Research![]() | Volume 8, Article 18, 08 Apr 2025
| Volume 8, Article 18, 08 Apr 2025
Lamya Abdo Al Aroomi1, Labiba Saeed Anam1, Mutahar Ahmed AL Qassimi2, Faten Hamid Ezzadeen2
1Yemen Field Epidemiology Training Program (YFETP), Ministry of Public Health and Population, Sana’a, Yemen, 2AFP Surveillance Program, Ministry of Public Health and Population, Sana’a, Yemen
&Corresponding author: Lamya Abdo Al Aroomi, Yemen Field Epidemiology Training Program, Ministry of Public Health and Population, Sana’a, Yemen, Email Address: drlamyaalaroomi@gmail.com
Received: 13 Dec 2024, Accepted: 04 Mar 2025, Published: 08 Apr 2025
Domain: Vaccine Preventable Diseases, Child Health, Polio Elimination
Keywords: Acute Flaccid Paralysis (AFP), Surveillance, Analysis, Sana’a City, Yemen
©Lamya Abdo Al Aroomi et al Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Lamya Abdo Al Aroomi et al Acute Flaccid Paralysis Surveillance Data Analysis, Sana’a City, Yemen, 2012-2021: A retrospective descriptive analysis. Journal of Interventional Epidemiology and Public Health. 2025;8:18. https://doi.org/10.37432/jieph-d-24-02043
Background: WHO certified Yemen polio-free in 2009. Outbreaks of circulating Vaccine Derived Polioviruses (cVDPV) threaten the eventual eradication of all polioviruses. In Yemen, two outbreaks of cVDPV type 1 and 2 were reported in 2020 and 2021-2022, respectively. This study aimed to describe trends and characteristics of AFP cases in Sanaa city over the last ten years, from 2012 to 2021.
Methods: This cross-sectional study involved retrospective descriptive analysis of surveillance data. All AFP cases reported to the AFP Surveillance System at the Ministry of Public Health and Population between January 2012 and December 2021 were included.
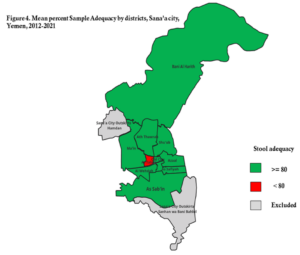
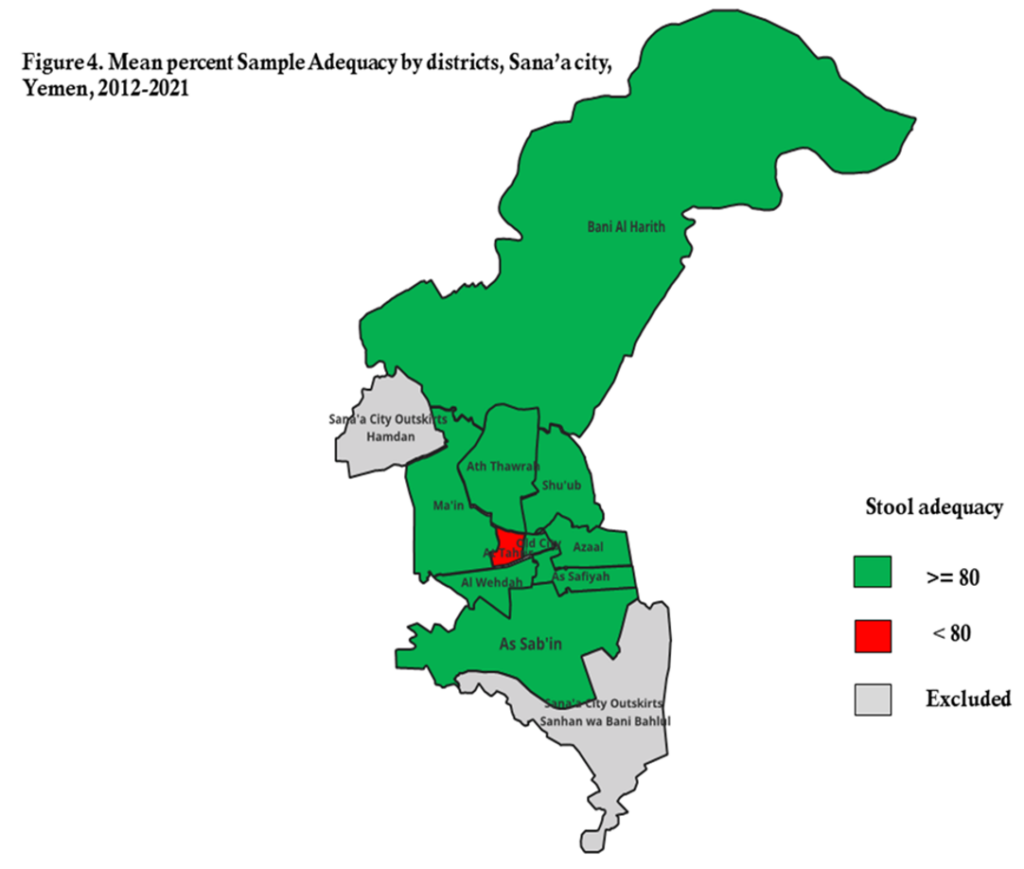
Results: During the ten years’ period, a total of 593 cases of AFP were reported in Sana’a City; none of which was confirmed as poliomyelitis. 56% of AFP cases were males, and 60% aged five years or younger. More than half (61%) of cases had received 4 doses or more of OPV. The predominant clinical feature was fever (79%). Paralysis progressed within 3 days of onset in 437 (74%) cases, which was asymmetrical in 202 (34%) cases. The annual incidence of non-polio AFP ranged from 2.6/100,000 to 4.9/100,000 (mean: 3.5/100,000), which met the WHO target. Regarding sample adequacy, we found that in 2017, the sample adequacy fell short of the expected minimal (80%) level, though all districts met the WHO target (>80%) except in At Tahrir District (77%).
Conclusions: The AFP surveillance system has improved over the past 10 years in Sana’a city. However, strengthening the two main indicators of AFP surveillance, especially sample adequacy, is recommended. It is advisable to establish a national laboratory that adheres to WHO-recommended procedures for detecting polioviruses in stool samples. Because zero doses were reported among 12% of AFP cases, maintaining high coverage through routine immunization and supporting supplementary immunization activities is crucial to ensure that most children are vaccinated, thereby contributing to the eradication of polio.
Poliomyelitis is one of the vaccine-preventable diseases caused by a virus. It invades the nervous system and can cause total paralysis in a matter of hours [1] WHO. Poliomyelitis [Internet]. Geneva (Switzerland): World Health Organization; 2025 Apr 2 [cited 2025 Apr 7]; [about 8 screens]. Available from: https://www.who.int/news-room/fact-sheets/detail/poliomyelitis.
