Lessons from the field | Open Access | Volume 9 (Suppl 13): Article 04 | Published: 22 May 2026

Views: 669
Menu, Tables and Figures
| Variable | Frequency | Percentage |
|---|---|---|
| Sex | ||
| Female | 101 | 26.6 |
| Male | 279 | 73.4 |
| Age | ||
| 18-30 | 229 | 60.3 |
| 31-49 | 142 | 37.4 |
| 50+ | 9 | 2.2 |
| Main purpose of attendance | ||
| Tourism/adventure/partying | 181 | 47.6 |
| Commercial/service provision | 145 | 38.2 |
| Security | 54 | 14.2 |
Table 1: Sociodemographic characteristics of the respondents
| Variable | N=380 | Experienced signs and symptoms | χ² | |
|---|---|---|---|---|
| Yes = 177 n (%) | No = 203 n (%) | |||
| Sex | 380 | 177 (Total) | 203 (Total) | 0.48 |
| Female | 101 | 44 (43.6) | 57 (56.4) | |
| Male | 279 | 133 (47.7) | 146 (52.3) | |
| Age | 380 | 177 | 203 | 0.29 |
| 18-30 | 229 | 101 (44.1) | 128 (55.9) | |
| 31-49 | 142 | 70 (49.3) | 72 (50.7) | |
| 50+ | 9 | 6 (66.7) | 3 (33.3) | |
| Main purpose of attendance | 380 | 177 | 203 | 0.01* |
| Tourism/adventure/partying | 181 | 83 (45.9) | 98 (54.1) | |
| Commercial/service provision | 145 | 59 (40.7) | 86 (59.3) | |
| Security | 54 | 35 (64.8) | 19 (35.2) | |
| * Significant difference at p<0.05 | ||||
Table 2: Signs and symptoms, by background characteristics of the respondents
Alex Mulyowa1,&, Cathelyne Kobumanzi1, Faith Ayesiga1, Irene Nakaziba1, Oliver Akello1, Salim Hasahya1, Mathius Amperiize1, Roseline Nuwamanya1, Edward Sebaggala1, Connie Nait1, Bernard Lubwama2, Suzanne Namusoke Kiwanuka1
1Department of Health Policy, Planning and Management, Makerere University School of Public Health, Kampala, Uganda, 2Division of Integrated Epidemiology and Surveillance, Ministry of Health, Kampala, Uganda
&Corresponding author: Alex Mulyowa, Department of Health Policy, Planning and Management, Makerere University School of Public Health, Kampala, Uganda, Email: alexandermulyowa@gmail.com ORCID: https://orcid.org/0000-0003-3627-7637
Received: 27 Oct 2025, Accepted: 15 May 2026, Published: 22 May 2026
Domain: Field Epidemiology
Keywords: surveillance, syndromic, mass gatherings, infectious disease, Uganda
©Alex Mulyowa et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Alex Mulyowa et al. Disease surveillance at a mass gathering: Lessons from the 2024 Nyege Nyege festival, Uganda. Journal of Interventional Epidemiology and Public Health. 2026; 9(Suppl 13):04. https://doi.org/10.37432/jieph-d-25-00254
Introduction: Mass gatherings are often associated with numerous public health challenges. In Uganda, recreational gatherings are gaining traction; however, little to no surveillance for key priority diseases of public health concern has been conducted. We conducted syndromic surveillance during the 2024 Nyege Nyege festival in Jinja City, Uganda.
Methods: This was a cross-sectional study. We collected data on sociodemographic characteristics and signs and symptoms from 380 respondents from 13th to 17th November 2024. Data was collected electronically using Kobo Collect. Descriptive analysis was performed using STATA version 16. Results were presented in the form of tables and graphs.
