Outbreak Investigation | Open Access | Volume 9 (2): Article 85 | Published: 26 May 2026

Views: 1,025
Menu, Tables and Figures
| Variable | Laboratory Outcome | Total suspected cases n(%) N=62 (100%) | |
|---|---|---|---|
| Positive n(%) N=6 (9.7%) | Negative n(%) N=56 (90.3%) | ||
| Age group (years) | Age range (1-68) years | ||
| <5 | 0 (0.0) | 3 (5.4) | 3 (4.8) |
| 5-14 | 0 (0.0) | 10 (17.9) | 10 (16.1) |
| 15-24 | 4 (66.7) | 24 (42.9) | 28 (45.2) |
| 25-34 | 0 (0.0) | 7 (12.5) | 7 (11.3) |
| 35-44 | 0 (0.0) | 6 (10.7) | 6 (9.7) |
| ≥45 | 2 (33.3) | 6 (10.7) | 8 (12.9) |
| Median age (IQR) | 19 (5-58) years | ||
| Sex | |||
| Female | 2 (33.3) | 32 (57.1) | 34 (54.8) |
| Male | 4 (66.7) | 24 (42.9) | 28 (45.2) |
| Occupation | |||
| Farmers | 4 (66.7) | 26 (46.4) | 30 (48.4) |
| Traders | 1 (16.7) | 13 (23.2) | 14 (22.6) |
| Government workers | 0 (0.0) | 3 (5.4) | 3 (4.8) |
| Student | 1 (16.7) | 14 (25) | 15 (24.2) |
| Sub-districts | |||
| Ahamansu | 0 (0.0) | 0 (0) | 0 (0.0) |
| Dodi | 0 (0.0) | 1 (1.8) | 1 (1.6) |
| Dodo | 0 (0.0) | 0 (0) | 0 (0.0) |
| Kadjebi-Asato | 6 (100) | 55 (98.2) | 61 (98.4) |
| Pampawie | 0 (0.0) | 0 (0) | 0 (0.0) |
| Health Facilities | |||
| Asato CHPS | 0 (0.0) | 7 (12.5) | 7 (11.3) |
| Dzindziso CHPS | 1 (16.7) | 7 (12.5) | 8 (12.9) |
| Kadjebi Health Centre | 5 (83.3) | 41 (73.2) | 46 (74.2) |
| Poase Cement Health Centre | 0 (0.0) | 1 (1.8) | 1 (1.6) |
Table 1: Summary of Dengue fever cases by Laboratory Outcome, Kadjebi District, July 1– August 16, 2024
Lambert Nyamekye Asamoah1,&, Eric Takyi1, John Sonnyinado Duako Baffoe2,3, Emmanuel Agbodogli1, Derrick Jack Atitsu1, Vida Akoma1, Mawuli Gohoho3,4, Thomas Vigbedor2,3, Charles Kwame Gedzeah1
1Kadjebi District Health Directorate, Ghana Health Service, Kadjebi, Ghana, 2Oti Regional Health Directorate, Ghana Health Service, Worawora, Ghana, 4Jasikan Municipal Health Directorate, Ghana Health Service, Jasikan, Ghana, 3Ghana Field Epidemiology and Laboratory Training Programme, Ghana
&Corresponding author: Lambert Nyamekye Asamoah, Kadjebi District Health Directorate, Ghana Health Service, Kadjebi, Ghana, Email: lambertasamoah@gmail.com ORCID: https://orcid.org/0009-0004-3168-7658
Received: 06 Mar 2025, Accepted: 22 May 2026, Published: 26 May 2026
Domain: Infectious Disease Epidemiology
Keywords: Dengue-like illness, Outbreak investigation, Kadjebi District, Aedes mosquito, Acute febrile illness
©Lambert Nyamekye Asamoah et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Lambert Nyamekye Asamoah et al., Dengue fever outbreak investigation in Kadjebi District, Ghana, 2024. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):85. https://doi.org/10.37432/jieph-d-26-00073
Introduction: Dengue fever is an arboviral disease transmitted by Aedes mosquitoes and is increasingly recognized in tropical areas where clinical overlap with malaria complicates diagnosis. In July 2024, two confirmed dengue cases were notified in Kadjebi District, Ghana, prompting a field investigation to confirm, characterize the outbreak, and guide control measures.