. Polio cases caused by either wild poliovirus (WPV) or circulating vaccine-derived poliovirus (cVDPV) are detected through surveillance for acute flaccid paralysis (AFP) and subsequent stool specimen testing at World Health Organization (WHO)-accredited laboratories in the Global Polio Laboratory Network [2]
Morales M. Progress toward polio eradication – worldwide, 2015–2016. MMWR Morb Mortal Wkly Rep [Internet]. 2016 May 13 [cited 2025 Apr 7]; 65(18):470–473. Available from: https://www.cdc.gov/mmwr/volumes/65/wr/mm6518a4.htm http://dx.doi.org/10.15585/mmwr.mm6518a4 Erratum in: Progress toward polio eradication — worldwide, 2015–2016. MMWR Morb Mortal Wkly Rep [Internet]. 2016 May 20 [cited 2025 Apr 7 ]; 65(19): 502. Available from: https://www.cdc.gov/mmwr/volumes/65/wr/mm6519a6.htm http://dx.doi.org/10.15585/mmwr.mm6519a6
. As a part of the worldwide campaign to eradicate polio, all countries do surveillance for polio by looking for clinical cases of AFP [3]
Simeonova I, Petrova Sv, Mladenova I. Acute flaccid paralysis registered for the period 2012-2020, in Stara Zagora Region. TJS [Internet]. 2021 June [cited 2025 Apr 7];19(2):152–5. Available from: http://tru.uni-sz.bg/tsj/Volume%2019,%202021,%20Number%202,%20Series%20Biomedical%20Sciences/7.pdf http://dx.doi.org/10.15547/tjs.2021.02.007 Download PDF to view full text.
An effective AFP surveillance system is essential to the broader effort to eradicate polio. AFP is mainly seen in children below 15 years of age. Accordingly, the goal of AFP surveillance is to detect, report, and investigate all AFP cases so that poliomyelitis can be ruled out as the cause of the paralysis. [4]
Amodan BO, Kisakye A, Okumu PT, Ahirirwe SR, Kadobera D, Driwale A, Ario AR. Trends of key surveillance performance indicators of acute flaccid paralysis: a descriptive analysis, Uganda, 2015–2020. BMC Public Health [Internet]. 2022 Sep 7 [cited 2025 Apr 7];22(1):1694. Available from: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-022-14077-w https://doi.org/10.1186/s12889-022-14077-w
,[5]
WHO Regional Office for the Meditteranean Region. Polio Eradication Initiative [Internet]. Nasr City (EG): WHO Regional Office for the Meditteranean Region; c2025 [cited 2025 Apr 7]; [about 8 screeens]. Available from: https://www.emro.who.int/polio-eradication/about-eradication/surveillance.html
.
Cases due to wild poliovirus have decreased by over 99% since 1988, from an estimated 350,000 cases in more than 125 endemic countries to just two endemic countries (as of October 2023) [1]
WHO. Poliomyelitis [Internet]. Geneva (Switzerland): World Health Organization; 2025 Apr 2 [cited 2025 Apr 7]; [about 8 screens]. Available from: https://www.who.int/news-room/fact-sheets/detail/poliomyelitis.
. The world has eradicated two of the three wild poliovirus strains, leaving only wild poliovirus type 1 still in circulation. In addition to stopping the wild virus, to achieve eradication, the world needs to end outbreaks of cVDPV (a non-wild variant of the virus that can emerge in under-immunized communities) that are currently spreading in parts of the world [6]
GPEI. polio today [Internet]. polio eradication.org; 2024 September 1. Available from: https://polioeradication.org/wp-content/uploads/2022/03/GPEI-General-Factsheet-20220330.pdf.
. In 2022, endemic wild poliovirus type 1 remains in two countries: Pakistan and Afghanistan [7]
WHO. Poliomyelitis (polio) [Internet]. Geneva (CH): WHO; c2025 [cited 2025 Apr 7]; [about 2 screens]. Available from: https://www.who.int/health-topics/poliomyelitis#tab=tab_1
.
At the national level, an outbreak of vaccine-derived poliovirus type 1 (cVDPV1) was reported in 2020 despite Yemen was certified free of polio since 2009 [8]
Al-Qassimi MA, Al Amad M, Al-Dar A, Al Sakaf E, Al Hadad A, Raja’a YA. Circulating vaccine derived polio virus type 2 outbreak and response in Yemen, 2021–2022, a retrospective descriptive analysis. BMC Infect Dis [Internet]. 2024 Mar 15 [cited 2025 Apr 7];24(1):321. Available from: https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-024-09215-1 https://doi.org/10.1186/s12879-024-09215-1. In late 2021 and 2022, cases of paralytic polio caused by vaccine-derived poliovirus type 2 were also detected [9]
Almoayed KA, Bin Break A, Al-Qassimi M, Assabri A, Khader Y. The acute flaccid paralysis (Afp) surveillance system in yemen, 2010-2015: descriptive study based on secondary data analysis. JMIR Public Health Surveill [Internet]. 2019 Dec 6 [cited 2025 Apr 7];5(4):e14413. Available from: http://publichealth.jmir.org/2019/4/e14413/ https://doi.org/10.2196/14413
. The marked negative impact of the 2015 war on immunization coverage could put Yemen at more risk of emergence and circulation of VDPV outbreaks [10]
Torbosh A, Al Amad MA, Al Serouri A, Khader Y. The impact of war in yemen on immunization coverage of children under one year of age: descriptive study. JMIR Public Health Surveill [Internet]. 2019 Oct 23 [cited 2025 Apr 7];5(4):e14461. Available from: http://publichealth.jmir.org/2019/4/e14461/ https://doi.org/10.2196/14461
. The health system infrastructure is mostly destroyed, routine immunization (RI) coverage is low, and significant numbers of vaccine-preventable disease outbreaks such as diphtheria and measles are reported [8] Al-Qassimi MA, Al Amad M, Al-Dar A, Al Sakaf E, Al Hadad A, Raja’a YA. Circulating vaccine derived polio virus type 2 outbreak and response in Yemen, 2021–2022, a retrospective descriptive analysis. BMC Infect Dis [Internet]. 2024 Mar 15 [cited 2025 Apr 7];24(1):321. Available from: https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-024-09215-1 https://doi.org/10.1186/s12879-024-09215-1
. This has led to a drop in vaccination rates and the re-emergence of cVDPV1 in 2020 and cVDPV2 in 2021 and 2022. Data from this analysis may contribute to a broader understanding of outbreak vulnerabilities in Sana’a city. In recent years, the number of reported AFP cases has reached high level. No previous studies have investigated the different aspects of AFP cases in Sana’a City, so this study aimed to describe trends in the incidence of AFP cases and the characteristics of these cases in Sanaa City over the last ten years from 2012 to 2021.
