Research | Open Access | Volume 9 (2): Article 98 | Published: 12 Jun 2026
Views: 25
Menu, Tables and Figures
| Characteristic | Total n (%) | FETP-Trained n (%) | Non-Trained n (%) | p-value |
|---|---|---|---|---|
| Sex | 0.070 | |||
| Female | 41 (31.8) | 6 (14.6) | 35 (85.4) | |
| Male | 88 (68.2) | 26 (29.5) | 62 (70.5) | |
| Education Level | 0.310 | |||
| Bachelor’s Degree | 43 (33.3) | 13 (30.2) | 30 (69.8) | |
| Diploma | 86 (66.7) | 19 (22.1) | 67 (77.9) | |
| Work Experience (years) | <0.0001 | |||
| <6 | 66 (51.2) | 4 (6.1) | 62 (93.9) | |
| 6–10 | 40 (31.0) | 19 (47.5) | 21 (52.5) | |
| >10 | 23 (17.8) | 9 (39.1) | 14 (60.9) | |
| Age (years) | 0.023 | |||
| <25 | 13 (10.1) | 0 (0.0) | 13 (100.0) | |
| 25–29 | 39 (30.2) | 8 (20.5) | 31 (79.5) | |
| 30–34 | 49 (38.0) | 12 (24.5) | 37 (75.5) | |
| ≥35 | 28 (21.7) | 12 (42.9) | 16 (57.1) | |
| Region | 0.018 | |||
| CRR | 31 (24.0) | 6 (19.4) | 25 (80.6) | |
| LRR | 19 (14.7) | 9 (47.4) | 10 (52.6) | |
| NBER | 11 (8.5) | 5 (45.5) | 6 (54.5) | |
| WHR2 | 68 (52.7) | 12 (17.6) | 56 (82.4) |
Table 1: Demographic Characteristics by FETP Training Status of Public Health Officers, The Gambia, 2025
| Domain / Indicator | Score Range | FETP-Trained (n = 32) Mean (SD) | Non-Trained (n = 97) Mean (SD) | p-value |
|---|---|---|---|---|
| Knowledge | ||||
| Overall knowledge score | 0–100% | 89.3 (11.4) | 81.6 (15.0) | 0.040 |
| Core surveillance functions | 0–8 | 6.8 (1.2) | 6.0 (1.9) | 0.030 |
| Knowledge of immediately notifiable diseases | 0–7 | 5.7 (1.3) | 4.9 (1.7) | 0.020 |
| Knowledge of reporting frequency requirements | 0–1 | 0.94 (0.24) | 0.86 (0.35) | 0.210 |
| Attitude | ||||
| Overall attitude score | 0–100% | 96.9 (4.8) | 89.8 (12.4) | 0.420 |
| Positive perception of surveillance importance | 1–2 | 2.0 (0.0) | 2.0 (0.2) | 0.560 |
| Confidence in detecting and reporting diseases | 1–2 | 1.9 (0.3) | 1.8 (0.4) | 0.180 |
| Motivation for routine surveillance reporting | 1–2 | 1.9 (0.3) | 1.9 (0.3) | 0.340 |
| Perceived institutional support for surveillance | 1–2 | 1.9 (0.3) | 1.7 (0.5) | 0.090 |
| Practice | ||||
| Overall practice score | 0–100% | 65.3 (17.8) | 57.2 (13.9) | 0.020 |
| Public health surveillance activities | 0–8 | 5.4 (2.0) | 4.6 (2.1) | 0.040 |
| Use of DHIS2 for reporting | 0–1 | 0.78 (0.42) | 0.69 (0.46) | 0.320 |
| Submission of weekly surveillance reports | 0–1 | 0.81 (0.40) | 0.72 (0.45) | 0.290 |
| Data quality practices (composite) | 0–100% | 70.2 (16.5) | 63.1 (19.0) | 0.040 |
| Data analysis and reporting activities | 0–100% | 68.5 (15.2) | 60.8 (17.1) | 0.030 |
Table 2: Comparison of Knowledge, Attitude, and Practice Scores Between FETP-Trained and Non-Trained Public Health Officers, The Gambia, 2025
| Variable | Adjusted Mean Difference β (95% CI) | p-value |
|---|---|---|
| Had FETP Training | ||
| Yes vs No | 8.24 (4.12 – 12.36) | <0.001 |
| Age | ||
| ≥35 vs <35 years | 3.45 (-0.89 – 7.79) | 0.118 |
| Sex | ||
| Male vs Female | 1.98 (-2.34 – 6.30) | 0.367 |
| Education Level | ||
| Bachelor’s vs Diploma | 5.67 (1.45 – 9.89) | 0.009 |
| Work Experience | ||
| ≥6 vs <6 years | 4.23 (0.01 – 8.45) | 0.049 |
| Region | ||
| CRR vs WHR2 | -2.15 (-7.01 – 2.71) | 0.382 |