Methods: A descriptive outbreak investigation was conducted using line list data, active case search, and environmental assessment. Suspected cases were defined as residents of the district presenting with acute febrile illness of 2–7 days’ duration with at least two compatible symptoms from July 1, 2024, to August 16, 2024. Serum samples were tested using rapid antigen detection and serological assays (IgM and IgG). Descriptive analysis summarized person, place, and time characteristics.
Results: A total of 62 suspected cases were identified, with a median age of 19 years (IQR: 5–58); 54.8% were female. Farmers (48.4%) and students (24.2%) were the most affected groups. Only 9.7% of cases were IgG positive, while all samples tested negative for antigen and IgM. The epidemic curve showed a sharp rise in early August 2024, followed by a rapid decline. Environmental assessment for 60 households identified multiple potential Aedes breeding sites, including discarded tyres 18(30%), natural water-holding sites 14(23.3%), blocked gutters 10 (16.7%), and uncovered water containers 7(11.7%).
Conclusion: The investigation identified a cluster of past infections of dengue fever illness in Kadjebi district with ecological conditions favourable for Aedes breeding. However, laboratory findings did not indicate acute dengue infection. Integrated vector control and household environmental sanitation targeted at the elimination of mosquito breeding sites, alongside improved surveillance, is recommended to prevent potential dengue transmission.
Dengue fever is a viral disease transmitted by Aedes mosquitoes, particularly Ae. aegypti and Ae. albopictus, and occurs widely in tropical and subtropical areas, mainly in urban and semi-urban settings [1]. It presents as a severe influenza-like illness that affects infants, children, and adults, though it rarely results in death [2]. Globally, more than 14 million dengue cases were reported in 2024 (from 6.8 million in 2023), corresponding to a case fatality rate (CFR) of 0.07%. The global surge in these cases may be attributed to several factors, not limited to globalization, rapid urbanization, and climate change [3]. In Africa, 168,851 cases were recorded during the same period, with a CFR of 0.09% [4]. However, this condition is often underdiagnosed because its clinical presentation overlaps with other common febrile illnesses, such as malaria [5].
In Ghana, unusual cases of malaria-like illness unresponsive to standard anti-malarial treatment were reported in 2024 across several districts in the Eastern Region and managed as acute febrile illness. Laboratory testing at the Noguchi Memorial Institute for Medical Research (NMIMR) using RT-PCR confirmed Dengue fever. This unusual event resulted in the Ghana Health Service declaring an outbreak on July 14, 2024, which in turn heightened surveillance across districts in the country [6].
On July 29, 2024, the National Public Health Reference Laboratory (NPHRL) notified the Kadjebi District Health Directorate of two confirmed cases of Dengue fever through the Surveillance Outbreak Response Management and Analysis System (SORMAS). This event is particularly significant as it represents the first confirmed dengue cases in the district, which suggests possible local transmission and necessitates an immediate public health response. Based on the above, a field investigation was conducted to confirm, characterise the outbreak, and implement control measures.
Outbreak design and setting
We conducted a retrospective descriptive outbreak investigation in the Kadjebi District of Ghana, which incorporated active case search and review of line list data. Dengue fever diagnosis and public awareness in the district were low before the identification of past infection cases. The district is bordered to the north by the Nkwanta South Municipality, south by the Jasikan Municipality, south-west by the Biakoye District, and North-West by the Krachi East Municipal. It also has a long border that stretches eastwards to the Republic of Togo [7]. The district experiences annual rainfall ranging from 1400 mm to 1800 mm, typically occurring from March to October or November, with a peak in June. These climatic conditions are highly conducive to mosquito breeding and also support agricultural activities, which often increase human–vector contact. In response to the endemic malaria burden associated with these ecological conditions, the district implements routine malaria elimination measures, including larval source management through monthly disinfection of mosquito breeding sites and seasonal malaria chemoprevention for children under five years during periods of peak transmission [8].