Description of AFP Surveillance system in Yemen
The AFP surveillance system was established in Yemen in 1998 [9] Almoayed KA, Bin Break A, Al-Qassimi M, Assabri A, Khader Y. The acute flaccid paralysis (Afp) surveillance system in yemen, 2010-2015: descriptive study based on secondary data analysis. JMIR Public Health Surveill [Internet]. 2019 Dec 6 [cited 2025 Apr 7];5(4):e14413. Available from: http://publichealth.jmir.org/2019/4/e14413/ https://doi.org/10.2196/14413
. The primary goals of the program include the early identification and examination of any AFP cases, assessment of the performance of the AFP Surveillance program using a customized local version of the standard WHO indicators, and confirming that Yemen remains polio-free [11]
Al-Dubaiee R, Al Qassimi M, Al-Dar A, Al Serouri A, Khader Y. Impact of the protracted war in yemen on the acute flaccid paralysis surveillance system: retrospective descriptive analysis. JMIR Public Health Surveill [Internet]. 2021 May 19 [cited 2025 Apr 7];7(5):e27638. Available from: https://publichealth.jmir.org/2021/5/e27638 https://doi.org/10.2196/27638
. The process for AFP surveillance begins with community informants or designated focal points in healthcare facilities reporting every case and submitting weekly updates, including reports where no cases have been found. District and governorate coordinators are tasked with collecting, analyzing, verifying, investigating, and ensuring the collection of stool samples from suspected cases. National-level surveillance activities comprise the verification, investigation, analysis, and coordination with the Expanded Program of Immunization (EPI) to implement necessary actions.
Since Yemen had no national polio lab, AFP specimens are sent abroad to accredited WHO-referral polio labs. During the ten years’ period, AFP samples were shipped out of Yemen either to the Polio KEMRI in Nairobi, Kenya or Oman’s National Polio Lab in Muscat (ONPL), Oman, and NAMRU-3 laboratory in Egypt. Meanwhile, plans are underway to improve Yemen’s laboratory testing capacity, that considered one of the foundations of a strong polio surveillance system [12]
12. WHO Eastern Meditteranean Region. Polio Eradication Initiative: Yemen [Internet]. Nasr City (EG): WHO Eastern Meditteranean Region; c2025 [cited 2025 Apr 7]: [about 5 screeens]. Available from: https://www.emro.who.int/polio-eradication/priority-countries/yemen.html
. Stool samples from all AFP cases were recently sent to ONPL in Oman. WHO-accredited polio lab results are used to determine the final classification of AFP cases.
Study design
A descriptive cross-sectional study involving retrospective secondary data analysis on AFP cases from Sanaa city, reported to the AFP surveillance office database at the Ministry of Public Health and Population (MoPHP) during the period from 2012 to 2021 inclusive.
Study setting
Sana’a is the capital of the Republic of Yemen and is divided into 10 administrative districts. According to EPI, the estimated number of children under 15 years of age at Sanaa city in 2021 was 1,976,355. As- Sab’in and Ma’in districts were the most populous, with 495,340 and 302,768 children under 15 years, respectively.
Study population
The study included all cases recorded based on the AFP standard case definition, which was maintained in the database at the national AFP surveillance office at MoPHP from 2012 to 2021. The WHO standard AFP case definition used was: “Any child under 15 years of age with AFP or any person of any age with paralytic illness if polio is suspected [13]
WHO Regional Office for South- East Asia. Surveillance Guide for Vaccine-Preventable Diseases in the WHO South-East Asia Region [Internet]. Geneva (CH): WHO Regional Office for South- East Asia; September 2017 [cited 2025 Apr 7]. Available from: https://iris.who.int/handle/10665/277459 Download PDFs to view full text
.
Data variables
The recorded sociodemographic factors included age, sex, district, vaccination history, year of onset, and clinical symptoms such as the presence of fever, paralysis progression, symmetry. Two important indicators were assessed based on WHO targets: Non-polio AFP rate and stool adequacy. Laboratory results from the testing of stool samples of AFP cases were included.
Definitions
Non-polio acute flaccid paralysis rate: According to the guidelines, the system should detect at least 2 AFP cases per 100,000 children under 15 years.
Stool adequacy: Defined as two stool specimens collected from an AFP case at least 24 hours apart and within 14 days of the onset of paralysis, and arriving at the laboratory in good condition. Adequate stool samples must be detected among at least 80% of all AFP cases.
The final classification of AFP cases
Once laboratory results have been received, all AFP cases undergo final case classification. AFP cases with adequate stool specimens are either discarded as non-polio AFP if no WPV or VDPV was found, or confirmed as polio if WPV or VDPV was found[14]
WHO. Global guidance for conducting acute flaccid paralysis (AFP) surveillance in the context of poliovirus eradication [Internet]. Geneva (CH): WHO; 2024 [cited 2025 Apr 7]; 104p. Available from: https://iris.who.int/handle/10665/376603 Download PDF to view full text
. If stool specimens are inadequate, final classification of the AFP case depends on the results of 60-day follow-up examination. If the 60-day follow-up examination shows no residual weakness, the case is classified as non-polio AFP. If the AFP case has residual paralysis, died or is lost to follow-up, it must be reviewed and classified by the National Polio Expert Committee (NPEC) [15]
WHO Regional Office for South- East Asia. Surveillance Guide for Vaccine-Preventable Diseases in the WHO South-East Asia Region: Module 3 [Internet]. Geneva (CH): WHO Regional Office for South- East Asia; September 2017 [cited 2025 Apr 7]. Available from: https://iris.who.int/bitstream/handle/10665/277459/Module3-Polio.pdf?sequence=9 Download PDF to view full text
.
Data analysis
The national AFP surveillance program data was thoroughly reviewed and verified, ensuring that the data is both complete and consistent through regular checks. After checking the data for completeness, Excel and Epi Info version 7.2 were used to generate a descriptive analysis of sociodemographic factors and clinical history. The main indicators were evaluated using the WHO-recommended surveillance standard [13]
WHO Regional Office for South- East Asia. Surveillance Guide for Vaccine-Preventable Diseases in the WHO South-East Asia Region [Internet]. Geneva (CH): WHO Regional Office for South- East Asia; September 2017 [cited 2025 Apr 7]. Available from: https://iris.who.int/handle/10665/277459 Download PDFs to view full text
. The population statistics utilized for the calculation of the rates were sourced from the EPI. A table was generated to display the frequencies of sociodemographic, clinical characteristics of AFP cases and final laboratory results of stool specimens. Graphs and maps were used to visualize vaccination status by districts and the performance of surveillance indicators by time and place.
Ethical consideration
The data extraction and ethical study direction were approved by the administration of the diseases control and surveillance and national AFP surveillance at MoPHP. Formal ethical approval was not sought because secondary data analysis of surveillance databases is considered a routine public health activity and one of the expected deliverables that must be accomplished by Yemen Field Epidemiology Training Program trainees. We ensured the confidentiality of patients by employing coded identifiers.
Over the ten years, a total of 593 AFP cases (an average of 59.3 cases per year) were reported. None of the AFP cases were confirmed as poliomyelitis. The highest number of reported cases occurred in 2021, accounting for 15% of the total (Table 2). Of the AFP cases, 334 (56%) were male, and 353 (60%) of the cases involved children aged 5 years or younger. Fever at the onset of paralysis was reported in 469 (79%) of the AFP cases, and paralysis progressed within 3 days of onset in 437 (74%) cases. Asymmetrical paralysis was observed in 202 (34%) of the cases. More than half of the AFP cases (61%) had received the recommended three or more doses of the oral polio vaccine (OPV), while 12% had not received any doses of OPV. The highest zero dose percent was reported in 2020 (Table 1).