| LRR vs WHR2 | 3.89 (-1.89 – 9.67) | 0.186 |
| NBER vs WHR2 | 4.12 (-2.34 – 10.58) | 0.210 |
| Had Other Public Health Training | ||
| Yes vs No | 2.45 (-5.67 – 10.57) | 0.552 |
| Constant | ||
| — | 72.34 (65.21 – 79.47) | <0.001 |
| Dependent Variable: Knowledge Score (%). Bold values indicate statistical significance (p < 0.05). β = unstandardized regression coefficient; CI = confidence interval. | ||
Table 3: Factors Associated with Knowledge (Multivariate Linear Regression) of Public Health Officers in Disease Surveillance in the Gambia, 2025
| Variable | Adjusted Mean Difference β (95% CI) | p-value |
|---|---|---|
| Had FETP Training | ||
| Yes vs No | 6.78 (3.12 – 10.44) | <0.001 |
| Knowledge Score | ||
| Per 10% increase | 1.23 (0.45 – 2.01) | 0.002 |
| Age | ||
| ≥35 vs <35 years | 2.34 (-1.45 – 6.13) | 0.224 |
| Sex | ||
| Male vs Female | 1.12 (-2.34 – 4.58) | 0.523 |
| Education Level | ||
| Bachelor’s vs Diploma | 2.89 (-0.78 – 6.56) | 0.122 |
| Work Experience | ||
| ≥6 vs <6 years | 3.45 (-0.23 – 7.13) | 0.066 |
| Region | ||
| CRR vs WHR2 | -4.23 (-8.45 – -0.01) | 0.049 |
| LRR vs WHR2 | 2.15 (-2.71 – 7.01) | 0.382 |
| NBER vs WHR2 | 3.45 (-2.34 – 9.24) | 0.241 |
| Perceived Institutional Support | ||
| Per 1-point increase | 2.67 (1.34 – 4.00) | <0.001 |
| Constant | ||
| — | 68.23 (58.34 – 78.12) | <0.001 |
| Dependent Variable: Attitude Score (%). Bold values indicate statistical significance (p < 0.05). β = unstandardized regression coefficient; CI = confidence interval. | ||
Table 4: Factors Associated with Attitude Score (Multivariate Linear Regression) of Public Health Officers in Disease Surveillance in The Gambia, 2025
| Variable | Adjusted Mean Difference β (95% CI) | p-value |
|---|---|---|
| Had FETP Training | ||
| Yes vs No | 7.89 (3.45 – 12.33) | <0.001 |
| Knowledge Score | ||
| Per 10% increase | 2.34 (1.12 – 3.56) | <0.001 |
| Attitude Score | ||
| Per 10% increase | 1.89 (0.67 – 3.11) | 0.002 |
| Age | ||
| ≥35 vs <35 years | 4.56 (0.89 – 8.23) | 0.015 |
| Sex | ||
| Male vs Female | 3.21 (0.45 – 6.87) | 0.085 |
| Education Level | ||
| Bachelor’s vs Diploma | 5.34 (1.67 – 9.01) | 0.005 |
| Work Experience | ||
| ≥6 vs <6 years | 4.89 (1.23 – 8.55) | 0.009 |
| Region | ||
| CRR vs WHR2 | -3.45 (-7.89 – 0.99) | 0.127 |
| LRR vs WHR2 | 6.78 (1.34 – 12.22) | 0.015 |
| NBER vs WHR2 | 7.12 (1.01 – 13.23) | 0.023 |
| Use of Surveillance Tools | ||
| Per 1-point increase | 4.23 (2.89 – 5.57) | <0.001 |
| Had Conducted Data Analysis | ||
| Yes vs No | 8.45 (4.89 – 12.01) | <0.001 |
| Dependent Variable: Practice Score (%). Model R² = 0.452. Bold values indicate statistical significance (p < 0.05). β = unstandardized regression coefficient; CI = confidence interval. | ||
Table 5: Factors Associated with Practice Score (Multivariate Linear Regression) of Public Health Officer in Diseases Surveillance, The Gambia
Sambou Mbye1,2,&, Obafemi Joseph Babalola3
1School of Public Health, University of Education, The Gambia, 2Gambia Field Epidemiology Training Program, Epidemic and Disease Control, Ministry of Health, The Gambia, 3Africa Field Epidemiology Network (AFENET), Plot 42 Lugogo Bypass, Kampala, Uganda.