Case definition
A suspected case was defined as any person resident in the Kadjebi District between July 1, 2024, and August 16, 2024, with acute febrile illness of 2–7 days duration accompanied by two or more of the following: headache, retro-orbital pain, myalgia, arthralgia, rash, haemorrhagic manifestations, or leucopaenia [9]. A confirmed case was also defined as any suspected case with laboratory confirmation of dengue infection, evidenced by a positive IgM antibody or a fourfold or greater increase in IgG antibody titres in serum specimens.
Specimen collection and transportation
Serum samples were collected and transported under cold chain conditions to the National Public Health Reference Laboratory (NPHRL) for dengue testing using rapid antigen detection and serological assays (IgM and IgG). Samples were triple-packaged and accompanied by case-based forms, with data entered into the SORMAS, in line with standard protocols [9].
Case finding
To identify additional cases, the contact tracing team followed up on the first confirmed cases in their households to identify and screen suspected and epidemiologically linked cases. In addition, the records review team visited Kadjebi Health Centre, where suspected cases identified between July 1, 2024, and August 16, 2024, were retrieved and actively followed up, with the necessary sample collection carried out.
Environmental assessment
The environmental assessment team conducted field visits in affected communities to identify potential mosquito breeding sites. Households and their immediate surroundings were observed using a standard checklist. The assessment focused on the presence of stagnant water and common Aedes breeding habitats such as water storage containers, discarded tyres, and blocked drainage.
Data source, tools, and variables collected
Standard IDSR tools, including SORMAS, dengue fever case investigation form, and contact line-listing form, were used to obtain data from all suspected cases. All information captured on SORMAS at the district level was accessible to the Regional Surveillance Officer, the Disease Surveillance Department, and the NPHRL. As cases were also accessible to the NPHRL, laboratory results were directly updated on SORMAS. The variables captured included demographics, symptoms, onset date, hospitalisation, exposure history, risk factors such as poor sanitation, standing water, high _Aedes_ mosquito exposure, and weak immunity increase the chance of severe disease, treatments, and laboratory results.
Data analysis
A retrospective descriptive analysis was conducted using the district-based line list of suspected dengue cases extracted from the SORMAS. Data was cleaned and analyzed in Microsoft Excel software, with variables standardized. Cases were classified based on their laboratory outcome. Descriptive statistics summarized person, place, and time. Age was reported as median (IQR), while categorical variables were presented as frequencies and proportions. Temporal trends were assessed using epidemic curves, and spatial distribution was described by health facility and subdistrict.
Ethical consideration
This investigation was part of the public health response, conducted in line with national IDSR guidelines, and therefore did not require ethical approval. However, permission was obtained from Kadjebi District Health Directorate before the investigation. Verbal informed consent was sought from the participants interviewed. Confidentiality was maintained using coded identifiers and password-protected data storage throughout the investigation.