AFP surveillance Performance
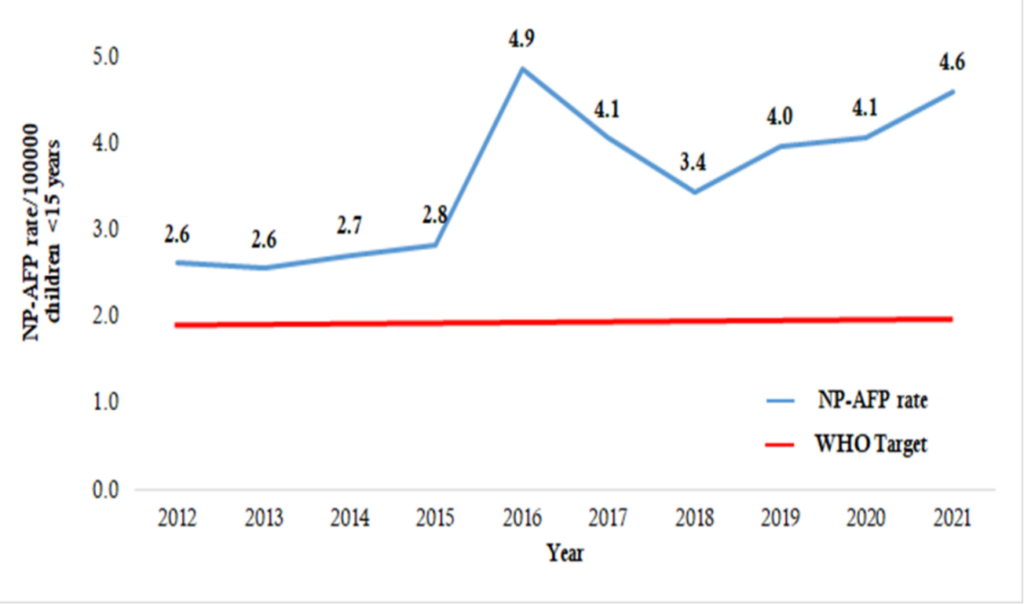
Annual NP-AFP rate: A steady increase in the NP-AFP rate was observed from 2012 to 2015, reaching its peak in 2016. The rate then decreased in 2018 to 3.4/100,000, but increased again from 2019 to 2021. Over the ten years, the non-polio AFP rate met the WHO minimum target of ≥ 2 cases per 100,000 children under 15 years, with an average rate of 3.5 /100,000. (Figure 1)
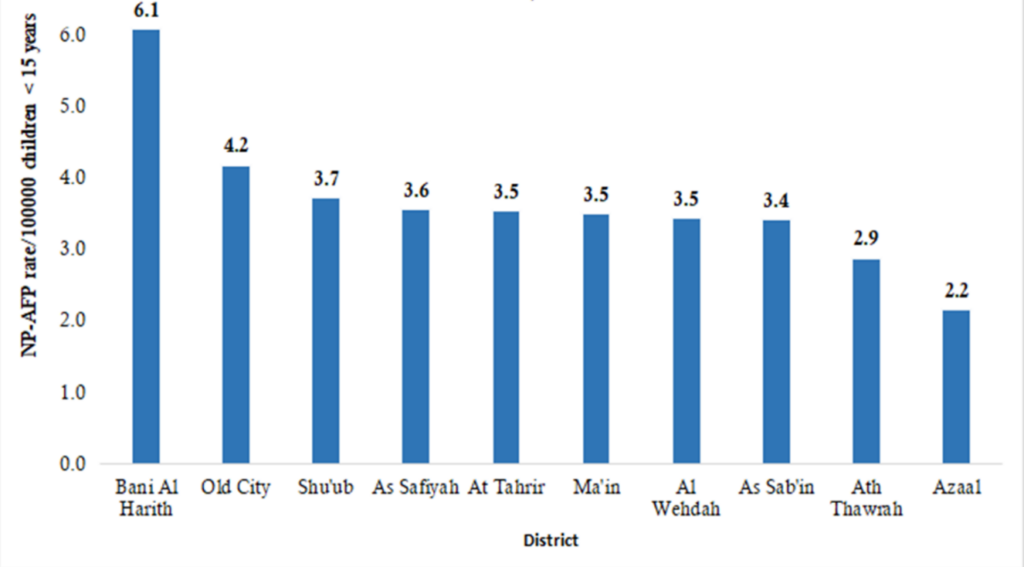
NP-AFP rate by district: The overall mean NP-AFP rate performance was achieved across all districts, with all districts maintaining a rate above the target level. The mean NP- AFP detection rate varied between districts, but all met the WHO standard level of ≥ 2 AFP cases per 100,000 children under 15 years of age over the ten – year period. The highest rates were detected in Bani AL- Harith and the Old City of Sana’a, while Azzal had the lowest rate. (Figure 2)
Stool Adequacy by year: With the exception of 2017, when only 74.6% of samples were sufficient, sample adequacy across the ten years exceeded the WHO minimum requirement of ≥ 80% (Table 2).
