Outbreak Investigation | Open Access | Volume 9 (2): Article 93 | Published: 04 Jun 2026

Views: 1,056
Menu, Tables and Figures
| Variables | Frequency (N) | Percent (%) |
|---|---|---|
| Gender | ||
| Female | 7 | 46.7% |
| Male | 8 | 53.3% |
| Age Range | ||
| <19 | 1 | 6.7% |
| 20-29 | 4 | 26.7% |
| 30-39 | 6 | 40.0% |
| 40+ | 4 | 26.6% |
| Exposure Category | ||
| Patients | 5 | 33.3% |
| Nurses | 4 | 26.7% |
| Index household members | 3 | 20.0% |
| Doctors | 1 | 6.7% |
| Hospital visitors | 1 | 6.7% |
| Cleaner | 1 | 6.7% |
Table 1: Case Classification by Gender, Age and Exposure Category
| Category | Condition/Symptom | Frequency (N, %) (N=15) |
|---|---|---|
| Comorbidities | Pneumonia | 1 (6.67%) |
| Pulmonary Tuberculosis | 1 (6.67%) | |
| Bacterial Meningitis | 1 (6.67%) | |
| Congestive Heart Failure (CHF) | 1 (6.67%) | |
| Hemorrhagic Stroke | 1 (6.67%) | |
| None | 11 (73.33%) | |
| Symptoms | Rashes | 15 (100%) |
| Itching | 15 (100%) | |
| General Body Weakness | 3 (20%) |
Note: Pneumonia and suspected pulmonary tuberculosis were both diagnosed in the index case.
Table 2: Distribution of reported comorbidities and Symptoms among affected cases (N=15)
Penehafo Laudika Johannes1,2,3,& Ndeshihafela Sakaria2,3, Dianah Mukuture Ewaga1,2, Silas Nghishihange2,3, Emilia Ashipala2,4, Ester Haipinge2,3, Joseph Mumangeni Tomas2,3, Lydia Ndaku Shilelo3
1University of Namibia, Department of Public Health, Oshakati, Namibia, 2Namibia Field Epidemiology and Laboratory Training Programme, Windhoek, Namibia, 3Ministry of Health and Social Services, Oshakati District, Oshakati, Namibia, 4Ministry of Health and Social Services, Epidemiology Division, Health Information and Research Directorate (HIRD), Windhoek, Namibia
&Corresponding author: Penehafo Laudika Johannes, Namibia Field Epidemiology and Laboratory Training Program, Email: johanneslaudika4@gmail.com ORCID: https://orcid.org/0009-0007-1311-5594
Received: 02 Mar 2026, Accepted: 28 May 2026, Published: 04 Jun 2026
Domain: Field Epidemiology
Keywords: Chickenpox, Varicella, Nosocomial outbreak Healthcare workers, Vaccination
©Penehafo Laudika Johannes et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Penehafo Laudika Johannes et al. An outbreak of suspected chickenpox at Intermediate Hospital Oshakati, Namibia, April 2025. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):93. https://doi.org/10.37432/jieph-d-26-00069
Introduction: On 18 April 2025, the Infection Prevention and Control Unit at Intermediate Hospital Oshakati was notified of a cluster of suspected varicella (chickenpox) cases in an adult medical ward. Varicella is highly contagious and can cause severe disease in unvaccinated adults, particularly in healthcare settings. We investigated and described the outbreak and recommended control measures.
Methods: We conducted a descriptive outbreak investigation. A suspected case was defined as any person present at the hospital between 31 March and 25 April 2025 who developed an acute generalised vesicular rash, with or without fever. Cases were identified through register review and interviews. Demographic, clinical, and exposure data were collected using a standardised line list. Data were analysed descriptively by person, place, and time. No analytic study was conducted due to the small number of cases and lack of variability in vaccination status.
Results: Fifteen suspected cases were identified, including healthcare workers (40%), inpatients (33.3%), household contacts (20%), and one visitor (6.7%). The median age was 31 years (IQR: 24–35), with 66.7% aged 20–39 years. The attack rate in the 65-bed ward was 7.7%. Two deaths occurred, yielding a case fatality rate of 13.3%. None of the cases had received varicella vaccination. The epidemic curve suggested propagated transmission consistent with nosocomial spread.