Results: Of the 380 respondents, 73.4% (n=279) were male, while 60.3% (n=229) were aged 18-30 years. The proportion of respondents reporting signs and symptoms differed significantly by main purpose of attendance (χ², p=0.01). Security personnel had the highest proportion reporting symptoms (64.8%, 35/54), compared with respondents attending for tourism/adventure/partying (45.9%, 83/181) and those involved in commercial/service provision (40.7%, 59/145). Headaches (28.2%) and body pains (10.7%) were the most commonly reported signs and symptoms among the respondents.
Conclusion: Nearly half of the respondents had experienced at least one sign or symptom of illness during the festival. The findings underscore the need for targeted interventions such as health education or risk communication campaigns on early detection of and seeking care against any emerging health threat.
The World Health Organization (WHO) defines mass gatherings as spontaneous or organised events that attract large numbers of attendees and strain local resources [1]. These gatherings may include religious celebrations, concerts, sporting events, street fairs, parades, and political rallies, each exhibiting distinct risk profiles [2]. Risk factors commonly linked to mass gatherings include high crowd density, restricted points of access, limited crowd control, and inadequate on-site medical care [1]. Poor preparation for extreme weather events, such as sudden changes in temperature, also further contributes to health and safety risks for attendees [1]. Specifically, mass gatherings pose distinct public health challenges regarding infectious disease surveillance and control [3, 4]. Examples of such challenges have been highlighted by the emergence of diseases such as COVID-19 and, more recently, Mpox [5, 6].
The Nyege Nyege festival, held annually in Uganda, has earned international acclaim as a lively celebration of music, art, and culture [7]. This four-day international music festival attracts more than 20,000 revellers [8]. However, one of the primary concerns is the heightened risk of infectious disease transmission. Previous studies have shown that the risk of transmission is almost twofold in crowded settings, especially if individuals are unvaccinated [9-11]. Unlike religious gatherings such as the annual Uganda Martyrs’ Day celebrations, the recreational nature of the Nyege Nyege festival attracts a more diverse and vibrant demographic, many of whom may not be mindful of the risk of infectious disease outbreaks. Relatedly, cholera and typhoid, which are associated with poor sanitation and contaminated food or water, are particularly concerning during such an event [12]. Often, the operation of temporary food vendors, many of whom work under informal conditions, elevates the risk of foodborne illnesses [13]. Additionally, environmental health risks are likely to arise from inadequate waste management or water pollution [14].
Syndromic surveillance, defined as the near real-time collection, analysis, interpretation and dissemination of health-related data in order to enable the early identification of the impact (or absence of impact) of potential health threats that may require public health action, is often advocated as a tool for the early detection of health threats, expedited outbreak responses, and the collection of valuable data to support future planning [15, 16]. It aligns with the WHO recommendations of the key considerations for public health for mass gatherings, which focus on a risk-based approach that encompasses evaluation, mitigation, and communication beginning in the early planning stages [17]. Syndromic surveillance supports these processes by strengthening situational analyses, identifying unusual events early and guiding timely response actions. However, since the inception of the Nyege Nyege festival in 2015, no surveillance for priority diseases of public health concern has been conducted during the event, despite its growing annual attendance. To address this gap, we conducted syndromic surveillance for infectious disease threats during the 2024 Nyege Nyege festival in Jinja, Uganda.
Study setting and population
The surveillance was conducted among revellers, both national and international, in Jinja City, in the eastern region of Uganda, from 13th to 17th November 2024. Jinja is along the northern shores of Lake Victoria, near the source of the Nile. According to the 2024 Uganda national census preliminary results, the city had a population of about 292,000 and a daytime population exceeding 400,000 due to its role as a commercial and industrial hub. The city offers numerous adventure activities such as water rafting, sailing, camping, bungee jumping, and swimming, among others. The scenic beauty of the leisure centres in Jinja offers numerous opportunities for sustainable tourism within the city. For this reason, the city has been considered the ideal location to host the Nyege Nyege festival for all nine editions that have so far been organised. Jinja’s location at the confluence of Lake Victoria and the source of the River Nile positions it as a focal point for vector-borne and water-borne diseases. Moreover, the festival’s timing in Uganda’s second wet season (September to November), when mosquito and parasite transmission peaks, is epidemiologically significant for surveillance. By epi week 46 (11th to 17th November 2024), Jinja had a malaria testing rate of 76.4% [18], although earlier reports from August 2024 had shown that the incidence in the district was between 250 and 450 people per 1000 per year [19].