Stool Adequacy by district: With the exception of At-Tahrir district, where the stool adequacy rate was 77%, below the minimum aim of 80%, other districts had stool adequacy rates that met or exceeded the minimum target. (Figure 4)
Vaccination status by district
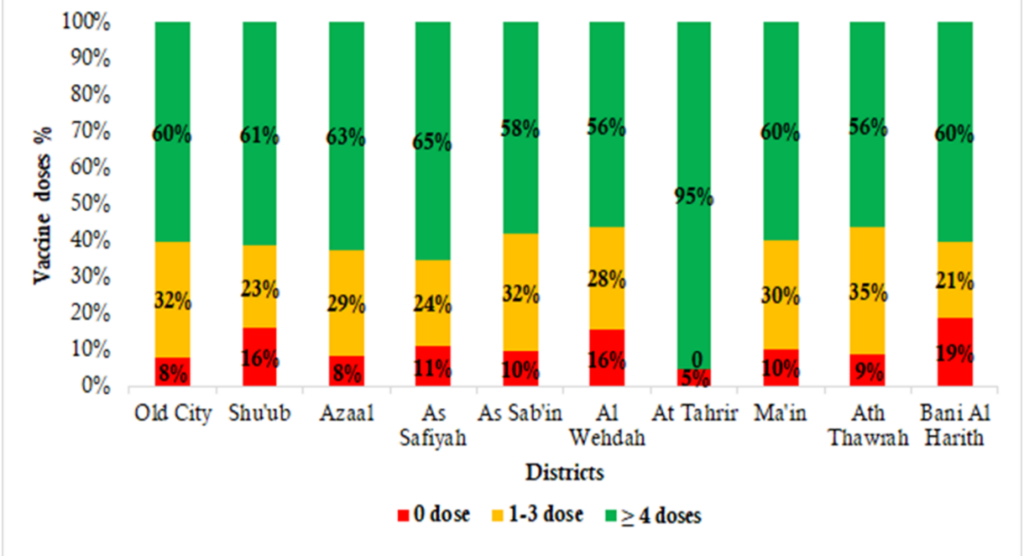
The vaccination status as 61% (362) of AFP cases received ≥ 4 doses of OPV. At Tahrir district showed the higher percentage (95%) of AFP cases who had received ≥ 4 doses of OPV. Of the total AFP cases, 27 % (158) had 1-3 doses and 12% (73) had zero doses (un-immunized). A higher percentage of zero doses was 19% in Bani AL Harith and 16% in Shu’ub and AL Wehdah Districts. (Figure 3)
Laboratory Results of AFP cases from the testing of samples
No virus isolated from 84.3 % of samples collected and tested. Sabin– like polioviruses accounted for 1.7% of the isolates while, 13.3% were non-polio enterovirus. Four cases with inadequate specimens were reviewed and discarded by NPEC. (Table 3)
Yemen was certified polio-free by WHO in 2009, but there is always a high risk of importing WPV from visitors and migrants coming from polio-endemic countries. So a strong surveillance system is important [16]
Abdel-Fattah A, EL-Gilany AH, El-Masry R, Kanddeel A. Acute flaccid paralysis in North East Delta, Egypt: A retrospective analysis of prospectively collected surveillance data. Journal of Infection and Public Health [Internet]. 2019 Apr 13 [version of record 2019 Sep 5: cited 2025 Apr 7];12(5):714–9. Available from: https://linkinghub.elsevier.com/retrieve/pii/S187603411930125X https://doi.org/10.1016/j.jiph.2019.03.016
. We analyzed the AFP surveillance data in Sana’a city from 2012 to 2021, after the new emergence of cVDPV1 in Saadah governorate and cVDPV2 confirmation of outbreak in the country. During the period of 2016, and from 2019 to 2021, the number of AFP cases were high compared to previous years. This is due to persistent efforts during the last years especially after the cVDPV1 that have been reported during 2020 from Saadah governorate. The involvement of pediatricians, clinicians and volunteers trained in community-based surveillance play an important role in increasing the reporting rate.
Our analysis revealed that no polio cases were reported over the last ten years in Sana’a city. This finding agrees with studies conducted in Egypt and Iran [16]
Abdel-Fattah A, EL-Gilany AH, El-Masry R, Kanddeel A. Acute flaccid paralysis in North East Delta, Egypt: A retrospective analysis of prospectively collected surveillance data. Journal of Infection and Public Health [Internet]. 2019 Apr 13 [version of record 2019 Sep 5: cited 2025 Apr 7];12(5):714–9. Available from: https://linkinghub.elsevier.com/retrieve/pii/S187603411930125X https://doi.org/10.1016/j.jiph.2019.03.016
,[17] Momen AA, Shakurnia A, Momen M. Eleven-year surveillance of acute flaccid paralysis in southwestern Iran. Turk J Pediatr [Internet]. 2019 Aug 25 [cited 2025 Apr 7];61(4):544–51. Available from: https://turkjpediatr.org/article/view/733 https://doi.org/10.24953/turkjped.2019.04.011 Download PDF to view Full text
. The demographic variables showed that the AFP cases were slightly higher among males compared to females, which was consistent with many other published studies in Sudan, and Kenya [18]
Tegegne AA, Fiona B, Shebeshi ME, Hailemariam FT, Aregay AK, Beyene B, Asemahgne EW, Woyessa DJ, Woyessa AB. Analysis of acute flaccid paralysis surveillance in Ethiopia, 2005-2015: progress and challenges. Pan Afr Med J [Internet]. 2017 Jun 9 [cited 2025 Apr 7];27(2): 10. Available from: http://www.panafrican-med-journal.com/content/series/27/2/10/full/ https://doi.org/10.11604/pamj.supp.2017.27.2.10694
,[19]
Tesfaye B, Sowe A, Kisangau N, Ogange J, Ntoburi S, Nekar I, Muitherero C, Camara Y, Gathenji C, Langat D, Sergon K, Limo H, Nzunza R, Kiptoon S, Kareko D, Onuekwusi I. An epidemiological analysis of Acute Flaccid Paralysis (Afp) surveillance in Kenya, 2016 to 2018. BMC Infect Dis [Internet]. 2020 Aug 18 [cited 2025 Apr 7];20(1):611. Available from: https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-020-05319-6 https://doi.org/10.1186/s12879-020-05319-6
. Most cases were 5 years old or younger, which was similar to the study findings in Egypt, Jordan, and Syria [16]
Abdel-Fattah A, EL-Gilany AH, El-Masry R, Kanddeel A. Acute flaccid paralysis in North East Delta, Egypt: A retrospective analysis of prospectively collected surveillance data. Journal of Infection and Public Health [Internet]. 2019 Apr 13 [version of record 2019 Sep 5: cited 2025 Apr 7];12(5):714–9. Available from: https://linkinghub.elsevier.com/retrieve/pii/S187603411930125X https://doi.org/10.1016/j.jiph.2019.03.016
,[20]
Zerriouh F, Khader Y, Qasem N, Abusal K, Iblan I, Ghaffari L, Abdallat M. Evaluation of the acute flaccid paralysis surveillance system in polio-free Jordan, 2012-2016: retrospective secondary analysis. JMIR Public Health Surveill [Internet]. 2019 Sep 27 [cited 2025 Apr 7];5(3):e14217. Available from: http://publichealth.jmir.org/2019/3/e14217/ https://doi.org/10.2196/14217
,[21]
Rayes R, Haar RJ, AlMhawish N. Epidemiological analysis of acute flaccid paralysis (Afp) surveillance in conflict-affected syria. BSJ [Internet]. 2022 [cited 2025 Apr 7];26(2): 87-93. Available from: https://escholarship.org/uc/item/2fp2t8fz https://doi.org/10.5070/BS326258287
.