Conclusions: This investigation identified a suspected nosocomial chickenpox outbreak affecting predominantly unvaccinated adults. The case fatality rate highlights their vulnerability to severe varicella outcomes, emphasising the urgent need to introduce varicella vaccination into Namibia’s national immunisation program, with priority given to healthcare workers and young adults. In response to the outbreak, isolation of cases, contact tracing, enhanced infection prevention measures, and active surveillance were implemented. Strengthening laboratory capacity is also recommended to support early detection and response to future outbreaks.
Chickenpox, or varicella, is a highly infectious disease caused by the varicella-zoster virus (VZV), a member of the herpesvirus family, with humans as its only natural host [1]. Varicella primarily spreads through airborne droplets or direct contact with fluid from skin lesions. Although it can affect anyone, children under 10 years are most commonly infected [2]. Symptoms include fever, fatigue, sore throat, and headache, and the illness usually lasts 5 to 7 days. Severe complications such as pneumonia and encephalitis may occur, especially in adults and immunocompromised individuals [3]. Symptoms appear 10 to 21 days after exposure, with an average incubation period of two weeks [4]. The infectious period begins one to two days before the rash appears and lasts approximately seven days, until all lesions have scabbed over [5].
According to the World Health Organisation, varicella affects approximately 140 million people globally each year, resulting in around 4.2 million severe cases requiring hospitalisation and approximately 4,200 deaths [6]. In tropical regions such as Africa, primary infection often occurs later in life compared to temperate, high-income countries, thereby increasing the risk of severe disease. This risk is further exacerbated by high HIV prevalence, ageing populations, and fragile healthcare systems. Despite this burden, there is a lack of synthesised and standardized epidemiological data on varicella in Africa, leading to a probable underestimation of its true impact [7].
In Namibia, chickenpox remains a public health concern, particularly due to limited access to vaccination in state health facilities. As most Namibians rely on public health services and cannot afford private vaccination, the population remains vulnerable to severe complications and death. Although national surveillance data are lacking, localized outbreaks such as the one reported at the University of Namibia’s Rundu Campus in 2018 highlight the continued public health relevance of the disease [8].
On 18 April 2025, the Infection Prevention and Control (IPC) Unit at Intermediate Hospital Oshakati received notification of a suspected chickenpox outbreak within the facility. The report originated from clinical staff who observed an unusual cluster of chickenpox-like symptoms among patients. Following this observation, the IPC Unit promptly alerted the Environmental Health Services for further investigation. A multidisciplinary team was assembled, comprising Senior Environmental Health Practitioners, a registered nurse, a Namibian Field Epidemiology and Laboratory Training Programme (NamFELTP) resident, and a Management Information Systems (MIS) Officer. On 22 April 2025, the team initiated the investigation by conducting face-to-face and telephonic interviews with suspected cases to collect clinical histories and exposure information.
By the time of notification, three suspected cases presenting with generalised vesicular rash had been observed within the same adult medical ward within a short period, meeting the facility’s internal threshold for outbreak alert. Therefore, this investigation aimed to investigate and describe the chickenpox outbreak at Intermediate Hospital Oshakati, identify its source and mode of transmission, and recommend appropriate control and preventive measures.
Outbreak setting
Intermediate Hospital Oshakati (IHO) is a tertiary referral hospital located in Oshakati District, Oshana Region, northern Namibia. The hospital serves a large catchment population of approximately 219,970 people and provides comprehensive healthcare services including inpatient, outpatient, emergency, and specialised medical care. The outbreak occurred in Ward 7, a general medical ward that admits adult patients with various conditions. The ward has a capacity of 65 beds, organised into rooms accommodating up to 10 patients each. During the outbreak period, the ward was operating at full capacity (bed occupancy rate: 100%), with a total staff complement of 25 nurses, three medical doctors, and approximately two intern doctors serving 65 admitted patients with various conditions. Nurses worked across two shifts (07:00–19:00 and 19:00–01:00), with approximately 13 nurses per shift, yielding a nurse-to-patient ratio of approximately 1:5 per shift. Additional support staff (including two cleaners) also worked regularly in the ward. The hospital has an established infection prevention and control structure, with a dedicated IPC and Disease Surveillance Nurse responsible for outbreak detection and response. Prior to this outbreak, Healthcare-Associated Infection (HAI) surveillance initiatives were in place, including a ward register for tracking hospital-acquired infections, routine IPC ward rounds, a reporting system for unusual disease clusters, and existing protocols for airborne precautions and PPE use.
