Research | Open Access | Volume 9 (3): Article 110 | Published: 08 Jul 2026

Views: 24
Menu, Tables and Figures
Table 1: Demographic characteristics of study participants in Oyo State, January 2022–April 2023. Data previously reported in [29].
| Variables | Frequency (N=289) | Percentage (%) |
|---|---|---|
| Sex | ||
| Male | 125 | 43.3 |
| Female | 164 | 56.7 |
| Age group in years | ||
| 0–14 | 41 | 14.2 |
| 15–29 | 58 | 20.0 |
| 30–44 | 106 | 36.7 |
| 45–59 | 54 | 18.7 |
| Above 60 | 30 | 10.4 |
| Educational level | ||
| No formal education | 96 | 33.2 |
| Primary | 105 | 36.3 |
| Secondary | 58 | 20.0 |
| Tertiary | 30 | 10.4 |
| Profession/Employment status | ||
| Civil servant | 45 | 15.6 |
| Farming | 59 | 20.4 |
| Cattle Breeders | 80 | 27.7 |
| Self-employed | 47 | 16.3 |
| Trading | 28 | 9.7 |
| Unemployed | 10 | 3.5 |
| Students | 20 | 6.9 |
Table 1: Demographic Characteristics of Study Participants in Oyo State, January 2022–April 2023. Data previously reported in [29]
Table 2: Correlation between LASV, rainfall, humidity and temperature
| Temperature | Rainfall | Humidity | LASV | |
|---|---|---|---|---|
| Temperature | 1 | |||
| Rainfall | -0.61 | 1 | ||
| Humidity | -0.83 | 0.76 | 1 | |
| LASV | 0.69 | -0.63 | -0.78 | 1 |
Interpretation: The correlation coefficient between Lassa fever occurrence and temperature (r = 0.69, p < 0.05) indicates a strong positive association, suggesting that LF cases increased with rising temperature. In contrast, rainfall (r = −0.63, p < 0.05) and humidity (r = −0.78, p < 0.05) show negative associations, indicating that LF occurrence decreased as rainfall and humidity increased. The association with humidity appears stronger than that with rainfall.
Olawale Sunday Animasaun1,2,3,4,&, Joseph Ojonugwa Shaibu5, Ibrahim Bola Gobir1,6, Piring’ar Mercy Niyang1,6, Busayo Kayode Akomolafe2,7, Olamide Priscilla Animasaun8, Iyabo Abibat Kareem9, Faith Naomi Ogundana10, Adigun Olanrewaju Adedayo9, Abiodun Adeleke Abatan11, Olusegun Olufikayo Ogundokun12, Rosemary Ajuma Audu2,5
1Georgetown Global Health Nigeria, Abuja, Nigeria, 2Faculty of Basic Medical and Applied Sciences, Molecular Biology and Genomics – Medical Virology Unit, Lead City University, Ibadan, Nigeria, 3Department of Medical Laboratory Services, Oyo State Primary Health Care Board, Ibadan, Nigeria, 4Nigeria Field Epidemiology and Laboratory Training Programme, 5Centre for Human Virology and Genomics, Nigerian Institute of Medical Research, Lagos, Nigeria 6Georgetown University Center for Global Health Practice and Impact, Washinton DC, United States of America, 7National Reference Laboratory, Nigeria Centre for Disease Control, Abuja, Nigeria, 8Department of Biochemistry, Federal University of Agriculture, Abeokuta, Nigeria, 9Oyo State Emergency Operations Center, Ministry of Health, Ibadan, Nigeria, 10Department of Medical Laboratory Services, ASR Police Reference Hospital Utako, Abuja, Nigeria, 11Department of Veterinary Services, Oyo State Ministry of Agriculture and Rural Development, Ibadan, Nigeria, 12LifeLabs Reference Laboratories, Burnaby, Canada
&Corresponding author: Olawale Sunday Animasaun, Georgetown Global Health Nigeria, Abuja, Nigeria, Email: oanimasaun@gghnigeria.org, olawalesundayanimasaun@gmail.com, ORCID: https://orcid.org/0000-0002-5203-6174
Received: 17 Nov 2025, Accepted: 02 Jul 2026, Published: 08 Jul 2026
Domain: Infectious Disease Epidemiology, One Health
Keywords: Lassa fever, diagnosis, rodent control, meteorological factors, One Health
©Olawale Sunday Animasaun et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Olawale Sunday Animasaun et al., One Health surveillance of Lassa fever in Oyo State, Nigeria. Journal of Interventional Epidemiology and Public Health. 2026; 9(3):110. https://doi.org/10.37432/jieph-d-25-00286
Introduction: Lassa fever (LF) is a severe viral haemorrhagic disease caused by Lassa virus (LASV) and remains endemic in Nigeria, where it is associated with recurrent outbreaks, substantial morbidity, and high mortality. The persistence of LF is driven by weak surveillance systems, limited diagnostic capacity, poor health-seeking behaviour, and complex interactions at the human–rodent–environment interface. In endemic settings, these factors contribute to under-detection of cases and sustained transmission. This study adopted a One Health-informed approach to assess the sero-molecular prevalence of LASV in humans, evaluate viral detection in rodents recovered following bait-based deratization activities and examine the influence of meteorological factors on LF occurrence in Oyo State, Nigeria.
Methods: Between January 2022 and April 2023, a cross-sectional study was conducted across selected high-risk LGAs in Oyo State. Blood samples (n = 289) were collected from febrile patients and screened for LASV using RT-qPCR and IgM/IgG ELISA. Rodents (n=30) were recovered in Iwajowa LGA, they were morphologically identified and tested for LASV using RT-qPCR. Meteorological data were obtained from the Nigerian Meteorological Agency to evaluate associations between climatic variables and LF occurrence. Data were analysed using descriptive statistics and bivariate correlation analysis.
Results: The overall LASV seroprevalence was 11.1% (32/289), comprising IgM positivity in 9.7%, IgG positivity in 4.8%, and dual IgM/IgG positivity in 3.5% of participants; three samples (1.0%) were confirmed positive by RT-qPCR. All recovered rodents tested negative for LASV RNA. Notably, no Mastomys species were recovered, while Rattus rattus, Mus musculus, and Cricetomys gambianus predominated. Correlation analysis showed a significant positive association between LF occurrence and temperature (r = 0.69, p < 0.05), and significant negative associations with rainfall (r = –0.63, p < 0.05) and humidity (r = –0.78, p < 0.05).
Conclusion: This study provides evidence of recent LASV exposure and limited molecular confirmation of active infection among suspected Lassa fever cases in Oyo State and underscores the importance of a One Health framework in understanding disease dynamics across human, animal, and environmental interfaces. The findings highlight the need to strengthen diagnostic capacity, improve surveillance and rodent control strategies, and integrate meteorological data into predictive early warning systems to enhance outbreak preparedness in endemic settings.
Lassa fever (LF) is an acute viral haemorrhagic disease caused by Lassa virus (LASV), a single-stranded RNA virus in the Arenaviridae family. The infection is zoonotic, with humans primarily acquiring it through contact with urine, feces, or saliva of infected multimammate rats (Mastomys natalensis), the natural reservoir of the virus [1,2]. Human-to-human transmission may also occur, especially in healthcare settings, via exposure to blood, body fluids, or contaminated materials [3]. First reported in 1969 in the town of Lassa, Borno State, northeastern Nigeria [4], LF remains a significant viral haemorrhagic fever across West Africa. It continues to pose major public health challenges in endemic countries including Nigeria, Sierra Leone, Liberia, and Guinea, characterized by recurrent outbreaks and substantial case fatality rates [5]. Recent surveillance and modeling studies by the West African Health Organization (WAHO) further highlight its persistent endemicity and public health burden in the region [5]. The ongoing efforts of the WAHO Lassa Fever Coalition, aimed at strengthening surveillance, enhancing diagnostic capacity, and accelerating vaccine access, further highlight the continuing regional importance of Lassa fever as a transboundary health threat [5, 6]. The World Health Organisation (WHO) estimates that approximately 300,000 to 500,000 infections occur annually across the region, with 5,000 to 10,000 deaths [3]. Nigeria, Sierra Leone, Liberia, and Guinea constitute the hyperendemic zone, although sporadic cases have been reported in Benin, Togo, and Côte d’Ivoire [7, 8]. LASV exhibits marked genetic diversity, forming multiple geographically associated phylogenetic lineages. Recent phylogenetic work and reviews classify LASV into seven lineages (I–VII) with distinct spatial distributions across West Africa: lineages I–III and VI circulate within Nigeria, lineage IV predominates in Sierra Leone, Guinea, and Liberia, lineage V in parts of Mali and Côte d’Ivoire, and lineage VII has been described in Togo/Benin [9,10]. Nigerian viruses themselves are heterogeneous: sublineages cluster regionally (e.g., lineage II in southern Nigeria and lineage III in north-central regions), and more recent sequencing studies continue to uncover novel sublineages and signs of reassortment and recombination in parts of West Africa. These genetic differences may affect diagnostics, antigenicity, virulence, and thus public-health impact, reinforcing the importance of local molecular surveillance.