At the time of the festival, Uganda was experiencing an active outbreak of Mpox across districts, Jinja inclusive. Given that Nyege Nyege is an international activity, and Uganda has often had disease threats of international concern e.g., Ebola and yellow fever, there was high risk of importation/exportation of diseases, risk of delayed access to healthcare because the foreigners are not familiar with existing health systems, risk of environmental risks due to short time for acclimatization and the immunity of respondents is usually unknown hence they were at risk of endemic diseases.
Data collection
The surveillance was done cross-sectionally by nine surveillance officers, using a validated data collection tool developed in KoboCollect. The surveillance officers were residents of the Field Epidemiology Training Program from Makerere University School of Public Health, supported by the African Field Epidemiology Network (AFENET). These officers were deployed under the close supervision of the Incident Command of the Division of Integrated Epidemiology and Surveillance, Ministry of Health, Uganda. This surveillance activity was also done in collaboration with both the Jinja City and District Health Offices and other institutions such as the Infectious Diseases Institute. The data tool was based on signs and symptoms for selected priority diseases such as Mpox, COVID–19 and any other Viral Haemorrhagic Fevers (VHFs) which have high transmission potential among crowds. These conditions were selected based on guidance from the Division of Integrated Epidemiology and Surveillance, Ministry of Health, and also due to the then-current context that there was an active Mpox outbreak across most districts in the country. Surveillance was also done for other common illnesses, including malaria and typhoid fever. Signs and symptoms investigation was based on suspect case definitions as per the National Technical Guidelines for Integrated Disease Surveillance and Response [20]. Signs and symptoms under investigation were: fever (temperature >37.5°C), cough, headache, generalised body weakness, peptic ulcer disease (PUD), shortness of breath, fainting or sudden collapse, abdominal pain or any unexplained bleeding. Body temperature was measured using temperature guns.
Peptic ulcer disease was defined as a respondent’s self-report of experiencing recurrent epigastric pain suggestive of ulcer disease, with or without prior diagnosis. Any other signs and symptoms reported by the respondents were also recorded by the surveillance officers. Data was collected from November 13th – 17th 2024. Other variables of interest were the respondent’s gender, age, and the duration of the signs and symptoms they were experiencing, if any. Within the crowd, surveillance officers used convenience sampling to select respondents, while at entry points, a mix of both convenience sampling and systematic sampling (where every 10th person was selected after being screened for temperature) was used to select respondents. They were all requested to take part in a brief 10-minute interview. We targeted to reach at least 450 respondents over the 5-day surveillance period, with each surveillance officer required to interview at least 10 respondents per day. However, given that some people declined to take part in the interview, we achieved a response rate of 84%.
Onsite emergency medical services were provided in designated tents from providers such as the Infectious Diseases Institute (IDI), the Uganda Red Cross Society (URCS) and Makerere University Joint AIDS Program (MJAP). Utilising medical records from each of these tents, an active case search was also instituted to identify any suspicious medical condition that warranted further attention. Individuals who exhibited any suspicious signs of infectious diseases were isolated and referred for further management. Further management was handled by the Red Cross teams who were actively on-site, 24 hours per day.
Data analysis
Data was downloaded into a Microsoft Excel file, cleaned and exported to STATA version 16 for analysis. Proportions and their corresponding percentages were computed to describe the sociodemographic characteristics of the respondents and other variables, including signs and symptoms. The results were presented using graphs and tables.