Investigation design
A descriptive approach was used to investigate and describe a chickenpox outbreak among patients at Intermediate Hospital Oshakati in April 2025.
Case definition
This investigation used case definitions adapted from the Council of State and Territorial Epidemiologists (CSTE) and the Centres for Disease Control and Prevention (CDC) varicella surveillance guidelines, modified to reflect the outbreak context and available data [9]. In the absence of laboratory confirmation, a clinical case definition was used to identify suspected cases for the purpose of outbreak detection and response.
Suspected Case: Any individual present in Intermediate Hospital Oshakati between 31 March and 25 April 2025 who developed an acute illness with a generalised vesicular rash, with or without fever and malaise.
Probable Case: A suspected case with an epidemiological link to another suspected case, including shared ward admission, direct contact with a suspected case, or exposure within the outbreak setting during the incubation period.
Confirmed Case: Not applicable in this investigation, as laboratory confirmation for varicella-zoster virus was not achieved due to specimen rejection and improper sample handling.
Data collection
Data collection involved reviewing the hospital register between 31 March and 25 April 2025 to identify suspected chickenpox cases using a standardized line list. Key variables included age, sex, symptom onset, rash onset, vaccination status, comorbidities, and outcomes. Face-to-face and phone interviews were conducted with suspected cases and their contacts to gather clinical histories and assess exposure. A structured contact tracing form was used to collect demographic data, exposure details, and symptom history. Data collection encompassed three distinct processes: index case identification through register review and clinical records; contact tracing to map exposures and identify persons at risk; and active case finding to detect additional cases among patients, healthcare workers, household contacts, and healthcare workers who sought care at private health facilities, where contact tracing was coordinated by the Oshakati district outbreak response team. This process helped identify the index case and additional cases linked to the outbreak. Where face-to-face interviews were not feasible, primarily because affected healthcare workers had sought care at private health facilities away from the hospital, and some household contacts resided outside the immediate area, telephonic interviews were conducted as the only practicable alternative. This approach may have introduced a risk of case misclassification, which is acknowledged in the limitations.
Attack rate calculation
The patient attack rate was calculated by dividing the number of suspected cases among patients by the total number of patients in the general medical ward during the outbreak period. Only patients who were exposed within the ward were included in this calculation. The overall healthcare worker (HCW) attack rate was calculated by dividing the number of affected HCWs by the total number of HCWs working in Ward 7 during the outbreak period (25 nurses, three doctors, two interns, and two cleaners; n=32). A nurse-specific attack rate was additionally calculated using only nurses as both the numerator and denominator to assess occupational risk within this cadre and to inform the nurse-to-patient ratio analysis.
Laboratory diagnosis
Initial specimens intended for varicella-zoster virus (VZV) PCR and Mpox testing were collected from two admitted cases but were rejected by the Namibia Institute of Pathology due to improper specimen handling, specifically the use of incorrect sample containers. Following the rejection, and given that both sampled patients had subsequently died, pus swabs were collected from the same two cases, representing 13.3% of the total suspected cases as the only remaining feasible specimens. These were sent to the Namibia Institute of Pathology for diagnostic assessment and examined using Gram stain microscopy, bacterial culture, and antibiotic susceptibility testing. No further specimens were collected from the remaining active cases, as the majority of affected healthcare workers sought and received treatment at private health facilities, where clinical diagnoses of chickenpox were made based on compatible presentation.
Data analysis
Descriptive analysis was conducted using Microsoft Excel. Continuous variables, such as age, were summarised using the median and interquartile range (IQR), while age was further categorised into four groups: <19 years, 20–29 years, 30–39 years, and 40 years and above. Categorical variables were analysed, and findings were presented in tabular and graphical formats to illustrate distribution patterns among cases. Given the small number of cases and the absence of variability in key exposures, particularly vaccination status, no analytic study was conducted, and no measures of association were calculated.
Ethical approval
Approval for the study was granted by the Ministry of Health and Social Services (Ref: 22/4/2/3). Participants were provided with relevant information about the data collection process, and verbal informed consent was obtained prior to participation. Confidentiality was ensured by securely storing all data in password-protected folders.