&Corresponding author: Sambou Mbye, School of Public Health, University of Education, The Gambia, Email: mbyesambou@gmail.com ORCID: https://orcid.org/0009-0001-4956-2907
Received: 08 Mar 2026, Accepted: 09 Jun 2026, Published: 12 Jun 2026
Domain: Field Epidemiology
Keywords: Field Epidemiology Training Program, Disease Surveillance, Knowledge, Attitudes, and Practices, Public Health Officers, The Gambia
©Sambou Mbye et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Sambou Mbye et al., Impact of the Field Epidemiology Training Program on knowledge, attitudes, and practices of public health officers in disease surveillance in The Gambia. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):98. https://doi.org/10.37432/jieph-d-26-00074
Introduction: The Field Epidemiology Training Program (FETP) was established in The Gambia to strengthen disease surveillance capacity among public health officers. Evidence on its impact on surveillance-related knowledge, attitudes, and practices (KAP) in the country remains limited. This study assessed factors associated with KAP among public health officers, with a particular focus on FETP training.
Methods: A cross-sectional survey was conducted among 129 public health officers across four health regions in The Gambia, including FETP-trained (n = 32) and non-trained (n = 97) personnel. Data were collected using a structured electronic questionnaire. Composite KAP scores were calculated as percentages. Bivariate analyses compared characteristics between groups. Multivariate linear regression models identified factors associated with knowledge, attitude, and practice scores.
Results: FETP-trained officers were significantly more likely to have ≥6 years of experience (p<0.0001) and be ≥35 years old (p=0.023). Distribution varied significantly by region (p=0.018). Overall mean scores were 83.5% (SD=14.5) for knowledge, 91.6% (SD=11.5) for attitude, and 59.2% (SD=15.3) for practice. FETP training was independently associated with significantly higher knowledge (β=8.24, p<0.001), attitude (β=6.78, p<0.001), and practice scores (β=7.89, p<0.001). Higher education (β=5.67, p=0.009) and work experience (β=4.23, p=0.049) were also associated with knowledge. Practice scores were additionally associated with knowledge (β=2.34, p<0.001), attitude (β=1.89, p=0.002), region, use of surveillance tools (β=4.23, p<0.001), and conducting data analysis (β=8.45, p<0.001).
Conclusion: FETP training is a strong, independent predictor of higher KAP scores among public health officers in The Gambia. However, the persistent knowledge-practice gap and regional variations highlight the need for concurrent system-level investments
Efficient and responsive disease surveillance systems are fundamental to global health security, enabling the early detection, verification, and control of infectious disease threats [1]. The World Health Organization emphasizes that robust surveillance is essential for timely public health action and for preventing localized events from evolving into widespread epidemics [2,3]. However, many low- and middle-income countries face persistent challenges, including shortages of trained epidemiologists and limited surveillance infrastructure, which hinder effective outbreak response [4,5].
To bridge these workforce gaps, the Field Epidemiology Training Program (FETP) was established globally, modelled after the U.S. Centres for Disease Control and Prevention’s Epidemic Intelligence Service. FETP uses a hands-on, “learning-by-doing” approach to build competencies in outbreak investigation, surveillance system strengthening, epidemiological analysis, and evidence-based decision-making [6]. Evaluations have shown that FETP contributes significantly to building national epidemiological capacity [7].
In West Africa, the 2014–2016 Ebola Virus Disease (EVD) outbreak, which resulted in 28,616 cases and 11,310 deaths across affected countries, exposed significant failures in national surveillance and response systems, underscoring the urgent need for a skilled field epidemiology workforce at all levels of the health system [8,9]. In response to these gaps, The Gambia launched its FETP training in 2016 through collaboration between the Ministry of Health and international partners. Since its inception, the program has trained 198 health professionals who have contributed to the detection and management of priority outbreaks, including COVID-19, measles, and meningitis [10].
FETP participation improves the knowledge, attitudes, and practices (KAP) of public health workers [11,12], but no similar evaluation has been conducted in The Gambia. Globally, the existing assessments of the FETPs often focus on outputs such as investigations conducted or graduates produced, rather than on changes in core competencies and behaviours among trained officers [13]. Given that frontline public health officers form the backbone of the national disease surveillance system, understanding whether FETP training improves their KAP is essential for evaluating the program’s effectiveness and informing future workforce development strategies [14]. This study, therefore, compared demographic characteristics between FETP-trained and non-trained public health officers; described itemised knowledge, attitude, and practice levels; identified factors associated with knowledge scores; determined predictors of attitude scores, including the role of knowledge; and assessed the independent effects of FETP training, knowledge, and attitudes on surveillance practices. Findings will support national efforts to strengthen epidemiological capacity, refine the FETP curriculum, and improve the country’s preparedness and response to public health threats.
Study design and setting
A cross-sectional study was conducted among public health officers involved in disease surveillance across four of The Gambia’s seven health regions. The Gambia is one of the smallest nations on the African continent with 2.7 million inhabitants [15]. The Ministry of Health (MoH), through the Epidemiology and Disease Control unit, is in charge of organizing, carrying out, and overseeing national public health initiatives, including disease surveillance and outbreak response efforts.