Ethical consideration
Approval was granted by the Higher Degrees Research and Ethics Committee of Makerere University School of Public Health. Verbal informed consent was obtained from all respondents. No identifying information on the respondents is presented. The surveillance was carried out in compliance with the Helsinki Declaration.
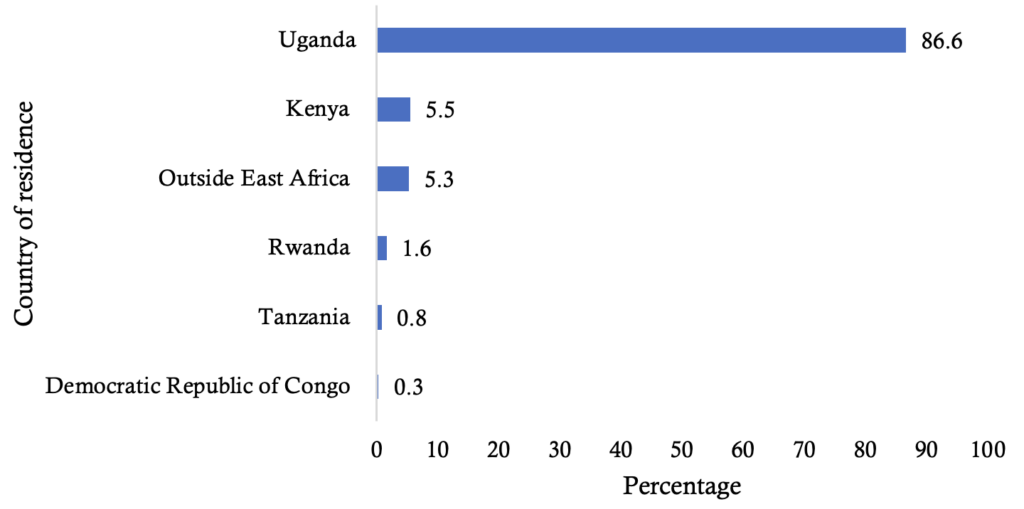
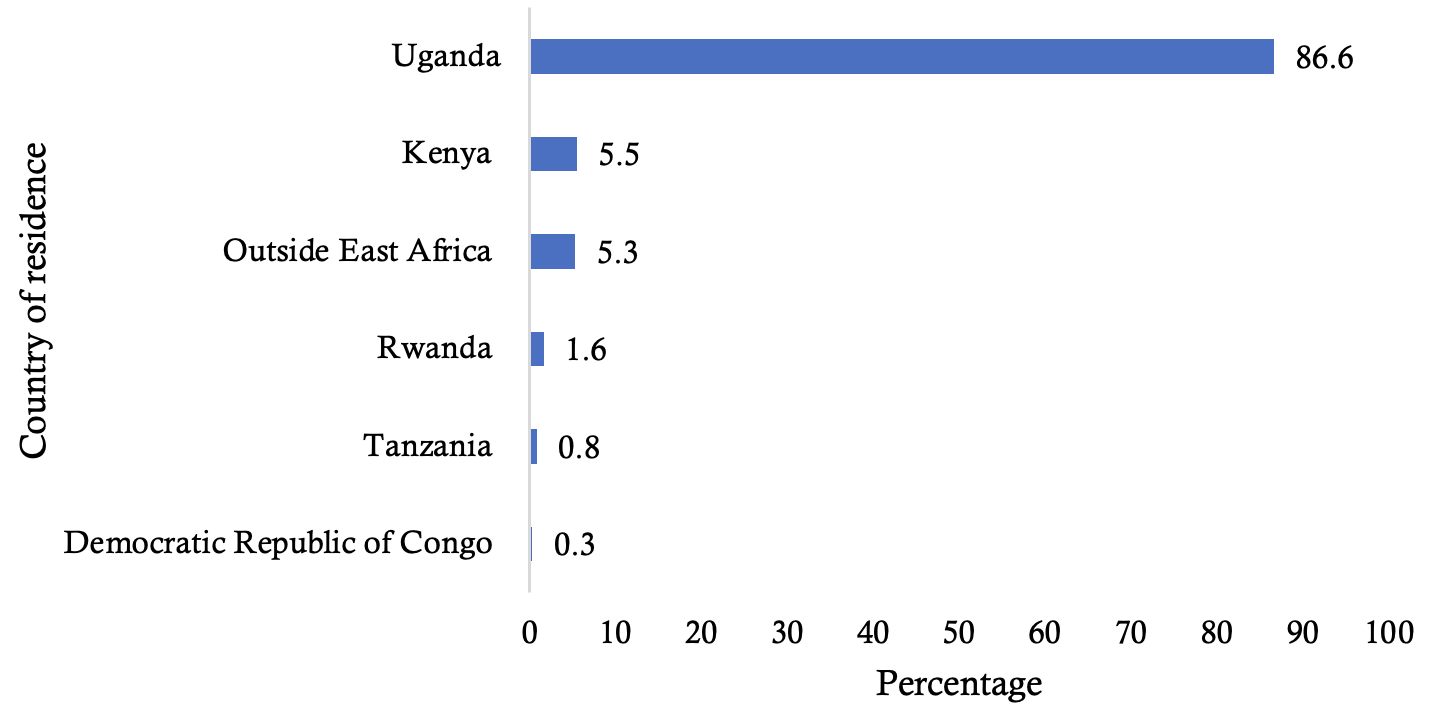
Three hundred eighty respondents were interviewed. Of these, three-fifths (60.3%, n=229) were aged 18-30 years, 73.4% (n=279) were male, while nearly half (47.6%, n=181) were