Demographic characteristics of the cases
A total of 15 individuals were affected in the chickenpox outbreak at Intermediate Hospital Oshakati, including one index case and 14 secondary cases. Males accounted for 53.3% (n = 8) and females for 46.7% (n = 7). The median age was 31 years (IQR: 24–35), with most cases aged 30–39 years (40.0%). Of these, 6 (40.0%) were healthcare workers, 5 (33.3%) were inpatients, 3 (20.0%) were household members of the index case, and 1 (6.7%) was a hospital visitor (Table 1).
Case description
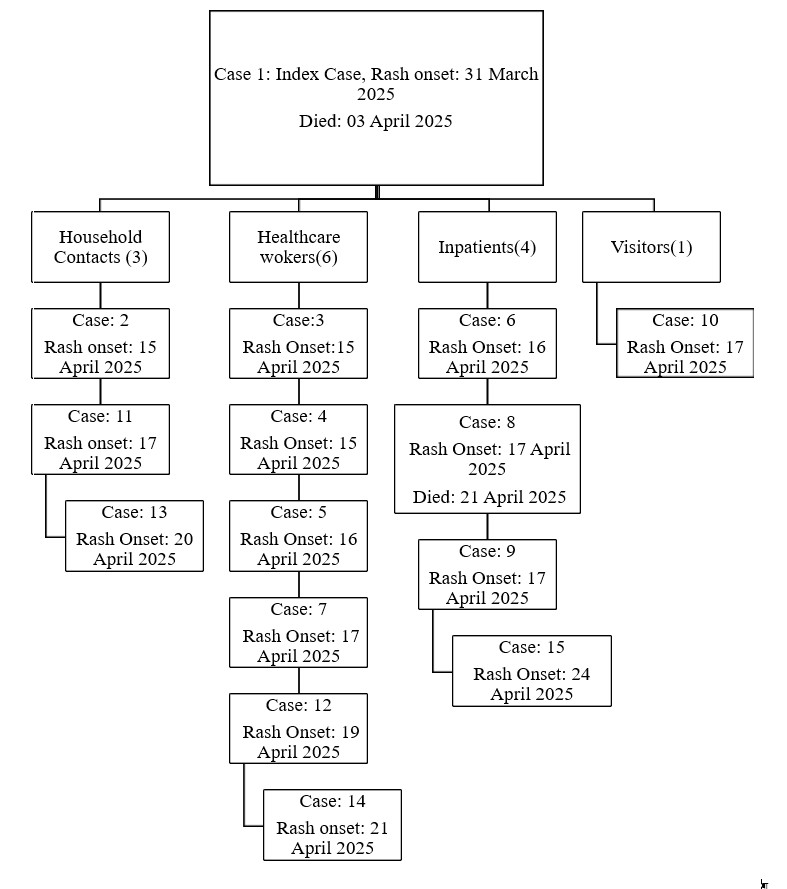
The index case was a 50-year-old male who travelled from Angola to Namibia on 01 March 2025 seeking medical care. On 31 March 2025, while in Ongwediva, he developed a generalised vesicular rash with prominent itching, with lesions distributed across the trunk, face, and extremities, present simultaneously at multiple stages of development (macules, papules, and vesicles). This distribution pattern is consistent with primary varicella infection rather than herpes zoster reactivation, which typically presents as a unilateral, dermatomal rash. Nursing staff who clinically assessed the rash noted the absence of features characteristic of Mpox, including deep pustular lesions, significant lymphadenopathy, and palms-and-soles involvement. Although the index case had recently travelled from Angola, a country reporting active Mpox transmission during the same epidemic period, the clinical rash characteristics were more consistent with primary varicella.
He presented to Intermediate Hospital Oshakati on 01 April 2025 with a history of coughing for more than one month and was admitted on the same day to Ward 7, Room 1, where he shared the room with two other patients: a 17-year-old male admitted for bacterial meningitis and a 26-year-old male admitted for congestive heart failure (CHF), who later became the second fatality. He was admitted with diagnoses of community-acquired pneumonia (CAP) and suspected pulmonary tuberculosis (PTB). No formal diagnosis of chickenpox was made at admission; a skin biopsy was taken, with results still pending at the time of the investigation. HIV testing returned a negative result, making immunosuppression an unlikely contributor to his illness, and bacteriological confirmation of PTB was not achieved, limiting the ability to fully attribute his death to any single condition. He was not placed in isolation immediately upon admission, remaining in Room 1 with the two other patients before being later transferred to an isolation room within the same ward. The exact duration of shared exposure prior to isolation could not be determined, as the index case died on 03 April 2025, before the formal investigation commenced on 22 April 2025, having been moved to an isolation room within the same ward shortly before his death.