The clinical variables showed that the predominant clinical history was fever at onset of paralysis, which is similar to findings of studies conducted in Egypt and Kenya [16]
Abdel-Fattah A, EL-Gilany AH, El-Masry R, Kanddeel A. Acute flaccid paralysis in North East Delta, Egypt: A retrospective analysis of prospectively collected surveillance data. Journal of Infection and Public Health [Internet]. 2019 Apr 13 [version of record 2019 Sep 5: cited 2025 Apr 7];12(5):714–9. Available from: https://linkinghub.elsevier.com/retrieve/pii/S187603411930125X https://doi.org/10.1016/j.jiph.2019.03.016,[19]
Tesfaye B, Sowe A, Kisangau N, Ogange J, Ntoburi S, Nekar I, Muitherero C, Camara Y, Gathenji C, Langat D, Sergon K, Limo H, Nzunza R, Kiptoon S, Kareko D, Onuekwusi I. An epidemiological analysis of Acute Flaccid Paralysis (Afp) surveillance in Kenya, 2016 to 2018. BMC Infect Dis [Internet]. 2020 Aug 18 [cited 2025 Apr 7];20(1):611. Available from: https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-020-05319-6 https://doi.org/10.1186/s12879-020-05319-6
. Paralysis was asymmetrical in one-third of cases, which was a lower proportion than that found in Ethiopia, Jordan, and Sudan [18]
Tegegne AA, Fiona B, Shebeshi ME, Hailemariam FT, Aregay AK, Beyene B, Asemahgne EW, Woyessa DJ, Woyessa AB. Analysis of acute flaccid paralysis surveillance in Ethiopia, 2005-2015: progress and challenges. Pan Afr Med J [Internet]. 2017 Jun 9 [cited 2025 Apr 7];27(2): 10. Available from: http://www.panafrican-med-journal.com/content/series/27/2/10/full/ https://doi.org/10.11604/pamj.supp.2017.27.2.10694
,[20]
Zerriouh F, Khader Y, Qasem N, Abusal K, Iblan I, Ghaffari L, Abdallat M. Evaluation of the acute flaccid paralysis surveillance system in polio-free Jordan, 2012-2016: retrospective secondary analysis. JMIR Public Health Surveill [Internet]. 2019 Sep 27 [cited 2025 Apr 7];5(3):e14217. Available from: http://publichealth.jmir.org/2019/3/e14217/ https://doi.org/10.2196/14217
,[22]
Tegegne AA, Maleghemi S, Anyuon AN, Zeleke FA, Legge GA, Ferede MA, et al. The sensitivity of acute flaccid paralysis surveillance-the case of South Sudan: retrospective secondary analysis of AFP surveillance data 2014-2019. Pan Afr Med J [Internet]. 2022 Jun 11 [cited 2025 Apr 7];42(1): 12. Available from: https://www.panafrican-med-journal.com/content/series/42/1/12/full/ https://doi.org/10.11604/pamj.supp.2022.42.1.33965. Paralysis progressed within 3 days among nearly two-thirds of cases, which was higher than those from Nigeria [23]
Hamisu AW, Johnson TM. Sensitivity of acute flaccid paralysis surveillance in Nigeria (2006-2015). J Infec Dis Treat [Internet]. 2016 Aug 6 [cited 2025 Apr 7];02(02): 13. Available from: http://infectious-diseases-and-treatment.imedpub.com/sensitivity-of-acute-flaccid-paralysis-surveillance-in-nigeria-20062015.php?aid=9975 http://dx.doi.org/10.21767/2472-1093.100018 Download PDF to view full text
.
The vaccination against polio is one of the most important measures to eradicate polio. Over the study period, more than half of cases had received 4 or more doses of OPV and this was similar to studies conducted in Sudan and Nigeria [22],[24]
Raji IA, Abubakar AU, Ahmad A, Gidado S, Olorukooba AA, Lawal BB, Umeokonkwo CD, Balogun M. Evaluation of acute flaccid paralysis surveillance indicators in Sokoto state, Nigeria, 2012–2019: a secondary data analysis. BMC Public Health [Internet]. 2021 Jun 15 [cited 2025 Apr 7];21(1):1148. Available from: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-021-11238-1 https://doi.org/10.1186/s12889-021-11238-1
. Zero-dose cases were reported in five years, and it did not exceed more than 2 cases per year except in 2020, when six cases were reported due to the impact of COVID-19 pandemic, which made major disruptions in all health services, including EPI. In addition to reviewing and improving routine immunization, every zero-dose AFP case is reported from the surveillance system to EPI, where a team of EPI and surveillance officers evaluates immunization activity and, in certain situations, conducts child vaccinations or mopping-up campaigns.
Regarding the NP-AFP rate by years, it met the WHO recommended minimum standard of 2/ 100,000 for all years. This agrees with studies conducted at the national level [9]
Almoayed KA, Bin Break A, Al-Qassimi M, Assabri A, Khader Y. The acute flaccid paralysis (Afp) surveillance system in yemen, 2010-2015: descriptive study based on secondary data analysis. JMIR Public Health Surveill [Internet]. 2019 Dec 6 [cited 2025 Apr 7];5(4):e14413. Available from: http://publichealth.jmir.org/2019/4/e14413/ https://doi.org/10.2196/14413
, [11]
Al-Dubaiee R, Al Qassimi M, Al-Dar A, Al Serouri A, Khader Y. Impact of the protracted war in yemen on the acute flaccid paralysis surveillance system: retrospective descriptive analysis. JMIR Public Health Surveill [Internet]. 2021 May 19 [cited 2025 Apr 7];7(5):e27638. Available from: https://publichealth.jmir.org/2021/5/e27638 https://doi.org/10.2196/27638
and previous studies carried out in Iran and Sudan [17]
Momen AA, Shakurnia A, Momen M. Eleven-year surveillance of acute flaccid paralysis in southwestern Iran. Turk J Pediatr [Internet]. 2019 Aug 25 [cited 2025 Apr 7];61(4):544–51. Available from: https://turkjpediatr.org/article/view/733 https://doi.org/10.24953/turkjped.2019.04.011 Download PDF to view Full text
, [22]
Tegegne AA, Maleghemi S, Anyuon AN, Zeleke FA, Legge GA, Ferede MA, et al. The sensitivity of acute flaccid paralysis surveillance-the case of South Sudan: retrospective secondary analysis of AFP surveillance data 2014-2019. Pan Afr Med J [Internet]. 2022 Jun 11 [cited 2025 Apr 7];42(1): 12. Available from: https://www.panafrican-med-journal.com/content/series/42/1/12/full/ https://doi.org/10.11604/pamj.supp.2022.42.1.33965
but is different from a study conducted in Jordan [20]
Zerriouh F, Khader Y, Qasem N, Abusal K, Iblan I, Ghaffari L, Abdallat M. Evaluation of the acute flaccid paralysis surveillance system in polio-free Jordan, 2012-2016: retrospective secondary analysis. JMIR Public Health Surveill [Internet]. 2019 Sep 27 [cited 2025 Apr 7];5(3):e14217. Available from: http://publichealth.jmir.org/2019/3/e14217/ https://doi.org/10.2196/14217
. The peak was in 2016, and this could be explained by active AFP surveillance and efforts from central levels in strengthening surveillance activities and peripheral levels in the notification. It may also be supported by community-based surveillance.