The Gambia established its own FETP in 2016 in collaboration with the African Field Epidemiology Network (AFENET), the U.S. CDC, the West Africa Health Organisation (WAHO), and other partners. Since then, eleven cohorts of frontline FETP and one cohort of FETP intermediates have been trained and graduated [16]. Both FETP-trained and non-FETP-trained public health officers were deployed as surveillance officers in The Gambia.
Study population and sampling
The study population consisted of Public Health Officers (PHOs) involved in disease surveillance at both district and regional levels in The Gambia. Participants included FETP-trained and non-FETP-trained personnel such as Disease Surveillance Officers, Regional Surveillance Officers, and Public Health Officers whose roles involve detecting, reporting, and responding to notifiable diseases and public health threats. The study included both Frontline and Intermediate Field Epidemiology Training Program (FETP) trainees. However, given that only one cohort of Intermediate-level trainees had been trained at the time of the study, FETP training was treated as a binary variable (trained vs. non-trained) in the analysis.
A multistage stratified sampling approach was used to select four of the seven health regions: Western Health Region 2 (WHR2), Central River Region (CRR), North Bank East Region (NBER), and Lower River Region (LRR).
PHOs actively involved in surveillance and outbreak response at regional, district, or facility levels were included, while those PHOs absent or on extended leave during data collection were excluded.
Sample size determination
The sample size for this study was determined to ensure adequate statistical power and representativeness of public health officers involved in surveillance and outbreak response across selected regions of The Gambia. The calculation was based on a finite population correction formula appropriate for cluster and stratified survey designs, as described by Dean and Sullivan (2013). The total population of eligible public health officers across the selected regions was estimated at 210. An assumed prevalence (p) of 31.6% was used, informed by findings from [17], with a precision (d) of ±5% and a confidence level of 95%, corresponding to a Z-score of 1.96 and an alpha level of 0.05. To account for the multistage stratified sampling and clustering at regional and facility levels, a design effect (DEFF) was incorporated into the calculation. Applying these parameters to the sample size equation resulted in a minimum required sample of 129 participants. This sample size was considered sufficient to provide reliable estimates while accounting for population size, sampling design, and expected variability, thereby ensuring the validity and generalizability of the study findings across the selected regions and health system levels [18].
Data collection
Data were collected using a structured, self-administered questionnaire deployed on KoBoToolbox. The tool was adapted from standard KAP survey frameworks and aligned with Integrated Disease Surveillance and Response (IDSR) guidelines and FETP competencies [19]. Content validity was reviewed by public health and surveillance experts, and the tool was pilot-tested with a small group of public health officers outside the study sites [20].
The questionnaire captured:
Variables and scoring
Knowledge: Assessed by 10 questions on core surveillance functions, immediately notifiable diseases, and reporting frequency. Each correct answer scored 1, with total scores converted to percentages.
Attitudes: Assessed by 8 questions using a 5-point Likert scale. Scores were summed up and converted to percentages.
Practices: Assessed by 13 questions on participation in public health activities (8 items), use of surveillance tools (3 items), data quality practices (1 composite), and data activities (1 composite). Responses were scored on a 0-2 scale (0=never/no participation, 1=occasional, 2=regular/frequent), summed, and converted to percentages.
Independent Variables: FETP training status, age, sex, education level, years of experience, region, other public health training, knowledge score, attitude score, perceived institutional support, use of surveillance tools, and having conducted data analysis in the past 6 months.
Data analysis
Data were analyzed using SPSS version 27 and R. Descriptive statistics summarized participant characteristics. Bivariate analyses (chi-square tests, independent t-tests) compared characteristics and crude KAP scores between FETP-trained and non-trained groups. Variables considered epidemiologically relevant based on prior literature and study objectives were initially assessed in bivariate analyses. Variables with a p-value <0.20 in bivariate analyses, together with variables considered important a priori (including age, sex, education level, work experience, and FETP training status), were entered into the multivariable regression models. This approach was used to identify independent predictors while controlling for potential confounding.
Model 1 (Knowledge): FETP training, age, sex, education, experience, region, other training
Model 2 (Attitude): FETP training, knowledge score, age, sex, education, experience, region, perceived institutional support
Model 3 (Practice): FETP training, knowledge score, attitude score, age, sex, education, experience, region, use of surveillance tools, and conducted data analysis
Spatial distribution of trained staff was mapped using QGIS.
Ethical considerations
This study was conducted under the administrative authority of the Ministry of Health as part of a routine public health surveillance system evaluation, in accordance with the Public Health Act 1989 of The Gambia, which mandates disease surveillance, reporting, and response to public health events. For the primary data collection phase, written informed consent was obtained from all surveillance personnel; participation remained voluntary and confidential. All data were processed anonymously, adhering to the ethical principles of the Declaration of Helsinki and national data protection statutes. Findings are intended solely for the optimisation of the Integrated Disease Surveillance and Response (IDSR) framework.