Following his death, a total of 14 secondary cases were recorded between 15 and 24 April 2025, comprising four inpatients, six healthcare workers, three household contacts of the index case, and one hospital visitor, all of whom had close contact with the index case either through sharing the same ward space or through occupational exposure (Figure 1).
The second fatality was a 26-year-old male patient with congestive heart failure who had been admitted to Room 1 of Ward 7 on 26 March 2025, five days prior to the index case’s admission on 01 April 2025. He therefore shared Room 1 directly with the index case from 01 April 2025 until the index case was transferred to isolation. He developed chickenpox symptoms, including itching and blisters on the body, on 17 April 2025, consistent with the 10–21-day incubation period following exposure to the index case. HIV testing returned a negative result, ruling out HIV-related immunosuppression as a contributing factor. He was subsequently transferred to isolation but died on 21 April 2025. Given that congestive heart failure carries significant baseline mortality, and that his varicella presentation was limited to cutaneous lesions with no documented features of severe disease such as pneumonitis or encephalitis, the direct causal contribution of varicella to his death remains uncertain. A formal death audit was not conducted
Epidemic curve
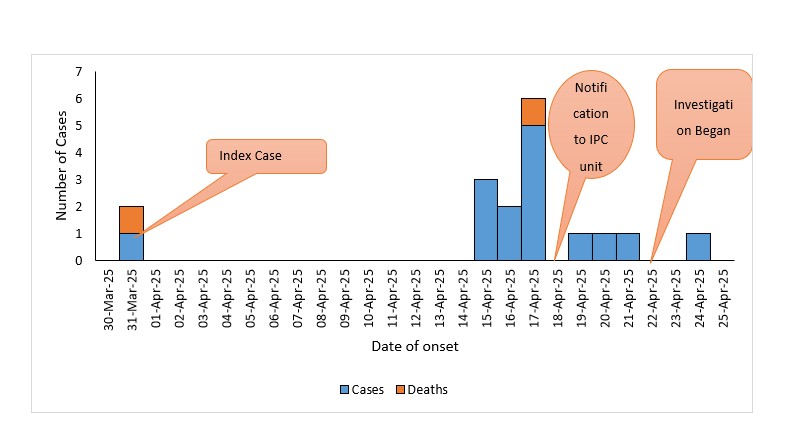
The first symptom onset in this outbreak occurred on 31 March 2025, marking the probable start of the outbreak period. The epidemic curve (Figure 2) shows an increase in the number of cases from 15 April 2025, with a peak on 17 April 2025 when five cases were reported. A total of 15 cases were recorded between 31 March and 24 April 2025.
Magnitude of Outbreak
All 15 individuals identified during the outbreak met the case definition for suspected chickenpox. The ward was operating at full capacity, with a bed occupancy rate of 100% during the outbreak period. A patient attack rate of 7.7% (5/65) was recorded among patients in the 65-bed ward, with two deaths resulting in a case fatality rate of 13.3%. The overall outbreak affected 15 individuals across all exposure categories, including patients, healthcare workers, household contacts, and one visitor.
Among healthcare workers, six individuals (four nurses, one intern doctor, and one cleaner) developed suspected chickenpox. Of the 25 nurses assigned to Ward 7, four developed suspected chickenpox, yielding a nurse attack rate of 16.0% (4/25). The overall HCW attack rate was 18.8% (6/32), based on a total HCW denominator of 32 (25 nurses, three doctors, two interns, and two cleaners). Three household contacts of the index case met the suspected case definition. As the total number of household members exposed to the index case was not fully documented, a secondary attack rate among household contacts could not be calculated.
Comorbid conditions were noted in four cases (26.7%); the index case presented with both pneumonia and suspected pulmonary tuberculosis, while one case each presented with bacterial meningitis, congestive heart failure, and haemorrhagic stroke, each accounting for 6.7%. The remaining 11 cases (73.3%) had no documented underlying conditions. All suspected cases presented with rashes and itching (100%), and 3 (20%) experienced general body weakness (Table 2).