Descriptive epidemiology
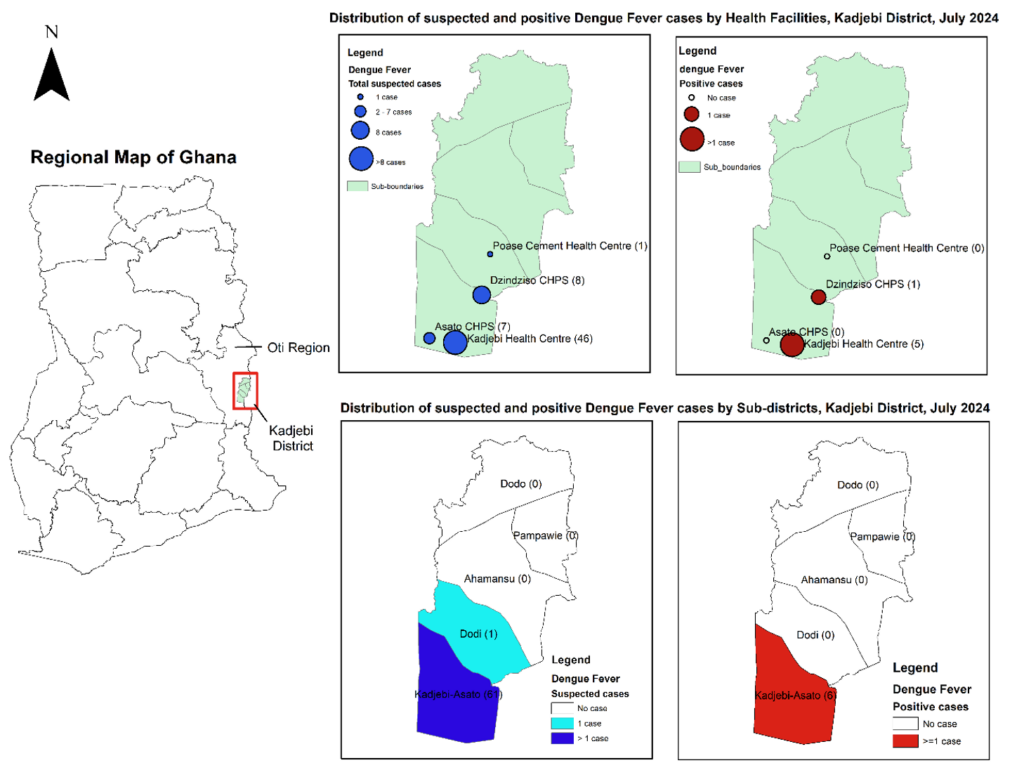
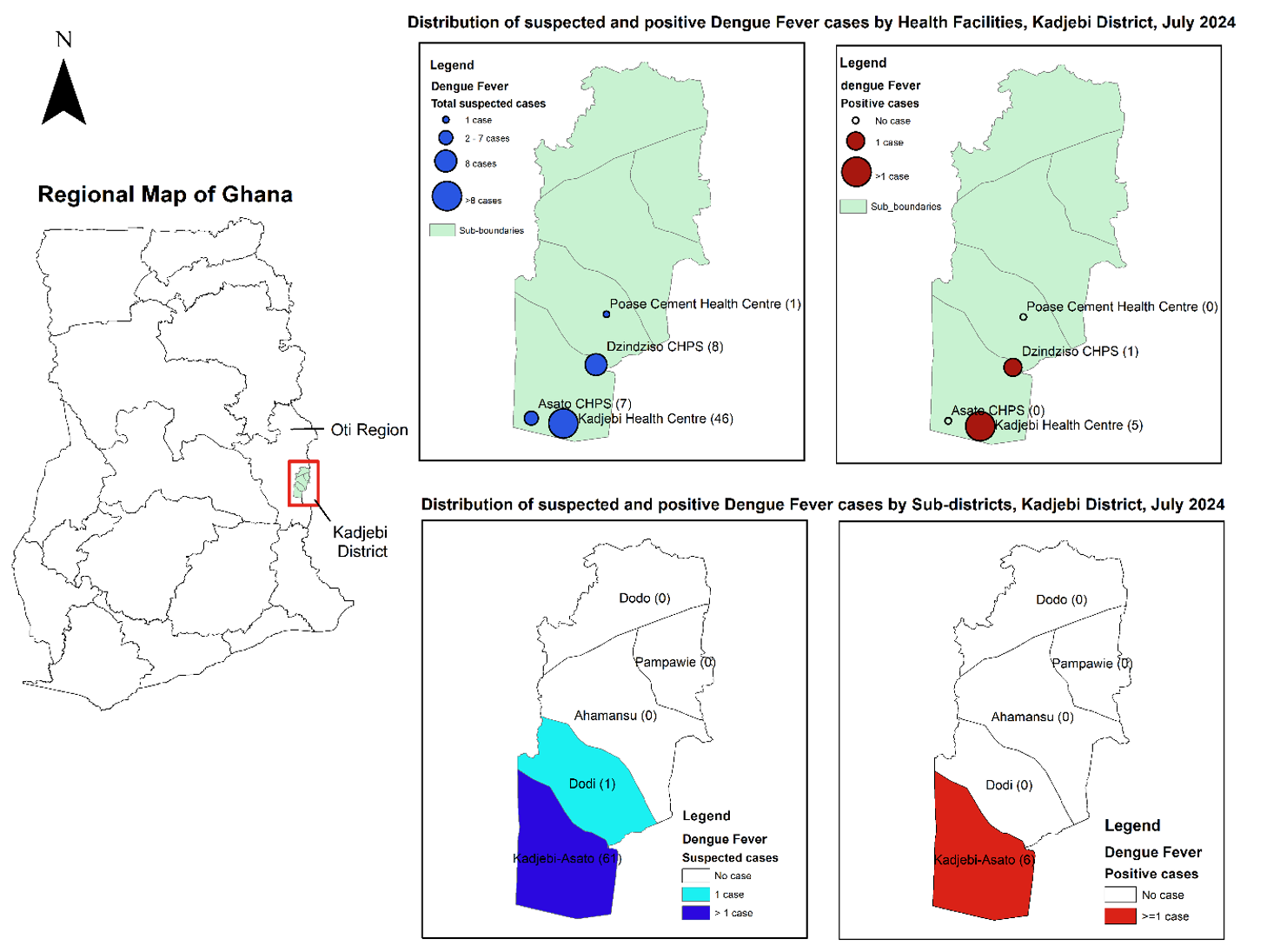
Overall, we identified 62 suspected cases, of which 34 (54.8%) were female and 28 (45.2%) were male. Nearly half of the cases, 28 (45.2%), were aged 15–24 years, followed by 10 (16.1%) in the 5–14 year age group, while children under 5 contributed the fewest cases, 3 (4.8%). The median age was 19 years, with an interquartile range (IQR) of 5–58 years. In terms of occupation, 30 (48.4%) were farmers, and students comprised one-quarter of the cases, 15 (24.2%) (Table 1). Almost all cases, 61 (98.4%), resided in the Kadjebi-Asato sub-district. Among health facilities, Kadjebi Health Centre reported the highest number of cases, 46 (74.2%), followed by Dzindziso CHPS with 8 (12.9%) (Figure 1).
Laboratory outcome
Six (9.7%) of the suspected cases were serologically positive (IgG) cases. All cases tested negative for both antigen detection and IgM. Among the IgG-positive cases, 4 (66.7%) were aged 15–24 years, and 4 (66.7%) were male. Farmers comprised the majority of positive cases, 4 (66.7%). All positive cases were reported in the Kadjebi-Asato sub-district. Specifically, Kadjebi Health Centre reported 5 (83.3%) of the positive cases, while Dzindziso CHPS reported 1 (16.7%) (Figure 1).