Of the 129 participants, 32 (24.8%) received FETP training. The majority were male (68.2%) and held a diploma as their highest educational qualification (66.7%). FETP-trained personnel were significantly more likely to have 6 or more years of work experience (p<0.0001) and to be 35 years or older (p=0.023). The distribution of trained staff also varied significantly by region (p=0.018), with LRR and NBER having a higher proportion of FETP-trained officers compared to WHR2 and CRR (Table 1).
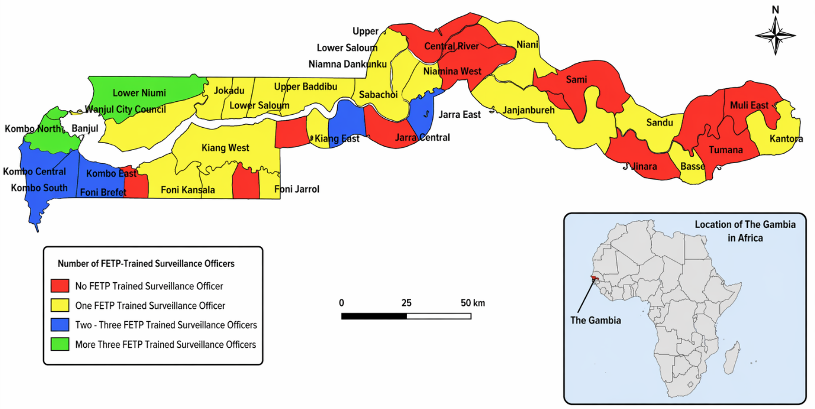
Geographical distribution of FETP-trained staff
Spatial analysis revealed an uneven distribution of FETP-trained personnel across the country. Several districts, particularly in rural regions, had no FETP-trained staff, while others were well-covered, indicating a disparity in training coverage (Figure 1).
Overall, FETP-trained officers demonstrated significantly higher knowledge and practice scores compared to their non-trained counterparts. The mean overall knowledge score was higher among trained officers (89.3 ± 11.4) than non-trained officers (81.6 ± 15.0), and this difference was statistically significant (p = 0.040). Similar patterns were observed across key knowledge components, including core surveillance functions (p = 0.030) and knowledge of immediately notifiable diseases (p = 0.020). However, there was no statistically significant difference in knowledge of reporting frequency requirements (p = 0.210, Table 2).
Although FETP-trained officers had higher mean attitude scores (96.9 ± 4.8) compared to non-trained officers (89.8 ± 12.4), this difference was not statistically significant (p = 0.420). Likewise, no significant differences were observed across individual attitude indicators, including perception of surveillance importance, confidence, motivation, and perceived institutional support.
In contrast, practice scores showed significant differences between the two groups. FETP-trained officers had higher overall practice scores (65.3 ± 17.8) compared to non-trained officers (57.2 ± 13.9), with the difference being statistically significant (p = 0.020). Significant differences were also observed in specific practice components, including participation in surveillance activities (p = 0.040), data quality practices (p = 0.040), and data analysis and reporting activities (p = 0.030). However, differences in routine reporting practices, such as the use of DHIS2 and submission of weekly reports, were not statistically significant (Table 2).
Factors associated with knowledge
In multivariate analysis, FETP training was the strongest predictor of higher knowledge scores (β=8.24, 95% CI: 4.12-12.36, p<0.001). Bachelor’s degree-level education (β=5.67, p=0.009) and having ≥6 years of work experience (β=4.23, p=0.049) were also independently associated with higher knowledge. Age, sex, region, and other public health training were not significant predictors. The model explained 31.2% of the variance in knowledge scores (Table 3).
Factors associated with attitude score
FETP training remained a significant predictor of positive attitudes (β=6.78, 95% CI: 3.12-10.44, p<0.001), even after adjusting for knowledge and other factors. Higher knowledge scores were also associated with more positive attitudes (β=1.23 per 10% increase, p=0.002). Perceived institutional support was strongly associated with attitudes (β=2.67, p<0.001). Notably, working in CRR was associated with lower attitude scores compared to WHR2 (β=-4.23, p=0.049). The model explained 28.4% of the variance (Table 4).
Factors associated with practice score
The final model, examining factors associated with practice scores, explained 45.2% of the variance. FETP training remained a significant independent predictor (β=7.89, 95% CI: 3.45-12.33, p<0.001). Both knowledge (β=2.34 per 10% increase, p<0.001) and attitude scores (β=1.89 per 10% increase, p=0.002) were also independently associated with better practices. Additional significant predictors included: age ≥35 years (β=4.56, p=0.015), bachelor’s degree education (β=5.34, p=0.005), ≥6 years’ experience (β=4.89, p=0.009), working in LRR (β=6.78, p=0.015) or NBER (β=7.12, p=0.023) compared to WHR2, frequent use of surveillance tools (β=4.23, p<0.001), and having conducted data analysis in the past 6 months (β=8.45, p<0.001) (Table 5).