The sample adequacy met the target in all years except in 2017, which is similar to the national study conducted for the evaluation AFP Surveillance System before and after the war [11]
Al-Dubaiee R, Al Qassimi M, Al-Dar A, Al Serouri A, Khader Y. Impact of the protracted war in yemen on the acute flaccid paralysis surveillance system: retrospective descriptive analysis. JMIR Public Health Surveill [Internet]. 2021 May 19 [cited 2025 Apr 7];7(5):e27638. Available from: https://publichealth.jmir.org/2021/5/e27638 https://doi.org/10.2196/27638
. In 2017, delay in sample collection was the cause of inaequate samples among nine AFP cases. Eight samples, three of which came from the At Tahrir district had been pending at Djibouti without maintaining the cold chain
In general, all districts met the WHO target. However, Bani AL Harith, Shu’ub and Sana’a old city districts showed the highest NP-AFP rate as compared to other districts. Regarding sample adequacy, all districts met the WHO target except At Tahrir district (77%). The sample adequacy target was unmet according to two national studies conducted before [9]
Almoayed KA, Bin Break A, Al-Qassimi M, Assabri A, Khader Y. The acute flaccid paralysis (Afp) surveillance system in yemen, 2010-2015: descriptive study based on secondary data analysis. JMIR Public Health Surveill [Internet]. 2019 Dec 6 [cited 2025 Apr 7];5(4):e14413. Available from: http://publichealth.jmir.org/2019/4/e14413/ https://doi.org/10.2196/14413
,[11]
Al-Dubaiee R, Al Qassimi M, Al-Dar A, Al Serouri A, Khader Y. Impact of the protracted war in yemen on the acute flaccid paralysis surveillance system: retrospective descriptive analysis. JMIR Public Health Surveill [Internet]. 2021 May 19 [cited 2025 Apr 7];7(5):e27638. Available from: https://publichealth.jmir.org/2021/5/e27638 https://doi.org/10.2196/27638
. These recurrent findings show that there is a gap and difficulty in meeting the target of specimen adequacy. This may be attributed to delay in detection and collection of stools due to a lack of training and logistics, or an unmaintained cold chain, leading to stools not arriving in good condition. In At Tahrir district, there were five cases out of 22 that had inadequate samples. In 2015; there was one inadequate sample attributed to transportation delays due to the impact of war. In 2017, three samples stayed at Djibouti for three months in a bad package without maintaining the reverse cold chain. In 2020, one sample was detected as inadequate due to delayed transportation to a WHO-accredited polio lab. This delay was linked to the effects of the COVID-19 pandemic on vaccine-preventable diseases, and quarantine measures at the airport.
The absence of a national laboratory for poliovirus testing in Yemen poses significant challenges, as samples are currently stored within the national AFP surveillance program before being dispatched to the WHO referral laboratory. High stool adequacy over the study period in the most districts is similar to a study conducted in Uganda [4]
Amodan BO, Kisakye A, Okumu PT, Ahirirwe SR, Kadobera D, Driwale A, Ario AR. Trends of key surveillance performance indicators of acute flaccid paralysis: a descriptive analysis, Uganda, 2015–2020. BMC Public Health [Internet]. 2022 Sep 7 [cited 2025 Apr 7];22(1):1694. Available from: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-022-14077-w https://doi.org/10.1186/s12889-022-14077-w
. Regular analysis of AFP surveillance data is important to identify the trends in cases and discover any gaps in the system performance and abnormal observations beyond what is expected. Although this study was a secondary data analysis, it enabled stakeholders and researchers to identify trends, changes, and patterns of problems under investigation. It also helped us conduct local comparative analysis by time, place, and person.
We concluded that the AFP surveillance system in Sana’a city during the 10 years period, has successfully fulfilled the WHO-recommended surveillance standard. However, we found that in 2017, the sample adequacy fell short of the expected minimal (80%) level. According to the district, the At Tahrir district failed to meet the sample adequacy target. More than half of AFP cases had received 4 or more doses of OPV. The highest percent of zero doses of AFP cases were reported in 2020. Majority of AFP cases were five years old or younger and males. Most cases had fever at the onset of paralysis. It is advised to preserve and improve the two primary AFP surveillance parameters, particularly sample adequacy.
To guarantee that AFP indicators are met, health professionals should be trained on the correct collection and transportation of specimens. It is essential to ensure that facilities are equipped with stool sample kits designed for transportation under-maintained reverse cold chain conditions. It was recommended that the first specimen should be collected at the time of the investigation. To avoid delays and minimize exposure to heat, timely shipment of samples to the reference lab is recommended. It is advisable to establish a national laboratory in Yemen that adheres to WHO-recommended procedures for the detection of polioviruses in stool samples. Furthermore, maintaining high coverage through routine immunization (RI) and supporting supplementary immunization activities (SIAs) is crucial to ensure that most children are vaccinated, thereby contributing to the eradication of polio.
What is already known about the topic
What this study adds
All authors participated in data interpretation, and revision, which was led by Lamya AL Aroomi. Lamya and Labiba drafted the manuscript, which was critically revised and approved by all authors. Lamya AL Aroomi was the principal author who designed the study protocol, which was reviewed by Labiba Anam and Mutahar AL Qassemi. Faten Hamid Ezzadeen assisted the author in obtaining and understanding each variable of the data.