Temporal distribution of cases
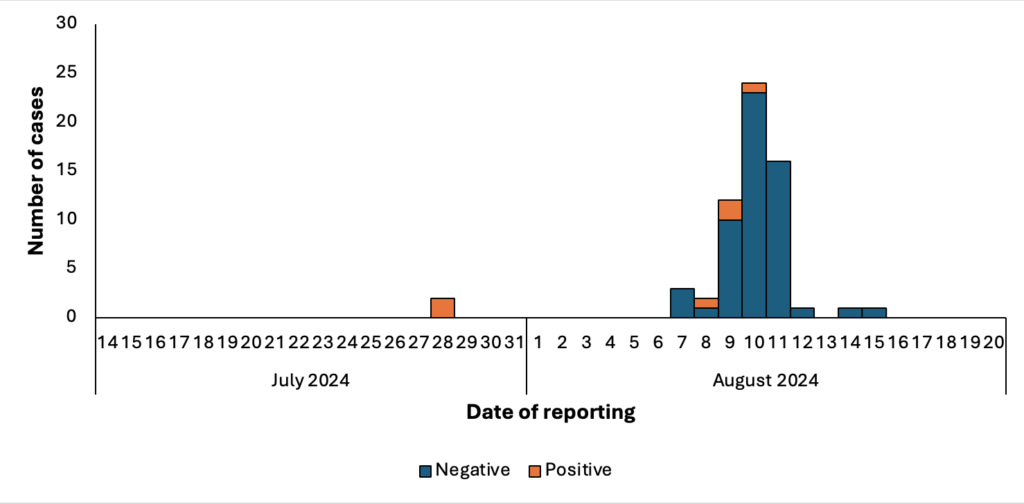
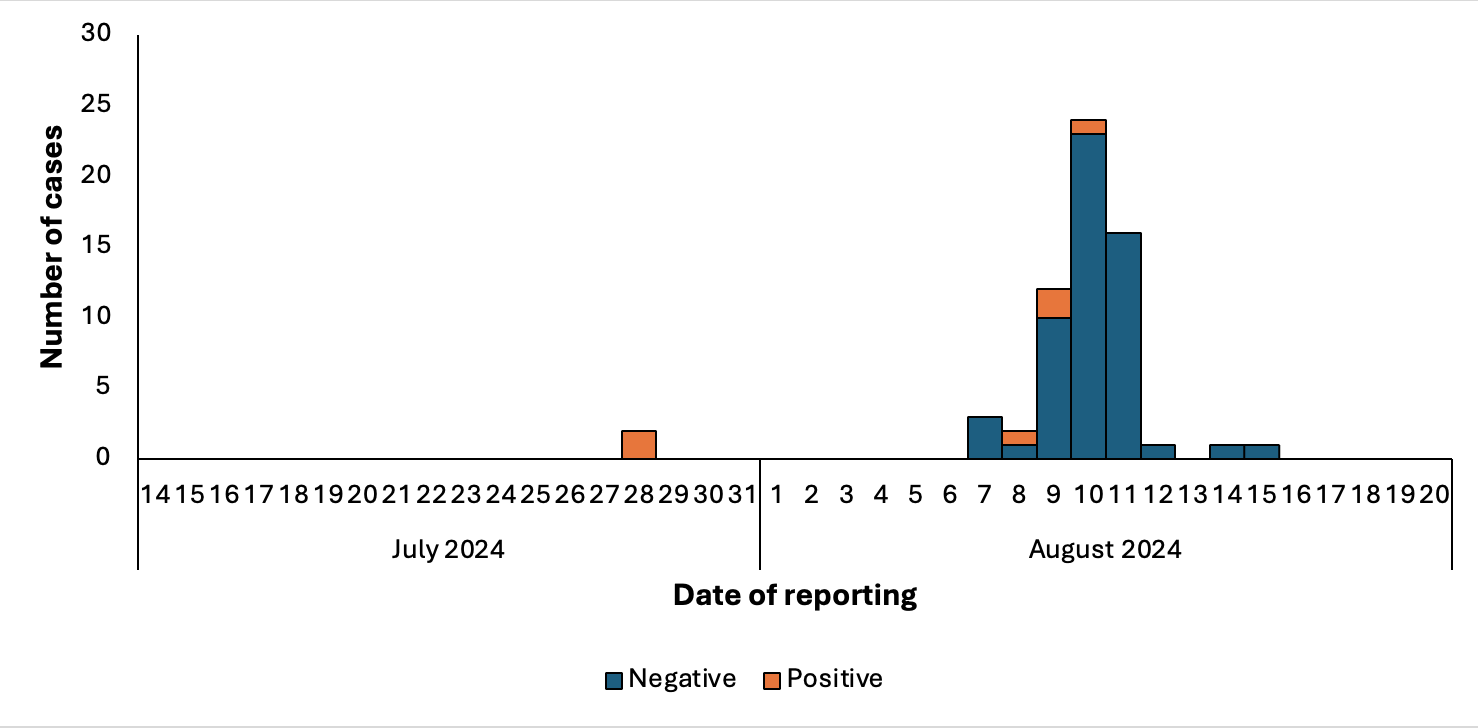
The first two confirmed cases were reported to the facility on July 28, 2024. One case involved a student and the other a farmer. No additional cases were reported until August 7, 2024, when the field investigation was underway. The number of cases reported increased sharply in early August, rising from 3 cases to a peak of 24, before declining to a single case on August 15, 2024. Apart from the two positive cases reported on July 28, 2024, active case searches and contact tracing identified four additional cases between August 8 and August 10, 2024 (Figure 2).