This study provides a comprehensive evaluation of surveillance-related knowledge, attitudes, and practices among public health officers in The Gambia. The findings demonstrate that FETP training is the strongest independent predictor of improved knowledge, attitudes, and practices. While knowledge and attitudes were generally high, a substantial gap between these domains and actual practice was observed. In addition, the uneven geographical distribution of trained personnel highlights disparities in workforce capacity. These findings underscore both the effectiveness of FETP in building individual competencies and the need for system-level interventions to translate these gains into consistent surveillance performance.
The significant differences in age and experience between FETP-trained and non-trained officers reflect the program’s selection criteria, which appropriately prioritise more experienced officers who can apply their skills upon return to service. However, the uneven geographical distribution of trained personnel observed in this study further differentiates The Gambia’s experience from countries that have institutionalised district-level placement of trained epidemiologists. Previous analyses indicate that equitable deployment of FETP graduates is critical for maximising program impact on surveillance performance and outbreak response [13,21]. Districts without trained personnel remain vulnerable to delayed detection and response, potentially undermining national health security. This finding underscores the importance of strategic workforce planning alongside training expansion.
Consistent with the program’s experiential “learning-by-doing” model, FETP-trained officers exhibited significantly higher knowledge scores compared with their non-trained counterparts. This finding aligns with evaluations from Ethiopia, the Eastern Mediterranean Region, and other low- and middle-income settings, where FETP participation has been shown to improve understanding of surveillance principles, outbreak investigation steps, and data use for decision-making [12,17]. The strong independent association observed after multivariate adjustment suggests that FETP training contributes to knowledge gains beyond what can be explained by education level or years of experience alone.
The itemized knowledge assessment revealed specific gaps requiring attention. Low recognition of maternal death as a notifiable condition (55.8%) is concerning, given that maternal mortality surveillance is a key component of IDSR. Similarly, only half of the respondents correctly identified early warning system functions, suggesting a need for curriculum reinforcement in these areas.
Attitude scores were generally high, but the multivariate analysis revealed important predictors. The strong association between knowledge and attitudes suggests that competence builds confidence; officers who understand surveillance principles are more likely to value and feel motivated to perform surveillance functions.
Perceived institutional support emerged as a critical factor. Officers who felt their facilities supported surveillance activities had significantly more positive attitudes. This finding underscores that individual motivation is shaped by the work environment, a concept supported by previous research on health worker performance [22]. The lower attitude scores in CRR compared to WHR2 may reflect regional disparities in supervisory support or resource allocation, highlighting the need for equitable system-level investments.
The fact that FETP training remained significant after controlling perceived support suggests that the program also fosters intrinsic motivation and professional identity, which are essential but often under-measured outcomes of workforce development programs [13].
The substantial gap between knowledge/attitude scores and practice scores is the study’s most striking finding. While officers know what to do and are motivated to do it, they face barriers to translating this into action. This pattern mirrors findings from other KAP studies among public health workers and reflects persistent challenges in health system performance [17].
The multivariable model for practice scores illuminates this gap. Beyond FETP training, knowledge, and attitudes, practical factors like using surveillance tools and conducting data analysis were strong predictors of overall practice. This suggests that practice improves with regular engagement, those who use the tools become more proficient. This “learning-by-doing” effect reinforces the value of FETP’s core methodology.
Regional variations in practice scores are noteworthy. Officers in LRR and NBER had significantly higher practice scores than those in WHR2, despite having similar or lower knowledge scores. This may reflect the “learning-by-doing” effect in rural areas where officers may have more autonomous responsibility for surveillance functions. Alternatively, it could indicate that WHR2 officers face greater systemic barriers, such as higher workload or competing priorities in more urbanised settings.
Several system-level factors may explain the overall knowledge-practice gap, including limited availability of surveillance tools, weak supportive supervision, high workload, and logistical constraints at district and facility levels. Prior research has shown that training alone is insufficient to sustain high-quality surveillance practices without parallel investments in infrastructure, mentorship, and organisational support [22,4]. The moderate practice scores observed in this study underscore the need to complement FETP training with broader health system strengthening interventions.
The observed knowledge–practice gap highlights the need for targeted system-level interventions to translate competency into consistent performance. Addressing this gap will require strengthening supportive supervision mechanisms, including routine mentorship, on-the-job coaching, and structured feedback systems to reinforce the application of surveillance skills. Ensuring the consistent availability of essential surveillance tools, such as reporting forms, digital platforms, and data analysis resources, is equally critical to enabling effective practice. In addition, institutionalizing periodic refresher training and continuous professional development programs can help sustain knowledge and reinforce practical skills over time.