in attendance mainly to party (Table 1). Furthermore, the median proportion of respondents from outside Uganda was 1.6 % (IQR: 0.55-5.4) (Figure 1).
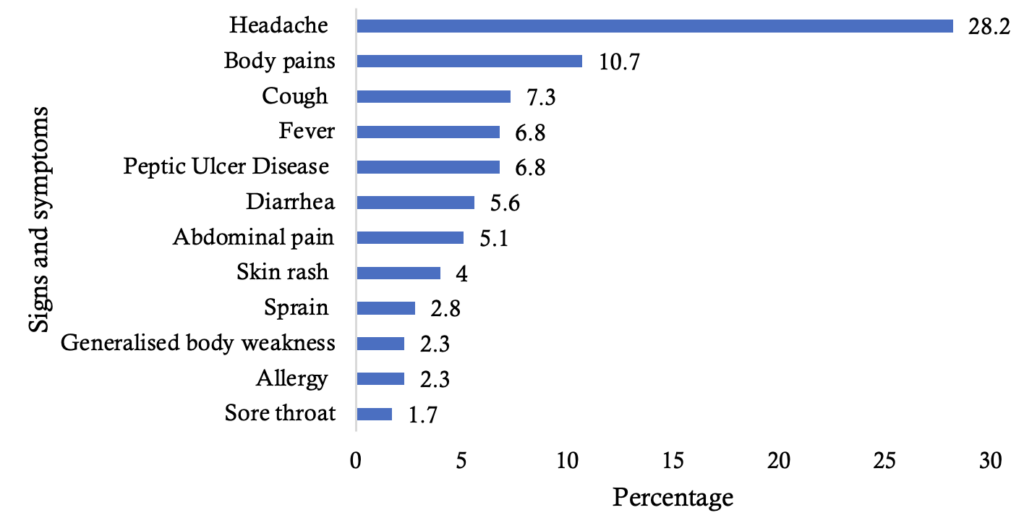
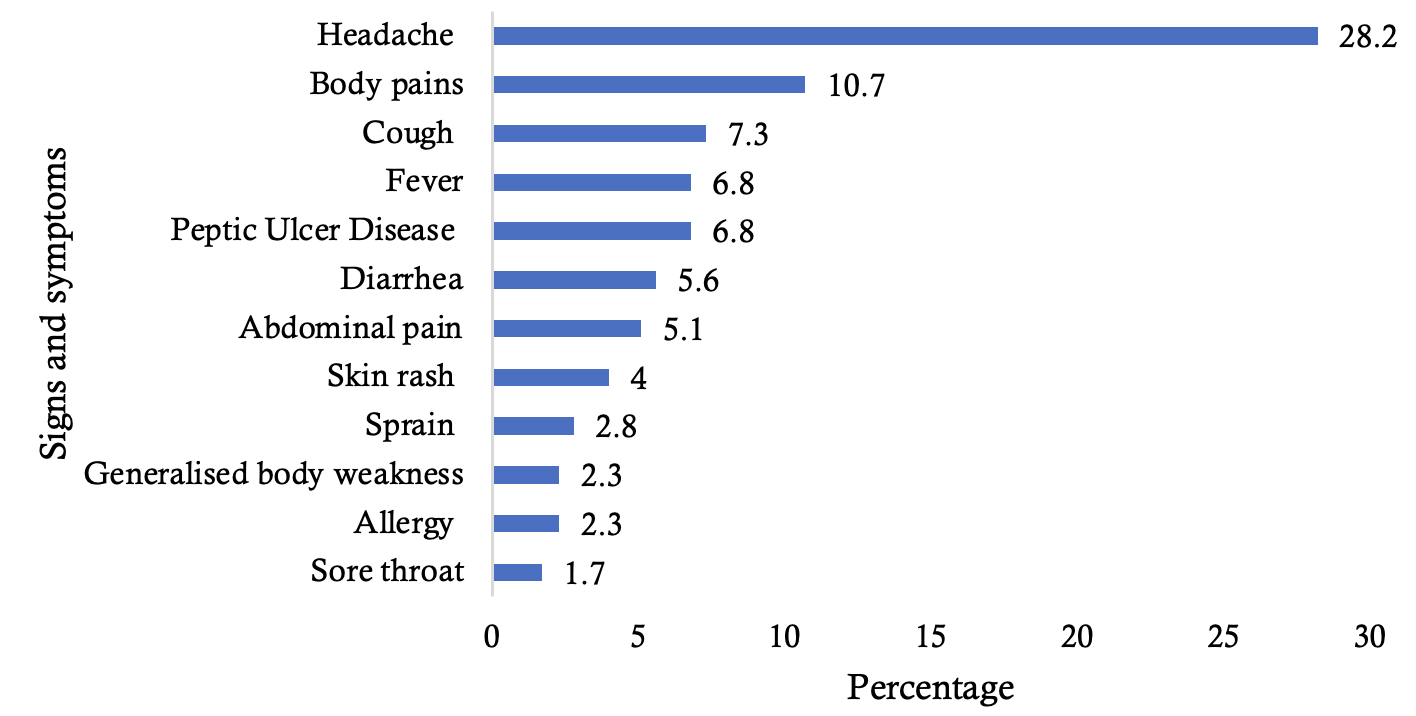
About 46.6% (n=177) of the respondents had experienced at least one sign and symptom of likely illnesses (Table 2). The proportion of respondents reporting signs and symptoms differed significantly by main purpose of attendance (χ², p=0.01). Security personnel had the highest proportion reporting symptoms (64.8%, 35/54), compared with respondents attending for tourism/adventure/partying (45.9%, 83/181) and those involved in commercial/service provision (40.7%, 59/145). When a Bonferroni correction was applied, we found that the statistical difference was between security personnel and commercial service providers (p=0.007), or between security personnel and those attending the party (p=0.04). Headaches were the most common symptoms experienced (28.2%), followed by acute respiratory tract infections (18.6%, Figure 2). About 7% of the respondents had fevers above 37.5°C, while another 7% had an unclear diagnosis of peptic ulcer disease (PUD).