Transmission dynamics are shaped by the ecology of reservoir rodents and by human behaviours and environmental change. Mastomys natalensis is synanthropic, abundant in peri-domestic environments and agricultural settings; factors that increase human–rodent contact, like poor housing, overcrowding, crop storage practices, and inadequate waste management, heighten spillover risk [4,11]. Seasonal patterns are often observed: in many endemic areas, LF incidence peaks during the dry season when rodent movement into homes increases as food availability declines. Climatic variability (rainfall, temperature, humidity) and land-use change (deforestation, urban expansion) modulate reservoir population dynamics and exposure risk, suggesting an environmental component to temporo-spatial risk that must inform surveillance and control.
In Nigeria, LF is a nationally notifiable disease and continues to cause recurrent seasonal outbreaks with substantial morbidity and mortality. According to the Nigeria Centre for Disease Control and Prevention [12], 8,542 suspected cases and 1,227 laboratory-confirmed cases were reported in 2023 across 28 states, with 211 deaths recorded, corresponding to a case fatality rate (CFR) of 17%. As of epidemiological week 35 of 2024, over 6,000 suspected cases and 170 deaths had already been documented, reaffirming the endemic nature of LF in Nigeria [12,13]. States within the southwestern, south-south, and north-central regions, including Ondo, Edo, Taraba, Bauchi, remain among the most affected. Ondo and Edo States alone accounted for over 60% of confirmed cases in 2023 [12].
Despite national progress in surveillance, the true burden of LF in Nigeria and West Africa is likely underestimated, primarily due to weak diagnostic capacity, low health-seeking behaviour and underreporting from rural health facilities, and clinical overlap with malaria and typhoid fever [14]. The nonspecific early symptoms of LF such as fever, malaise, and headache often lead to delayed diagnosis and inappropriate treatment. Furthermore, climatic and ecological conditions in parts of Nigeria, including fluctuating temperature, rainfall, and humidity, provide favourable habitats for Mastomys rodents, promoting sustained viral circulation and human exposure [15,16]. The epidemiology of Lassa fever is driven by a complex interplay between human behaviour, animal ecology, and environmental change. Deforestation, rapid urbanisation, poor sanitation, and unsafe food storage practices have expanded human–rodent contact interfaces in many communities [1,14]. The Mastomys natalensis rat thrives in human dwellings and farmlands, where it contaminates stored grains and household items with urine and faeces containing LASV [16]. This ecological linkage highlights the need for a One Health approach, integrating human, animal, and environmental health to design and implement effective surveillance and control strategies [17,18].
The One Health approach, supported by the WHO, the World Organisation for Animal Health (WOAH), the Food and Agriculture Organization (FAO), and the United Nations Environment Programme (UNEP), emphasize that the majority of emerging and re-emerging infectious diseases are of animal origin. Lassa fever serves as a prime example of such a zoonotic disease [18]. Integrated surveillance of both human cases and rodent reservoirs is critical for understanding local transmission dynamics and predicting outbreak risks.
Previous studies have successfully detected LASV in Mastomys rodents across several Nigerian states, including Edo, Ebonyi, Plateau, and Ondo [1,15,16]. However, data on Lassa virus ecology, sero-molecular prevalence, and rodent-related evidence of LASV occurrence in Oyo State remain limited. Oyo State is of particular epidemiological interest due to its rapid urban expansion, large and growing population, and persistent challenges in solid waste management, factors that may influence rodent ecology and opportunities for human–rodent interaction.
In recent years, Nigeria has implemented several targeted interventions aimed at strengthening Lassa fever prevention, control, and clinical management capacities. One notable initiative is the Lassa Fever Clinical Management Fellowship (LFCMF) championed by the Georgetown University Center for Global Health Practice and Impact (GU-CGPHI), which was designed to enhance the knowledge and skills of frontline healthcare workers in the diagnosis, case management, and infection prevention practices for Lassa fever. The fellowship program has demonstrated measurable improvement in clinical preparedness and capacity within endemic regions [19]. In addition, community-centered interventions employing human-centered design approaches such as the novel Local Innovations Scaled through Enterprise Networks (LISTEN) model have been successfully piloted in Ondo State, Nigeria to foster local ownership, promote hygiene and sanitation, and reduce rodent–human contact [20]. These participatory approaches underscore the importance of local innovation and stakeholder engagement in sustainable Lassa fever prevention [20]. However, behavioural studies continue to reveal substantial gaps between knowledge of Lassa fever transmission risks and actual preventive practices among residents in high-burden areas, emphasizing the need for continuous risk communication and community mobilization [21, 22].
Conducting comprehensive serological and molecular surveillance of LASV among febrile patients, alongside rodent-related evidence as well as assessing climatic factors can provide crucial insights into the epidemiology of the disease in this region. However, despite these insights, the environmental and ecological correlates of LF transmission in southwestern Nigeria remain poorly understood. There is a need to enhance understanding of the local epidemiology of Lassa fever, support risk-based public health interventions, and strengthen integrated surveillance systems at the human–animal–environment interface. Ultimately, this will contribute to Nigeria’s broader efforts under the National One Health Strategic Plan (2022–2026) to prevent, detect, and respond to zoonotic diseases through multisectoral collaboration.
This study, therefore, employed a One Health-informed approach to assess the sero-molecular prevalence of Lassa fever virus in humans, evaluate LASV occurrence in recovered rodents, and examine associated meteorological factors in Oyo State, Nigeria. Specifically, the aim of this study was to determine the seroprevalence and molecular detection rate of LASV among suspected LF patients, investigate LASV detection in rodents recovered from households and surrounding environments during targeted deratization activities in selected communities, and assess the influence of key meteorological factors, including temperature, rainfall, and humidity, on LASV transmission dynamics in Oyo State, Nigeria.
Study setting
Oyo State is situated in the South-West geopolitical zone of Nigeria, with Ibadan serving as its capital. The State comprises 33 constitutionally recognised Local Government Areas (LGAs), and in 2016, the government approved the establishment of 35 Local Council Development Areas (LCDAs) to enhance administrative and developmental efficiency. According to projections based on the 2011 National Population Commission (NPC) data, the State had an estimated population of approximately 8,050,527 in 2019, assuming an average annual growth rate of 2.83%. Oyo State experiences two main seasons: the dry season (November to March) and the wet season (April to October). The dry season is marked by low humidity, high temperatures, and minimal rainfall, whereas the wet season is characterized by increased humidity, lower temperatures, and heavy rainfall, sometimes resulting in flooding. Average daily temperatures range between 25 °C and 35 °C throughout the year. The State’s vegetation shows a gradual ecological transition from tropical rainforest in the south to Guinea savannah in the north, with dense forest cover in southern areas giving way to open grasslands interspersed with trees in northern zones [23]. This study was conducted across ten high-risk Local Government Areas (LGAs) in Oyo State, Nigeria, identified based on previous reports of viral haemorrhagic infections from researchers, the Oyo State Ministry of Health, and the Nigeria Centre for Disease Control and Prevention (NCDC). The selected LGAs included Ido, Oyo East, Oorelope, Ona-Ara, Akinyele, Oluyole, Iwajowa, Ogbomosho South, Ibarapa Central, and Ibadan Southeast.
Study design, duration and population
This study employed a cross-sectional design involving human surveillance, meteorological data evaluation, and rodent post-deratization recovery assessment to investigate LASV dynamics. The study was conducted over the period from January 2022 to April 2023. The study population consisted of a mixed cohort. Participants included febrile in- and out-patients attending selected healthcare facilities. Additional participants were recruited through active community case searches, which involved house-to-house case findings in selected Local Government Areas (LGAs). Some participants were also enrolled following reports to the State Public Health Emergency Operation Centre, in accordance with the Integrated Disease Surveillance and Response (IDSR) strategy implemented within the state.
Inclusion and exclusion criteria
Participants included in the study were patients within the study locations during the study period who met the predefined suspected Lassa fever case definition (fever ≥38°C with compatible clinical symptoms and/or epidemiological risk factors) and provided written informed consent. Febrile patients with laboratory-confirmed alternative diagnoses explaining their symptoms (e.g., malaria or other infections) were excluded.