Laboratory results
The two pus swab specimens yielded growth of Staphylococcus aureus, consistent with secondary bacterial infection of skin lesions rather than primary varicella-zoster virus (VZV) infection. PCR confirmation of VZV was not achieved due to initial specimen rejection. Clinical diagnoses of chickenpox made at private facilities among affected healthcare workers, together with compatible clinical features and strong epidemiological links, which include shared ward exposure, temporal clustering, and contact with the index case, collectively support the classification of all 15 cases as suspected varicella. No cases were classified as probable or confirmed; all 15 cases met the suspected case definition only, as laboratory confirmation was not achieved. Mpox was considered a differential diagnosis given the epidemiological context; however, laboratory testing for Mpox was also not performed due to the same specimen handling limitations.
A varicella (chickenpox) outbreak is defined as the occurrence of five or more epidemiologically linked cases within a specific setting, such as a hospital ward or household, with each new case appearing within 10 to 21 days after the previous one, the incubation period for the virus [10]. This investigation identified a nosocomial varicella outbreak at Intermediate Hospital Oshakati, as the number of cases exceeded the expected threshold and was consistent with person-to-person propagated transmission originating from a single index case. The epidemic curve supports this interpretation, demonstrating clustering of secondary cases within one incubation period following exposure to the index case in a shared ward setting.
The age distribution observed in this outbreak deviates from the classical epidemiological profile of varicella, which typically affects children under 10 years in high-transmission settings. The shift toward adults aged 20–39 years is consistent with emerging evidence from China, where surveillance data reported by Luan et al. showed increasing varicella incidence among adolescents and young adults, particularly in the 15–19 age group [11]. Our findings suggest a further shift toward older adults, likely reflecting delayed primary exposure due to gaps in childhood immunisation and waning natural immunity. This highlights the need to review current outbreak preparedness and adjust vaccination strategies to better protect young adults. The complete absence of varicella vaccination among affected individuals is consistent with a similar outbreak reported in Yirga Chefe, Southern Ethiopia [12]. Both outbreaks highlight the high transmission potential of varicella in close-contact, low-immunity settings, emphasising the critical role of vaccination in preventing nosocomial spread.
The case fatality rate must be interpreted with considerable caution due to significant pre-existing comorbidities in both deceased cases and the absence of a formal death audit. Given these confounding factors, the CFR reported here is unlikely to reflect the true severity of varicella alone and should not be used as a standalone indicator of varicella mortality in this context.
The patient attack rate of 7.7% recorded in this outbreak, although seemingly low, should be interpreted in the context of a fully occupied 65-bed ward operating under constrained staffing conditions and high patient turnover. This rate reflects transmission among admitted patients only. Among the 25 nurses assigned to Ward 7, a nurse attack rate of 16.0% (4/25) was recorded, and the overall HCW attack rate was 18.8% (6/32), highlighting substantial occupational risk in this setting. Nosocomial varicella outbreaks in comparable low-vaccination hospital settings have reported patient attack rates ranging from 10% in a 50-bed rehabilitation ward in India to 14% in a hospital outbreak triggered by herpes zoster, suggesting that timely implementation of airborne precautions and isolation in this investigation may have partially limited patient-to-patient transmission [13]. Nevertheless, the extension of cases beyond the ward to healthcare workers, household contacts, and a visitor emphasizes that the effective reproductive number exceeded what the patient attack rate alone captures, highlighting the importance of a whole-facility rather than ward-confined approach to nosocomial outbreak containment.
An important differential diagnosis to consider is Mpox, particularly given the epidemiological context of recent travel from Angola, a country reporting active Mpox transmission during the same epidemic period, and the age group predominantly affected, which mirrors the distribution of Mpox cases in ongoing African outbreaks [14–17]. However, the clinical presentation was more consistent with primary varicella, characterized by a generalized vesicular rash with lesions simultaneously at multiple stages of development, rather than the deep pustular lesions, significant lymphadenopathy, and palms-and-soles involvement typically associated with Mpox. Although the collective clinical and epidemiological evidence supports varicella as the more probable diagnosis, the inability to rule out Mpox through laboratory testing remains an important limitation.