Equally important is the strategic and equitable deployment of FETP-trained personnel. Prioritising placement in underserved rural districts and identified “red zones” would help reduce disparities in surveillance capacity and improve early detection and response to public health threats. Establishing minimum staffing benchmarks, such as at least one trained surveillance officer per district, alongside data-driven workforce planning, could further enhance national coverage. Together, these measures would ensure that investments in training translate into measurable improvements in surveillance performance and health system resilience.
Key strengths include the robust multistage sampling, inclusion of a comparison group, itemised KAP assessment identifying specific gaps, and multivariate models that identify independent predictors while controlling confounders. The three-model approach, examining knowledge, then attitude (including knowledge), then practice (including both), provides insight into the causal pathway through which FETP may influence performance.
However, limitations exist. The cross-sectional design precludes causal inference. Reliance on self-reported KAP measures is susceptible to social desirability bias, which may have overestimated actual practice [23]. The moderate sample size, while adequately powered for the main analyses, limits detection of small effect sizes in some subgroup analyses. Finally, the study did not directly observe the quality of outbreak investigations or measure actual surveillance performance data, such as timeliness or completeness of reporting.
FETP training in The Gambia is independently associated with higher knowledge, more positive attitudes, and better disease surveillance practices among public health officers. The program appears effective in strengthening individual capacity and professional orientation toward surveillance, moderate practice scores and uneven distribution of trained personnel highlight persistent system-level challenges. Expanding FETP coverage, ensuring equitable placement of trained officers, and strengthening supportive supervision and infrastructure are essential to fully translate training gains into improved surveillance performance and national health security.
To maximize the program’s impact on national health security, we recommend:
What is already known about the topic
What this study adds
| Characteristic | Total n (%) | FETP-Trained n (%) | Non-Trained n (%) | p-value |
|---|---|---|---|---|
| Sex | 0.070 | |||
| Female | 41 (31.8) | 6 (14.6) | 35 (85.4) | |
| Male | 88 (68.2) | 26 (29.5) | 62 (70.5) | |
| Education Level | 0.310 | |||
| Bachelor’s Degree | 43 (33.3) | 13 (30.2) | 30 (69.8) | |
| Diploma | 86 (66.7) | 19 (22.1) | 67 (77.9) | |
| Work Experience (years) | <0.0001 | |||
| <6 | 66 (51.2) | 4 (6.1) | 62 (93.9) | |
| 6–10 | 40 (31.0) | 19 (47.5) | 21 (52.5) | |
| >10 | 23 (17.8) | 9 (39.1) | 14 (60.9) | |
| Age (years) | 0.023 | |||
| <25 | 13 (10.1) | 0 (0.0) | 13 (100.0) | |
| 25–29 | 39 (30.2) | 8 (20.5) | 31 (79.5) | |
| 30–34 | 49 (38.0) | 12 (24.5) | 37 (75.5) | |
| ≥35 | 28 (21.7) | 12 (42.9) | 16 (57.1) | |
| Region | 0.018 | |||
| CRR | 31 (24.0) | 6 (19.4) | 25 (80.6) | |
| LRR | 19 (14.7) | 9 (47.4) | 10 (52.6) | |
| NBER | 11 (8.5) | 5 (45.5) | 6 (54.5) | |
| WHR2 | 68 (52.7) | 12 (17.6) | 56 (82.4) |
| Domain / Indicator | Score Range | FETP-Trained (n = 32) Mean (SD) | Non-Trained (n = 97) Mean (SD) | p-value |
|---|---|---|---|---|
| Knowledge | ||||
| Overall knowledge score | 0–100% | 89.3 (11.4) | 81.6 (15.0) | 0.040 |
| Core surveillance functions | 0–8 | 6.8 (1.2) | 6.0 (1.9) | 0.030 |
| Knowledge of immediately notifiable diseases | 0–7 | 5.7 (1.3) | 4.9 (1.7) | 0.020 |
| Knowledge of reporting frequency requirements | 0–1 | 0.94 (0.24) | 0.86 (0.35) | 0.210 |
| Attitude | ||||