| Characteristics | Year of onset of paralysis | Total N (%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2012 n (%) | 2013 n (%) | 2014 n (%) | 2015 n (%) | 2016 n (%) | 2017 n (%) | 2018 n (%) | 2019 n (%) | 2020 n (%) | 2021 n (%) | ||
| Sex | |||||||||||
| Male | 18 (54.5) | 16 (47.0) | 25 (65.7) | 21 (50.0) | 33 (43.4) | 43 (64.1) | 39 (65.0) | 36 (49.3) | 47 (59.4) | 56 (61.5) | 334 (56.3) |
| Female | 15 (45.4) | 18 (52.9) | 13 (34.2) | 21 (50.0) | 43 (56.5) | 24 (35.8) | 21 (35.0) | 37 (50.6) | 32 (40.5) | 35 (38.4) | 259 (43.6) |
| Age | |||||||||||
| 0–5 years | 24 (72.7) | 19 (55.8) | 19 (50.0) | 33 (78.5) | 52 (68.4) | 39 (58.2) | 33 (55.0) | 41 (56.1) | 44 (55.7) | 49 (53.8) | 353 (59.5) |
| 6–9 years | 5 (15.1) | 5 (14.7) | 8 (21.0) | 4 (9.5) | 9 (11.8) | 12 (17.9) | 12 (20.0) | 14 (19.2) | 18 (22.7) | 10 (10.9) | 97 (16.3) |
| 10–15+ | 3 (12.1) | 10 (29.4) | 11 (28.9) | 5 (11.9) | 15 (19.7) | 16 (23.8) | 15 (25.0) | 18 (24.6) | 17 (21.0) | 32 (35.1) | 143 (24.1) |
| Vaccination status | |||||||||||
| Zero dose | 5 (15.1) | 5 (14.7) | 6 (15.7) | 1 (2.3) | 1 (1.3) | 8 (11.9) | 4 (6.6) | 9 (12.3) | 20 (25.3) | 14 (15.3) | 73 (12.3) |
| 1–3 doses | 15 (45.4) | 12 (35.2) | 9 (23.6) | 11 (26.1) | 9 (21.0) | 9 (13.4) | 18 (30.0) | 23 (31.5) | 16 (20.2) | 36 (31.8) | 158 (26.6) |
| >=4 doses | 13 (39.3) | 17 (50.0) | 23 (60.5) | 30 (71.4) | 59 (77.6) | 50 (74.6) | 38 (63.3) | 41 (56.1) | 43 (54.4) | 43 (52.7) | 362 (61.0) |
| Clinical history | |||||||||||
| Fever at onset of paralysis | 21 (63.6) | 22 (64.7) | 35 (92.1) | 36 (85.7) | 57 (75.0) | 53 (79.1) | 55 (91.6) | 62 (84.9) | 55 (69.6) | 73 (80.2) | 469 (79.0) |
| Paralysis progressed within 3 days | 28 (84.8) | 25 (73.5) | 28 (73.6) | 30 (71.4) | 57 (75.0) | 56 (83.5) | 43 (81.6) | 61 (83.5) | 52 (80.0) | 57 (62.6) | 437 (73.6) |
| Asymmetrical paralysis | 9 (27.2) | 7 (20.5) | 10 (26.3) | 3 (7.1) | 30 (39.4) | 22 (47.7) | 22 (36.6) | 21 (28.5) | 26 (25.5) | 26 (28.6) | 202 (34.0) |
| Performance Indicators | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 |
|---|---|---|---|---|---|---|---|---|---|---|
| Number of cases reported annually | 33 | 34 | 38 | 42 | 76 | 67 | 60 | 73 | 79 | 91 |
| Non-polio AFP rate/100,000 below 15 yrs. (Target ≥2) | 2.6 | 2.6 | 2.7 | 2.8 | 4.9 | 4.1 | 3.4 | 4.0 | 4.1 | 4.6 |
| Proportion of AFP cases with Adequate sample (Target ≥80%) | 90.9 | 82.3 | 97.3 | 88.1 | 88.1 | 74.6 | 95 | 91.7 | 88.6 | 91.2 |
| Lab result | N | % |
|---|---|---|
| No virus isolated | 500 | 84.3 |
| Non-polio enteroviruses | 79 | 13.3 |
| Sabin-like (SL) | 10 | 1.7 |
| Discarded by NPEC* | 4 | 0.7 |
Views: 5,264
Menu, Tables and figures
| Characteristics | Year of onset of paralysis | Total N (%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2012 n (%) | 2013 n (%) | 2014 n (%) | 2015 n (%) | 2016 n (%) | 2017 n (%) | 2018 n (%) | 2019 n (%) | 2020 n (%) | 2021 n (%) | ||
| Sex | |||||||||||
| Male | 18 (54.5) | 16 (47.0) | 25 (65.7) | 21 (50.0) | 33 (43.4) | 43 (64.1) | 39 (65.0) | 36 (49.3) | 47 (59.4) | 56 (61.5) | 334 (56.3) |
| Female | 15 (45.4) | 18 (52.9) | 13 (34.2) | 21 (50.0) | 43 (56.5) | 24 (35.8) | 21 (35.0) | 37 (50.6) | 32 (40.5) | 35 (38.4) | 259 (43.6) |
| Age | |||||||||||
| 0–5 years | 24 (72.7) | 19 (55.8) | 19 (50.0) | 33 (78.5) | 52 (68.4) | 39 (58.2) | 33 (55.0) | 41 (56.1) | 44 (55.7) | 49 (53.8) | 353 (59.5) |
| 6–9 years | 5 (15.1) | 5 (14.7) | 8 (21.0) | 4 (9.5) | 9 (11.8) | 12 (17.9) | 12 (20.0) | 14 (19.2) | 18 (22.7) | 10 (10.9) | 97 (16.3) |
| 10–15+ | 3 (12.1) | 10 (29.4) | 11 (28.9) | 5 (11.9) | 15 (19.7) | 16 (23.8) | 15 (25.0) | 18 (24.6) | 17 (21.0) | 32 (35.1) | 143 (24.1) |
| Vaccination status | |||||||||||
| Zero dose | 5 (15.1) | 5 (14.7) | 6 (15.7) | 1 (2.3) | 1 (1.3) | 8 (11.9) | 4 (6.6) | 9 (12.3) | 20 (25.3) | 14 (15.3) | 73 (12.3) |
| 1–3 doses | 15 (45.4) | 12 (35.2) | 9 (23.6) | 11 (26.1) | 9 (21.0) | 9 (13.4) | 18 (30.0) | 23 (31.5) | 16 (20.2) | 36 (31.8) | 158 (26.6) |
| >=4 doses | 13 (39.3) | 17 (50.0) | 23 (60.5) | 30 (71.4) | 59 (77.6) | 50 (74.6) | 38 (63.3) | 41 (56.1) | 43 (54.4) | 43 (52.7) | 362 (61.0) |
| Clinical history | |||||||||||
| Fever at onset of paralysis | 21 (63.6) | 22 (64.7) | 35 (92.1) | 36 (85.7) | 57 (75.0) | 53 (79.1) | 55 (91.6) | 62 (84.9) | 55 (69.6) | 73 (80.2) | 469 (79.0) |
| Paralysis progressed within 3 days | 28 (84.8) | 25 (73.5) | 28 (73.6) | 30 (71.4) | 57 (75.0) | 56 (83.5) | 43 (81.6) | 61 (83.5) | 52 (80.0) | 57 (62.6) | 437 (73.6) |
| Asymmetrical paralysis | 9 (27.2) | 7 (20.5) | 10 (26.3) | 3 (7.1) | 30 (39.4) | 22 (47.7) | 22 (36.6) | 21 (28.5) | 26 (25.5) | 26 (28.6) | 202 (34.0) |
| Performance Indicators | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 |
|---|---|---|---|---|---|---|---|---|---|---|
| Number of cases reported annually | 33 | 34 | 38 | 42 | 76 | 67 | 60 | 73 | 79 | 91 |
| Non-polio AFP rate/100,000 below 15 yrs. (Target ≥2) | 2.6 | 2.6 | 2.7 | 2.8 | 4.9 | 4.1 | 3.4 | 4.0 | 4.1 | 4.6 |
| Proportion of AFP cases with Adequate sample (Target ≥80%) | 90.9 | 82.3 | 97.3 | 88.1 | 88.1 | 74.6 | 95 | 91.7 | 88.6 | 91.2 |
| Lab result | N | % |
|---|---|---|
| No virus isolated | 500 | 84.3 |
| Non-polio enteroviruses | 79 | 13.3 |
| Sabin-like (SL) | 10 | 1.7 |
| Discarded by NPEC* | 4 | 0.7 |
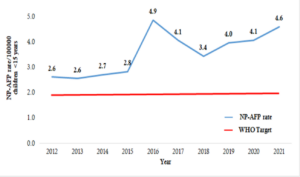
Figure 1: Trends of non-polio AFP rate, Sana’a City, Yemen, 2012-2021
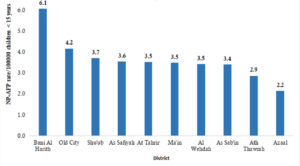
Figure 2: Mean of Non-Polio AFP rate /100,000 by districts, Sana’a city, Yemen, 2012-2021
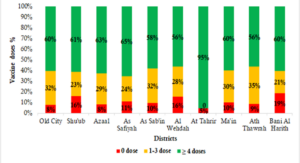
Figure 3: Doses of Oral Polio Vaccine of AFP cases by districts, Sana’a city, Yemen, 2012-2021 n=593