Sample size
The number of patients needed for the study (sample size) was determined using Fisher’s formula. The sample size was calculated based on a seroprevalence estimate of 18% from previous studies [24]. A non-response rate of 10% was considered.
$$N = \frac{Z^2(PQ)}{D^2}$$
Where:
N = Required sample size
D = Level of statistical significance = 0.05
Z = Standard normal deviation = 1.96
P = Prevalence from previous studies = 18% = 0.18
Q = 1 − P = 0.82
Thus:
$$N = \frac{(1.96)^2 \times 0.18 \times 0.82}{(0.05)^2}$$
N=227
Adjusting for a 10% non-response rate:
$$\begin{align}
N_f &= \frac{227}{1 – 0.1} \\
N_f &= 253
\end{align}$$
Therefore, a minimum sample size of 253 participants was required for the study. However, a total of 289 participants were enrolled to improve study power.
Case definitions
Alert case: Any person who has an unexplained fever (i.e., malaria and other common causes of fever have been ruled out), with or without bleeding. OR Any person who died after an unexplained severe illness with fever and bleeding.
Suspected case: Any individual presenting with fever for 3-21 days with a measured temperature of 38 °C or more with one or more of the following: malaise, fever, headache, sore throat, cough, nausea, vomiting, diarrhoea, myalgia, chest pain, hearing loss and either: a. History of contact with excreta or urine or rodents. b. History of contact with a probable or confirmed Lassa fever case within a period of 21 days of onset of symptoms, OR Any person with inexplicable bleeding/ haemorrhage. OR In Neonates: Maternal Lassa fever +/- signs and symptoms.
Confirmed case: A suspected case with a laboratory confirmation (positive IgM antibody, PCR or virus isolation)
Probable case: A suspected case who died or absconded without the collection of a specimen for laboratory testing. For the purpose of this study, LASV-specific IgM positivity was interpreted as evidence of recent infection or exposure, whereas RT-PCR positivity was considered evidence of active infection with detectable viral RNA. Serological and molecular findings were therefore analysed and reported separately where appropriate. All definitions are adapted from the NCDC (2018) Technical Guidelines for IDSR in Nigeria.
Sampling technique
A purposive sampling method was employed to recruit participants who met the established case definitions for Lassa fever.
Data collection
A quantitative data collection approach was utilised. Information was gathered from consenting participants using semi-structured, interviewer-administered questionnaires, designed to capture demographic, clinical, and epidemiological variables relevant to the study objectives.
Sample collection, transportation, and storage
Approximately 5 mL of whole blood was aseptically collected from each participant via venipuncture into ethylene diamine tetraacetic acid (EDTA) anticoagulant tubes. Samples were transported under cold chain conditions (2–4 °C) using a triple packaging system to the designated laboratory. Upon arrival, samples were centrifuged at 3,000 × g for 5 minutes to separate plasma. The resulting plasma was aliquoted into two portions for serological and molecular analyses, and subsequently stored at −20 °C until testing.
Deratization exercise and rodent assessments
A targeted rodent assessment and deratization exercise was conducted in Agbaruru Community, Iwajowa Local Government Area (LGA), Oyo State, following the confirmation of a human Lassa fever case in the community. Upon confirmation of the case, outbreak response activities were immediately initiated by the State and LGA One Health Rapid Response Team (OH-RRT) under the coordination of the State Public Health Emergency Operations Centre (PHEOC) and partners. These activities included contact tracing, active case search, case investigation, community engagement, and risk communication aimed at interrupting transmission and identifying additional cases. As part of the environmental investigation, a deratization and rodent recovery exercise was subsequently conducted within one month of outbreak confirmation. This component was implemented as an exploratory One Health-informed investigation to assess the potential presence of LASV among rodents recovered from affected households and their surrounding environments and to generate preliminary evidence on possible rodent involvement in the outbreak.
The exercise focused on residences and nearby areas where confirmed human LASV cases had been identified, with particular attention to locations showing visible evidence of rodent infestation such as droppings, burrows, gnaw marks, food contamination, and frequently used rodent pathways. Special emphasis was placed on areas likely to harbor Mastomys species, the recognized natural reservoir of LASV.
As part of the deratization intervention, rodenticide baits were prepared using phostoxin (aluminium phosphide) mixed with crushed roasted fish to enhance palatability and improve attraction to rodents. The prepared bait mixtures were divided into small portions, enclosed in nylon sachets, and strategically placed along identified rodent routes and high-activity locations within both residential dwellings and surrounding external environments. These included kitchens, food preparation areas, grain storage facilities, refuse disposal sites, wall corners, crevices, and other locations with visible signs of rodent activity. The baited sites were left overnight to maximize rodent exposure. Subsequently, dead rodents recovered from baited households and surrounding environments were carefully collected using appropriate biosafety precautions and transported for laboratory investigation.
Recovered rodents were subjected to preliminary species identification based on external morphological characteristics, including body size, fur coloration, tail length relative to body size, ear shape, snout appearance, foot structure, and the number and arrangement of mammary glands, in line with standard morphological features associated with Mastomys species.
Following identification, tissue specimens including liver and spleen, together with blood samples, were aseptically collected from the recovered rodents using sterile dissecting instruments and transferred into sterile universal containers. Samples were immediately preserved at 4°C and maintained under cold-chain conditions during transportation to the laboratory to preserve sample integrity.
In the laboratory, tissue specimens were processed under aseptic conditions. The liver and spleen tissues were mechanically crushed and homogenized to facilitate cellular disruption and release of viral RNA for downstream molecular analysis. The homogenized tissue suspension, together with blood, was subsequently processed for RNA extraction using standard extraction protocols in accordance with manufacturer recommendations. Extracted RNA was then subjected to real-time reverse transcription polymerase chain reaction (RT-PCR) for detection of Lassa fever virus, following established diagnostic protocols, including appropriate amplification controls and recommended cycling conditions.
This rodent component represented a targeted post-case environmental assessment conducted after confirmation of human LASV cases and was intended to provide exploratory evidence of possible rodent involvement within affected households and surrounding environments, rather than a structured ecological rodent trapping survey.
Laboratory analysis
All laboratory procedures were conducted at the ISO 15189-accredited laboratory of the Centre for Human Virology and Genomics, Nigerian Institute of Medical Research (NIMR), Yaba, Lagos, Nigeria.
RNA extraction
RNA was extracted from human plasma and harvested organs (mechanically homogenised) using the Jena Bioscience Viral DNA+RNA Purification Kit (Jena, Germany), following the manufacturer’s instructions. Extracted RNA samples were stored at −20 °C until further analysis.
Real-time PCR (qPCR) analysis
One-step reverse transcriptase real-time PCR (RT-qPCR) was performed to detect Lassa virus using a QuantStudio 5 instrument. The amplification protocol included denaturation, primer annealing, and elongation steps, optimized to ensure efficient amplification of target genes. Each run included positive and negative controls: ATCC panels and total RNA extracts from a previous study were used as positive controls. The primers and probes used for LASV detection are Lassa Virus S36 (5′- ACC GGG GAT CCT AGG CAT TT -3′) and LVS_339-d (5′- GTT CTT TGT GCA GGA MAG GGG CAT KGT CAT -3′) [13].
PCR cycling conditions
The amplification protocol consisted of an initial denaturation at 94 °C for 5 minutes, followed by 36 cycles of:
This was followed by a final elongation step at 72 °C for 7 minutes, and a hold at 10 °C until further processing.
PCR reaction mix
Each 25 µL PCR reaction contained:
A Ct cutoff value of <38 was used to define LASV positivity, based on prior assay validation, control performance, and optimization to ensure reliable detection while maintaining assay sensitivity and specificity.
Serological analysis
Serological detection of Lassa virus (LASV) antibodies was performed using the ReLASV® Pan-Lassa NP IgG/IgM ELISA Kit (Zalgen Labs, USA), which targets human anti-LASV nucleoprotein (NP) antibodies. The assay has a reported specificity of 92.6% (95% CI: 87.5–96.5%) and sensitivity of 96.4% (95% CI: 93.5–98.5%).
Procedure: Serum samples were diluted and added, along with calibrators and controls, to antigen-coated microwells. After incubation and washing, bound antibodies were detected using horseradish peroxidase (HRP)-conjugated anti-human IgG or IgM and visualized with a chromogenic substrate. Optical density (OD) was measured at 450 nm with a 620–650 nm reference wavelength. All samples were tested in duplicate, and mean OD values were calculated. Antibody concentrations were determined using a four-parameter logistic calibration curve.
Quality control: Assay validity was ensured by including positive and negative controls in each run. Reagent blanks had OD < 0.150, duplicate values showed ≤25% coefficient of variation, and control recovery met manufacturer specifications.
Interpretation: Results were classified as positive, negative, or equivocal according to the manufacturer’s guidelines. The assay detects antibodies against the LASV nucleoprotein specific to the three most prevalent lineages: Lineages II and III in Nigeria, and Lineage IV in Sierra Leone, Guinea, Liberia, and Mali.