This study described syndromic surveillance for disease threats during a large recreational mass gathering in Uganda. Approximately half of the respondents had experienced at least one sign and symptom of illness. However, no alerts were reported, nor was there identification of any suspected cases for infectious diseases.
Our study found that 46.6% of the respondents had experienced at least one sign and symptom that could have been suggestive of likely illnesses. Headaches and body pains were among the most commonly reported symptoms. In the context of a large outdoor mass gathering, these symptoms may reflect dehydration, fatigue, sleep deprivation, prolonged standing, heat exposure, alcohol consumption, or early manifestations of infectious and non-infectious conditions [21]. This finding is consistent with results from a study done in Uganda on syndromic surveillance during a religious mass gathering [11], suggesting that there could be substantial health burdens among persons attending these mass gatherings. While our data do not identify specific infections, the observed burden of symptoms may signal emerging health threats, suggesting that there could be potential for rapid spread of communicable diseases in such settings. Therefore, the current evidence highlights the need for targeted interventions such as effective risk communication, or onsite availability and accessibility of medical services for timely management of illnesses as they emerge, and early detection of potential outbreaks.
Notably, we found that there was a significant difference across groups of persons attending Nyege Nyege. It is plausible that the nature of participation in a large mass gathering may influence individuals’ exposure to health risks [22]. In our study, security personnel could have experienced more signs and symptoms given their prolonged exposures to environmental risks such as crowd-related pressures, heat, dehydration or limited rest across the 4 days of the festival. Similarly, individuals who were in attendance to party could have experienced signs and symptoms due to behavioural factors such as binge alcohol consumption, consumption of unsafe food or paying limited attention to hygiene, all of which may ultimately increase their susceptibility to illness symptoms [23]. Collectively, these findings underscore the need to implement health promotion messaging such as food hygiene and personal health behaviours, while taking into account risk assessments for varying behaviours of the persons in attendance.
Notably, the Nyege Nyege festival demonstrated that there was multisectoral collaboration, evidenced by different sectors at the event; health, security, welfare – all of which are critical for public health preparedness and response. Previous evidence has shown that in the event of an outbreak, the scope and complexity of the outbreak underscores that no single agency can work alone to effectively control and mitigate its impact [24]. As such, the WHO asserts that collaboration across sectors is key in identifying potential health risks, preventing and managing such risks, minimising their potential impact and responding to public health emergencies if they occur [25]. Altogether, this evidence suggests that integrated approaches for cross-sector collaboration are warranted to strengthen health system resilience to manage potential health threats during mass gatherings.
This study had some limitations and strengths. First, the surveillance activity was limited to only the duration of the festival; therefore, it is possible that some negative health events which manifested after respondents left the event could have been missed. Secondly, we relied largely on self-reported symptoms, which may have led to underreporting of some conditions of interest. Thirdly, we did not collect information about respondents’ chronic conditions or vaccination status for influenza and COVID-19, which limited our ability to assess whether underlying vulnerability or immune protection influenced the occurrence of reported symptoms.
Additionally, we did not perform any microbiological investigations; therefore, the reported signs and symptoms could not be attributed to specific infectious or non-infectious causes. As such, the findings should be interpreted as syndromic indicators useful for early warning and situational awareness rather than confirmed diagnoses. Fourth, the WHO framework for public health preparedness during mass gatherings encompasses several domains, including risk communication, environmental health, food and water safety, emergency medical services, contingency planning, partner coordination, and operational planning.
However, this Nyege Nyege surveillance activity presents findings primarily focused on disease surveillance and outbreak response. Caution is therefore required in interpreting the findings as full implementation of WHO mass gathering recommendations. Finally, our sample was predominantly male and aged 18-30 years, which limits generalizability of findings to females and other age groups. However, this over-representation also reflects the demographic profile of attendees at such a festival. Nonetheless, our findings remain relevant as they support the need for targeted surveillance during mass gatherings. Despite the aforementioned limitations, the findings contribute to the growing body of evidence that emphasises the need for emergency preparedness in high-risk environments for infectious disease transmission.