Regarding vaccination, the varicella vaccine is currently not included in Namibia’s national EPI, with access largely limited to the private sector, rendering it unaffordable for the majority of the population who rely on public health services [8]. Evidence from countries with routine varicella vaccination programs demonstrates significant reductions in incidence, hospitalisations, and deaths [18]. Given that the varicella vaccine has never been included in Namibia’s national EPI and is unavailable in the public sector, there was no prior occasion at which any of the affected individuals would have been expected to be vaccinated, underscoring the programmatic gap this outbreak exposes. Given the epidemiological shift toward adults and healthcare workers observed in this outbreak, a targeted vaccination strategy is recommended as a first step, prioritising healthcare workers at occupational risk and young adults aged 20–39 years. As vaccine coverage and health system capacity strengthen, a transition toward routine childhood vaccination within the EPI should be considered to achieve long-term population immunity.
Prior to this outbreak, the hospital had Healthcare Associated Infection (HAI) surveillance initiatives in place, including ward registers for tracking hospital acquired infections, routine IPC ward rounds, reporting systems for unusual disease clusters, and established airborne precaution and PPE protocols. Despite these existing structures, the outbreak exposed gaps in the timely implementation of isolation measures and proper specimen handling. Similar findings have been reported in hospitals in Bangladesh and South Africa, where overcrowding and understaffing compromised the effective implementation of IPC measures despite existing protocols [19,20]. In addition, delayed recognition and isolation of varicella cases have previously been identified as major contributors to nosocomial VZV transmission in healthcare settings [21]. These findings highlight the need to strengthen and reinforce existing IPC systems and practices rather than establish entirely new mechanisms. Furthermore, the dispersal of cases to private health facilities emphasizes the importance of stronger collaboration between the public and private health sectors for surveillance, contact tracing, and case management during public health events. This challenge has also been reported across sub–Saharan Africa, where fragmented surveillance systems limit timely outbreak detection and response [22]. Staffing constraints in this outbreak, including a fully occupied ward with a nurse-to-patient ratio of approximately 1:5 per shift, likely reduced the capacity for close patient monitoring and consistent adherence to IPC protocols, thereby facilitating nosocomial spread. Similar evidence from a tertiary-level hospital study showed that higher patient-nurse ratios were associated with an increased risk of healthcare-associated infections, including nosocomial varicella [23].
Applying the 7-1-7 framework revealed substantial gaps in timeliness. Detection occurred approximately 18 days after symptom onset, nearly three times the 7-day target. This delay was largely due to the index case’s death before diagnosis, the absence of varicella from Namibia’s notifiable disease list, and limited laboratory capacity. Although the investigation began four days after notification, the outbreak had already peaked by that time. These delays are consistent with findings from multi-country 7-1-7 evaluations, where limited laboratory capacity and gaps in notifiable disease legislation are among the most frequently reported barriers to timely detection [24,25]. An outbreak early action review is therefore recommended as a quality improvement initiative to systematically identify and address bottlenecks that contributed to the delayed response and to strengthen preparedness for future nosocomial outbreaks.
Limitation
The source of exposure could not be definitively established, as the index case died before the investigation commenced. Moreover, the initial PCR specimens were rejected by the laboratory due to improper specimen handling, and no further specimens were collected from remaining active cases, limiting laboratory confirmation of VZV. The inability to rule out Mpox through laboratory testing also remains an important limitation given the epidemiological context. The long incubation period made it challenging to determine the outbreak’s true extent. A formal death audit was not conducted, making it difficult to confirm whether fatalities were directly attributable to varicella or underlying comorbidities, and therefore the CFR should be interpreted with caution. Furthermore, varicella is not a notifiable disease in Namibia, which may have contributed to underreporting. Additionally, this investigation was primarily descriptive, and no analytical study was performed to statistically assess risk factors. However, potential contributing factors such as lack of vaccination, close contact in shared spaces, and existing comorbidities were observed descriptively; therefore, confounding could not be assessed. The total number of household members exposed to the index case was not fully documented, precluding calculation of a secondary attack rate among contacts.
Public Health Action Taken
Following the identification of a suspected chickenpox outbreak at Intermediate Hospital Oshakati, several immediate public health actions were taken to control the spread and protect both patients and healthcare workers. All suspected cases were promptly isolated and treated to reduce the risk of transmission. Healthcare workers and anyone who had contact with infected individuals were required to wear appropriate personal protective equipment (PPE) at all times, in line with airborne precaution protocols. The affected ward was thoroughly disinfected using appropriate cleaning agents, and routine cleaning and disinfection were intensified to maintain high standards of infection prevention and control.