Meteorological parameters
Monthly data on minimum and maximum temperature, rainfall, and relative humidity during the study period were obtained from the Nigeria Meteorological Agency (NIMET), through the State office located at Aerodrome Estate, Samonda, Ibadan, and the Corporate Head Office in Abuja.
Data analysis
Data was entered and cleaned using Microsoft Excel 2019 and analyzed with IBM SPSS Statistics version 25 (IBM Corp., Armonk, NY, USA). Descriptive statistics summarized sociodemographic characteristics, clinical symptoms, and laboratory results. Categorical variables were reported as frequencies and percentages, while continuous variables were expressed as means ± standard deviations (SD). Bivariate correlation analysis was performed using Pearson’s correlation coefficient (r) to evaluate associations between Lassa virus (LASV) occurrence and meteorological parameters (temperature, rainfall, humidity).
Ethical considerations
The study received ethical approval from the Institutional Review Board (IRB) of the Nigerian Institute of Medical Research (NIMR; IRB-19-006). Additional approvals and permissions were obtained from the Oyo State Ministry of Health, Department of Public Health (SMOH/EPID/016/005), as well as the officers-in-charge of participating healthcare facilities. Written informed consent was obtained from all participants. For adults, both oral and written consent (signed or thumb-printed) were collected. For minors, parental or guardian consent was obtained in addition to assent from the minors. Participants with limited literacy were provided explanations in the local language, detailing the study’s purpose, procedures, risks, and benefits. Participation was voluntary, with assurance that individuals could withdraw at any time without penalty. Confidentiality and privacy were maintained using unique identifiers and secure data storage. Participants were informed of potential temporary discomfort during sample collection and were ensured of privacy throughout interviews and laboratory procedure.