Environmental assessment
We observed that among 60 household environments assessed, uncovered or poorly covered water containers were present in 7(11.7%) of households. Discarded items such as tyres and containers were found in 18 (30%) of compounds. Blocked drainages with stagnant water were identified in 10 (16.7%). Natural water-holding sites were noted in 14 (23.3%) of households.
This investigation identified evidence of dengue-like illness with serological evidence of past exposure in the Kadjebi district of Ghana. Most suspected cases occurred among young adults aged 15–24 years, with farmers and students constituting the most affected groups. This pattern is consistent with findings from other African settings, where younger populations are disproportionately affected due to higher exposure to outdoor environments and vector habitats [10]. A study reported that a total of 157,031 suspected cases were recorded across 10 of the 15 ECOWAS member states, the majority of whom were young people. Of these, 72,799 were confirmed or probable cases, resulting in 748 deaths and an overall case fatality rate of 1.0% [11].
The epidemic curve showed a sharp increase in early August, followed by a rapid decline. This pattern suggests focal transmission, although laboratory findings do not provide evidence of acute dengue infection. The observed trend is consistent with conditions that may favour mosquito breeding during the rainy season, as described in the ecological context of the district where rainfall supports vector proliferation [12]. The subsequent decline may reflect intensified surveillance and response measures following outbreak notification, including active case search and contact tracing, which enhanced case detection during the early phase of the response.
The laboratory findings suggest no evidence of acute dengue infection among tested samples, as all specimens were negative for both antigen and IgM. The presence of IgG positivity alone indicates prior exposure to dengue or a related flavivirus and does not support recent infection or active transmission within the district. This highlights important diagnostic limitations in outbreak investigations relying solely on serological testing, particularly when samples are collected outside the acute phase of illness. Similar challenges have been reported in Ghana and other endemic settings, where molecular testing such as RT-PCR is required to confirm acute dengue infection among patients initially misclassified as malaria [10]. Despite the absence of laboratory confirmation of acute infection, the clustering of clinically compatible cases, temporal association, and epidemiological linkage support a syndromic outbreak of dengue-like illness.
Environmental assessment identified multiple potential breeding sites, including discarded tyres, blocked gutters, uncovered containers, and natural water-holding areas. These findings are consistent with known Aedes breeding behaviour in Ghana, where both artificial and natural habitats contribute to transmission [12]. Although larval source management is routinely implemented for malaria control, dengue vectors exploit additional habitats that may not be routinely targeted. This highlights the need for integrated vector control approaches alongside community engagement.
This outbreak mirrors patterns seen in other African settings, where dengue is often underdiagnosed due to clinical similarity with malaria. In Ghana, recognition of dengue was initially prompted by malaria-like illness unresponsive to treatment in 2024 [4], reinforcing the importance of including dengue in the differential diagnosis of acute febrile illness.
