232 | 71 |
| Health facilities | 2 | 0.6 |
| People* | 94 | 29 |
| Table 3: Assessment of knowledge towards mpox among healthcare workers’, Uganda, August–September, 2024 | ||
| Variable | Frequency | Percentage |
|---|---|---|
| Accessed to mpox information | ||
| Yes | 295 | 87 |
| No | 44 | 13 |
| Received training on mpox | ||
| Yes | 39 | 12 |
| No | 300 | 88 |
| Aware of the causative agent for mpox | ||
| Yes | 268 | 79 |
| No | 71 | 21 |
| Aware of ongoing mpox outbreak | ||
| Yes | 211 | 62 |
| No | 128 | 38 |
| Aware of clinical manifestations for mpox | ||
| Yes | 43 | 13 |
| No | 296 | 87 |
| Aware of availability of mpox vaccine | ||
| Yes | 100 | 29 |
| No | 239 | 71 |
| Table 4: Source of health information among healthcare workers’, Uganda, August-September, 2024 | ||
| Source of information | Frequency | Percentage (%) |
|---|---|---|
| Media outlets* | 319 | 93 |
| Health platforms* | 273 | 81 |
| Colleagues* | 167 | 49 |
| Social media* | 178 | 43 |
| Community* | 87 | 26 |
| Media outlets=Radios, Television, Newspaper, Health platforms=Ministry of Health, Health facility, Colleagues=Healthcare workers, Friends and family, Social media=WhatsApp, Facebook, X, Google, Instagram, Community=Voluntary health teams, Church leaders, Community leaders | ||
| Table 5: Assessment of attitude towards mpox among healthcare workers, Uganda, August–September, 2024 (n=339) | ||||||
| Characteristics | Agree (n) | (%) | Disagree (n) | (%) | Don’t know (n) | (%) |
|---|---|---|---|---|---|---|
| One should go to hospital if they present mpox clinical features | 313 | 92 | 4 | 1.2 | 22 | 6.5 |
| Mpox transmission can increase by direct contact | 288 | 85 | 4 | 1.2 | 47 | 14 |
| Mpox is a serious disease | 286 | 84 | 9 | 2.7 | 44 | 13 |
| Mpox infection could increase by overcrowding | 279 | 82 | 11 | 3.2 | 49 | 14.5 |
| Hand washing could protect someone from mpox | 251 | 74 | 40 | 11.8 | 48 | 14.2 |
| Wearing PPE* does not protect one from mpox | 35 | 10 | 269 | 79.4 | 35 | 10 |
| Mpox disease does not lead to death | 27 | 7.9 | 276 | 81 | 36 | 11 |
| PPE=Personal protective equipment | ||||||
| Table 6: Factors associated with knowledge towards mpox among healthcare workers’, Uganda, August–September, 2024 | ||||
| Characteristics | Knowledge level | uPR 95% CI | aPR 95% CI | |
|---|---|---|---|---|
| Adequate n (%) | Inadequate n (%) | |||
| Age (years) | ||||
| 18-35 | 214 (75) | 39 (74) | Ref | |
| ≥36 | 72 (25) | 14 (26) | 1.1 (0.57-1.9) | – |
| Sex | ||||
| Female | 181 (63) | 34 (64) | Ref | |
| Male | 105 (37) | 19 (36) | 0.97 (0.55-1.7) | – |
| Marital status | ||||
| Married | 128 (45) | 21 (40) | Ref | |
| Un-married | 158 (55) | 32 (60) | 1.2 (0.69-2.1) | – |
| Level of education | ||||
| Masters | 8 (2.8) | 2 (3.8) | 2.5 (0.35-18) | – |
| Bachelors | 23 (8.0) | 2 (3.8) | Ref | |
| Diploma | 75 (26) | 17 (32) | 2.3 (0.53-10) | – |
| Certificate | 169 (59) | 27 (51) | 1.7 (0.41-7.3) | – |
| Years of experience | ||||
| <5 | 140 (54) | 23 (48) | Ref | |
| ≥5 | 119 (46) | 25 (52) | 1.2 (0.69-2.2) | – |
| Designation | ||||
| Clinicians | 63 (22) | 6 (11) | Ref | |
| Nurses/midwives | 178 (62) | 32 (60) | 1.8 (0.73-4.2) | 1.7 (0.69-3.9) |
| Laboratory technicians | 39 (14) | 13 (25) | 2.9 (1.1-7.6) | 2.7 (1.0-7.2) |
| Others* | 6 (2.0) | 2 (3.8) | 2.9 (.58-14) | 2.9 (0.59-15) |
| Health facility level** | ||||
| Lower level | 40 (14) | 14 (26) | Ref | |
| Higher level | 246 (86) | 39 (74) | 2.6 (1.7-3.8) | – |
| Access to mpox information | ||||
| No | 42 (15) | 2 (3.8) | Ref | |
| Yes | 244 (85) | 51 (96) | 3.8 (0.93-15) | 3.4 (0.85-14) |
| Previous mpox-specific training | ||||
| No | 52 (2.6) | 248 (97) | Ref | |
| Yes | 38 (83) | 1 (17) | 0.15 (0.02-1.1) | 0.17 (0.02-1.2) |
| Others*=Radiographers and pharmacists, Lower level**= Health centre (HC) III and II and Higher level**= Hospitals and HC IV | ||||