The rodent component involved post-deratization specimen recovery rather than experimental animal manipulation. All rodent handling, specimen collection, transportation, and disposal were conducted in accordance with standard biosafety and ethical procedures for safe handling of potentially infectious material.
Sociodemographic characteristics of study participants
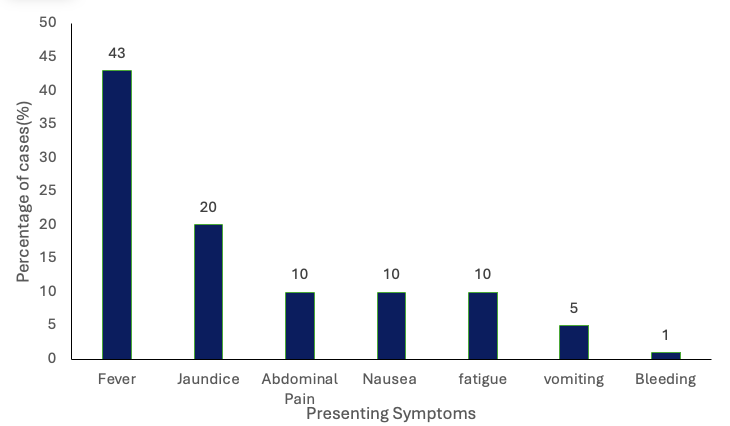
A total of 289 febrile patients clinically suspected of LF were enrolled in this study. Table 1 shows that the age group 30–44 years constituted the majority, accounting for 106 (36.7%) of participants. There were more female participants [164 (56.7%)] than males. A total of 80 (27.7%) of the participants were Fulani cattle breeders, while 105 (36.3%) had attained at least a primary-level education. Clinical symptoms observed among suspected LF cases indicated that fever was the most common presentation, occurring in 43% of participants, followed by jaundice (20%), while 1% presented with bleeding manifestations (Figure 1).
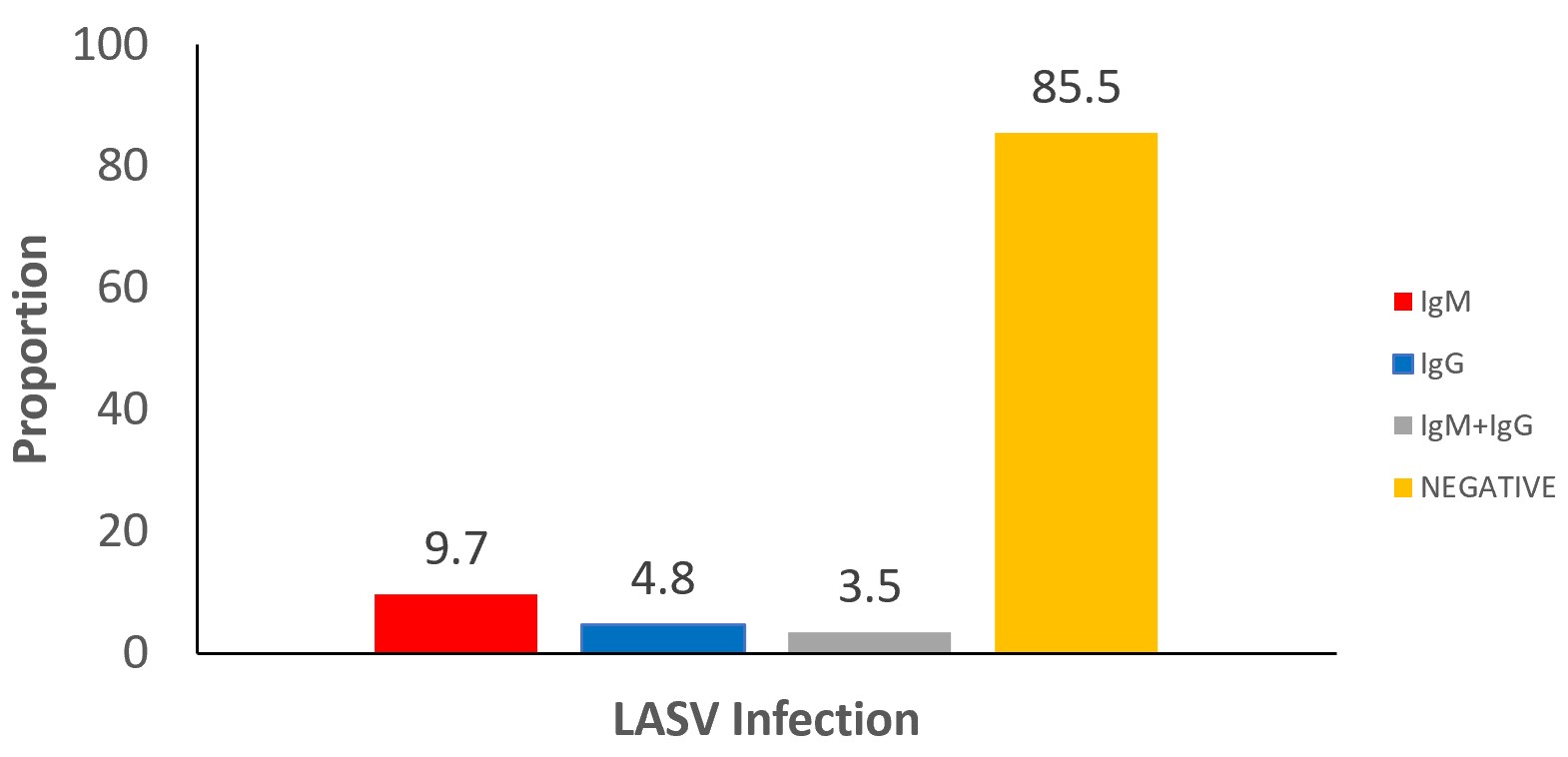
Serological results
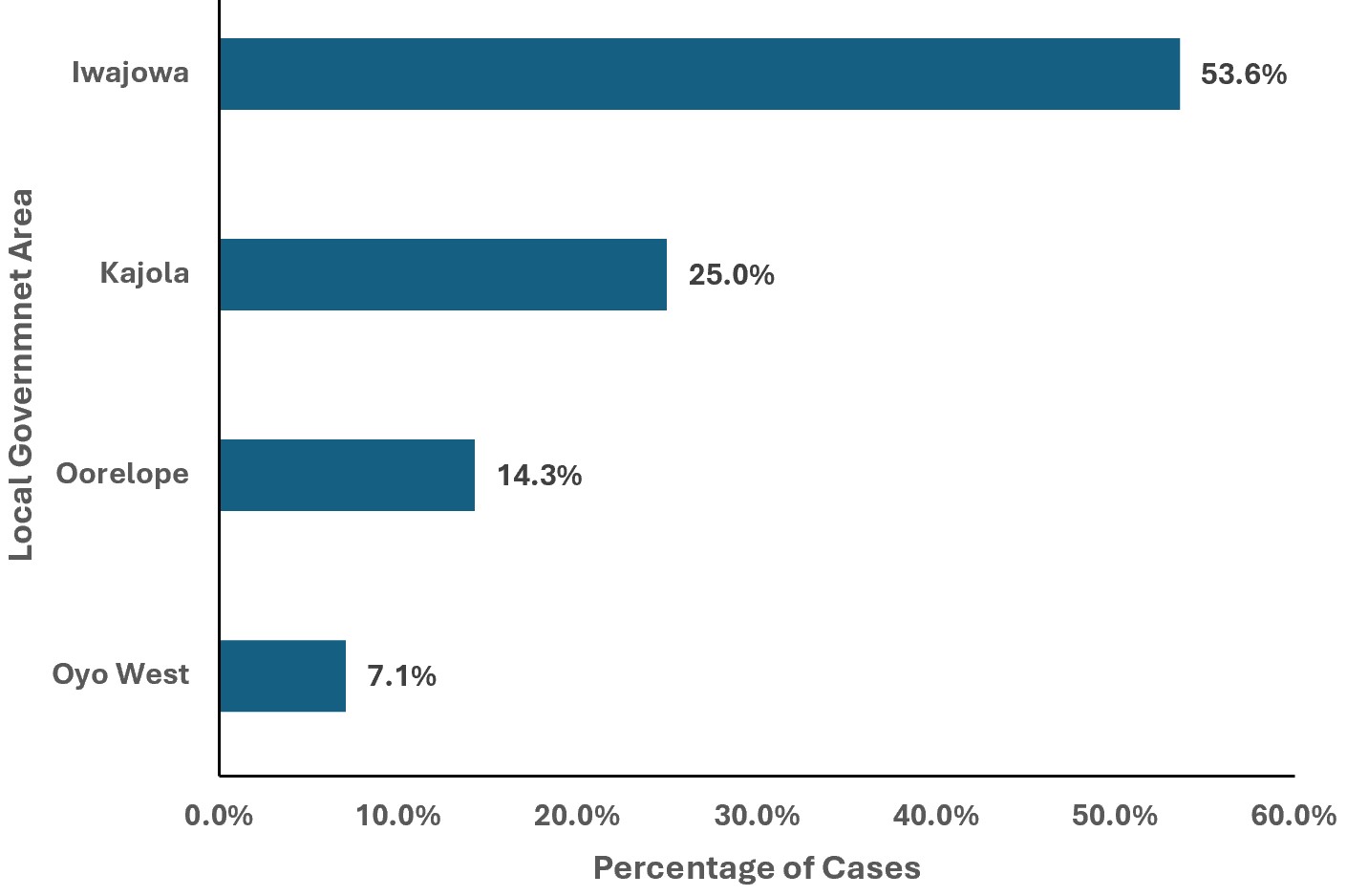
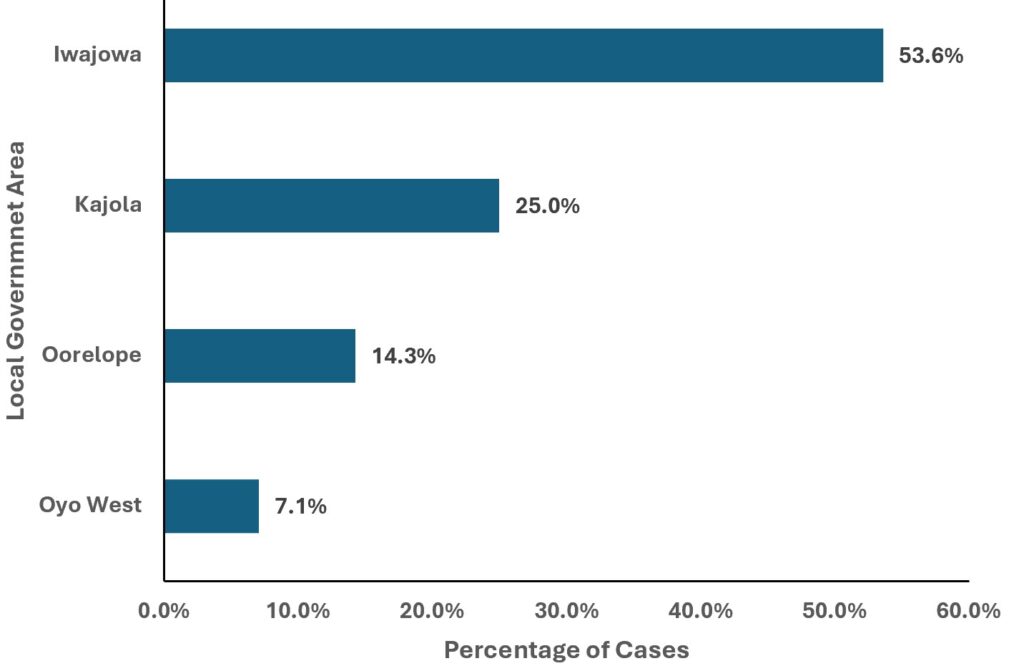
Overall, LASV seroprevalence was 11.1% (32/289), based on participants positive for LASV IgM and/or IgG antibodies. Among the participants, 28/289 (9.7%) were positive for LASV IgM antibodies, while 14/289 (4.8%) were positive for LASV IgG antibodies. Concurrent IgM and IgG positivity was observed in 10/289 (3.5%) participants, suggesting recent exposure or infection with evidence of prior immune response. (Figure 2). This positivity is for LASV nucleoprotein-specific antigen against the three most prevalent lineages of LASV (lineage II, III in Nigeria and lineage IV in Sierra Leone, Guinea, Liberia, and Mali). The LASV positive IgM samples were seen from patients from Iwajowa LGA 15/28 (53.6%), Kajola LGA 7/28 (25.0%), Oorelope LGA 4(14.3%), Oyo West LGA 2/28 (7.1%) (Figure 3).