As part of the public health response, existing malaria prevention interventions were promoted at the household level, including the use of insecticide-treated nets, wearing of long-sleeved clothing, and environmental sanitation measures such as cleaning gutters and emptying stagnant water from containers, including cans and tyres. Health facilities were also engaged and oriented on the signs and symptoms of dengue fever to support intensified surveillance and early case detection.
Limitations
The interpretation of these findings should consider these limitations, including reliance on IgG-based testing, which reflects past exposure rather than acute infection, and the restriction of the investigation to a single district, which may underestimate the broader extent of similar febrile illness.
This investigation identified a cluster of dengue-like illness in Kadjebi District, mainly among young adults and persons engaged in farming and schooling activities. This cluster occurred during the rainy season, which favours mosquito breeding in the presence of discarded tyres and containers and uncovered water storage containers within household environments. Although IgG positivity was detected, there was no evidence of acute dengue infection and laboratory findings did not support recent or active transmission. Integrated vector control and household environmental sanitation targeted at elimination of mosquito breeding sites, alongside improved surveillance is recommended to prevent potential dengue transmission and strengthen outbreak detection.
What is already known about the topic
What this study adds
Lambert N. Asamoah led the investigation and response to the outbreak and wrote the manuscript. Thomas Vigbedor, Emmanuel Agbodogli, Derrick J. Atitsu, Vida Koma, and Charles K. Gedzeah provided technical assistance during the outbreak investigation. During the outbreak investigation, John S.D. Baffoe and Mawuli Gohoho provided technical guidance, data analysis, as well as edited the manuscript. The outbreak investigation and response were supervised by Eric Takyi and Alphonsus Nindow, who also edited and reviewed the manuscript. All authors have read and approved the manuscript for publication.
| Variable | Laboratory Outcome | Total suspected cases n(%) N=62 (100%) | |
|---|---|---|---|
| Positive n(%) N=6 (9.7%) | Negative n(%) N=56 (90.3%) | ||
| Age group (years) | Age range (1-68) years | ||
| <5 | 0 (0.0) | 3 (5.4) | 3 (4.8) |
| 5-14 | 0 (0.0) | 10 (17.9) | 10 (16.1) |
| 15-24 | 4 (66.7) | 24 (42.9) | 28 (45.2) |
| 25-34 | 0 (0.0) | 7 (12.5) | 7 (11.3) |
| 35-44 | 0 (0.0) | 6 (10.7) | 6 (9.7) |
| ≥45 | 2 (33.3) | 6 (10.7) | 8 (12.9) |
| Median age (IQR) | 19 (5-58) years | ||
| Sex | |||
| Female | 2 (33.3) | 32 (57.1) | 34 (54.8) |
| Male | 4 (66.7) | 24 (42.9) | 28 (45.2) |
| Occupation | |||
| Farmers | 4 (66.7) | 26 (46.4) | 30 (48.4) |
| Traders | 1 (16.7) | 13 (23.2) | 14 (22.6) |
| Government workers | 0 (0.0) | 3 (5.4) | 3 (4.8) |
| Student | 1 (16.7) | 14 (25) | 15 (24.2) |
| Sub-districts | |||
| Ahamansu | 0 (0.0) | 0 (0) | 0 (0.0) |
| Dodi | 0 (0.0) | 1 (1.8) | 1 (1.6) |
| Dodo | 0 (0.0) | 0 (0) | 0 (0.0) |
| Kadjebi-Asato | 6 (100) | 55 (98.2) | 61 (98.4) |
| Pampawie | 0 (0.0) | 0 (0) | 0 (0.0) |
| Health Facilities | |||
| Asato CHPS | 0 (0.0) | 7 (12.5) | 7 (11.3) |
| Dzindziso CHPS | 1 (16.7) | 7 (12.5) | 8 (12.9) |
| Kadjebi Health Centre | 5 (83.3) | 41 (73.2) | 46 (74.2) |
| Poase Cement Health Centre | 0 (0.0) | 1 (1.8) | 1 (1.6) |