| Overall attitude score | 0–100% | 96.9 (4.8) | 89.8 (12.4) | 0.420 |
| Positive perception of surveillance importance | 1–2 | 2.0 (0.0) | 2.0 (0.2) | 0.560 |
| Confidence in detecting and reporting diseases | 1–2 | 1.9 (0.3) | 1.8 (0.4) | 0.180 |
| Motivation for routine surveillance reporting | 1–2 | 1.9 (0.3) | 1.9 (0.3) | 0.340 |
| Perceived institutional support for surveillance | 1–2 | 1.9 (0.3) | 1.7 (0.5) | 0.090 |
| Practice | ||||
| Overall practice score | 0–100% | 65.3 (17.8) | 57.2 (13.9) | 0.020 |
| Public health surveillance activities | 0–8 | 5.4 (2.0) | 4.6 (2.1) | 0.040 |
| Use of DHIS2 for reporting | 0–1 | 0.78 (0.42) | 0.69 (0.46) | 0.320 |
| Submission of weekly surveillance reports | 0–1 | 0.81 (0.40) | 0.72 (0.45) | 0.290 |
| Data quality practices (composite) | 0–100% | 70.2 (16.5) | 63.1 (19.0) | 0.040 |
| Data analysis and reporting activities | 0–100% | 68.5 (15.2) | 60.8 (17.1) | 0.030 |
| Variable | Adjusted Mean Difference β (95% CI) | p-value |
|---|---|---|
| Had FETP Training | ||
| Yes vs No | 8.24 (4.12 – 12.36) | <0.001 |
| Age | ||
| ≥35 vs <35 years | 3.45 (-0.89 – 7.79) | 0.118 |
| Sex | ||
| Male vs Female | 1.98 (-2.34 – 6.30) | 0.367 |
| Education Level | ||
| Bachelor’s vs Diploma | 5.67 (1.45 – 9.89) | 0.009 |
| Work Experience | ||
| ≥6 vs <6 years | 4.23 (0.01 – 8.45) | 0.049 |
| Region | ||
| CRR vs WHR2 | -2.15 (-7.01 – 2.71) | 0.382 |
| LRR vs WHR2 | 3.89 (-1.89 – 9.67) | 0.186 |
| NBER vs WHR2 | 4.12 (-2.34 – 10.58) | 0.210 |
| Had Other Public Health Training | ||
| Yes vs No | 2.45 (-5.67 – 10.57) | 0.552 |
| Constant | ||
| — | 72.34 (65.21 – 79.47) | <0.001 |
| Dependent Variable: Knowledge Score (%). Bold values indicate statistical significance (p < 0.05). β = unstandardized regression coefficient; CI = confidence interval. | ||
| Variable | Adjusted Mean Difference β (95% CI) | p-value |
|---|---|---|
| Had FETP Training | ||
| Yes vs No | 6.78 (3.12 – 10.44) | <0.001 |
| Knowledge Score | ||
| Per 10% increase | 1.23 (0.45 – 2.01) | 0.002 |
| Age | ||
| ≥35 vs <35 years | 2.34 (-1.45 – 6.13) | 0.224 |
| Sex | ||
| Male vs Female | 1.12 (-2.34 – 4.58) | 0.523 |
| Education Level | ||
| Bachelor’s vs Diploma | 2.89 (-0.78 – 6.56) | 0.122 |
| Work Experience | ||
| ≥6 vs <6 years | 3.45 (-0.23 – 7.13) | 0.066 |
| Region | ||
| CRR vs WHR2 | -4.23 (-8.45 – -0.01) | 0.049 |
| LRR vs WHR2 | 2.15 (-2.71 – 7.01) | 0.382 |
| NBER vs WHR2 | 3.45 (-2.34 – 9.24) | 0.241 |
| Perceived Institutional Support | ||
| Per 1-point increase | 2.67 (1.34 – 4.00) | <0.001 |
| Constant | ||
| — | 68.23 (58.34 – 78.12) | <0.001 |
| Dependent Variable: Attitude Score (%). Bold values indicate statistical significance (p < 0.05). β = unstandardized regression coefficient; CI = confidence interval. | ||
| Variable | Adjusted Mean Difference β (95% CI) | p-value |
|---|---|---|
| Had FETP Training | ||
| Yes vs No | 7.89 (3.45 – 12.33) | <0.001 |
| Knowledge Score | ||
| Per 10% increase | 2.34 (1.12 – 3.56) | <0.001 |
| Attitude Score | ||
| Per 10% increase | 1.89 (0.67 – 3.11) | 0.002 |
| Age | ||
| ≥35 vs <35 years | 4.56 (0.89 – 8.23) | 0.015 |
| Sex | ||
| Male vs Female | 3.21 (0.45 – 6.87) | 0.085 |
| Education Level | ||
| Bachelor’s vs Diploma | 5.34 (1.67 – 9.01) | 0.005 |
| Work Experience | ||
| ≥6 vs <6 years | 4.89 (1.23 – 8.55) | 0.009 |
| Region | ||
| CRR vs WHR2 | -3.45 (-7.89 – 0.99) | 0.127 |
| LRR vs WHR2 | 6.78 (1.34 – 12.22) | 0.015 |
| NBER vs WHR2 | 7.12 (1.01 – 13.23) | 0.023 |
| Use of Surveillance Tools | ||
| Per 1-point increase | 4.23 (2.89 – 5.57) | <0.001 |
| Had Conducted Data Analysis | ||
| Yes vs No | 8.45 (4.89 – 12.01) | <0.001 |
| Dependent Variable: Practice Score (%). Model R² = 0.452. Bold values indicate statistical significance (p < 0.05). β = unstandardized regression coefficient; CI = confidence interval. | ||