Pus swab samples were collected and sent to the Namibia Institute of Pathology for laboratory testing. Healthcare workers and patients who were affected were interviewed to assess their exposure and vaccination status, and to identify additional contacts. Contact tracing commenced immediately, with all exposed individuals placed under active monitoring. Daily surveillance checks were carried out in other wards to quickly identify any new cases. The outbreak was officially reported to hospital management and the district surveillance team to coordinate the response. Movement of patients and visitors in and around the isolation room was restricted to limit further spread.
Strengthening of healthcare-associated infection (HAI) surveillance and IPC protocols was identified as a critical area for improvement, particularly in light of recent major nosocomial outbreaks globally, including Marburg virus disease in Rwanda, Ebola virus disease outbreaks, and Mpox, all of which have highlighted the devastating consequences of inadequate IPC measures in healthcare settings [26–28]. In response, in-service training on laboratory surveillance, including proper specimen collection, handling, and triple packaging, was recommended to address gaps identified during the investigation. Enhanced adherence to existing IPC protocols, including airborne precaution measures and appropriate PPE use, was also reinforced across all wards.
This investigation identified a nosocomial outbreak of suspected varicella (chickenpox) at Intermediate Hospital Oshakati in April 2025. The findings reveal an epidemiological shift in the burden of varicella infection, with the majority of cases occurring among unvaccinated adults aged 20–39 years. These results highlight the urgent need to introduce varicella vaccination into Namibia’s national immunization program, with priority given to healthcare workers and young adults. Strengthening HAI surveillance and IPC practices within healthcare facilities is equally critical to prevent and rapidly contain future nosocomial outbreaks. The delayed detection observed in this investigation was partly attributable to varicella not being a notifiable disease in Namibia; adding it to the national notifiable disease list is therefore recommended to improve surveillance sensitivity and enable more timely outbreak detection and response in future.
Recommendation
What is already known about the topic
What this study adds
The authors did not receive any specific funding for this work.
Data availability
The dataset upon which the findings are based belong to the Ministry of Health and social services of Namibia under the Epidemiology sub-division. The dataset is publicly available upon request from the corresponding author and with permission from the Ministry of Health and Social Services.
The author would like to extend their sincere gratitude to the clinical staff at Intermediate Hospital Oshakati for their prompt outbreak reporting. Special appreciation is also extended to the patients and household contacts for their valuable cooperation throughout the investigation. Furthermore, the University of Namibia and the Field Epidemiology and Laboratory Training Program (FELTP) are acknowledged for their continuous academic guidance and mentorship during this study.
Penehafo Laudika Johannes drafted the proposal, cleaned and analyzed the data, and wrote the manuscript. Ndeshihafela Sakaria and Lydia Shilelo reviewed the proposal, the results, and the manuscript. Silas Nghishihange, Emilia Ashipala, Dianah Ewaga, Tomas Joseph, and Ester Haipinge contributed by reviewing the proposal and the results.
| Variables | Frequency (N) | Percent (%) |
|---|---|---|
| Gender | ||
| Female | 7 | 46.7% |
| Male | 8 | 53.3% |
| Age Range | ||
| <19 | 1 | 6.7% |
| 20-29 | 4 | 26.7% |
| 30-39 | 6 | 40.0% |
| 40+ | 4 | 26.6% |
| Exposure Category | ||
| Patients | 5 | 33.3% |
| Nurses | 4 | 26.7% |
| Index household members | 3 | 20.0% |
| Doctors | 1 | 6.7% |
| Hospital visitors | 1 | 6.7% |
| Cleaner | 1 | 6.7% |
| Category | Condition/Symptom | Frequency (N, %) (N=15) |
|---|---|---|
| Comorbidities | Pneumonia | 1 (6.67%) |
| Pulmonary Tuberculosis | 1 (6.67%) | |
| Bacterial Meningitis | 1 (6.67%) | |
| Congestive Heart Failure (CHF) | 1 (6.67%) | |
| Hemorrhagic Stroke | 1 (6.67%) | |
| None | 11 (73.33%) | |
| Symptoms | Rashes | 15 (100%) |
| Itching | 15 (100%) | |
| General Body Weakness | 3 (20%) |
Note: Pneumonia and suspected pulmonary tuberculosis were both diagnosed in the index case.