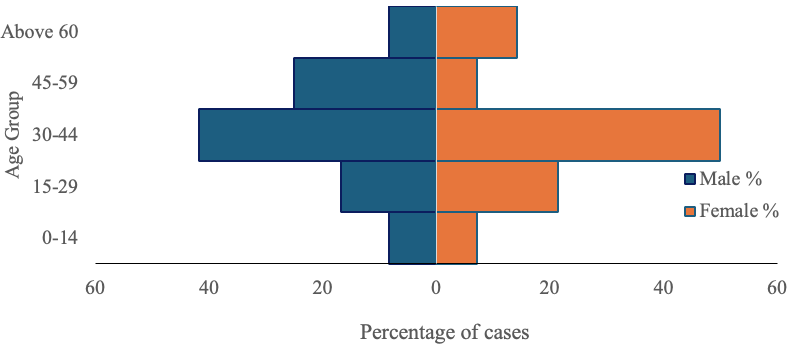
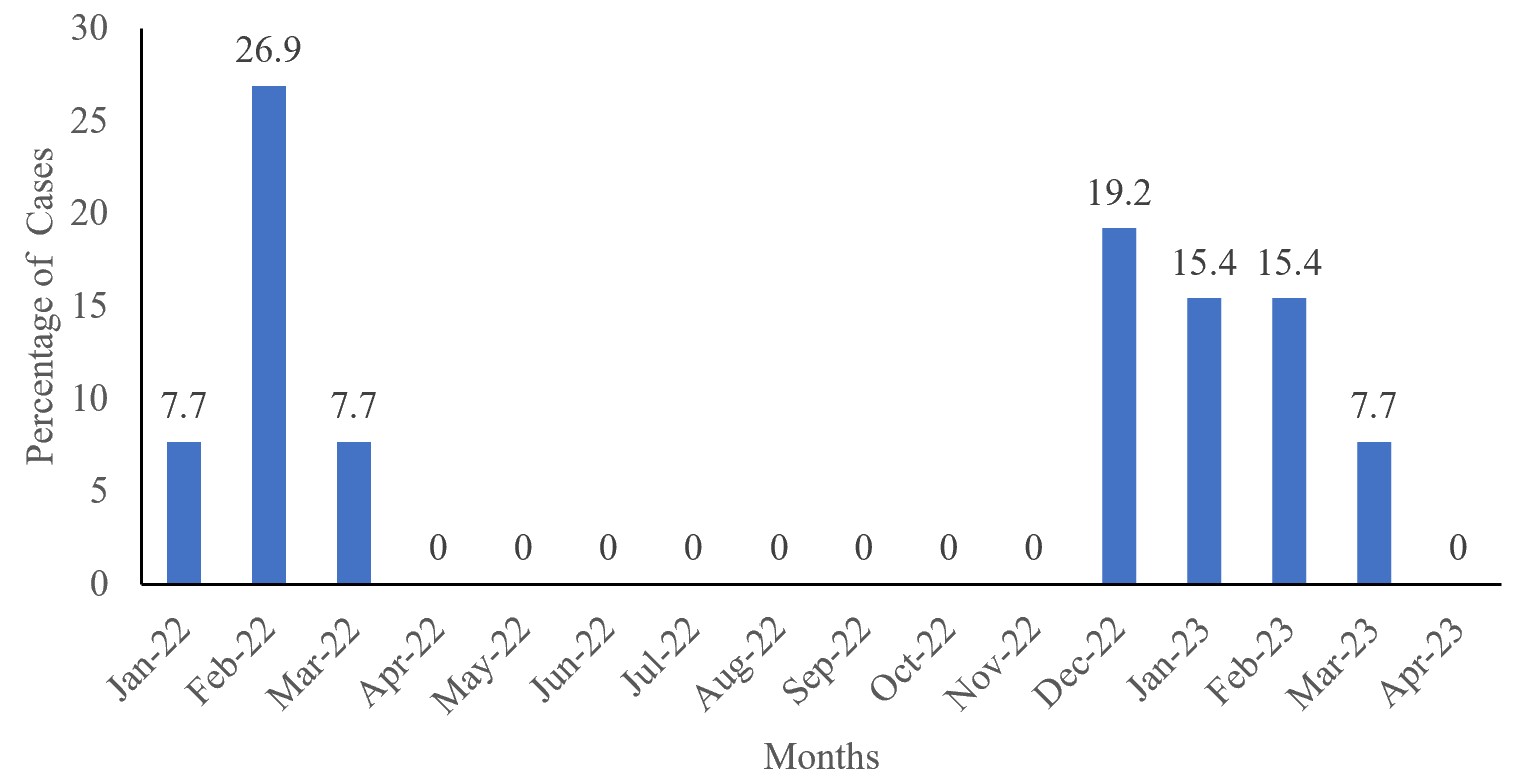
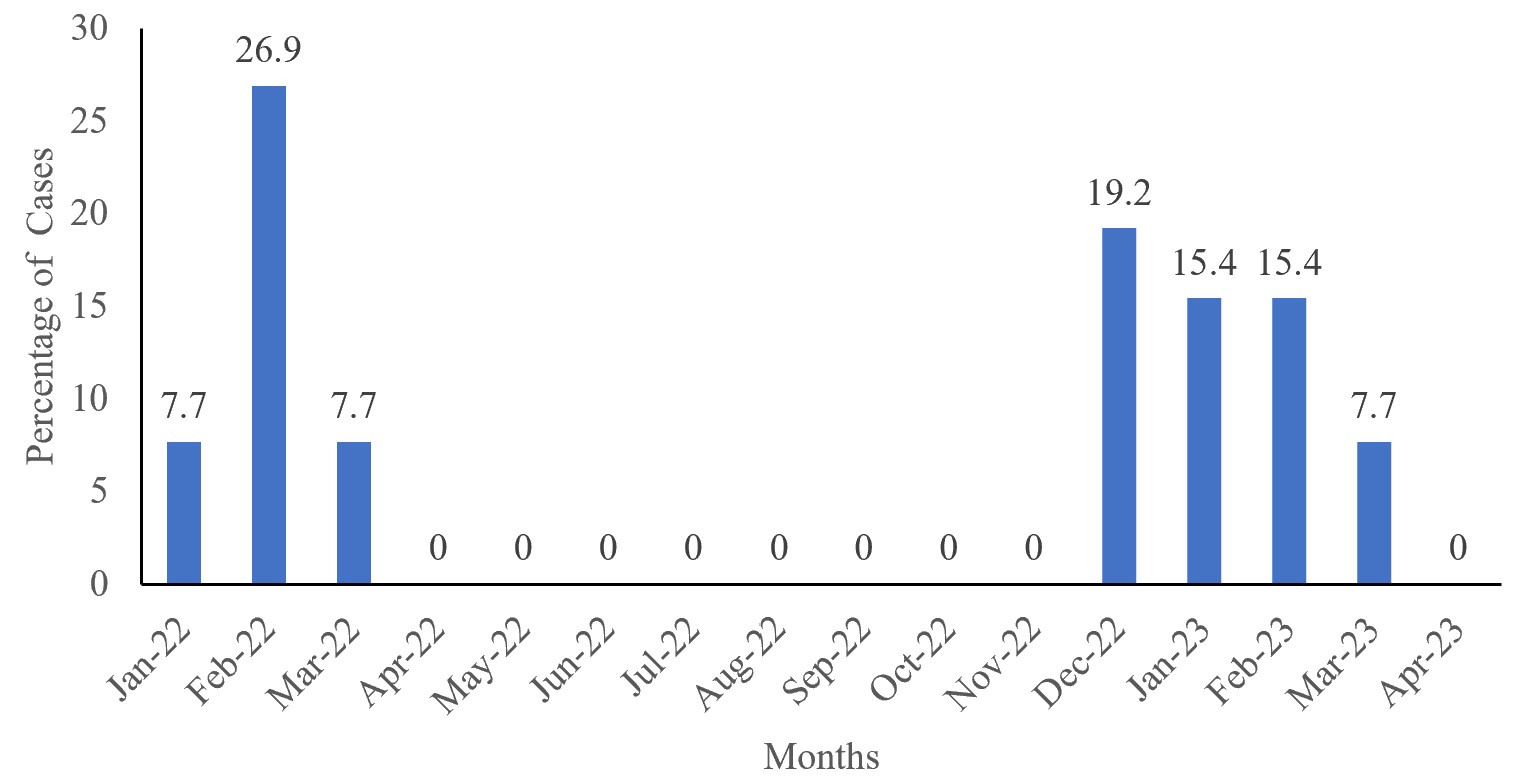
Females are the most affected, 15/28(53.6%), and the age group 30-44 years were the most affected, as seen in Figure 4. LASV cases peak during the dry season, January-March of each year, 2022 and 2023 (Figure 5).
Rodent species identification and characterization
A total of 30 dead rodents were recovered from baited locations in Agbaruru Community, Iwajowa LGA, Oyo State, during the deratization exercise. Morphological identification based on external features such as body size, fur colour, tail length, ear shape, foot structure, snout appearance, and mammary pattern showed that none of the recovered rodents belonged to the Mastomys genus. The identified rodents consisted mainly of Rattus rattus (black rat)(n=16), Mus musculus (house mouse) (n= 8), and Cricetomys gambianus (Gambian giant pouched rat) (n=6).
Molecular detection of LASV in human samples
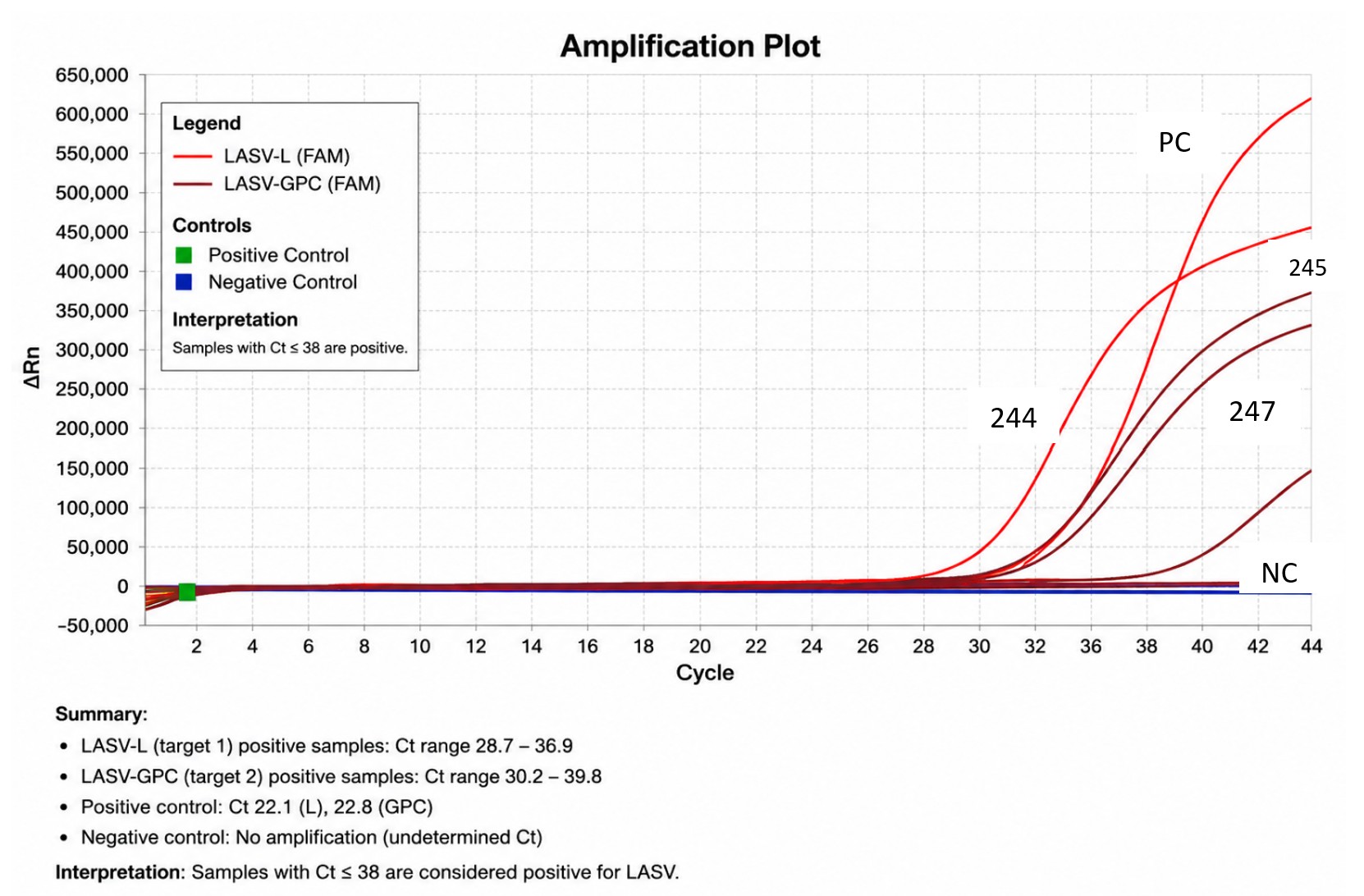
RT-qPCR analysis of RNA extracted from 289 human samples detected LASV RNA in 3 (1.0%) participants, while the remaining samples tested negative (Figure 6). The three RT-qPCR-positive samples were identified from Iwajowa (n = 2) and Kajola (n = 1) LGAs of Oyo State. Two (66.7%) of the positive cases were male, while one (33.3%) was female. All positive individuals were within the 30–44-year age group. The cycle threshold (Ct) values ranged from 32 to 35, indicating low levels of detectable viral RNA. Notably, all RT-qPCR-positive participants were also positive for LASV IgM antibodies, providing molecular evidence of recent or active infection.