Syndromic surveillance conducted during the Nyege Nyege festival was key in monitoring and managing health risks that are often associated with mass gatherings. About half of the respondents reported experiencing at least one sign and symptom suggestive of illness. While there were no suspected cases nor registered for infectious diseases that warranted further medical attention, the study highlighted that with the presence of such a large, mobile population in close proximity, the event remains a potential hotspot for disease transmission. Notably, security personnel reported a higher burden of symptoms than other respondent groups, suggesting the need to prioritize their well-being through occupational health measures such as scheduled rest breaks. Additionally, given the behavioural and environmental risks commonly associated with such festivals, there is a need to strengthen targeted risk communication before and during the events, focusing on messaging on safer alcohol use, food and water hygiene, hand hygiene, sexual health, injury prevention, and early care-seeking for illness symptoms. Finally, from a systems perspective, mass gatherings often create interconnected public health challenges extending beyond syndromic surveillance alone, including risks related to HIV and other sexually transmitted infections, injuries, substance use, waste management, and pressure on local health services. There is thus a need for integrated, multisectoral preparedness and response strategies aimed at safeguarding the health of attendees.
Our findings have important implications for practice, policy and programming. First, as part of the continuous efforts to curb disease transmission during mass gathering surveillance, there is a need to prioritise action-after reviews to systematically assess the gaps in surveillance activities and strengthen mechanisms for coordination across sectors. Secondly, there is a need to mandate minimum public health requirements, such as sanitation and hygiene provisions or on-site basic medical support, for organisers of mass gatherings, enforceable through licensing processes. Thirdly, given the unique demographic of persons attending the Nyege Nyege festival, targeted health education and risk communication campaigns aimed at attendees are urgently warranted.
What is already known about the topic
What this study adds
AM wrote the first draft of the manuscript, contributed to methodology design and performed formal analysis. CK, FA, OA, SH, MA, RN, ES contributed to methodology design, analysis and editing the manuscript. CN, ANK, BL and SNK supervised, reviewed and edited the manuscript for substantial intellectual content. All authors read and approved the final version prior to submission.
| Variable | Frequency | Percentage |
|---|---|---|
| Sex | ||
| Female | 101 | 26.6 |
| Male | 279 | 73.4 |
| Age | ||
| 18-30 | 229 | 60.3 |
| 31-49 | 142 | 37.4 |
| 50+ | 9 | 2.2 |
| Main purpose of attendance | ||
| Tourism/adventure/partying | 181 | 47.6 |
| Commercial/service provision | 145 | 38.2 |
| Security | 54 | 14.2 |
| Variable | N=380 | Experienced signs and symptoms | χ² | |
|---|---|---|---|---|
| Yes = 177 n (%) | No = 203 n (%) | |||
| Sex | 380 | 177 (Total) | 203 (Total) | 0.48 |
| Female | 101 | 44 (43.6) | 57 (56.4) | |
| Male | 279 | 133 (47.7) | 146 (52.3) | |
| Age | 380 | 177 | 203 | 0.29 |
| 18-30 | 229 | 101 (44.1) | 128 (55.9) | |
| 31-49 | 142 | 70 (49.3) | 72 (50.7) | |
| 50+ | 9 | 6 (66.7) | 3 (33.3) | |
| Main purpose of attendance | 380 | 177 | 203 | 0.01* |
| Tourism/adventure/partying | 181 | 83 (45.9) | 98 (54.1) | |
| Commercial/service provision | 145 | 59 (40.7) | 86 (59.3) | |
| Security | 54 | 35 (64.8) | 19 (35.2) | |
| * Significant difference at p<0.05 | ||||