Molecular detection of LASV in rodent samples
RT-qPCR screening of blood and tissue specimens obtained from 30 rodents did not detect LASV RNA in any of the samples analyzed. Although no evidence of active LASV infection was identified among the rodents captured during the study period, these findings should be interpreted cautiously, as the absence of detection does not exclude focal or temporal circulation of the virus within local rodent populations.
Meteorological parameters
The correlation between LASV incidence and selected environmental factors, as shown in Table 2, indicates that variations in rainfall, humidity, and temperature are significantly associated with Lassa virus activity.
Oyo State reported laboratory-confirmed cases of LF, with a CFR of 50% between 2012 and 2016 [25]. However, no confirmed cases were documented between 2017 and 2021, until the re-emergence identified in this study, beginning in late 2021 and continuing into 2022. This long interval without confirmed cases raises an important epidemiological question as to whether LF transmission was truly interrupted or whether limitations in surveillance intensity, diagnostic capacity, and case detection contributed to under-recognition of ongoing transmission. Although surveillance records from the State Ministry of Health Epidemiology Unit indicate continued testing of suspected LF cases during this period, which were largely reported as negative, the prolonged absence of confirmed cases may suggest limitations in diagnostic sensitivity, case ascertainment, or overall surveillance yield. The subsequent identification of confirmed cases in this study, together with increased reports of undifferentiated febrile illness in hotspot LGAs toward late 2021, suggests that low-level or focal transmission may have persisted but remained undetected. A more plausible explanation is that surveillance intensity and active case finding were suboptimal during part of this period, until strengthened sensitization and active surveillance efforts were implemented by the Oyo State Public Health Emergency Operations Centre, complemented by this study in 2021/2022. These findings reinforce the critical importance of sustained high-quality surveillance systems, early case detection, and rapid response mechanisms for viral haemorrhagic fevers in endemic and at-risk settings [5,8].
In this study, the overall LASV seroprevalence among suspected LF patients was 11.1% (32/289), indicating ongoing exposure within the study population and suggesting a substantial burden of LASV-compatible febrile illness that may reflect underdiagnosis and incompletely detected community transmission. This aligns with a study in Edo State, where LASV seroprevalence ranged from 1.7% to 23.7% among occupational groups of health workers, and is comparable though lower than the 18.0% and 21.3% reported in other studies [24, 26, 27]. This level of seropositivity implies that LASV transmission may not be solely episodic but could be occurring at a low-to-moderate and sustained level within affected communities. The detection of IgM antibodies in 9.7% of participants is particularly important, as it indicates recent or acute infection and supports evidence of ongoing transmission during the study period, while IgG positivity in 4.8% reflects prior exposure and suggests sustained community-level circulation over time. The detection of both IgM and IgG antibodies in 3.5% suggests recent or ongoing Lassa virus exposure with concurrent development of longer-term immune response. This pattern may indicate transitional seroconversion following recent infection, reflecting active transmission within the study population and underscoring the need for sustained surveillance and targeted public health interventions.
Molecular confirmation and infection staging
The detection of LASV RNA in three participants provides molecular confirmation of active LASV infection and complements the serological findings. Although only a small proportion of participants were RT-qPCR positive, the presence of detectable viral RNA indicates ongoing transmission within the study area and highlights the value of combining molecular and serological approaches for comprehensive LASV surveillance. This low RNA detection may reflect late clinical presentation, suboptimal timing of sample collection relative to the transient viraemic phase, or the narrow window of detectable viraemia in Lassa fever infection. The presence of RT-qPCR positivity among some IgM-positive (3/28) participants indicates overlap between active viral replication and the early antibody response. This finding suggests that several individuals were likely transitioning from the acute viraemic stage to the convalescent phase of infection at the time of sampling, which may account for reduced viral RNA detectability despite evidence of recent exposure as demonstrated by IgM seropositivity.
The coexistence of IgM, IgG, and RT-qPCR positivity demonstrates different stages of infection within the population, reflecting heterogeneous exposure dynamics. Importantly, these findings highlight the value of integrating serological and molecular diagnostics in LF surveillance systems, particularly in resource-limited settings where reliance on molecular testing alone may underestimate true infection burden due to the timing of sample collection and variable viral loads.
Demographic and spatial distribution of cases
The age distribution and demographic patterns observed, with higher positivity among adults aged 30–44 and 45–59 years and a higher proportion among females, may reflect increased exposure through occupational, domestic, or peri-domestic activities. This is consistent with known epidemiology of LF in endemic regions where exposure risk is closely linked to environmental interaction, household roles, food handling, and agricultural activities. The spatial clustering of cases in LGAs such as Iwajowa, Kajola, Oorelope, and Oyo West further suggests localized transmission hotspots potentially driven by environmental and socio-behavioural factors.
Notably, confirmed cases were predominantly in rural areas, particularly among Fulani cattle-breeding communities, possibly due to closer contact with infected rodents and poor hygiene practices facilitating infection through contaminated food or bodily fluids. Further studies are needed to clarify the high prevalence among these occupational and ethnic groups as well as location predisposing factors [28].
Diagnostic and surveillance challenges in Nigeria
Nigeria continues to face major challenges in LF surveillance due to the non-specific early clinical presentation of the disease, which overlaps with common febrile illnesses such as malaria and typhoid fever. This often leads to delays in case suspicion, testing, and treatment initiation. Additionally, limited access to diagnostics at peripheral levels contributes to under-detection and delayed outbreak recognition. These systemic challenges may facilitate ongoing transmission before cases are identified and isolated, reinforcing the need for improved point-of-care diagnostics and strengthened surveillance systems.
Seasonal and meteorological patterns
Lassa fever demonstrates a consistent and well-recognized seasonal pattern, with increased transmission during the dry months, although some studies suggest that infections may occur throughout the year. This pattern has been widely documented in endemic settings, including Nigeria and Guinea [28, 29]. The present study aligns with this epidemiological pattern, with cases clustering within the same dry-season period across 2022 and 2023. This seasonality is largely driven by ecological and environmental factors influencing transmission dynamics rather than intrinsic changes in the virus. Lassa virus, as an enveloped RNA virus, does not exhibit prolonged environmental persistence under natural conditions. Instead, transmission is primarily sustained through continuous contamination of the environment via the excreta of infected Mastomys natalensis rodents. These ecological processes are further shaped by meteorological conditions. Warmer and drier environments may indirectly enhance transmission by altering the behaviour and ecology of the rodent reservoir, particularly Mastomys natalensis, leading to increased movement into human dwellings in search of food and water. This increases the likelihood of human–rodent contact and exposure to contaminated materials. Additionally, dry conditions may facilitate the dispersal of contaminated dust and fomites derived from rodent excreta, thereby increasing opportunities for indirect exposure. Although rainfall and humidity were inversely associated with case occurrence, these relationships should be interpreted as ecological correlations rather than direct causal determinants. Overall, the findings reinforce seasonality as a key ecological driver of LF epidemiology, reflecting the complex interplay between environmental conditions, rodent reservoir dynamics, and human behavioural exposure patterns in endemic West African settings.
Rodent findings and ecological interpretation
Following community-based deratization activities in Agbaruru (Iwajowa LGA), 30 rodents were recovered and screened, and all tested negative for LASV RNA using RT-PCR. Morphological identification revealed that none of the recovered rodents was Mastomys natalensis, the primary reservoir host of LASV in West Africa [1,17], while peri-domestic species such as Rattus rattus, Mus musculus, and Cricetomys gambianus predominated. However, these findings should be interpreted with caution due to methodological limitations. Rodent recovery was conducted following bait-based deratization activities in response to human LF confirmed cases, rather than through systematic ecological trapping over time. As such, the sample may not be representative of the broader rodent population or reservoir dynamics in the community. Additionally, the relatively small sample size limits the ability to draw definitive conclusions regarding the absence of LASV circulation in local rodent populations. Moreover, the absence of LASV detection in recovered rodents, despite confirmed human infections, is epidemiologically important and may reflect spatial and temporal mismatches between human infection and rodent sampling, focal or transient enzootic circulation, or limitations in the sampling strategy and period. These findings highlight that human Lassa fever cases can occur even when concurrent rodent infection is not detected in localized investigations, underscoring the complexity and heterogeneity of LASV transmission dynamics in endemic settings. While the source of infection could not be established through the rodent investigation, the findings do not exclude alternative transmission pathways, including unobserved rodent exposure, localized reservoir circulation, or possible secondary human-to-human transmission.
Integrated One Health interpretation
Taken together, the combined human serological, molecular, meteorological, and rodent findings illustrate a complex and heterogeneous transmission landscape. From a One Health perspective, this study provides an integrated but exploratory assessment of LF dynamics at the human–animal–environment interface. While the human and environmental components are robust, the rodent component is limited by design and should be interpreted as an opportunistic post-outbreak assessment rather than a structured ecological surveillance study.
Public health implications
From a public health perspective, the findings underscore the need to strengthen integrated Lassa fever early warning systems that combine routine surveillance data with meteorological inputs from the Nigerian Meteorological Agency (NiMet) to enable climate-informed risk prediction. There is also a critical need to enhance diagnostic capacity at primary and secondary health facility levels to ensure early detection of cases and timely clinical management. In addition, sustained community-level interventions focusing on improved sanitation, rodent-proofing of households, and safer food storage practices are essential to reduce human–rodent contact. Given the observed seasonal patterns, preparedness strategies should also prioritize dry-season surge planning, including intensified surveillance, risk communication, and rapid response capacity during periods of increased transmission risk. Finally, strengthening diagnostic capacity, ensuring sustained and sensitive surveillance systems, improving early case detection, and integrating human surveillance with environmental monitoring and climate data within a One Health framework remain critical priorities for improving outbreak preparedness across Nigeria and similar endemic settings.
Limitations
Limitations of the study include the non-random selection of human participants, as only suspected LF cases were enrolled, which may introduce selection bias and limit generalizability to the broader population. Molecular sequencing of RT-qPCR–positive samples could not be performed due to low viral load yield, which limited genome recovery for further molecular characterization and phylogenetic analysis. In addition, the rodent component was restricted to a single LGA, one community, and a single season over a short sampling period, and was based on post-deratization recovery rather than systematic ecological trapping. This may not fully represent the spatial and temporal distribution of Lassa virus reservoirs across Oyo State. The study also employed a cross-sectional design; therefore, associations observed between LASV occurrence and meteorological variables should be interpreted as correlational rather than causal. Overall, the findings should be considered exploratory and hypothesis-generating, and they represent a snapshot of transmission dynamics that cannot be used to infer temporal transmission chains or sustained transmission pathways.
This study demonstrated an overall LASV seroprevalence of 11.1% with IgM seroprevalence of 9.7%, indicating recent infection and IgG seroprevalence of 4.8%, suggesting prior exposure. RT-qPCR analysis confirmed three LASV-positive human cases (1.0%), providing molecular evidence of active infection. Meteorological analysis showed positive association with temperature and negative associations with rainfall and humidity, suggesting seasonal influence on LF occurrence. No LASV RNA was detected in rodent samples recovered during community-based deratization activities. Overall, these findings suggest recent LASV exposure with limited molecular confirmation of active infection among suspected cases in Oyo State, highlighting the need for strengthened surveillance, early detection, and integrated public health response.
This study provides important epidemiological evidence on the seroprevalence, active infection, and transmission dynamics of LF in Oyo State, southwestern Nigeria, highlighting ongoing but under-detected circulation of LASV in the study area. It contributes to understanding the relationship between human infection patterns, environmental factors, and localised transmission hotspots, while emphasising the value of integrating serological, molecular, and meteorological data in Lassa fever surveillance. The findings underscore the need for strengthened diagnostic capacity, sustained surveillance, and application of a One Health-informed approach to improve early detection, outbreak preparedness, and response in endemic settings. These results also add to the growing body of evidence supporting integrated zoonotic disease surveillance in Nigeria. The findings complement other regional One Health surveillance efforts, such as those described by Animasaun et al. 2024 [30], reinforcing the interconnected nature of zoonotic and arboviral disease surveillance.
Suggested Areas for Further Study
What is already known about the topic
What this study adds
The authors sincerely acknowledge the support of the Centre for Human Virology and Genomics, NIMR, particularly Miss Fatimah Awonju, Miss Blessing Agada, and Mr. David Ojo, for their contributions to the laboratory analyses. We also appreciate the assistance of the Oyo State Ministry of Health Emergency Operations Centre staff, especially Dr. Akinyode Akinfemi (Former State Epidemiologist), Mrs. Titilope Akinleye (State Disease Surveillance and Notification Officer), and MLS Ajibola Omotosho (Deputy State Laboratory Focal Person), for their support during fieldwork, sample collection, active case searches, and rodent post-deratization recovery assessment. Gratitude is extended to the Public Health Team at the WHO Oyo State Office, led by Dr. Philips Zorto, for their support throughout the study. We also acknowledge the teaching and non-teaching staff of the Department of Biological Sciences, Lead City University, particularly Dr. Felicia Adesina (Former Head of Department) and Dr. Nike Bakare (Current Head of Department and former Postgraduate Coordinator), for their continuous support and valuable contributions to this study, which was conducted as part of the first author’s PhD thesis.
OSA and RAA conceptualized and designed the study, participated in the fieldwork and laboratory analyses, drafted and refined the manuscript. JOS contributed to the study design, laboratory analyses, and manuscript editing. OPA, AOA, IAK, and BKA participated in fieldwork and assisted with aspects of the laboratory analyses. OOO and FNO supported data management, data analysis, and manuscript writing. BIG and PMN critically reviewed the literature, methodology, and study results; ensured data quality and appropriateness of analysis; recommended revisions to improve the manuscript; AAA provided expert guidance and supervised the rodent post-deratization recovery assessment, and identification contributed to data interpretation. OSA coordinated the overall project implementation and manuscript writing. RAA supervised the project, provided critical technical oversight, and gave final approval for submission. All authors contributed to manuscript drafting, critically reviewed the content for intellectual merit, and approved the final version prior to submission.
Availability of data
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request. Relevant data supporting the findings of this study are included within the published article.
| Variables | Frequency (N=289) | Percentage (%) |
|---|---|---|
| Sex | ||
| Male | 125 | 43.3 |
| Female | 164 | 56.7 |
| Age group in years | ||
| 0–14 | 41 | 14.2 |
| 15–29 | 58 | 20.0 |
| 30–44 | 106 | 36.7 |
| 45–59 | 54 | 18.7 |
| Above 60 | 30 | 10.4 |
| Educational level | ||
| No formal education | 96 | 33.2 |
| Primary | 105 | 36.3 |
| Secondary | 58 | 20.0 |
| Tertiary | 30 | 10.4 |
| Profession/Employment status | ||
| Civil servant | 45 | 15.6 |
| Farming | 59 | 20.4 |
| Cattle Breeders | 80 | 27.7 |
| Self-employed | 47 | 16.3 |
| Trading | 28 | 9.7 |
| Unemployed | 10 | 3.5 |
| Students | 20 | 6.9 |
| Temperature | Rainfall | Humidity | LASV | |
|---|---|---|---|---|
| Temperature | 1 | |||
| Rainfall | -0.61 | 1 | ||
| Humidity | -0.83 | 0.76 | 1 | |
| LASV | 0.69 | -0.63 | -0.78 | 1 |